Back to Journals » Psychology Research and Behavior Management » Volume 13
Psychometric Properties of the Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS) in the Iranian Older Adults
Authors Mavali S, Mahmoodi H ![]() , Sarbakhsh P
, Sarbakhsh P ![]() , Shaghaghi A
, Shaghaghi A ![]()
Received 4 April 2020
Accepted for publication 25 July 2020
Published 18 August 2020 Volume 2020:13 Pages 693—700
DOI https://doi.org/10.2147/PRBM.S256323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Einar Thorsteinsson
Sonia Mavali,1 Hassan Mahmoodi,2 Parvin Sarbakhsh,3 Abdolreza Shaghaghi1
1Department of Health Education and Promotion, Faculty of Health, Tabriz University of Medial Sciences, Tabriz, Iran; 2Social Determinants of Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, Sanandaj, Iran; 3Department of Biostatistics and Epidemiology, Faculty of Health, Tabriz University of Medial Sciences, Tabriz, Iran
Correspondence: Abdolreza Shaghaghi
Department of Health Education and Promotion, Faculty of Health, Tabriz University of Medial Sciences, Tabriz 51666614711, Iran
Tel +009 411 333622
Email [email protected]
Purpose: Mental wellbeing is considered as an important and effective factor in older adults’ psychological health. Due to lack of a standard instrument for the assessment of mental wellbeing in Iranian older adults, the present study was performed to examine validity and reliability of the Persian version of the Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS-P) for use among Iranian older adults.
Patients and Methods: The study sample included 304 older adults aged 60 and over, admitted to the Shohada Educational Hospital affiliated to the Tabriz University of Medical Sciences, North West of Iran. The participants were recruited through the convenience sampling method in May to September 2017.
Results: The mean and standard deviation of the mental wellbeing score were 50.30 and 8.82, respectively. Exploratory factor analysis (EFA) results demonstrated a one-factor solution with 13 items which was verified by the confirmatory factor analysis (CFA). The estimated internal consistency measure of Cronbach’s alpha (0.93) and two weeks’ time test-retest reliability index (0.84) met the prerequisite criteria.
Conclusion: According to the results, the WEMWBS-P with 13 items has acceptable validity and reliability to assess the mental wellbeing of Iranian and other Persian-speaking older adults.
Keywords: older adults, Iran, mental wellbeing
Introduction
Mental wellbeing has been referred to experience of happiness1 in the literature and as a single construct which could embody a person’s personality structure. Having a positive approach toward life events and a balanced positive and negative emotional state2 can be regarded as an important factor in older adults’ mental health.3,4 Mental wellbeing has been reported to be associated with lower risk of premature mortality, lower risk of physical disorders, better mental health, and lower use of healthcare services.5,6 Mental wellbeing has also been suggested to be an important factor in mental health and fruitful interpersonal relationships.7
Age-related changes that affect older adults’ health and functioning can negatively influence their mental wellbeing.8 More than 20% of people aged 55 years and over have reported having a kind of mental health problem.9 Different factors, such as loneliness and social isolation, social limitations, self-determination and feelings of insecurity can influence older adults’ mental wellbeing.10 While reduced mental wellbeing in older adults due to their age-related physical and mental capacities’ deterioration should be considered as natural and inevitable phenomena, it is necessary to increase the public’s attention toward the mental wellbeing and possible deviances in mental health during old age.11
Impairments in mental wellbeing can reduce older adults’ ability to perform everyday tasks, reduce their independence, and affect their quality of life.12 Therefore, early diagnosis of this impairment can potentially reduce health care costs for families and communities and help in developing strategies to cope with this inevitable challenge.13
Various instruments have been developed to assess mental wellbeing, such as the 20-item Positive and Negative Affect Schedule (PANAS),14 the 5-item Satisfaction with Life Scale (SWLS),15 the 54-item Ryff’s Psychological Well-Being Scales (PWB),16 the 5-item Short Depression-Happiness Scale (SDHS)17 and the Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS).18
Among the invented instruments, the WEMWBS, due to its conciseness and simplicity, can be applied in research and practice settings to measure mental wellbeing and affective-emotional and cognitive aspects and psychological functioning through 14 items.
