Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 18
Psychometric Evaluation of the HIV Knowledge Questionnaire-18 in a Black Canadian Population
Authors Nyambi A ![]() , Alvarez E
, Alvarez E ![]() , Anderson LN
, Anderson LN ![]() , Jackson-Best F, Tharao W, Etowa EB
, Jackson-Best F, Tharao W, Etowa EB ![]() , Baidoobonso S, Owino M, Djiadeu P, Lawson DO
, Baidoobonso S, Owino M, Djiadeu P, Lawson DO ![]() , Mbuagbaw L
, Mbuagbaw L
Received 11 March 2026
Accepted for publication 6 May 2026
Published 15 May 2026 Volume 2026:18 607376
DOI https://doi.org/10.2147/HIV.S607376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Agatha Nyambi,1 Elizabeth Alvarez,1 Laura N Anderson,1 Fatimah Jackson-Best,1 Wangari Tharao,2 Egbe B Etowa,3 Shamara Baidoobonso,4 Maureen Owino,5 Pascal Djiadeu,1 Daeria O Lawson,1 Lawrence Mbuagbaw1,6– 10
1Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada; 2Women’s Health in Women’s Hands Community Health Centre, Toronto, ON, Canada; 3Daphne Cockwell School of Nursing, Faculty of Community Services, Toronto Metropolitan University, Toronto, ON, Canada; 4Department of Community Health and Epidemiology, Dalhousie University, Halifax, NS, Canada; 5Faculty of Environmental and Urban Change, York University, Toronto, ON, Canada; 6Department of Anesthesia, McMaster University, Hamilton, ON, Canada; 7Department of Pediatrics, McMaster University, Hamilton, ON, Canada; 8Biostatistics Unit, Father Sean O’Sullivan Research Centre, St Joseph’s Healthcare, Hamilton, ON, Canada; 9Centre for Development of Best Practices in Health (CDBPH), Yaoundé Central Hospital, Yaoundé, Cameroon; 10Division of Epidemiology and Biostatistics, Department of Global Health, Stellenbosch University, Cape Town, South Africa
Correspondence: Agatha Nyambi, Department of Health Research Methods, Evidence, and Impact, McMaster University, 1280 Main Street West, Hamilton, ON, L8S4L8, Canada, Email [email protected]
Introduction: This cross‑sectional study examined HIV/AIDS knowledge as a determinant of preventative and self‑protective sexual behaviour. The HIV Knowledge Questionnaire-18 (HIV-KQ-18) is one of the most widely used HIV knowledge scales. The objective of this study was to test the psychometric properties of the HIV-KQ-18 in Black people in Ontario.
Methods: We analyzed the data from 1302 participants who completed the HIV-KQ-18 in a study conducted among Black people in Ontario. We estimated the internal consistency of this scale using Cronbach’s alpha. We analyzed the construct validity of the scale, testing hypotheses about HIV knowledge and age, education, employment status, gender, language and city using one-way ANOVA and independent sample t-tests.
Results: Cronbach’s alpha for the scale was 0.82 (95% CI: 0.80– 0.84) suggesting good internal consistency. We observed significant differences in HIV knowledge scores across age, employment status, education, and gender. Higher HIV knowledge scores were also observed among participants residing in Toronto compared to Ottawa and among those who completed the questionnaire in English compared to French.
Conclusion: The HIV-KQ-18 is a valid instrument to assess the level of HIV/AIDS knowledge among Black Ontarians, with robust internal consistency and construct validity. The HIV-KQ-18 identified important differences in HIV knowledge based on the characteristics examined, indicating the need for targeted initiatives to increase HIV-related knowledge.
Plain Language Summary: HIV knowledge plays an important role in helping people protect their health and prevent HIV transmission. In Ontario, Black communities carry a higher burden of HIV, yet many tools used to measure HIV knowledge have not been tested to make sure they work well in this population. This study was done to find out whether a commonly used questionnaire, the HIV Knowledge Questionnaire-18 (HIV-KQ-18), is a reliable and meaningful way to measure HIV knowledge among Black people in Ontario.
We analysed survey data from 1302 Black participants living in Toronto and Ottawa who completed the HIV-KQ-18 as part of a larger community study. The questionnaire asks 18 true-or-false questions about HIV transmission and prevention. We examined how consistently the questionnaire measured HIV knowledge and whether it could detect differences in knowledge between groups based on age, education, employment, language, gender, and city of residence.
The results showed that the HIV‑KQ‑18 consistently measured HIV knowledge and was able to identify differences in knowledge between groups in this population. Higher knowledge scores were linked with higher education, full-time employment, and middle adulthood. Participants living in Toronto and those who completed the survey in English also scored higher.
These findings mean that the HIV-KQ-18 can be confidently used to assess HIV knowledge among Black Canadians. The results also highlight the need for targeted, culturally appropriate education efforts to address knowledge gaps in specific groups.
