Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
PTSD patients show increasing cytokine levels during treatment despite reduced psychological distress
Authors Toft H ![]() , Bramness JG, Lien L, Abebe DS, Wampold BE, Tilden T, Hestad KA
, Bramness JG, Lien L, Abebe DS, Wampold BE, Tilden T, Hestad KA ![]() , Neupane SP
, Neupane SP ![]()
Received 9 May 2018
Accepted for publication 2 July 2018
Published 17 September 2018 Volume 2018:14 Pages 2367—2378
DOI https://doi.org/10.2147/NDT.S173659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Helge Toft,1,2 Jørgen G Bramness,1,3 Lars Lien,1,4 Dawit S Abebe,1,5 Bruce E Wampold,6,7 Terje Tilden,6 Knut Hestad,4,8,9 Sudan Prasad Neupane1,10
1Norwegian National Advisory Unit on Concurrent Substance Abuse and Mental Health Disorders, Innlandet Hospital Trust, Ottestad, Norway; 2Institute of Clinical Medicine, University of Oslo, Oslo, Norway; 3Institute of Clinical Medicine, UiT, Norway's Arctic University, Tromsø, Norway; 4Department of Health Studies, Inland Norway University of Applied Sciences, Elverum, Norway; 5Department of Nursing and Health Promotion, Oslo Metropolitan University, Oslo, Norway; 6Research Institute, Modum Psychiatric Center, Vikersund, Norway; 7Department of Counseling Psychology, University of Wisconsin-Madison, Madison, WI, USA; 8Department of Research, Innlandet Hospital Trust, Brumunddal, Norway; 9Department of Psychology, Norwegian University of Science and Technology (NTNU), Trondheim, Norway; 10Norwegian Center for Addiction Research (SERAF), Institute of Clinical Medicine, University of Oslo, Oslo, Norway
Background: A reciprocal relationship between activated innate immune system and changes in mood and behavior has been established. There is still a paucity of knowledge on how the immune system responds during psychiatric treatment. We aimed to explore circulating cytokines and assess psychiatric symptom severity scores during 12 weeks of inpatient psychiatric treatment.
Methods: The study was a longitudinal assessment of 124 patients (88 women and 36 men) in treatment at Modum Psychiatric Center, Norway. The patient sample comprised a mixed psychiatric population of whom 39 were diagnosed with posttraumatic stress disorder (PTSD). Serum blood samples for cytokine analysis and measures of mental distress using Global Severity Index were collected at admission (T0), halfway (T1), and before discharge (T2). Other factors assessed were age, gender, and the use of antidepressants and anti-inflammatory drugs. Multilevel modeling was used for longitudinal analyses to assess the repeated cytokine samples within each patient.
Results: Overall level of IL-1RA was higher in PTSD patients when compared to those without PTSD (P=0.021). The level of IL-1β, MCP-1, and TNF-α increased over time in PTSD compared to non-PTSD patients (P=0.025, P=0.011 and P=0.008, respectively). All patients experienced reduced mental distress as measured by self-reported Global Severity Index scores. Stratified analysis showed that PTSD patients who used anti-inflammatory drugs had higher levels of IL-1β (P=0.007) and TNF-α (P=0.049) than PTSD patients who did not use such drugs.
Conclusion: The study indicates that traumatized patients may have a distinct neuroimmune development during recovery. Their activated immune system shows even further activation during their rehabilitation despite symptom reduction.
Keywords: cytokines, trauma, inflammation, PTSD, immune activation
Introduction
Patients with various psychiatric disorders have been found to exhibit a low-grade inflammatory state characterized by elevated levels of pro- and anti-inflammatory cytokines.1,2 In particular, major depression disorder (MDD) and inflammation has been extensively studied in the recent years. Cytokine levels have been found to be elevated in depression3 and to be reduced over time following treatment.4
The large body of evidence on heightened circulating cytokines in MDD patients contrasts the conflicting and lesser evidence on immune response in patients with PTSD.5 Previous research has shown both altered immune response and no difference from healthy controls in cross-sectional assessments.6 Further, some studies have reported that recovery from PTSD and MDD is accompanied by reduction in levels of various pro- and anti-inflammatory cytokines, even to the levels of healthy controls, regardless of treatment modality or outcome.7,8 Such correlations highlight the possibility that specific immune markers may be useful in monitoring and intervening in the involved neuroimmune dysregulation.9 Treatment of patients with PTSD could improve not only symptoms but also rebalance the chronic inflammatory state, as measured by levels of circulating inflammatory cytokines.
Inconsistent findings in previous research could be due to various confounders like the use of anti-inflammatory drugs,10 which might alter inflammatory activity by inhibiting production of enzymes COX-1 and COX-2.11 Such drugs have been reported to relieve depression symptoms by reducing levels of IL-6,12 and also attenuate effects of the antidepressive selective serotonin reuptake inhibitors drugs when used in combination.13
We have earlier found bivariate associations between trauma and IL-1RA and TNF-α in a cross-sectional assessment,14 and we decided to explore these relationships longitudinally. Research suggests that the immunological response in PTSD patients differs from the response in psychiatric patients without PTSD. On this background, we hypothesized that patients with PTSD might have higher cytokine levels and possibly increasing trajectories over time, and thus exhibit an inflammatory pattern different from other patients. The aim was to explore levels and development of cytokines in PTSD patients vs patients without PTSD, and see this in light of their self-reported levels of mental distress, taking the use of anti-inflammatory drugs into account.
