Back to Journals » Substance Abuse and Rehabilitation » Volume 16
Psychometric Properties of the Arabic Version of the Addiction Severity Index (ASI-5): A Cross-Cultural Validation Study in Egypt and Saudi Arabia
Authors Abouzed M ![]() , Aljadani A, Gabr A, Elsheikh M, Almuqahwi MS, Alrashidy MF, Alrashidi GK, Soliman MF, Altamimi AN, Alenze NS, Elsaadouni N
, Aljadani A, Gabr A, Elsheikh M, Almuqahwi MS, Alrashidy MF, Alrashidi GK, Soliman MF, Altamimi AN, Alenze NS, Elsaadouni N
Received 13 February 2025
Accepted for publication 7 May 2025
Published 10 May 2025 Volume 2025:16 Pages 129—136
DOI https://doi.org/10.2147/SAR.S519241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra Badgaiyan
Mohamed Abouzed,1 Ahmed Aljadani,2 Amgad Gabr,1 Mohamed Elsheikh,1 Mohamed Saad Almuqahwi,3 Mohamed Fayed Alrashidy,4 Ghali Khalaf Alrashidi,4 Mahmoud Farag Soliman,5 Amal Nasser Altamimi,4 Nida Saleh Alenze,4 Nisrin Elsaadouni6
1Psychiatry Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 2College of Medicine, University of Ha’il, Ha’il, Saudi Arabia; 3Erada Mental Hospital, Dammam, Saudi Arabia; 4Erada Mental Hospital, Ha’il, Saudi Arabia; 5Psychiatry Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 6Psychiatry Department, Faculty of Medicine, Mansoura University, Mansoura, Egypt
Correspondence: Mohamed Abouzed, Psychiatry Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt, Email [email protected]
Background: The Addiction Severity Index (ASI) is a globally recognized tool for assessing substance use disorder (SUD) severity. Despite its widespread use, no validated Arabic version exists. This study aimed to validate the Arabic ASI-5 in Egypt and Saudi Arabia and evaluate its psychometric properties.
Methods: : A cross-sectional study recruited 400 participants (200 per country) from inpatient/outpatient SUD treatment centers. The ASI-5 underwent forward-backward translation, pilot testing, and cultural adaptation. Internal consistency (Cronbach’s α), test-retest reliability (Spearman’s ρ), and inter-observer reliability were assessed. Convergent and discriminant validity were evaluated using adjusted Spearman’s correlations.
Results: The Arabic ASI-5 demonstrated acceptable internal consistency (α = 0.61– 0.82), with medical (α = 0.78) and psychiatric (α = 0.82) domains showing the highest reliability. Lower consistency in drug (α = 0.62) and legal (α = 0.61) domains reflected cultural and methodological factors. Test-retest (ρ = 0.55– 0.98) and inter-observer reliability (ρ = 0.78– 0.99) were strong. Convergent validity was robust for medical and psychiatric domains (r = 0.70– 0.85).
Conclusion: The Arabic ASI-5 is a reliable tool for assessing SUD severity in Arabic-speaking populations. Further refinement of drug and legal domains is recommended to enhance cultural relevance.
Keywords: addiction severity index, substance use disorder, cross-cultural validation, psychometrics
Introduction
The Addiction Severity Index (ASI)1 is widely recognized as one of the most frequently utilized assessment tools in the field of substance abuse. Initially developed in 1980,1 the ASI has undergone revisions, with the most recent version being the ASI-6.2 While the ASI-6 has been developed, the ASI-5 remains widely used due to its compatibility with existing translations and study designs.3 This version evaluates the impact of substance use across seven key life domains: medical status, employment, alcohol use, drug use, legal status, family/social relationships, and psychiatric status.4 When alcohol and drug use are combined, the assessment covers six domains. The ASI measures the severity of substance use over the past 30 days as well as across the individual’s lifetime. Each domain generates a composite score (CS) that reflects the individual’s current level of functioning, primarily for research purposes.1
The original English version of the ASI has demonstrated strong reliability and validity among individuals with substance use disorders.1–5 Initial validation studies were conducted on large patient samples. For example, McLellan et al1 reported favorable results in a study involving 524 male veterans with alcohol and drug dependence. Another study by the same authors reinforced these findings using a sample of 181 patients from three different alcohol and drug treatment centers.6 The ASI has also shown good inter-observer and test-retest reliability, as well as strong convergent and discriminant validity.1 Hendricks et al7 further confirmed the instrument’s validity, reporting Cronbach’s α values above 0.70 for all composite scores, except in the employment domain.