This study was conducted to translate and assess psychometric properties of the Persian translated version of the WEMWBS-P for use among Iranian and other Persian-speaking older adults.
Patients and Methods
The study participants were 300 patients admitted to the Shohada hospital affiliated to the Tabriz University of Medical Sciences, North West of Iran from May to September 2017. The sample size was selected according to the minimum sample size recommended for analysis of covariance (ANCOVA). The present study was approved by the Medical Ethics Board of Trustees (MEBoT) in the Tabriz University of Medical Sciences (approval number: 5/D/1030407-1395-12-11).
The conventional translation/back translation procedure was followed to translate the original English form of the WEMWBS into Persian by two independent proficient translators (Forward translation). The two translators reached consensus about mismatches in a face to face meeting. In the next step, the Persian translated questionnaire was translated back into English by two other translators with good knowledge of English and experience in translating texts from Persian to English (Backward translation). The back translated version was compared to the original scale at the next stage and any disagreement was resolved with consensus. The final Persian version of the WEMWBS was sent to a panel of experts including 10 psychologists and health care scholars for their opinions about the WEMWBS-P and to assess lucidity of the wordings and comprehensibility of the items. Slight modifications were made based on their feedback.
Inclusion and Exclusion Criteria
Based on the United Nations (UN) agreed cutoff point of 60 years to refer to the older population,19 those aged above 60 years and with the ability to understand and speak Persian were eligible to be included in the study. Older adults with cognitive impairments or other severely limiting complications with potential to curtail completion of the informed consent form were excluded from the study.
The Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS)
The WEMWBS was developed by Tennant et al in 2007.18 It has 14 items that are rated on a 5-point Likert-type scale ranging from 1 (Never) to 5 (Always). The highest and lowest scores on the scale are 14 and 70, respectively. The higher scores indicate better mental health. The WEMWBS only assesses the positive aspect of mental health and can be used for assessment of mental health on the society, group and individual levels. It has been translated into different languages for mental health screening.20–29 The existent research evidence has shown its applicability in different geographical and cultural groups.23 The performed factor analysis by Tennant et al suggested a one factor solution for the WEMWBS with the Cronbach’s alpha level of 0.89 and 0.91 among the students and general public respectively.18
Data Analysis
Exploratory factor analysis (EFA) was carried out to determine the unidimensionality of the constructs in the WEMWBS-P. The EFA was performed using the SPSS software, version 22. Principal Component Analysis (PCA) as the default extraction method and the Varimax Rotation to assess the underlying structure of the data were performed and decision was made based on eigenvalues < 1 and a scree plots showing the number of factors. Varimax rotation is the common orthogonal rotation used in factor analysis to associate each original item with one factor by splitting the items as much as possible into disjoint sets of factors. Thus, every extracted factor is represented with small number of variables and interpretation of the results will be simplified.30 The minimum factor loading for a variable or item was 0.4. The significance level was set at P<0.0.5 level. Ceiling and floor effects were examined based on percentage of scores at the boundaries of the scaling and considered to be a problem if more than 20% of the study attendees achieved either the best or worst possible score.31 The skewness and kurtosis of the scores’ distribution were also investigated to ensure that they were within acceptable limits (less than ±2) for analyses.32
Construct Validity
Based on the EFA results which were used to examine the factor structure a CFA was conducted to confirm the factors extracted from the EFA. The Chi-Squared test, Chi-Squared to df ratio (χ2/df), Comparative Fit Index (CFI), Root Mean Square Residual (RMR), Tucker Lewis Index (TLI) and Adjusted Goodness Of Fit index (AGFI) were used to assess the output model goodness of fit.
RMSA and RMR ≤ 0.08; CFI, GFI, and TLI > 0.9; and χ2/df < 5 were considered as acceptable ranges to indicate fitness of the model to the data.21
The reliability of the instrument was assessed using a two-week interval test-retest reliably assessment and its internal consistency was assessed using the Cronbach’s alpha coefficient.
Those older adults who had participated in the pilot study to determine test-retest coefficients were excluded from the main study. Participation in the study was completely voluntarily, and participants were reassured about confidentiality of their personal information. A written informed consent was obtained from the study participants and all the study procedures were conducted in accordance with the Declaration of Helsinki.