Materials and methods
Study participants and recruitment procedure
The study is part of a larger research project and some methods have been presented elsewhere.14 The patients were recruited from a high-threshold psychiatric center in Norway treating patients with depression, anxiety, and eating or trauma disorders. Enrolled patients have previously tried treatment elsewhere with no or little success, many of them for years. They were offered a 12 weeks inpatient treatment program where a multidisciplinary staff provided psychotherapy treatment and psychoeducation both in groups and individually. Psychopharmacological treatment was used to some extent, but hospital policy restricted the use of such drugs to a minimum. Patients with self-destructive behavior, severe substance abuse, or psychotic disorders were not treated here, but some patients may have had comorbid addiction. Data were collected from March 2015 until April 2016 by the first author. The patients received written and oral information about the study during one of their first group sessions. Of the 249 patients approached, 148 (59%) gave their written consent. One patient chose to withdraw her consent. We identified 19 patients to have extreme cytokine levels above the 95th percentile, and they were excluded due to suspected ongoing infections. One additional female patient was excluded from cytokine analyses due to failed venipuncture, and lastly 4 patients were identified as outliers and excluded after residual diagnostics was conducted. The study thus consisted of 88 women (71%, mean age 38.98 years, SD 11.31) and 36 men (29%, mean age 49.06 years, SD 9.36), giving a total of 124 patients. The study was approved by the Norwegian Regional Committee for Medical and Health Research Ethics prior to data collection (reference number 2014/2189).
Methods
A psychiatrist or psychologist at the facility performed the MINI clinical interview,15 giving diagnosis according to the 10th Revision of the International Classification of Diseases and Related Health Problems (ICD-10). Thirty-one patients met the criteria for PTSD diagnosis as their primary disorder, with an additional 8 with PTSD as secondary diagnosis, 31 patients with mood disorders, 54 with anxiety disorders, and 20 with eating disorders. There were 53 patients diagnosed with 1 disorder, 56 with 2 disorders or more, and 15 patients with no registered disorder due to missing data. These 15 patients were excluded from analyses involving diagnoses. The symptom severity was assessed by the patients themselves using the Hopkins Symptom Checklist (HSCL-90R) questionnaire. The patients filled out the digital questionnaire on a computer or tablet 3 times during their stay during one of the first days (T0), the second at halfway (T1), and the last just before discharge (T2). The 90 questions measure the level of general distress for the last 7 days. The answers to each question range from 0 to 4 and corresponds to “not at all,” “a little bit,” “moderately,” “quite a bit,” and “extremely.” Mean score is calculated for the HSCL-90R, referred to as the Global Severity Index Index (GSI).16 The HSCL-90R has been found to provide valid evaluation of the severity of symptoms in a broad range of psychiatric patients.17 Based on previous literature, we set the cutoff score for caseness at 0.85.18 The drugs that the patients used during the stay were recorded by the first author by looking into their medical charts.
Blood collection and serum preparation
The blood samples were also drawn at T0, T1 and T2. The blood samples were collected between 08.00 am and 09.00 am, except for one of the groups from the department of depression, who had their blood drawn between 12.00 am and 3.00 pm. Vacuette 8 mL serum containers were used for blood collection. These were turned upside-down for approximately 8–10 times immediately after the blood was drawn, and set to rest in a blood tube stand for a minimum of 30 minutes and a maximum of 1 hour. They were then centrifuged in a Kubota 2420 swing-out centrifuge set at 10 minutes. The centrifugation power reached 1,917 g, and the centrifugal process was conducted at room temperature. Finally, the blood was drawn with 1 mL single-use pipettes into Nunc tubes before they were set to rest in −80°C until assay.
Cytokine and chemokine measurements
We analyzed 7 cytokines and 1 chemokine based on the available literature on the neuroimmune correlates of psychiatric disorders. The cytokines were IL-1β, IL-1RA, IL-6, IL-10, IL-17A, IFN-y, and TNF-α and the chemokine was MCP-1. Four cytokines had too many values under the limit of detection (LOD) (>55%) and were excluded from the study. The following markers were taken into consideration: IL-1β, IL-IRA, MCP-1 and TNF-α. All blood samples were thawed on ice, vortexed, and then spun down a tube with 250 μL serum at 14,000× g for 10 minutes at 4°C, before before a 4 fold dilution and further processing. Cytokine measurements were performed using Bio-Plex xMAP technology (Bio-Rad, Austin, TX, USA) with a Luminex IS 100 instrument (Bio-Rad), powered using Bio-Plex Manager (version 6.0.1) software (Bio-Rad). The assay was performed according to the manufacturer’s instructions, but an additional standard point was included. To achieve more reliable results, individual sets of samples from patients were run in the same assay, all samples were assayed in duplicate and a magnetic plate washer was used during assay set up. The StatLIA software package (ver. 3.2, Brendan Scientific, Carlsbad, CA, USA), incorporating a weighted, 5-parameter logistic curve-fitting method, was used to calculate sample cytokine concentrations. Longitudinal controls were used in order to validate interassay variation; IL-1β (18.1), IL-1RA (10.2), MCP-1 (6.7), and TNF-α (7.4). The interassay percent coefficient of variability (CV) in parentheses is a measure of variation between plates, where a lower figure is better. Any figure below 21% is considered acceptable. The mean interassay percent CV for all blood sample plates was 10.4%. The unit of measurement was picograms per milliliter (pg/mL). The LODs were 0.01 pg/mL for IL-1β, 3 pg/mL for IL-1RA, 0.76 pg/mL for MCP-1, and 0.02 pg/mL for TNF-α.
Imputation
Cytokine levels below LOD were imputed with 1% of the mean value. At T0 we performed 64 (50.39%) imputations for IL-1β, 1 (0.8%) for IL-1RA, 9 (7.1%) for MCP-1, and 53 (41.7%) for TNF-α. One patient did not have the first blood sample collected. At T1, there were 62 imputations (51.2%) for IL-1β, no imputations for IL-1RA, 5 (5.2%) for MCP-1, and 7 (5.8%) for TNF-α. Seven patients did not show up for blood sampling at T1. At T2, we had 64 imputations (53.8%) for IL-1β, no imputations for IL-1RA, 8 (7.2%) for MCP-1, and 45 (37.8%) for TNF-α. Eleven patients did not show up for blood sampling at T2.