Keywords: black Canadians, HIV knowledge, psychometric properties
Introduction
The World Health Organization (WHO) estimated that in 2023 there were over 39 million people living with HIV worldwide including an estimated total of 1.3 million people who were newly diagnosed.1 In Canada, the Public Health Agency of Canada (PHAC) reported an HIV incidence rate of 4.0 per 100,000 in 2020 with 1520 new diagnoses.2 In 2023, among new diagnoses in Canada where race was reported, 18% of the cases were Black people. 2 In Ontario, the Ontario HIV Epidemiology and Surveillance Initiative (OHESI) reported that in 2020, Black communities accounted for approximately 25% of new HIV diagnoses,3 despite comprising only about 5% of the total population in Ontario.4,5 Due to this disproportionate burden, Black communities have been recognized as a priority population in Ontario by the Ontario Advisory Committee on HIV/AIDS.6
HIV knowledge has been identified as a determinant of preventative or self-protective sexual behaviour. The Health Belief Model (HBM) is a commonly used conceptual framework used to understand HIV risk-taking behaviours. Applying the HBM to HIV prevention, this framework theorizes that individuals are motivated to act based on their perceived susceptibility to HIV, the perceived severity of HIV, the perceived benefits about the effectiveness of preventative measures or actions and the perceived barriers to taking preventative action.7,8 These domains are informed by HIV knowledge. Similarly, the Information Motivation Behavioural Skills (IMB) model identifies information about HIV transmission and prevention as a prerequisite to preventative actions.9
The HIV Knowledge Questionnaire (HIV-KQ) is one of the most widely used HIV knowledge scales.10 The 45-item HIV-KQ was developed to measure HIV knowledge about HIV transmission, prevention and knowledge of the consequences of HIV infection in general populations.11 Subsequently, the brief HIV Knowledge Questionnaire (HIV-KQ-18) is an 18-item instrument adapted from the original 45-item questionnaire.12 The HIV-KQ-18 has high levels of internal consistency (Cronbach’s alpha = 0.75 to 0.89) and a high correlation with the 45-item HIV-KQ (r = 0.93 to 0.97).12
The HIV-KQ-18 has not been tested among Black people in Ontario; therefore, an examination of the psychometric properties of the questionnaire is necessary. Validity and reliability are the main psychometric properties of an instrument or scale.13 A reliable instrument measures the same construct consistently and an instrument is considered valid if it measures the intended construct.13 Previous research has shown that HIV knowledge instruments may perform differently across subpopulations, highlighting the importance of examining scale performance within groups disproportionately affected by HIV.14,15 Among Black communities in Canada, structural inequities and differential access to health information may shape both HIV knowledge acquisition and interpretation of survey items.16,17 This supports the need for a psychometric examination of the HIV-KQ-18 to ensure adequate psychometric performance when measuring HIV knowledge among Black communities. The validation of this instrument in this population will inform a more contextualized interpretation of study results, which allows researchers to better identify knowledge gaps to inform future education and prevention interventions.
The HIV-KQ-18 was used to measure the HIV knowledge of participants in a cross-sectional study of HIV epidemiology among Black communities in Ontario, the A/C study.18 Among the participants of the A/C study, we used the HIV-KQ-18 and previously reported that only 56% had high knowledge. However, the psychometric properties of the HIV-KQ-18 have not been evaluated in this population. The A/C study found and reported that only 56.5% of survey participants had high knowledge about HIV transmission and acquisition.19
The objective of this study is to examine the psychometric properties of the HIV-KQ-18 questionnaire in a Black population with a focus on construct validity and internal consistency.
Methods
Study Design and Sample
The A/C study recruited participants that met the following criteria: born in a Caribbean or sub-Saharan African country, or born elsewhere (including Canada) with a parent born in one of those countries; aged 15–64 years old at the time of the survey; residence in the Greater Toronto Area (Toronto) or Ottawa, Ontario; capacity to communicate in English or French; and capable of providing informed consent. Participants were recruited by peer recruiters from January to December 2019.
The study was approved by the following affiliated institutional Research Ethics Boards (REBs): University of Ottawa Research Ethics Board; Ottawa Public Health Research Ethics Board; Toronto Public Health Research Ethics Board; Laurentian University Research Ethics Board; and University of Toronto. All methods were carried out in accordance with relevant guidelines and regulations.
Instrument
In this study, we used data collected through the HIV-KQ-18 questionnaire (the study instrument) to measure participants’ HIV knowledge. The questionnaire (see Supplementary File 1) consists of 18 statements about HIV and participants were asked to indicate whether they think the statement is true or false.12 Responses to the questionnaire were then computed into a knowledge score with one point for every correct answer for a maximum of 18 points.