Results
The mean and standard deviation of participants’ age were 70.65 and 8.71, respectively. Among the study respondents 160 (52.6%) were women, 200 (65.8%) were married, and 187 (61.5%) were illiterate. The mean and standard deviation of mental wellbeing score were 50.30 and 8.82 respectively. There was a significant relationship between the mental wellbeing score and gender, education and marital status (Table 1).
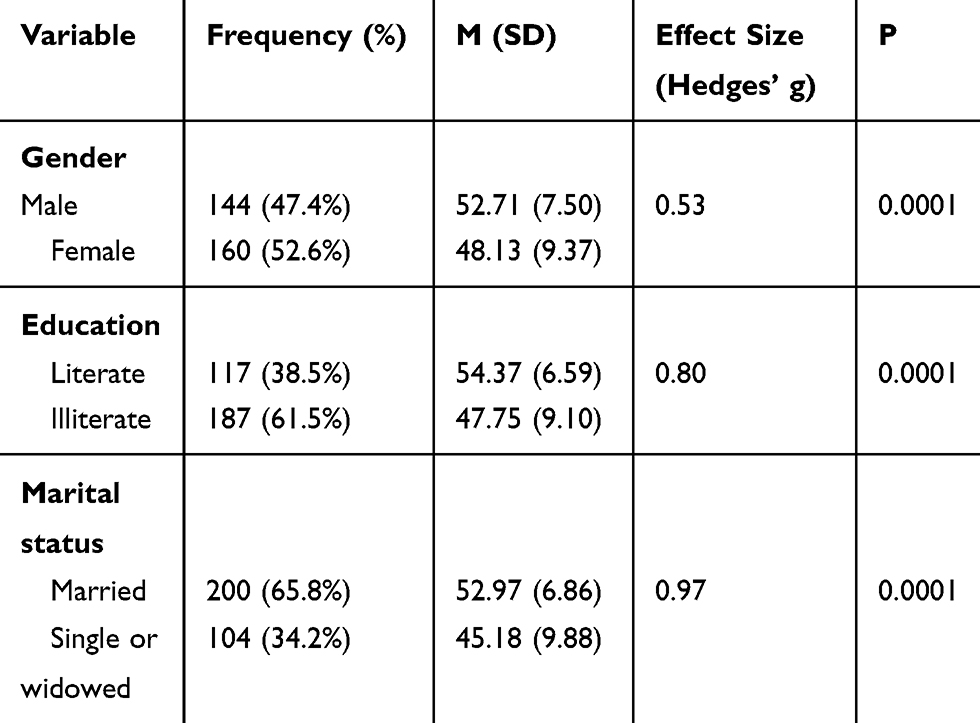 |
Table 1 Socio-Demographic Properties of the Study Participants and Their Association with the Total Mental Wellbeing Score |
Normality and Ceiling and Floor Effects
The mental wellbeing score had a normal distribution (skewness=−0.849, kurtosis=0.272) with a skewness to the right (Figure 1).
 |
Figure 1 Distribution of the studied Iranian older adults’ according to their WEMWBS-P scores. |
The ceiling effect was below 20% for the 14 items, except for items 8 (I have been feeling good about myself), 9 (I have been feeling close to other people), 10 (I have been feeling confident), and 12 (I have been feeling loved). The floor effect was also below 20% for the 14 items, except for item 4 (I have been feeling interested in other people) and for the total mental wellbeing score. All of the items of the WEMWBS-P were positively correlated with the total mental wellbeing score (Table 2).
 |
Table 2 Values of the Floor and Ceiling Effects, The Item-Total Correlations, and Factor Analysis Loadings in the Analysis of the Psychometric Properties of the Persian Version of Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS) |
Content Validity
The final, translated scale was sent to a panel of experts including 10 psychologists and health care scholars for their opinions about the WEMWBS-P. The Content Validity Index (CVI) for all the scale’s items was calculated based on a panel of experts’ ratings in terms of their relevance to the targeted construct. The Lawshe’s Content Validity Ratio (CVR) was also estimated to quantify content validity and corroborate congruence of the items with the intended construct.34 The analysis results revealed good content validity (CVR = 0.84, CVI = 0.85) of the WEMWBS-P.