Statistical analyses
The Mann–Whitney U Test, the Wilcoxon signed rank test and the Kruskal–Wallis equality-of-populations rank test were used for bivariate analyses at T0 and to assess differences in GSI scores between groups at T0, T1, and T2. Multilevel modeling was conducted for longitudinal data analyses.19 The material comprised 3 observations of each patient, which gave a 2-level structure with cytokine measurements nested within patients across time. Due to the dependency of cytokine measurements within patients, multilevel modeling was chosen as the statistical method for the longitudinal results. In multilevel modeling, all available data is used. Thus, a patient lacking data from one measurement is still included and contributes to estimation of model parameters. We used a stepwise modeling approach, where the multilevel models were initially run as empty models including only the dependent variable and random intercept. Next, a random slope was added in models. The −2 Log Likelihood and Bayes Information Criterion (BIC) were performed to assess model fit. A model with random intercept and slope gave a better fit for all cytokines than a model with random intercept only. Patients differed at cytokine levels at treatment initiation, and allowing the patients to have different slopes of cytokines during treatment improved model fit. The following likelihood ratio tests were performed: IL-1β: χ2(2) =17.96, P≤0.001, IL-1RA: χ2(2) =15.09, P≤0.001, MCP-1: χ2(2) =12.90, P≤0.001, and TNF-α: χ2(2) =55.85, P≤0.001. The fixed and random effects are presented in Table S1. The assumption of homoscedastic residual variance and normally distributed residuals was inspected by plotting residual distribution in histograms and QQ-plots with Gauss curves. It was formally confirmed with likelihood ratio tests that the residual variance differed over time for IL-1β (χ2[2] =14.01, P<0.001), for TNF-α (χ2[2] =7.20, P=0.027), and for IL-1RA (χ2[2] =55.02, P<0.001). Chemokine MCP-1 did not improve model fit when we allowed for heteroscedastic residuals (χ2[2] =3.27, P=0.195), and thus the assumption of homoscedastic residuals was considered met for MCP-1. Consequently, we allowed for heteroscedastic residual distribution for IL-1β, IL-1RA, and TNF-α, which gave a block diagonal structure in the covariance matrix for the residuals, allowing the estimates in each block to differ. For all four markers, we applied robust standard errors to account for nonnormally distributed errors. The assumption of linearity was confirmed by visually inspecting spaghetti plots of cytokine development. Unstructured covariance was chosen due to the low number of repeated measurements. All multilevel models were in addition adjusted for age and gender, which did not significantly alter the P-values. Consequently, we chose to present the results without this adjustment. Some patient groups had different lengths of inpatient stay due to holiday seasons and due to minor differences between departments. Because of this inequality, the average length of stay for all patient groups was calculated. This gave a time variable encoded as 0 (T0), 5 weeks (T1), and 11 weeks (T2) of stay. For bivariate analyses, we attempted to normalize the skewed cytokine data by log transformation. The Kolmogorov–Smirnov test of normality remained significant after log transformation. We also explored bivariate analyses with and without log transformed data and found no significant changes. We then decided to run all analyses with nontransformed data. Those who did not attend every blood sample collection were defined as missing completely at random (MCAR), which indicated no specific pattern of missing data. Consequently, there was no increased variability which could bias the regression coefficients. MCAR was confirmed by Little’s MCAR test20 with χ2=9.73 (P=0.973). All tests were 2-sided, and P-values below 0.05 were considered statistically significant. No correction for multiple hypothesis testing was implemented as we considered the study to be exploratory. The statistical package STATA (StataCorp. 2015, Stata Statistical Software: Release 15, StataCorp LP, College Station, TX, USA) was used for all statistical analyses.
Results
Table 1 shows the mean cytokine levels across demographic variables and sample characteristics at T0. Male patients had higher levels of chemokine MCP-1 (P=0.046). Patients who used anti-inflammatory drugs were found to have higher levels of cytokine IL-1β (P=0.038), and almost reached significance in levels of TNF-α (P=0.062). Having PTSD diagnosis was almost related to higher levels of cytokine IL-1RA (P=0.074).
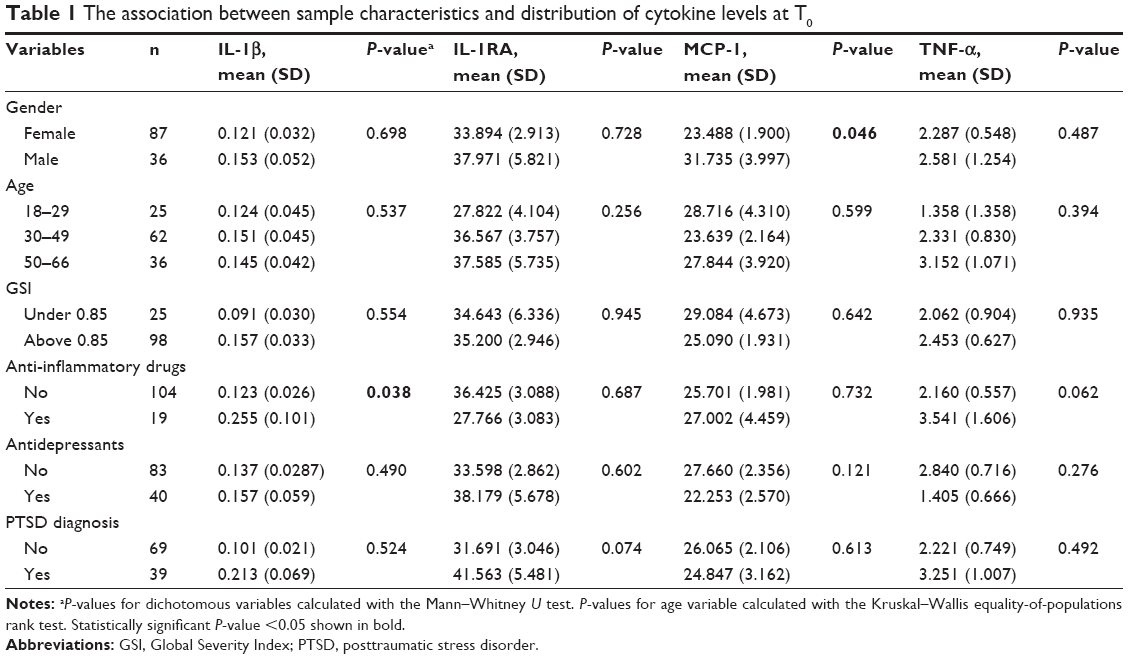 | Table 1 The association between sample characteristics and distribution of cytokine levels at T0 |
When analyzing the main effect of PTSD and the effect of PTSD in interaction with time on cytokines (Table 2), we found that the overall level of IL-1RA was higher in PTSD than in non-PTSD patients (P=0.021). Patients with PTSD showed increasing development of IL-1β (P=0.025), MCP-1 (P=0.011), and TNF-α (P=0.008). The initial levels and decreasing GSI score in all patients are visualized in Figure 1. Bivariate analysis of GSI score differed between PTSD and non-PTSD at T0 (P=0.007) and T2 (P=0.001). Patients without PTSD decreased from T0 to T1 (P=0.017), from T1 to T2 (P=0.003), and from T0 to T2 (P≤0.001). Patients with PTSD decreased from T0 to T1 (P=0.024) and from T0 to T2 (P=0.051). The level and development of cytokines IL-1β, IL-1RA, and TNF-α and chemokine MCP-1 are illustrated in Figure 2A–D.