The ASI’s utility extends globally, with validated translations available in several countries, including China,8 Japan,9 Turkey,10 France,11 and the Netherlands.7 This widespread use underscores its effectiveness as an assessment tool for informing treatment and rehabilitation plans.
Substance use disorders are a growing concern in Egypt and Saudi Arabia, with significant public health implications. The prevalence of drug use in Saudi Arabia is estimated at 7–8%,12 posing a significant public health challenge. The most commonly abused drugs are amphetamines, heroin, alcohol, and cannabis, with a high incidence of poly-substance abuse. The young adult population (ages 12–22) is disproportionately affected, comprising 70% of all PWUDs.13 In Egypt, a national survey of 106,480 individuals aged 20–45 from various regions revealed a 13.3% lifetime prevalence of substance use.14
This study focuses on validating the Arabic version of the ASI-5 to address gaps in culturally appropriate assessment tools.
Aim: To evaluate the psychometric properties of the Arabic ASI-5 in Arabic-speaking populations.
Methods
Study Design and Participants
A cross-sectional study recruited 400 participants (200 each from Egypt and Saudi Arabia) meeting DSM-5 criteria for substance use disorder (SUD). Inclusion criteria included fluency in Arabic, age ≥18 years, and primary use of amphetamines, cannabis, alcohol or benzodiazepines. Exclusion criteria included acute intoxication or severe cognitive impairment.
Instrument Adaptation
The ASI-5 underwent forward-backward translation by bilingual experts. Discrepancies were resolved through consensus. Pilot testing with 20 participants (10 per country) identified ambiguities in legal terminology (eg, “illegal activities”), which were refined by a panel of clinicians and linguists.
Participants
Inclusion and Exclusion Criteria
Participants were included in the study if they met the diagnostic criteria for substance dependence as defined by the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5),15 primarily used amphetamines, cannabis, or benzodiazepines (either alone or in combination with other substances), demonstrated fluency in Arabic to ensure accurate comprehension of the Addiction Severity Index (ASI) items, and were aged 18 years or older.
Participants were excluded if they exhibited severe cognitive or psychiatric impairments that could compromise their ability to provide reliable responses, were acutely intoxicated at the time of the interview, or were unable to provide informed consent due to severe mental or physical conditions.
Sample Size
A total of 400 participants were recruited, with 200 participants from Egypt and 200 participants from Saudi Arabia. The sample size was determined based on previous validation studies of the ASI in other languages, which typically included 200–500 participants to ensure robust statistical analyses.
Instrument
Addiction Severity Index (ASI)
The 5th edition of the ASI was used as the primary instrument. The ASI is a semi-structured interview designed to assess the severity of substance abuse and the need for treatment across seven domains:
Medical, Employment, Alcohol, Drugs, Legal, Family/Social and Psychiatric.
Each domain provides a Composite Score (CS) that reflects the severity of problems in that area. The CSs range from 0 to 1, with higher scores indicating greater severity.
Arabic Adaptation
The ASI was translated into Arabic using a forward-backward translation process:
Forward Translation: The original English version of the ASI was translated into Arabic by two independent bilingual experts.
Backward Translation: The Arabic version was translated back into English by two other bilingual experts to ensure accuracy and consistency.
Pilot Testing: The Arabic ASI was pilot-tested with 20 participants to identify any linguistic or cultural issues. Feedback was used to refine the final version.
Procedures
Trained research assistants conducted face-to-face interviews (45–60 minutes). Test-retest reliability was assessed in 100 participants (50 per country) over a 7–14-day interval. Inter-observer reliability involved dual independent scoring of 50 videotaped interviews.
Data Analysis
Descriptive Statistics
Means, standard deviations, and percentages were calculated for all items and composite scores (CSs) to describe the sample characteristics and substance use patterns.