Statistical Analysis
Descriptive statistics were calculated using Stata version 17.20 We computed frequencies and percentages for categorical variables. Although the HIV‑KQ‑18 was developed as a continuous measure and does not have empirically established cut‑off scores, categories of HIV knowledge were created for descriptive purposes to aid interpretation. We categorized participants into four knowledge levels: No HIV knowledge (score = 0), Low HIV knowledge (score = 1–6), Moderate HIV knowledge (score = 7–12), and High HIV knowledge (score = 13–18). For each category, the number and proportion of participants [n (%)] were reported. Consistent with prior practice, all psychometric analyses were conducted using continuous scores. We calculated the overall mean HIV-KQ-18 score with its standard deviation (SD) to summarize central tendency and variability in HIV knowledge across the sample. Missing data were minimal and were handled using complete‑case analysis. The sample size was determined by the available data from the A/C study. With 1302 participants, the sample size exceeds commonly recommended thresholds for psychometric validation studies and was considered adequate to evaluate internal consistency and construct validity of the HIV‑KQ‑18.
Internal Consistency
We estimated internal consistency of this scale using Cronbach’s alpha score. Internal consistency describes how closely the items on a scale are related to each other or the degree to which all items assess the same concept or construct.21 Acceptable values of alpha range from 0.70 to 0.95.21,22 We estimated the corrected item-total correlation which is the correlation between a single item and the sum of all the other items in a scale excluding the item itself.23 The commonly accepted cut-off for this measure is 0.30.23 The Cronbach’s alpha for the scale with the removal of individual items was also calculated.
Construct Validity
Construct validity refers to the agreement of the scale with theoretical constructs.24 Known-groups validity is a type of construct validity which is used to measure whether a scale is able to distinguish between groups that are known to differ on the construct.25 We hypothesized that we would find differences in HIV knowledge in the sampled population by age, education and employment. In previous international research, these factors have been associated with HIV knowledge.26–29 We hypothesized that older age groups, those with higher levels of education and those with full-time employment had higher levels of HIV knowledge. We also examined the relationship between gender, city, and language as exploratory constructs and hypothesized that we would find differences in scores in these additional categories. We used the ANOVA test and t-tests to compare HIV knowledge levels for the subgroups of interest, followed by post-hoc pairwise comparisons using the Bonferroni correction where necessary.30
Results
Out of 1380 participants who participated in the A/C study, 1302 completed the HIV-KQ-18 questionnaire. Most participants were women (n = 813, 62%) and were employed either full-time or part-time (n = 718, 55%). The majority were from Toronto (n = 816, 63%) and completed the questionnaire in English (n = 1208, 93%). The complete sociodemographic information of the included participants is presented in Table 1.
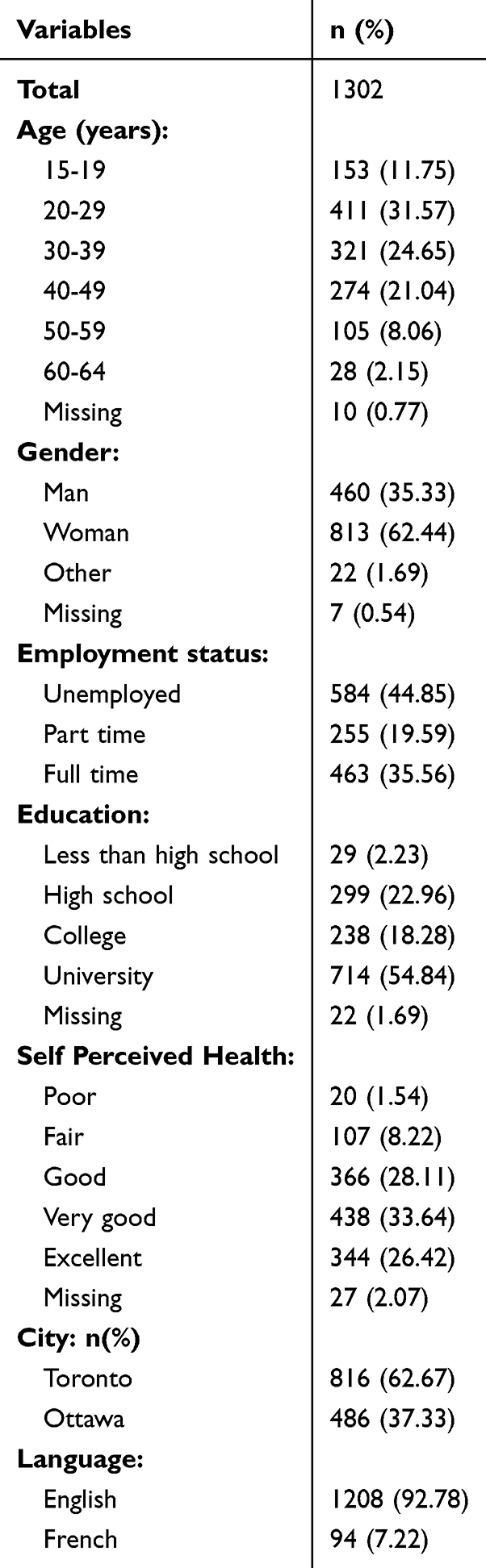 |
Table 1 Socio-Demographic Characteristics of Participants (N=1302) |
The mean knowledge score for all participants in this sample was 12.45 or 69.1% (95% confidence interval [CI]: 12.23, 12.67) out of a total of 18 potential points, meaning on average participants provided a correct response to ~70% of the items in the questionnaire. The overall performance of participants to the questions in the HIV-KQ-18 is presented in Supplementary File 1. Out of 1302 participants, 2.38% (n = 31) had no HIV knowledge (0 out of 18 points), 7.60% (n = 99) had low HIV knowledge (1 to 6 out of 18 points), 30.18% (n = 393) had moderate HIV knowledge (7 to 12 out of 18 points) and 59.83% (n = 779) had high HIV knowledge (13 to 18 out of 18 points). The socio-demographic characteristics of participants by HIV knowledge level with the mean score of each group are presented in Table 2.