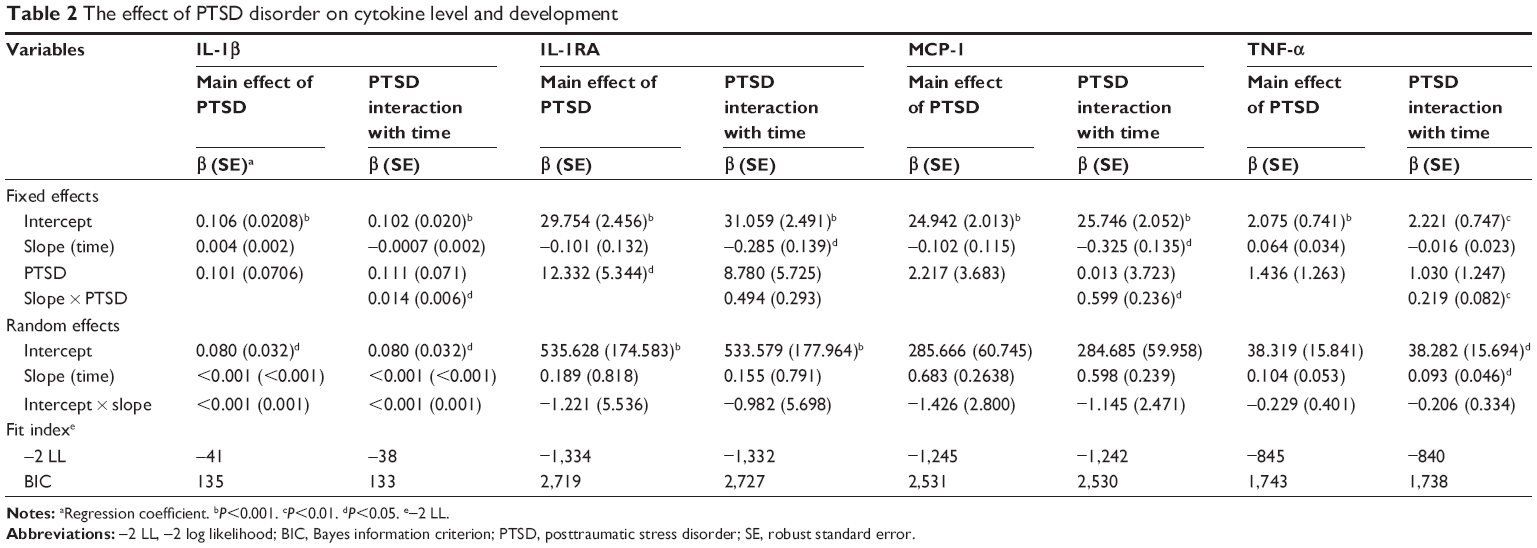 | Table 2 The effect of PTSD disorder on cytokine level and development |
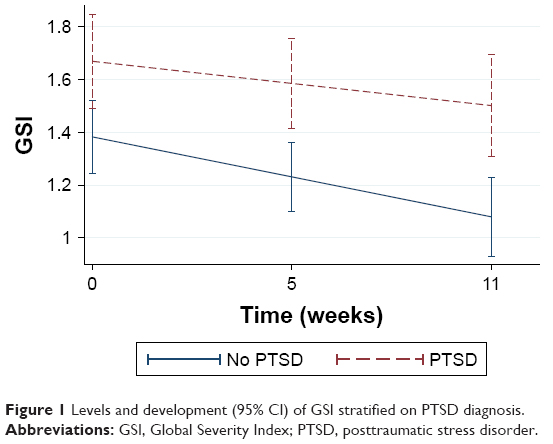 | Figure 1 Levels and development (95% CI) of GSI stratified on PTSD diagnosis. |
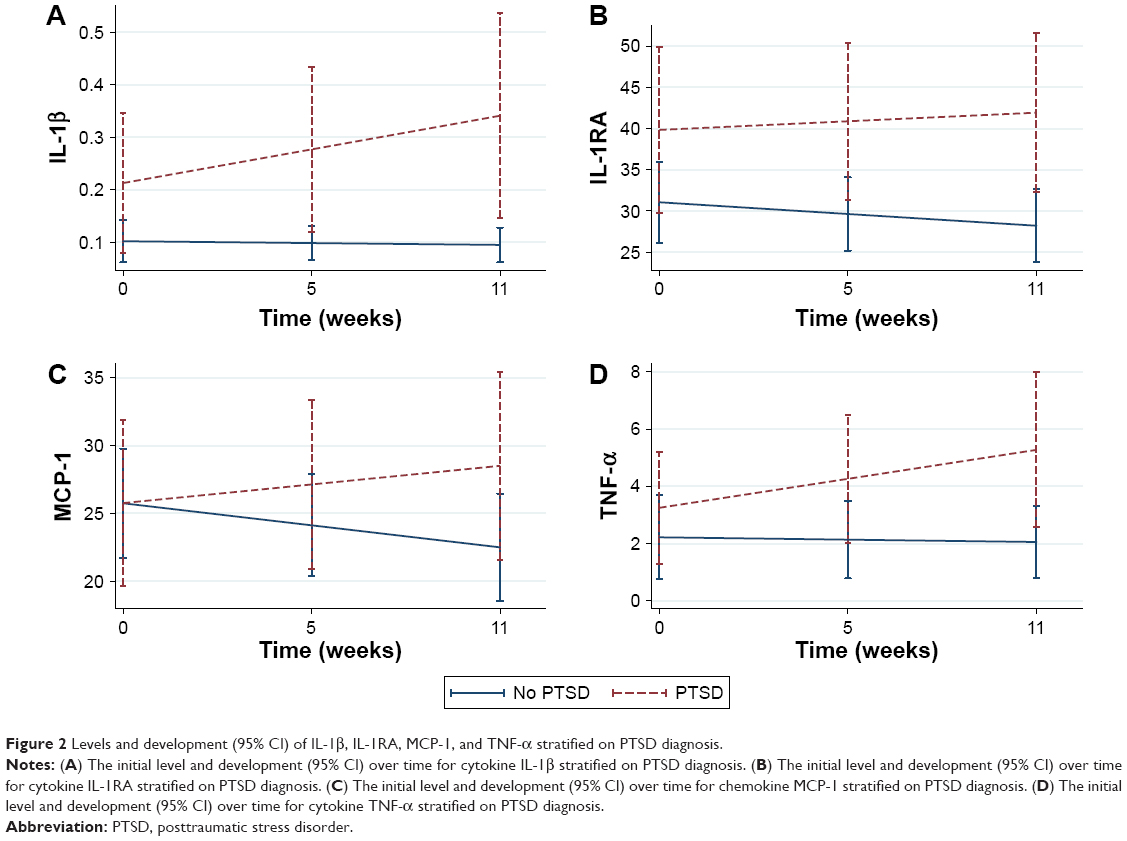 | Figure 2 Levels and development (95% CI) of IL-1β, IL-1RA, MCP-1, and TNF-α stratified on PTSD diagnosis. |
Those of the general patient sample who used anti-inflammatory drugs during treatment (n=27) were found to have higher overall levels of IL-1β (P<0.05) than those who did not (n=97) use such drugs (Table 3). To disentangle the relationship between cytokines, PTSD, and anti-inflammatory drugs, we stratified PTSD disorder and ran the anti-inflammatory drugs variable as a predictor and in interaction with time. The patients with PTSD (Table S2) who used anti-inflammatory drugs (n=12) had a higher overall level of IL-1β (P=0.007) as compared to PTSD patients who did not use such drugs (n=28). We also found a higher overall level of TNF-α in this strata (P=0.049). The patients without PTSD (Table S3) who used anti-inflammatory drugs (n=13) had an overall level of MCP-1 which was higher (P=0.025) than in those who did not use such drugs (n=56).
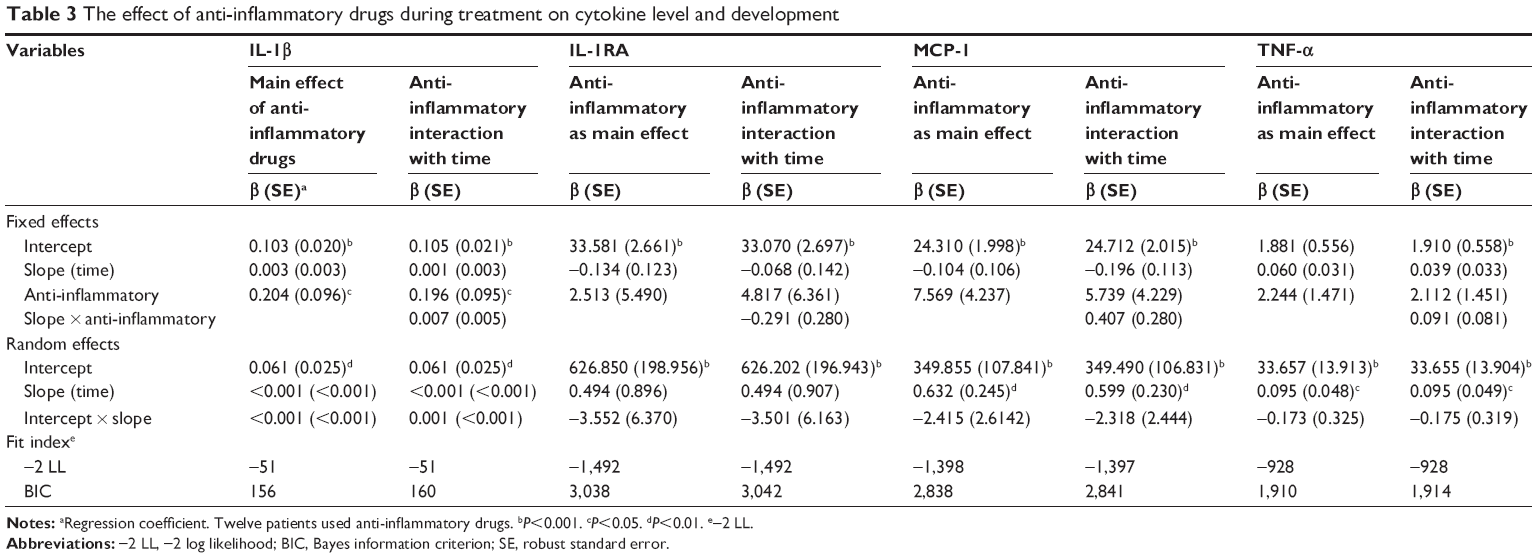 | Table 3 The effect of anti-inflammatory drugs during treatment on cytokine level and development |
Discussion
In this study, having PTSD disorder was related to higher overall level of anti-inflammatory cytokine IL-1RA when compared to patients without PTSD diagnosis. An increasing development of proinflammatory cytokines IL-1β and TNF-α and of proinflammatory chemokine MCP-1 was found. The increasing development during treatment occurred in parallel with a decreasing level of symptom severity, as indicated by the self-reported GSI score.