Internal Consistency
Internal consistency was evaluated using Cronbach’s α (threshold: ≥0.65). Spearman correlations, adjusted for Type I error via Bonferroni correction, assessed validity and reliability. Analyses were performed using SPSS v26 and R v4.0. A significant level of p < 0.05 was used for all statistical tests.
Ethical Considerations
The study was approved by the Ethics Committees of the participating institutions in Egypt and Saudi Arabia. Written informed consent was obtained from all participants, and confidentiality was maintained throughout the study. Participants were informed that their participation was voluntary and that they could withdraw at any time without affecting their treatment.
Results
Participant Characteristics
Participants were predominantly male (65%), unemployed (75%), with a mean age of 31.8 years (SD = 7.5). Polysubstance use was reported by 85%, primarily involving amphetamines (75%), cannabis (70%), and benzodiazepines (55%).
Internal Consistency
Cronbach’s α ranged from 0.61 (legal) to 0.82 (psychiatric). Lower consistency in drug (α = 0.62) and legal (α = 0.61) domains was attributed to cultural stigma and heterogeneous substance use patterns (Table 1).
 |
Table 1 Internal Consistency and Validity of ASI-5 Domains |
Reliability
Test-retest reliability was strong (ρ = 0.55–0.98), while inter-observer reliability ranged from 0.78 (medical) to 0.99 (alcohol) (Table 2).
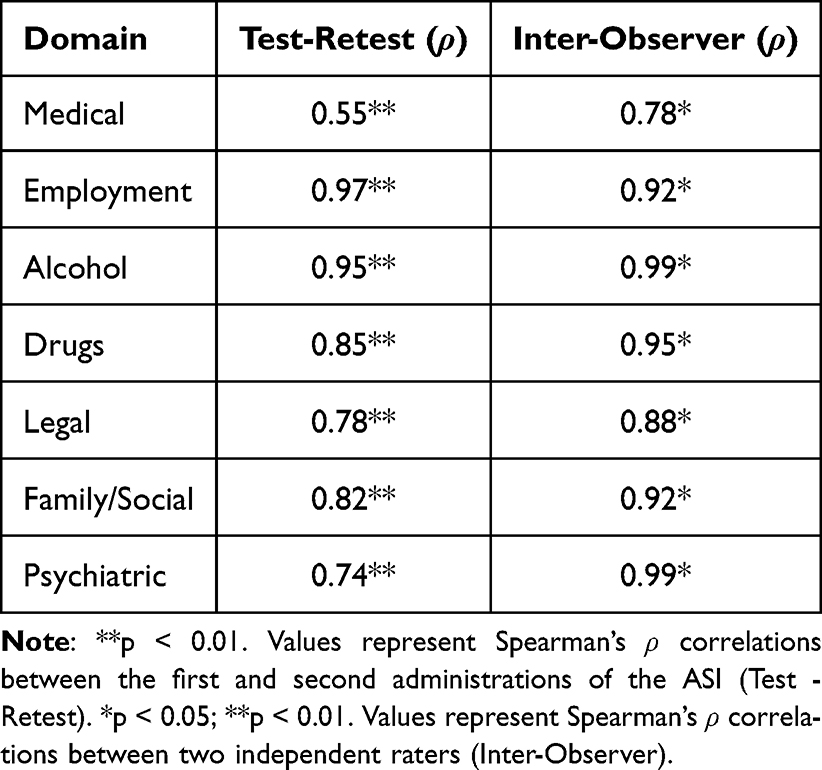 |
Table 2 Reliability Analysis |
Validity
Convergent validity was highest in medical (r = 0.70–0.85) and psychiatric (r = 0.10–0.85) domains. Discriminant validity confirmed domain independence (r < 0.40), except for a moderate psychiatric-family/social correlation (r = 0.39, p < 0.01) (Table 2).