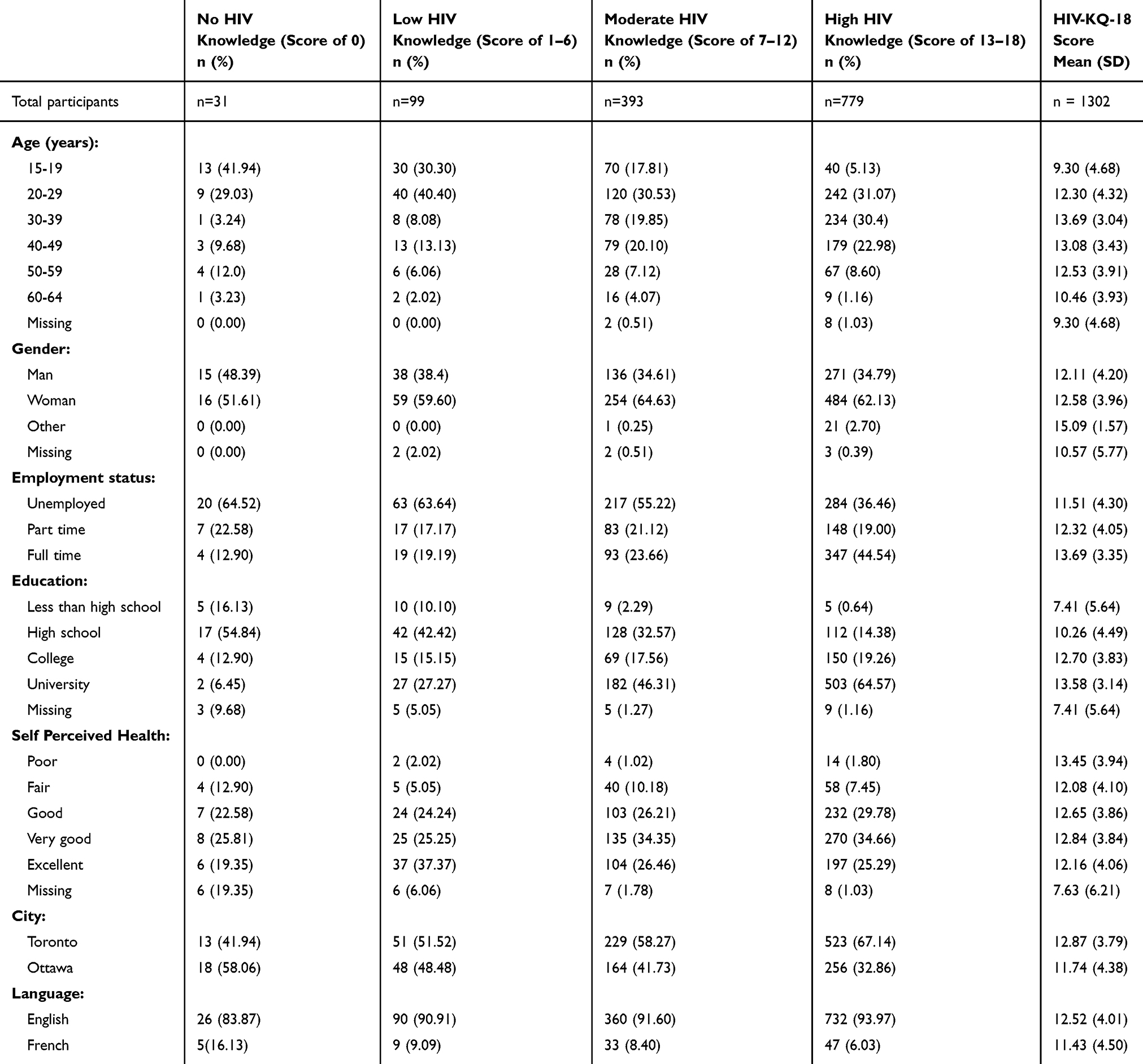 |
Table 2 Socio-Demographic Characteristics of Participants by HIV Knowledge Level (Score Out of 18 Points) |
Internal Consistency
The Cronbach’s alpha for the scale was 0.82 (95% CI 0.80–0.84) suggesting good internal consistency. The “alpha if removed” for each item varied slightly. The corrected item-total correlation values ranged from 0.24 to 0.58 indicating a moderate relationship between individual items and the total scale score. The full item total statistics are reported in Table 3.