Reliability of the Scale
The internal consistency of the WEMWBS-P was assessed using Cronbach’s alpha coefficient which was in the acceptable range (0.93).
Factor Structure
The factor analysis using the PCA method with 152 participants, revealed a KMO of 0.94, indicating that the data were appropriate for factor analysis. The Bartlett’s test of Sphericity which is the test for null hypothesis that the correlation matrix has an identity matrix also confirmed correlations between the variables and suitability of the EFA for data analysis (P<0.0001). According to the results of factor analysis (Table 2) and the scree plot (Figure 2), one factor was extracted that explained 60% of the variance of the total score. Item number 4 was eliminated due to having a factor loading below 0.2. Finally, the WEMWBS-P with one factor and 13 items was validated among the Iranian older adults. The total variance explained by the scale’s one factor was 53% and the Scree plot supported the unidimensionality of the WEMWBS-P questionnaire (Figure 2).
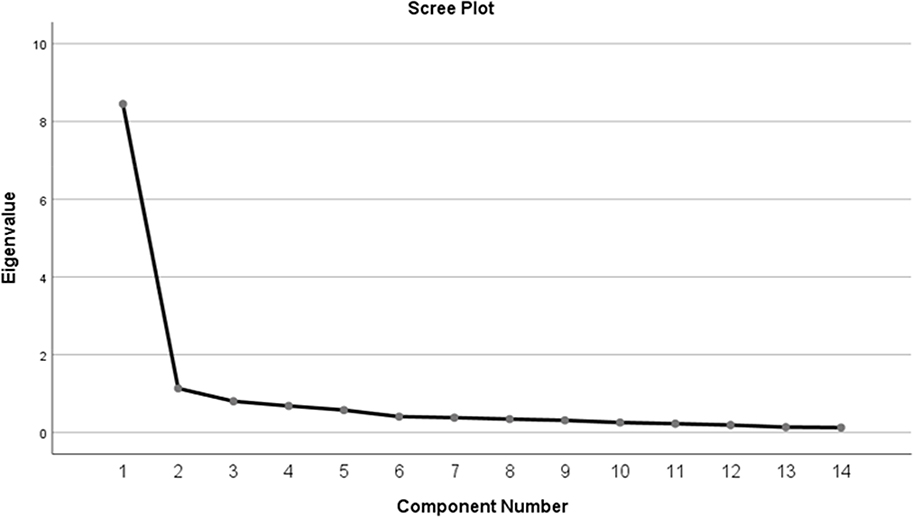 |
Figure 2 Scree plot representing the eigenvalues of the extracted variables obtained in the principal-component analysis for psychometric validation of the WEMWBS-P. |
Following the results obtained in the EFA, the CFA led to the flowing values: χ2/df = 2.10 (P<0.0001), CFI = 0.909, RMSEA = 0.084, TLI = 0.891, GFI = 0.872 and AGFI = 0.820 which are all confirmatory of the EFA outputs.
Discussion
Due to lack of a standard instrument for assessment of mental wellbeing in Iranian older adults, the present study was performed to examine validity and reliability of the Persian version of the Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS-P) for use among Iranian older adults. The results indicated that the WEMWBS-P with one factor and 13 items had acceptable validity and reliability to assess the mental wellbeing of Iranian older adults.18,25,26,35 This finding is consistent with the results of previous studies with different languages and in different populations, extracting one factor for the instrument. However, in contrary to the previous studies in which no item of the scale had been excluded, in the present study, item number 4 was eliminated due to an eigenvalue of below 0.2. This difference can be related to the cultural diversity of the population under study and the way the older adults perceived the item.
The WEMWBS-P indicated a high internal consistency. Consistent with this result, the reliability of the scale has been reported to be high in different populations.18,24,26 The data distribution had skewness to the left. Consistent with this finding, previous studies on the psychometric properties of the WEMWBS-P in different populations, including the general population, have indicated skewness to the left.24,26,27 However, in the Spanish and English speaking populations, the scores on the WEWBS had normal distribution. This difference between the findings can be due to differences in participants’ age and sample sizes. Therefore, it is recommended that the scale be studied in different populations using larger sample sizes.