Discussion
Summary of Key Findings
This study validated the Arabic version of the 5th edition of the Addiction Severity Index (ASI) in a sample of 400 patients with multiple substance dependence from Egypt and Saudi Arabia. The results demonstrated that the Arabic ASI has good internal consistency, acceptable convergent and discriminant validity, and high test-retest and inter-observer reliability. The findings are consistent with previous validation studies of the ASI in other languages and cultural contexts, supporting its use as a reliable and valid tool for assessing substance abuse severity in Arabic-speaking populations.
The internal consistency of the Arabic ASI, as measured by Cronbach’s α, was moderate to excellent across most domains. The medical (α = 0.78) and psychiatric (α = 0.82) domains showed the highest internal consistency, which is consistent with previous validation studies.6,7 However, the drug (α = 0.62) and legal (α = 0.61) domains had lower internal consistency, which may be attributed to the heterogeneity of substance use patterns and legal issues in the sample.
The lower internal consistency in the drug domain may reflect the diverse patterns of substance use in the Middle East, where polydrug use (eg, combining amphetamines, cannabis, and benzodiazepines) is common. This finding aligns with previous studies that have reported challenges in achieving high internal consistency for the drug domain due to the complexity of polydrug use.16
The legal domain’s lower internal consistency may be due to cultural differences in the interpretation of Engaged in substance-related illegal activities (eg, possession, trafficking), such as the severity of legal problems or the willingness to disclose illegal activities. This finding is consistent with studies that have reported similar challenges in other non-Western populations.5
The Arabic ASI demonstrated acceptable convergent and discriminant validity, supporting its ability to measure distinct constructs across the seven domains. The moderate correlation between the psychiatric and family/social domains (r = 0.39, p < 0.01) suggests some overlap, which is consistent with previous studies that have found similar correlations.3 This overlap may reflect the interconnected nature of psychiatric and family/social problems in individuals with substance dependence.
The strong item-scale correlations within the medical and psychiatric domains support the convergent validity of the Arabic ASI. However, the weaker correlations in the drug and legal domains highlight the need for further refinement of these sections to better capture the complexity of substance use and legal issues in Arabic-speaking populations.
The low correlations between items in one domain and the composite scores of other domains support the discriminant validity of the Arabic ASI, indicating that each domain measures distinct aspects of substance abuse severity.
The Arabic ASI demonstrated high test-retest and inter-observer reliability, indicating that it produces consistent results over time and across different raters. The test-retest correlations ranged from 0.55 to 0.98, and the inter-observer correlations ranged from 0.78 to 0.99, which are consistent with data reported in studies from the United States, the Netherlands, China, Switzerland, and Japan.8–10,17,18 However, the alpha values for the medical and occupational domains were below the threshold of 0.7. Specifically, the medical domain yielded an alpha value of 0.581, which may be attributed to the way hospitalization data was collected—focusing on the frequency of hospital visits rather than the total number of days spent in the hospital.
The high test-retest reliability suggests that the Arabic ASI is stable over time, even in a population experiencing significant life changes due to substance dependence and treatment. However, the lower test-retest correlation for the medical domain (ρ = 0.55) may reflect the impact of withdrawal symptoms or acute medical conditions on participants’ responses.
The high inter-observer reliability indicates that the Arabic ASI can be administered consistently by different raters, which is critical for its use in clinical and research settings.
The findings of this study are consistent with previous validation studies of the ASI in other languages and cultural contexts. For example:
The Cronbach’s α values for the Arabic ASI are comparable to those reported in the Dutch,17 Spanish,19 and French20 versions of the ASI.
The test-retest and inter-observer reliability coefficients for the Arabic ASI are similar to or higher than those reported in previous studies.4,5 The lower internal consistency observed in the drug and legal domains of the Arabic version of the ASI-5 may be attributed to several cultural, methodological, and contextual factors. In the drug domain, the heterogeneity of substance use patterns, such as the prevalence of polydrug use (eg, combining amphetamines, cannabis, and benzodiazepines) and the absence of culturally specific substances like khat, may contribute to variability in responses. Additionally, the stigma surrounding substance use in Arabic-speaking cultures may lead to underreporting or inconsistent reporting of drug use behaviors. In the legal domain, participants’ reluctance to disclose illegal activities due to fear of legal repercussions or social judgment, combined with differences in legal systems and the complexity of legal items, may result in inconsistent responses. Furthermore, ambiguity in item wording and potential translation issues could lead to misinterpretation, while self-report bias and small sample sizes for specific subdomains may also affect internal consistency.