Our findings are in accordance with some, but not all previous research. Studies have found PTSD symptoms to decrease over time,10 with increasing IL-1β levels,21 but also with decreasing IL-1β levels.22 Increasing levels of TNF-α have also been found despite decreasing symptom severity.23 The patients who received inpatient psychotherapy, as our patients did, showed increasing cytokine levels during treatment. Possibly, PTSD patients in inpatient intensive treatment reexperience previous trauma through talk therapy or by exposure therapy, while nontraumatized individuals may not have such an experience in their therapy sessions. Also, patients suffering from PTSD are known to have disruption in their hypothalamic-pituitary-adrenal (HPA) axis vs immune system feedback and may have adapted to prolonged cortisol release24 resulting from years of chronic stress, inflammation, and cortisol production. In the short term, these responses would be desirable in attempts to protect the individual, but the chronic inflammatory activation in PTSD patients ultimately results in an impaired feedback regulation due to glucocorticoid resistance.25
Cytokine TNF-α is regarded as a key inflammatory cytokine of the immune response,26 but elevated levels of proinflammatory cytokines TNF-α and IL-1β have simultaneously been found in PTSD patients when compared to controls,27 and it has been postulated that a combination of several elevated cytokines may be an indicator of PTSD.26 We also found chemokine MCP-1 and cytokine IL-1β to increase over time in PTSD patients. It may be that increased TNF-α level accompanied by elevated IL-1β and MCP-1 could be viewed as biomarkers in PTSD. The increasing inflammatory response and the declining GSI score over 12 weeks in the current study suggests that PTSD patients who experience reduced psychiatric symptoms do not reflect their psychological improvement at the inflammatory level. Psychiatric symptoms were reduced, but this effect could possibly have been improved to a greater extent if immune rebalancing had occurred in parallel through pharmacotherapy targeting the immune system.28
Anti-inflammatory agents have been suggested to reduce IL-1β and play a role in future treatment of PTSD.10,29 We analyzed anti-inflammatory drug use in the patient sample in general to get an impression of overall levels and development of inflammatory markers. We found a higher level of IL-1β in those using anti-inflammatory drugs. As many studies suggest that PTSD patients differ in immunological response,30,31 we stratified the sample according to PTSD diagnosis. The overall levels of IL-1β, MCP-1, and TNF-α were higher in PTSD patients who used such drugs. In the strata of patients without PTSD who used anti-inflammatory drugs, there was a significant relationship with level of chemokine MCP-1. This could suggest that patients using anti-inflammatory drugs have a reduced immunological response, but PTSD patients do not seem to benefit from using such drugs. Anti-inflammatory drugs have been postulated as a future remedy in PTSD treatment in a systematic review,10 and could potentially have contributed to declining cytokine slopes over time if the observation period had been longer than 12 weeks. However, the current results do not lend support to this hypothesis. It should be noted that patients who used anti-inflammatory drugs at any time point during the stay were coded as users regardless of frequency of use. Cytokine levels are likely elevated in such patients due to infections and not due to the use of anti-inflammatory drugs, which makes cytokine levels in this group conditional to confounding by indication. In some respect, our results challenge the therapeutic use of pharmaceuticals with immunomodulating capabilities in treatment of PTSD patients, which has been suggested.6,10,29 Nevertheless, antidepressive drugs are hypothesized to partly act on mood disorders through anti-inflammatory effects,12,32 and have been found to have clinical effect on PTSD symptoms.28,33
A limitation to the present study is that the patients were not fasting at blood collection time. Meal frequency has been found to be associated with increased cytokine production.34 Further, body mass index was not measured. Both low and high amount of body fat has been reported to affect production of proinflammatory cytokines.35 Furthermore, we did not assess smoking status. Smokers have been found to have a higher basal level of cytokines when compared to nonsmokers.36 It is also important to take into consideration that the patients in the current study had their maladies for many years, many since their childhood, without improving from other psychiatric treatment. As such, they could be regarded as a treatment-resistant population with mental and biological status more trait-like than state-like. This suggests that 12 weeks of observation is a rather short amount of time for observing significant changes. This limits the conclusions that can be drawn. The reader should bear in mind that there is a risk of type 2 errors due to small sample size. The strength of this study is that we utilized a longitudinal design and analyzed cytokines over time in a mixed psychiatric population with a comparison between PTSD and non-PTSD patients.
Conclusion
Patients with PTSD had higher levels of some inflammatory markers, and their levels increased during treatment despite a decreasing symptom load.