Our findings showed that the ceiling effect for all the items, except items 6, 8, 9, 10, and 12, and the floor effect for all the items, except item 4 were below 20%. Previous studies conducted in other populations have also shown ceiling and floor effects in the items of this scale.26,35 This discrepancy in the findings can be related to different sample sizes. In other words, sample size in the study by Dong et al, with nurses, was smaller than that in our study, and sample sizes in the studies conducted in Spanish and English populations were larger than our sample.18,26,35
A Cronbach’s alpha coefficient of 0.93 and item-total correlations from 0.50 to 0.80 were found for the WEMWBS-P. In line with these results, previous studies have also found high Cronbach’s alphas for the WEMWBS-P.24,26,35 These results indicate that this scale has a high internal consistency.
According to the results, there was a significant gender difference in the mental wellbeing score. This finding is consistent with that of Santos et al.28 However, some previous studies have not found gender differences in mental wellbeing.18,24 This difference in the results can be due to differences in participants’ age, health status, and disorders and different cultural beliefs regarding mental wellbeing in different populations. In addition, our population included hospitalized older adults aged 60 and over; this can also explain some differences between our findings and those of previous studies.
According to the study results, the literate older adults had better mental wellbeing than illiterate older adults. In line with this finding, Ibitoye et al showed that highly educated older adults had a better mental wellbeing profile.35 A higher educational attainment appears to be an influential covariate of mental wellbeing in older adults however, in a number of other studies, significant difference was not observed in mental wellbeing between people with higher and lower educational qualifications.29 These contrasting findings may imply that education level alone is not a strong determinant of older adults’ mental wellbeing, and further research is required to verify complex interplay among the education level, other predictors and mental wellbeing in old age.
Another finding was that the married older adults had better mental wellbeing than those who were single or widowed. Consistent with this result, previous studies have shown that marital status could predict mental wellbeing, with married individuals scoring higher on mental wellbeing than single individuals.36,37 It appears that the presence of a supportive partner could have a benevolent impact on the mental wellbeing of married older adults. Old age is generally accompanied by certain stressors, such as being away from children, suffering from chronic disorders, reduced contact with peers, lower participation in the society and financial problems thence, presence of a partner could mitigate hurdles of facing these challenges.
Limitations
Interpretation of this study’s findings warrants further scrutiny due to the recruited sample attributes. Hospitalized older adults were approached in this research to collect data for psychometric appraisal of the WEMWBS-P. Therefore, probability of response bias as result of the interviewees’ health status and their subsequent imprecise responses to the study questions should not be dismissed completely. Bias due to the patients’ awkward perceptions about their overall health and illness or hospital experiences and in consequence, their tendency to inflate their responses to cast a more favorable or worse health status than the actual health condition could be another source of uncertainty in this study.38,39
Other factors such as anxiety, depression, and resilience, socio-demographic and psychosocial variables were also shown in previous studies40–42 to affect self-perceived burden of health conditions. Thus, reliable assessment of mental wellbeing warrants careful consideration in future studies.
Conclusion
The study findings revealed relatively robust validity and reliability properties for the WEMWBS-P to be applied in studies on assessment of Iranian and other Persian-speaking older adults’ mental wellbeing. Further cross-cultural, cross-linguistic and comparative multi-national studies are recommended to provide more cogent evidence for bridging the knowledge gap about feasibility and desirability of the WEMWBS-P application in diverse settings.
Acknowledgments
The authors wish to sincerely thank the older adults who patiently participated in this project. This work was supported by the Tabriz University of Medical Sciences under Grant 5/D/1046928- 1396-01-19.
Disclosure
The authors declare no conflicts of interest for this article.
References
1. Seligman MEP, Csikszentmihalyi M. Positive Psychology: An Introduction. In: Flow and the Foundations of Positive Psychology. Springer; 2014:279–298.
2. Walker SS, Schimmack U. Validity of a happiness implicit association test as a measure of subjective well-being. J Res Pers. 2008;42(2):490–497. doi:10.1016/j.jrp.2007.07.005
3. Vázquez C, Hervás G, Rahona JJ, Gómez D. Psychological well-being and health. Contributions of positive psychology. Annu Clin Heal Psychol. 2009;5:15–27.