To address these issues, modifications such as refining item wording to ensure cultural relevance, incorporating questions on polydrug use and culturally specific substances, reducing stigma through neutral language, and supplementing self-reports with objective measures (eg, biological markers) could improve the reliability of these domains. Additionally, expanding the legal domain to include culturally relevant legal concepts and increasing the sample size for subdomains may enhance internal consistency. These adjustments would strengthen the Arabic ASI-5 as a tool for assessing substance abuse severity in Arabic-speaking populations.
Limitations
Despite its strengths, this study has several limitations:
Sample Characteristics: The sample was limited to patients from Egypt and Saudi Arabia, which may limit the generalizability of the findings to other Arabic-speaking countries or populations with different substance use patterns.
Self-Report Bias: The reliance on self-reported data may introduce bias, particularly in domains such as legal and drug use, where participants may underreport or overreport their behaviors.
Cultural Differences: The ASI was originally developed in a Western context, and some items may not fully capture the cultural and contextual factors that influence substance use and related problems in the Middle East.
Small Subgroup Analyses: The sample size for test-retest and inter-observer reliability analyses was relatively small, which may limit the robustness of these findings.
Implications for Clinical Practice and Research
The Arabic version of the ASI is a valuable tool for assessing substance abuse severity and treatment needs in Arabic-speaking populations. Its strong psychometric properties make it suitable for use in both clinical and research settings. However, further refinement of the drug and legal domains may be needed to improve their internal consistency and validity.
Clinical Practice: The Arabic ASI can be used to guide treatment planning and monitor progress in patients with multiple substance dependence. It can also help clinicians identify areas of need, such as psychiatric or family/social problems, that may require additional intervention.
Research: The Arabic ASI can be used to conduct cross-cultural comparisons of substance abuse severity and treatment outcomes. It can also be used to evaluate the effectiveness of substance abuse interventions in Arabic-speaking populations.
Future Directions
Future Research Should Focus on
Refining the Drug and Legal Domains: Additional items or modifications to existing items may be needed to better capture the complexity of substance use and legal issues in Arabic-speaking populations.
Validating the ASI in Other Arabic-Speaking Countries: Future studies should validate the Arabic ASI in other Arabic-speaking countries to ensure its applicability across different cultural contexts.
Exploring Cultural Adaptations: Further research is needed to explore how cultural factors, such as stigma or family dynamics, influence the interpretation and reporting of ASI items in Arabic-speaking populations.
Conclusion
The Arabic ASI-5 fills a critical gap in SUD assessment for Arabic-speaking populations. While it is reliable for clinical use, refining drug and legal domains with culturally specific items (eg, khat use, legal system nuances) is recommended. Future studies should explore ASI-6 adaptations and validate the tool in broader Arabic-speaking regions.
Data Sharing Statement
Access to data is restricted by third-party privacy or ethical considerations. Information can be provided upon request with proper justification.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the authors used Quillbot in order to improve readability and language of the work. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Institutional Review Board Statement
Research was conducted in compliance with the Nuremberg Code and Declaration of Helsinki, having received authorization from Al-Azhar University.
The use of the collected data for research purposes was approved by the Ethics Committee of the Security Sciences Institute of Hail Cluster Review Board (IRB) 2025-42.