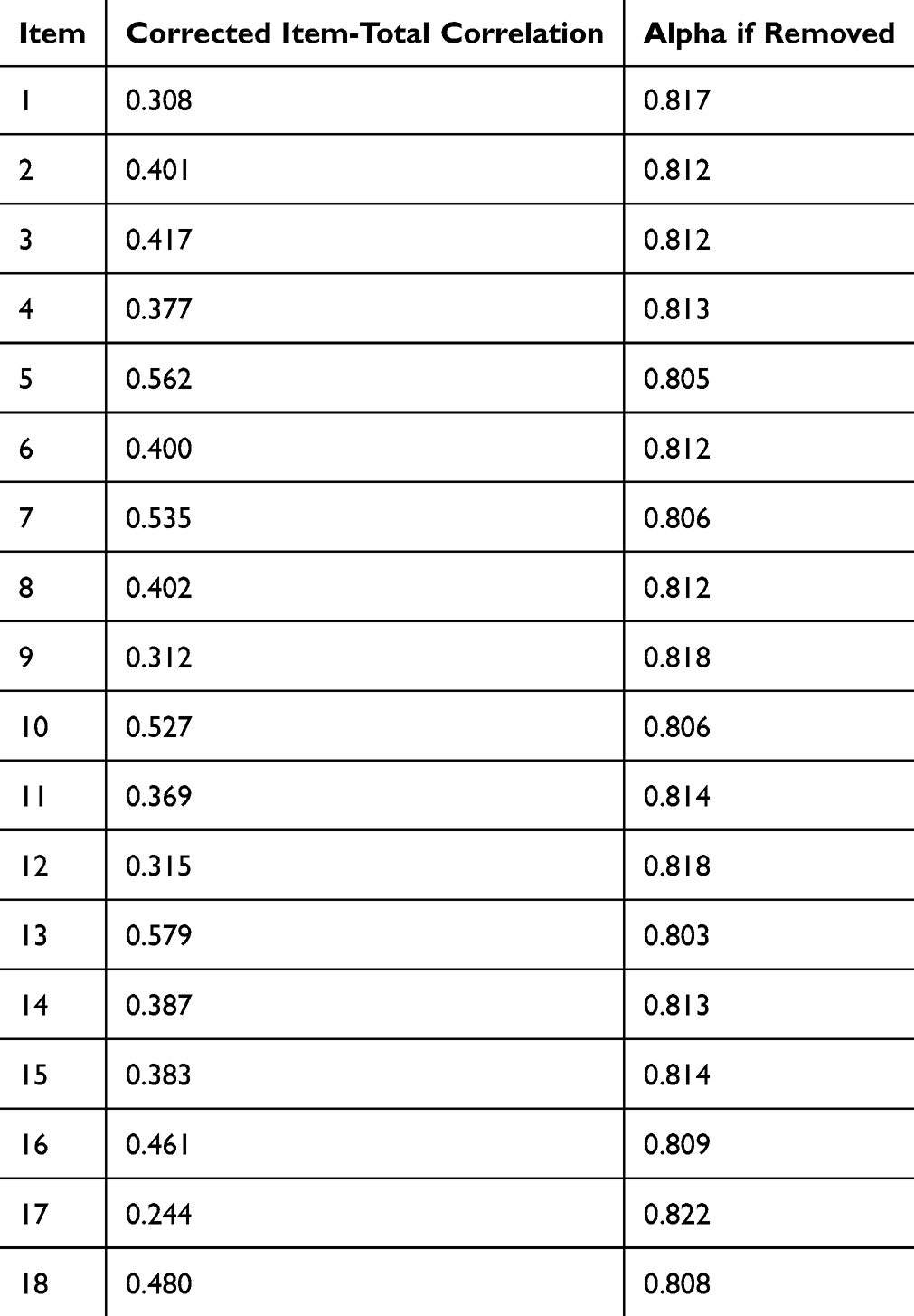 |
Table 3 Item-Total Statistics |
Construct Validity
A one-way ANOVA to compare the effect of age on HIV knowledge scores revealed that there was a statistically significant difference in mean scores between at least two age groups (F(5, 1286) = [30.30]; p = < 0.001). Post hoc analysis using the Bonferroni correction indicated those aged 15 to 19 scored significantly lower than all other age groups except for those aged 60 to 64 (mean difference [MD] = −1.16; 95% CI [−1.16, 3.49]; p > 0.999). Participants ages 20 to 29 scored significantly higher than those aged 15 to 19 (MD = 3.00; 95% CI: [1.93, 4.08]; p < 0.001) and significantly lower than those aged 30 to 39 (MD = −1.39; 95% CI: [0.55, 2.23]; p < 0.001). Those aged 30 to 39 also had significantly higher scores than those aged 60 to 64 (MD = 3.23; 95% CI: [1.00, 5.46]; p < 0.001). Participants aged 40 to 49 had significantly higher scores than those aged 60 to 64 (MD = 2.62; 95% CI: [0.38, 4.87]; p = 0.009).