4. Abdallah S, Mahony S, Marks N, et al. Measuring our progress: the power of well-being. London: New Economic Foundation. 2011.
5. Keyes CLM. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J Consult Clin Psychol. 2005;73(3):539. doi:10.1037/0022-006x.73.3.539
6. Nordentoft M. Prevention of suicide and attempted suicide in Denmark. Dan Med Bull. 2007;54(4):306–369.
7. Keyes CLM, Shmotkin D, Ryff CD. Optimizing well-being: the empirical encounter of two traditions. J Pers Soc Psychol. 2002;82(6):1007. doi:10.1037/0022-3514.82.6.1007
8. Snowden M, Dhingra SS, Keyes CLM, Anderson LA. Changes in mental well-being in the transition to late life: findings from MIDUS I and II. Am J Public Health. 2010;100(12):2385–2388. doi:10.2105/ajph.2010.193391
9. Ritchie K, Artero S, Beluche I, et al. Prevalence of DSM-IV psychiatric disorder in the French elderly population. Br J Psychiatry. 2004;184(2):147–152. doi:10.1192/bjp.184.2.147
10. Moyle W, Clarke C, Gracia N, et al. Older people maintaining mental health well‐being through resilience: an appreciative inquiry study in four countries. J Nurs Healthc Chronic Illn. 2010;2(2):113–121. doi:10.1111/j.1752-9824.2010.01050.x
11. Health NI for, Excellence C. Occupational Therapy Interventions and Physical Activity Interventions to Promote the Mental Wellbeing of Older People in Primary Care and Residential Care. NICE; 2008.
12. de Mendonça Lima CA, Ivbijaro G. Mental health and wellbeing of older people: opportunities and challenges. Ment Health Fam Med. 2013;10(3):125.
13. World Health Organization. Good Health Adds Life to Years: Global Brief for World Health Day 2012; 2012.
14. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063. doi:10.1037/0022-3514.54.6.1063
15. Diener ED, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49(1):71–75. doi:10.1207/s15327752jpa4901_13
16. Ryff CD, Keyes CLM. The structure of psychological well-being revisited. J Pers Soc Psychol. 1995;69(4):719. doi:10.1037/0022-3514.69.4.719
17. Joseph S, Linley PA, Harwood J, Lewis CA, McCollam P. Rapid assessment of well‐being: the Short Depression‐Happiness Scale (SDHS). Psychol Psychother Theory, Res Pract. 2004;77(4):463–478. doi:10.1348/1476083042555406
18. Tennant R, Hiller L, Fishwick R, et al. The Warwick-Edinburgh mental well-being scale (WEMWBS): development and UK validation. Health Qual Life Outcomes. 2007;5(1):63. doi:10.1186/1477-7525-5-63
19. United Nations. 2017. Department of Economic and Social Affairs, Population Division (2017). World Population Ageing 2017 - Highlights (ST/ESA/SER.A/397).
20. Stewart-Brown S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): performance in different cultural and geographical groups. In: Mental Well-Being. Springer; 2013:133–150.