Acknowledgment
We would like to thank the staff and patients at Modum Psychiatric Center who chose to participate in this study. We also want to thank Innlandet Hospital Trust, Health Region South-East, Norway, for funding this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Dantzer R, O’Connor JC, Lawson MA, Kelley KW. Inflammation-associated depression: from serotonin to kynurenine. Psychoneuroendocrinology. 2011;36(3):426–436. | ||
Wieck A, Grassi-Oliveira R, Hartmann do Prado C, Teixeira AL, Bauer ME. Neuroimmunoendocrine interactions in post-traumatic stress disorder: focus on long-term implications of childhood maltreatment. Neuroimmunomodulation. 2014;21(2–3):145–151. | ||
Köhler CA, Freitas TH, Maes M, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. 2017;135(5):373–387. | ||
Köhler CA, Freitas TH, Stubbs B, et al. Peripheral Alterations in Cytokine and Chemokine Levels After Antidepressant Drug Treatment for Major Depressive Disorder: Systematic Review and Meta-Analysis. Mol Neurobiol. 2018;55(5):4195–4206. | ||
Wang Z, Young MR. PTSD, a Disorder with an Immunological Component. Front Immunol. 2016;7:219. | ||
Passos IC, Vasconcelos-Moreno MP, Costa LG, et al. Inflammatory markers in post-traumatic stress disorder: a systematic review, meta-analysis, and meta-regression. Lancet Psychiatry. 2015;2(11):1002–1012. | ||
Dahl J, Ormstad H, Aass HC, Sandvik L, Malt UF, Andreassen OA. Recovery from major depressive disorder episode after non-pharmacological treatment is associated with normalized cytokine levels. Acta Psychiatr Scand. 2016;134(1):40–47. | ||
Gill JM, Saligan L, Lee H, Rotolo S, Szanton S. Women in recovery from PTSD have similar inflammation and quality of life as non-traumatized controls. J Psychosom Res. 2013;74(4):301–306. | ||
Maes M, Yirmyia R, Noraberg J, et al. The inflammatory & neurodegenerative (I&ND) hypothesis of depression: leads for future research and new drug developments in depression. Metab Brain Dis. 2009;24(1):27–53. | ||
Waheed A, Dalton B, Wesemann U, Ibrahim MAA, Himmerich H. A Systematic Review of Interleukin-1β in Post-Traumatic Stress Disorder: Evidence from Human and Animal Studies. J Interferon Cytokine Res. 2018;38(1):1–11. | ||
Eyre HA, Air T, Proctor S, Rositano S, Baune BT. A critical review of the efficacy of non-steroidal anti-inflammatory drugs in depression. Prog Neuropsychopharmacol Biol Psychiatry. 2015;57:11–16. | ||
Abbasi SH, Hosseini F, Modabbernia A, Ashrafi M, Akhondzadeh S. Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: randomized double-blind placebo-controlled study. J Affect Disord. 2012;141(2–3):308–314. | ||
Warner-Schmidt JL, Vanover KE, Chen EY, Marshall JJ, Greengard P. Antidepressant effects of selective serotonin reuptake inhibitors (SSRIs) are attenuated by antiinflammatory drugs in mice and humans. Proc Natl Acad Sci U S A. 2011;108(22):9262–9267. | ||
Toft H, Neupane SP, Bramness JG, Tilden T, Wampold BE, Lien L. The effect of trauma and alcohol on the relationship between level of cytokines and depression among patients entering psychiatric treatment. BMC Psychiatry. 2018;18(1):95. | ||
Sheehan DV, Lecrubier Y, Sheehan KH. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):34–57. | ||
Derogatis L, Lipman R, Covi L. SCL-90. Psychopharmacol Bull. 1973;9:13–28. | ||
Bech P, Bille J, Møller SB, Hellström LC, Østergaard SD. Psychometric validation of the Hopkins Symptom Checklist (SCL-90) subscales for depression, anxiety, and interpersonal sensitivity. J Affect Disord. 2014;160:98–103. | ||
Pedersen G, Karterud S. Is SCL-90R helpful for the clinician in assessing DSM-IV symptom disorders? Acta Psychiatr Scand. 2004;110(3):215–224. | ||
Rabe-Hesketh S, Skrondal A. Multilevel and Longitudinal Modeling Using Stata, Volume I: Continuous Responses. Vol 25. 2016. Stata Press. Texas, USA. | ||