We found statistically significant differences in mean scores by employment status (F(2, 1299) = [39.93]; p < 0.001). Post-hoc analysis showed statistically significant differences in scores between all groups. Participants who reported that they were employed full time had significantly higher scores than those employed part time (MD = 1.38; 95% CI: [0.64, 2.11]; p < 0.001) and unemployed participants (MD = 2.18; 95% CI: [1.60, 2.77]; p < 0.001).
We found statistically significant differences in mean scores by education level (F(3, 1276) = [75.76]; p < 0.001). Post-hoc analysis showed statistically significant differences in scores between all education levels. Participants who reported that they completed university had significantly higher scores than those who reported completing college (MD = 0.88; 95% CI: [0.15, 1.61]; p = <0.001), high school (MD = 3.32; 95% CI: [2.65, 4.00]; p < 0.001) and less than high school (MD = 6.17; 95% CI: [4.32, 8.02]; p < 0.001).
We also found statistically significant differences in mean scores by gender (F(2, 1292) = [6.76]; p = 0.001). Post-hoc analysis revealed significantly higher scores among participants who identified themselves in gender categories other than men (MD = 2.98; 95% CI: [0.87, 5.08]; p < 0.001) or women (MD = 2.51; 95% CI: [0.43, 4.60]; p = 0.012). There was no statistically significant difference between the scores of men and women (MD = 0.47, 95% CI: [−0.1, 1.03]; p = 0.144).
Independent two sample t-tests revealed higher HIV knowledge scores among those living in Toronto compared to Ottawa (MD=1.13, 95% CI: 0.68–1.58; p = <0.001). We also found higher scores among those who completed the questionnaire in English compared to French (MD = 1.08, 95% CI: 0.24–1.94; p = 0.012). Table 4 presents a summary of all the psychometric properties we examined in this study.
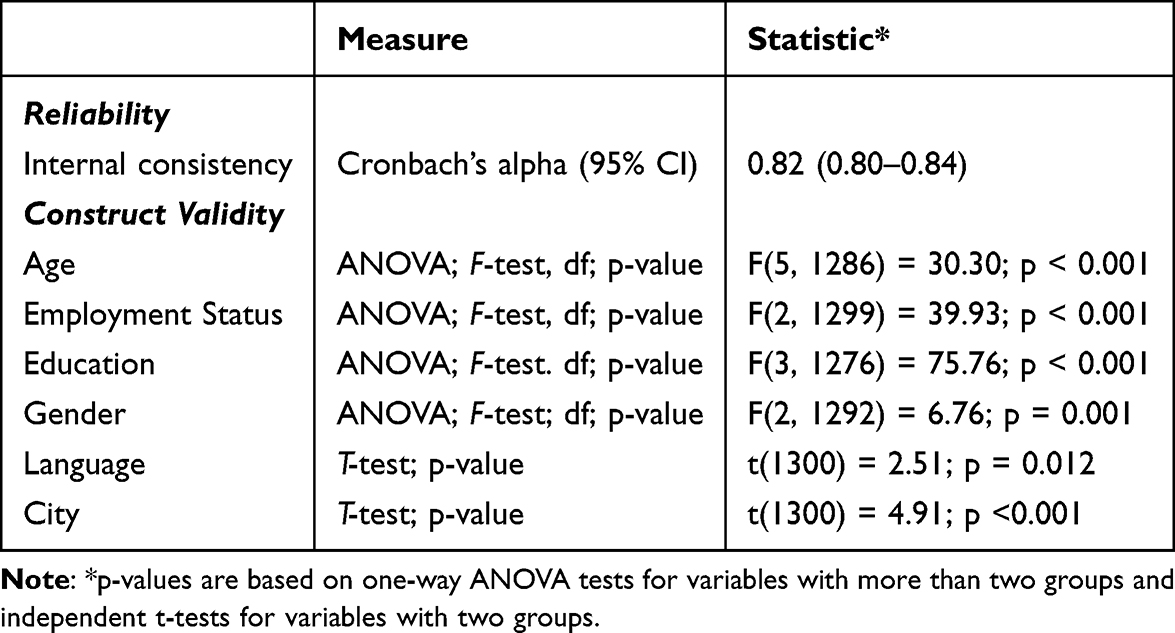 |
Table 4 Summary of Psychometric Properties |
Discussion
Our findings suggest that the HIV-KQ-18 demonstrates acceptable psychometric performance for use in a Black Canadian population. The mean knowledge score of 69.1% for the overall sample was similar to that of the populations sampled in the development study for the HIV-KQ-18 which ranged from 69.2% to 72.5%.12 The Cronbach’s alpha score of 0.82 is well within the range of acceptable values.21 In our examination of the internal consistency of the questionnaire, we found that the value of alpha varied slightly with the removal of items, however the range of values was between 0.81 and 0.82 confirming that the instrument is well constructed. The corrected item-total correlation values ranged from 0.24 to 0.58 indicating a moderate relationship between individual items and the total scale score. One item (Item 17) fell below the threshold of 0.30; however, the removal of that item does not significantly change the Cronbach’s alpha of the scale. Future qualitative studies may be necessary to provide additional insight into the cultural appropriateness of the items and to determine whether any modifications of items are necessary to improve clarity.