Funding
No external funding was obtained for this study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. McLellan AT, Luborsky L, Woody MD, O’Brien C. An improved diagnostic evaluation instrument for substance abuse patients. J Nerv Ment Dis. 1980;168:26–33. doi:10.1097/00005053-198001000-00006
2. Cacciola JS, Alterman AI, Habing B, McLellan AT. Recent status scores for version 6 of the Addiction Severity Index (ASI-6). Addiction. 2011;106(9):1588–1602. doi:10.1111/j.1360-0443.2011.03482.x
3. Denis CM, Cacciola JS, Alterman AI. Addiction Severity Index (ASI) summary scores: comparison of the recent status scores of the ASI–6 and the composite scores of the ASI–5. J Subst Abuse Treat. 2013;45(5):444–450. doi:10.1016/j.jsat.2013.06.003
4. McLellan AT, Kushner H, Metzger D, et al. The fifth edition of the addiction severity index. J Subst Abuse Treat. 1992;9:199–213. doi:10.1016/0740-5472(92)90062-S
5. Hodgins D, El-Guebaly MD, EL-GUEBALY N. More data on the addiction severity index reliability and validity with the mentally ill substance abuser. J Nerv Ment Dis. 1992;180:197–201. doi:10.1097/00005053-199203000-00009
6. McLellan AT, Luborsky L, Cacciola J, et al. New data from the addiction severity index – reliability and validity in three centers. J Nerv Ment Dis. 1985;173:412–423. doi:10.1097/00005053-198507000-00005
7. Hendriks VM, Kaplan CD, Van Limbeek J, Geerlings P. The addiction severity index reliability and validity in a Dutch addict population. J Subst Abuse Treat. 1989;6:133–141. doi:10.1016/0740-5472(89)90041-X
8. Luo W, Wu Z, Wei X. Reliability and validity of the Chinese version of the addiction severity index. J Acquir Immune Defic Syndr. 2010;55(Suppl 1):S121–S125. doi:10.1097/QAI.0b013e3181c7dfca
9. Haraguchi A, Ogai Y, Senoo E, et al. Verification of the addiction severity index Japanese version as a treatment–customization, prediction and comparison tool for alcohol dependent patient. Int J Environ Res Public Health. 2009;6(8):2205–2225. doi:10.3390/ijerph6082205
10. Demirbaş H, Özgür Ilhan İ, Doğan YB, et al. Reliability and validity of the Turkish version of the addiction severity index in male alcohol dependents. Noro Psikiyatr Ars. 2014;51(3):216–221. doi:10.4274/npa.y6767
11. Krenz S, Dieckmann S, Favrat B, et al. French version of the addiction severity index. 5th Edition: validity and reliability among Swiss opiate dependent patients. French validation of the addiction severity index. Eur Addict Res. 2004;10(4):173–179. doi:10.1159/000079839
12. Saquib N, Rajab AM, Saquib J, et al. Substance use disorders in Saudi Arabia: a scoping review. Subst Abuse Treat Prev Policy. 2020;15(41). doi:10.1186/s13011-020-00285-3
13. Ibrahim Y, Hussain SM, Alnasser S, Almohandes H, Sarhandi I. Patterns and sociodemographic characteristics of substance abuse in Al Qassim, SaudiArabia: a retrospective study at a psychiatric rehabilitation center. Ann SaudiMed. 2018;38(5):319–325.
14. Hamdi E, Sabry N, Sedrak A, Khowailed A, Loza N, Rabie M. Ramy H Sociodemographic indicators for substance use and abuse in Egypt. J Addiction Prevention. 2016;4(1):8.
15. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Arlington, VA: American Psychiatric Publishing; 2013.
16. Alterman AL, Brown LS, Zaballero A, McKay J. The interviewer severity ratings and composite scores of the ASI: a further look. Drug Alcohol Depend. 1994;34:201–209. doi:10.1016/0376-8716(94)90157-0
17. Leonhard C, Mulvey K, Gastfriend DR, et al. The Addiction Severity Index: a field study of internal consistency and validity. J Subst Abuse Treat. 2000;18(2):129–135. doi:10.1016/S0740-5472(99)00025-2
18. Luo W, Guo CX, Han DL, et al. Reliability and validity of Chinese version of the Addiction Severity Index among drug users in the community. Biomed Environ Sci. 2012;25(6):684–689. doi:10.3967/0895-3988.2012.06.010
19. Sandi-Esquivel LE, Avila Corrales K. Validity of the Addiction Severity Index (adapted version) in a Costa Rican population group. Bull Pan Am Health Organ. 1990;24:70–76.
20. Daeppen JB, Burnand B, Schnyder C, Bonjour M, Pécoud A, Yersin B. Validation of the addiction severity index in French-speaking alcoholic patients. J Stud Alcohol. 1996;57:585590. doi:10.15288/jsa.1996.57.585
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.