Little RJA. A test of Missing Completely at Random for Multivariate Data with Missing Values. J Am Stat Assoc. 1988;83(404):1198–1202. | ||
Jergović M, Bendelja K, Savić Mlakar A, et al. Circulating levels of hormones, lipids, and immune mediators in post-traumatic stress disorder – a 3-month follow-up study. Front Psychiatry. 2015;14;6:49. | ||
Tucker P, Ruwe WD, Masters B, et al. Neuroimmune and cortisol changes in selective serotonin reuptake inhibitor and placebo treatment of chronic posttraumatic stress disorder. Biol Psychiatry. 2004;56(2):121–128. | ||
Himmerich H, Willmund GD, Zimmermann P, et al. Serum concentrations of TNF-α and its soluble receptors during psychotherapy in German soldiers suffering from combat-related PTSD. Psychiatr Danub. 2016;28(3):293–298. | ||
Gill J, Vythilingam M, Page GG. Low cortisol, high DHEA, and high levels of stimulated TNF-alpha, and IL-6 in women with PTSD. J Trauma Stress. 2008;21(6):530–539. | ||
Raison CL, Miller AH. When not enough is too much: the role of insufficient glucocorticoid signaling in the pathophysiology of stress-related disorders. Am J Psychiatry. 2003;160(9):1554–1565. | ||
Hussein S, Dalton B, Willmund GD, Ibrahim MAA, Himmerich H. A Systematic Review of Tumor Necrosis Factor-α in Post-Traumatic Stress Disorder: Evidence from Human and Animal Studies. Psychiatr Danub. 2017;29(4):407–420. | ||
von Känel R, Hepp U, Kraemer B, et al. Evidence for low-grade systemic proinflammatory activity in patients with posttraumatic stress disorder. J Psychiatr Res. 2007;41(9):744–752. | ||
Wang Z, Caughron B, Young MRI. Posttraumatic Stress Disorder: An Immunological Disorder? Front Psychiatry. 2017;8:222. | ||
Miller MW, Lin AP, Wolf EJ, Miller DR. Oxidative Stress, Inflammation, and Neuroprogression in Chronic PTSD. Harv Rev Psychiatry. 2018;26(2):57–69. | ||
Guo M, Liu T, Guo JC, Jiang XL, Chen F, Gao YS. Study on serum cytokine levels in posttraumatic stress disorder patients. Asian Pac J Trop Med. 2012;5(4):323–325. | ||
Gola H, Engler H, Sommershof A, et al. Posttraumatic stress disorder is associated with an enhanced spontaneous production of pro-inflammatory cytokines by peripheral blood mononuclear cells. BMC Psychiatry. 2013;13(1):1. | ||
Brunoni AR, Machado-Vieira R, Zarate CA, et al. Cytokines plasma levels during antidepressant treatment with sertraline and transcranial direct current stimulation (tDCS): results from a factorial, randomized, controlled trial. Psychopharmacology. 2014;231(7):1315–1323. | ||
Stein DJ, Ipser JC, Seedat S. Pharmacotherapy for post traumatic stress disorder (PTSD). Cochrane Database Syst Rev. 2006;1:Cd002795. | ||
Dixit VD, Yang H, Sayeed KS, et al. Controlled meal frequency without caloric restriction alters peripheral blood mononuclear cell cytokine production. J Inflamm. 2011;8(1):1. | ||
Pisetsky DS, Trace SE, Brownley KA, et al. The expression of cytokines and chemokines in the blood of patients with severe weight loss from anorexia nervosa: an exploratory study. Cytokine. 2014;69(1):110–115. | ||
Belchamber K, Hall DA, Hourani SM. Smoking enhances the proinflammatory effects of nucleotides on cytokine release from human lung. PLoS One. 2014;9(6):e99711. |
Supplementary materials
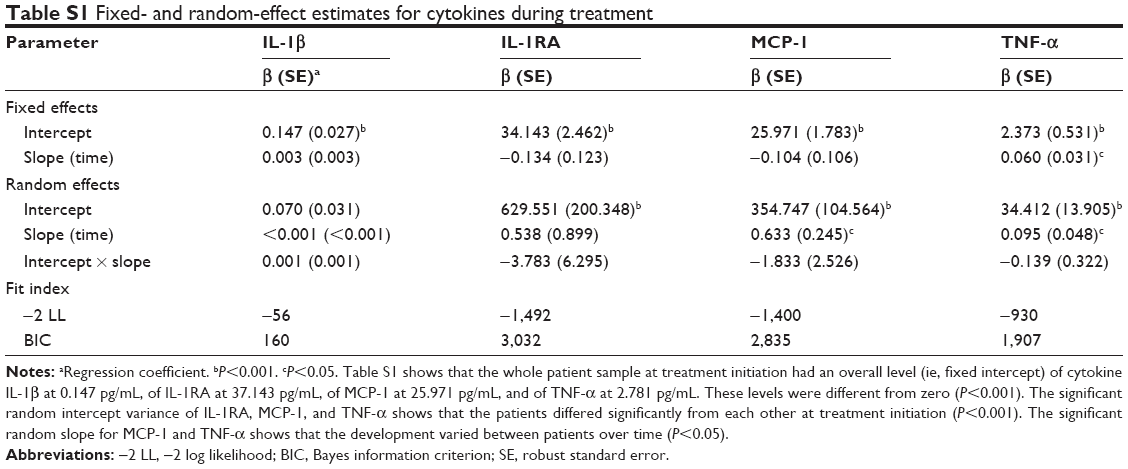 | Table S1 Fixed- and random-effect estimates for cytokines during treatment |
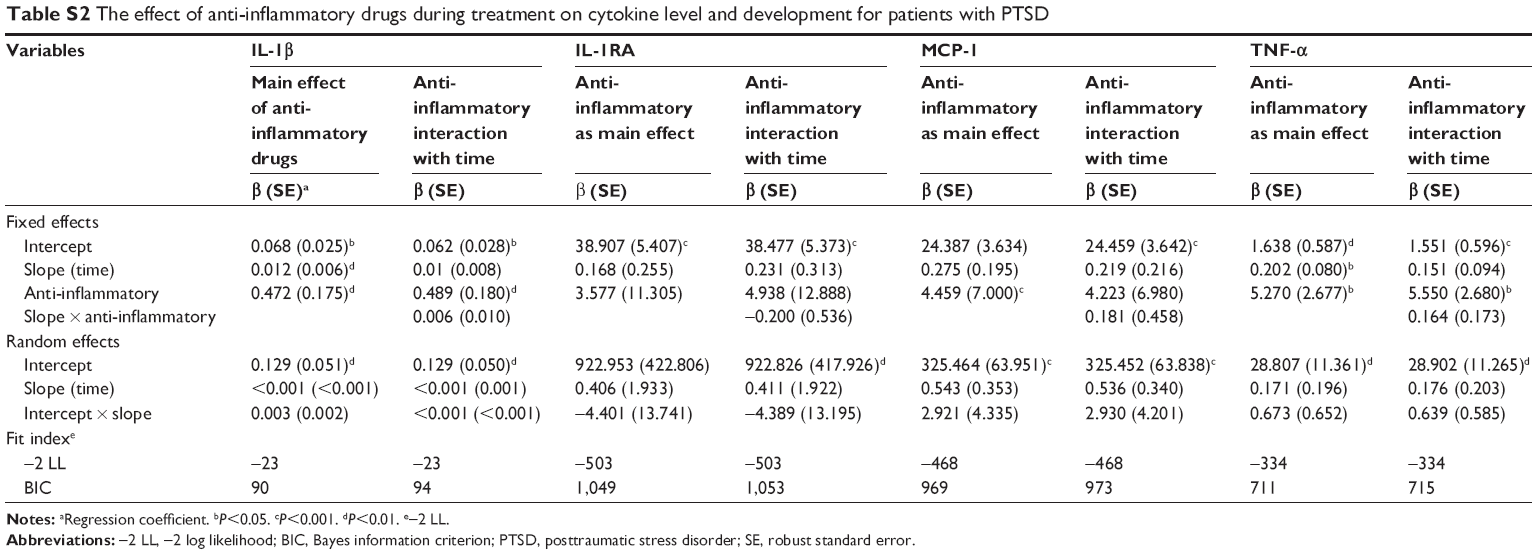 | Table S2 The effect of anti-inflammatory drugs during treatment on cytokine level and development for patients with PTSD |
 | Table S3 The effect of anti-inflammatory drugs during treatment on cytokine level and development for patients without PTSD |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.