Our findings indicate that the HIV-KQ-18 effectively differentiates participants’ levels of HIV knowledge based on their education level, employment status, and age, consistent with our a priori hypotheses. Participants with higher education levels and full-time employment had higher HIV knowledge than those with lower education levels and those who reported being employed part-time or unemployed. We also hypothesized that HIV knowledge would increase with age, and we found this to be true; however, participants ages 60 to 64 had a statistically significant lower score than all other age groups except those aged 15 to 19 indicating that the oldest age groups and youngest have similar HIV knowledge. In a study conducted in the United States using this instrument in a population of older adults, with an average age of 73.7, the researchers reported an average knowledge score of 10.8 which is similar to the average score of 10.46 in this study among those in the oldest age group.31 A Canadian study examining predictors of HIV knowledge in rural and urban Canadian populations in Ontario, British Columbia and Newfoundland found that age was a significant predictor, and those in age groups over 50 were less likely to be categorized as having high knowledge of HIV/AIDS.32 This might indicate the need for targeted interventions for older adults, as education campaigns are often designed for younger populations. This gap in outreach efforts might lead older populations to assume they are not at risk for contracting HIV leading to lapses in the most up to date information about HIV.
We also examined gender, language and the city of questionnaire administration as exploratory constructs. The relationship between HIV knowledge and gender varies in different populations. A systematic review examining the relationship between gender and HIV knowledge among adolescents in low and middle income countries found that males were consistently found to have higher HIV knowledge scores than females.33 Similarly, in a systematic review of HIV knowledge and attitudes in the Middle East and North Africa, researchers found that while male populations often had higher HIV knowledge, there were exceptions to that overall trend in some populations in Afghanistan, Iran and Pakistan where female populations had more HIV knowledge.34 There are no similar evidence syntheses including Canadian populations; however, other Canadian studies have not found significant differences in HIV knowledge by gender.32,35 In this study, participants who identified themselves in gender categories other than men or women had significantly higher scores. This finding warrants further examination. This may suggest that interventions targeting those who identify outside of the gender binary have been more effective.
Participants from Toronto and those who completed the questionnaire in English had higher scores than those who participated in Ottawa and completed the questionnaire in French respectively. Canada is a bilingual country, however, in Ontario most francophones reside in Eastern Ontario, a region which includes the city of Ottawa.36 In this study, 4.4% (n = 38) of Toronto participants took the questionnaire in French compared to 12.5% (n = 66) of participants in Ottawa. Our findings suggest that there may be a need for targeted initiatives focused on Francophone populations and those in Ottawa.
Our study is the first validation study of the HIV-KQ-18 in a Black Canadian population with a robust sample of over 1300 participants from two large Canadian cities. However, there are limitations to our findings. First, due to the cross-sectional design, we were not able to assess other psychometric properties such as test–retest reliability. Second, due to our recruitment in urban cities, there may be additional considerations for Black Canadians who live in rural communities which we are unable to assess. Finally, there is no validated French version of this instrument, therefore additional validation studies to develop a French version of this instrument may be necessary.