21. Stewart-Brown S, Tennant A, Tennant R, Platt S, Parkinson J, Weich S. Internal construct validity of the Warwick-Edinburgh mental well-being scale (WEMWBS): a Rasch analysis using data from the Scottish health education population survey. Health Qual Life Outcomes. 2009;7(1):15. doi:10.1186/1477-7525-7-15
22. López MA, Gabilondo A, Codony M, et al. Adaptation into Spanish of the Warwick–Edinburgh Mental Well-being Scale (WEMWBS) and preliminary validation in a student sample. Qual Life Res. 2013;22(5):1099–1104. doi:10.1007/s11136-012-0238-z
23. Castellví P, Forero CG, Codony M, et al. The Spanish version of the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) is valid for use in the general population. Qual Life Res. 2014;23(3):857–868. doi:10.1007/s11136-013-0513-7
24. Lloyd K, Devine P. Psychometric properties of the warwick–edinburgh mental well-being scale (WEMWBS) in Northern Ireland. J Ment Heal. 2012;21(3):257–263. doi:10.3109/09638237.2012.670883
25. McDonald RP, Ho M-HR. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7(1):64. doi:10.1037/1082-989x.7.1.64
26. Dong A, Chen X, Zhu L, et al. Translation and validation of a Chinese version of the warwick–edinburgh mental well‐being scale with undergraduate nursing trainees. J Psychiatr Ment Health Nurs. 2016;23(9–10):554–560. doi:10.1111/jpm.12344
27. Bartram DJ, Yadegarfar G, Sinclair JMA, Baldwin DS. Validation of the Warwick–Edinburgh Mental Well-being Scale (WEMWBS) as an overall indicator of population mental health and well-being in the UK veterinary profession. Vet J. 2011;187(3):397–398. doi:10.1016/j.tvjl.2010.02.010
28. Kim S, Jung H-Y, Na K-S, et al. A validation study of the Korean version of warwick-edinburgh mental well-being scale. J Korean Neuropsychiatr Assoc. 2014;53(4):237–245. doi:10.4306/jknpa.2014.53.4.237
29. Santos JJA, Costa TA, Guilherme JH, et al. Adaptation and cross-cultural validation of the Brazilian version of the Warwick-Edinburgh mental well-being scale. Rev Assoc Med Bras. 2015;61(3):209–214. doi:10.1590/1806-9282.61.03.209
30. Abdi H. Factor rotations in factor analyses. In Lewis-Beck M, Bryman A, Futing T, editors. Encyclopedia of Social Science Research Methods. 2004. Thousand Oaks (CA): Sage; 978–982.
31. Tabachnick BG, Fidell LS, Ullman JB. Using Multivariate Statistics. Boston: Pearson; 2019.
32. McHorney CA, Tarlov AR. Individual-patient monitoring in clinical practice: are available health status surveys adequate? Qual Life Res. 1995;4:293–307. doi:10.1007/BF01593882
33. Warwick Medical School. Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS). Available from: https://warwick.ac.uk/fac/sci/med/research/platform/wemwbs/. Accessed August 5, 2020.
34. Lawshe CH. A quantitative approach to content validity 1. Pers Psychol. 1975;28(4):563–575. doi:10.1111/j.1744-6570.1975.tb01393.x
35. Ibitoye OG, Sanuade OA, Adebowale AS, Ayeni O. Psychological well-being of the Elderly in Nigeria. Niger J Sociol Anthropol. 2014;12:1.
36. Trousselard M, Steiler D, Dutheil F, et al. Validation of the Warwick-Edinburgh mental well-being scale (WEMWBS) in French psychiatric and general populations. Psychiatry Res. 2016;245:282–290. doi:10.1016/j.psychres.2016.08.050
37. Vaingankar JA, Abdin E, Chong SA, et al. Psychometric properties of the short Warwick Edinburgh mental well-being scale (SWEMWBS) in service users with schizophrenia, depression and anxiety spectrum disorders. Health Qual Life Outcomes. 2017;15(1):153. doi:10.1186/s12955-017-0728-3
38. Knowles S, Swan L, Salzberg M, Castle D, Langham R. Exploring the relationships between health status, illness perceptions, coping strategies and psychological morbidity in a chronic kidney disease cohort. Am J Med Sci. 2014;348(4):271–276. doi:10.1097/MAJ.0000000000000242
39. Plys E, Desrichard O. Associations between positive and negative affect and the way people perceive their health goals. Front Psychol. 2020;11:334. doi:10.3389/fpsyg.2020.00334
40. Lee BJ, Lamichhane DK, Jung DY, Moon SH, Kim SJ, Kim HC. Psychosocial factors and psychological well-being: a study from a nationally representative sample of Korean workers. Ind Health. 2016;54(3):237–245. doi:10.2486/indhealth.2015-0191
41. Oskrochi G, Bani-Mustafa A, Oskrochi Y. Factors affecting psychological well-being: evidence from two nationally representative surveys. PLoS One. 2018;13(6):e0198638. doi:10.1371/journal.pone.0198638
42. Cho J, Martin P, Margrett J, MacDonald M, Poon LW. The relationship between physical health and psychological well-being among oldest-old adults. J Aging Res. 2011;2011:605041. doi:10.4061/2011/605041
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.