Conclusion
Our psychometric analysis shows that the HIV-KQ-18 is a valid and reliable instrument to assess HIV knowledge among Black Canadians. We encourage the use of the instrument in future Canadian research. Future research should assess additional psychometric properties of the HIV‑KQ‑18, to further strengthen evidence for its use among Black Canadians.
Ethics Approval and Consent to Participate
The A/C study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the following Research Ethics Boards: Toronto Public Health Research Ethics Board (TPH REB, 18 Jun 2018); Ottawa Public Health Research Ethics Board (OPH REB; 3 April 2018); Laurentian University Research Ethics Board (LU REB; 17 November 2017); University of Ottawa Research Ethics Board (1 September 2018) University of Toronto (25 June 2018). All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained from all subjects.
Acknowledgments
We acknowledge the support of the Public Health Agency of Canada’s National HIV and Retrovirology Laboratories for performing the dried blood spot testing; the community members, interviewers, study coordinators, community organizations (Women’s Health in Women’s Hands, Black Creek Community Health Centre, Somerset West Community Health Centre, Canadians of African Descent Health Organization, AIDS committee of Ottawa, African Canadian Association of Ottawa, TAIBU Community Health Centre, Africans in Partnership Against AIDS, African and Black Diaspora Global Network, Black Health Alliance, Bruce House, Regent Park Community Health Centre), partner institutions and participants who contributed their valuable time to this research. Also, we thank the numerous collaborators, colleagues and partners who were involved in earlier stages of this project. The abstract of this paper was presented as a conference talk at the 2025 Canadian Association for HIV Research (CAHR) Conference with interim findings and published in the abstract book.37
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The A/C study was supported by an award/grant from The Ontario HIV Treatment Network (EFP 1057). The A/C study was also supported by the Canadian Institutes of Health Research through an Operating Grant in the HIV/AIDS Community-Based Research (CBR) Program (163414).
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNAIDS 2023 Report. UNAIDS - global report 2023. Available from: https://thepath.unaids.org/.
2. Canada PHA of. HIV in Canada, surveillance report to December 31, 2022. 2024. Available from: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/hiv-canada-surveillance-report-december-31-2022.html.
3. Ontario HIV Epidemiology and Surveillance Initiative. Trends in HIV testing, diagnoses and the care cascade in Ontario in 2022. OHESI. 2023. Available from: https://www.ohesi.ca/trends-in-hiv-testing-diagnoses-and-the-care-cascade-in-ontario-in-2022/.
4. Government of Canada. Census of population. 2001. Available from: https://www12.statcan.gc.ca/census-recensement/index-eng.cfm.
5. Government of Canada. Black history month 2023. by the numbers. 2023. Available from: https://www.statcan.gc.ca/en/dai/smr08/2023/smr08_270.
6. Ontario Advisory Committee on HIV/AIDS. OACHA HIV Action Plan to 2030. Available from: https://www.ontario.ca/files/2023-12/moh-oacha-hiv-action-plan-en-2023-12-01.pdf.
7. Tarkang EE, Zotor FB. Application of the health belief model (HBM) in HIV prevention: a literature review. Central Afr J Public Health. 2015;1(1):1–10. doi:10.11648/j.cajph.20150101.11
8. DiClemente RJ, Peterson JL. Preventing AIDS: Theories and Methods of Behavioral Interventions. Springer US; 1994. doi:10.1007/978-1-4899-1193-3
9. Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychol Bull. 1992;111(3):455–474. doi:10.1037/0033-2909.111.3.455
10. Stewart JL, Wallace DD, Nance A, et al. Validated HIV knowledge scales for use with adults and adolescents: a systematic review. AIDS Behav. 2022;26(5):1695–1715. doi:10.1007/s10461-021-03521-4
11. Carey M, Morrison-Beedy D, Johnson B. The HIV-knowledge questionnaire: development and evaluation of a reliable, valid, and practical self-administered questionnaire. AIDS Behav. 1997;1(1):61–74. doi:10.1023/A:1026218005943
12. Carey MP, Schroder KEE. Development and psychometric evaluation of the brief HIV knowledge questionnaire. AIDS Educ Prev. 2002;14(2):172–182. doi:10.1521/aeap.14.2.172.23902
13. Ginty AT. Psychometric properties. In: Gellman MD editor. Encyclopedia of Behavioral Medicine. Springer International Publishing; 2020:1770–1771. doi:10.1007/978-3-030-39903-0_480
14. Burke HM, Fleming PJ, Guest G. Assessment of the psychometric properties of HIV knowledge items across five countries. AIDS Educ Prev. 2014;26(6):577–587. doi:10.1521/aeap.2014.26.6.577
15. Oglesby WH, Alemagno SA. Psychometric properties of an HIV knowledge scale administered with populations at high risk for HIV infection. Health Promot Pract. 2013;14(6):859–867. doi:10.1177/1524839912470453
16. Baidoobonso S, Bauer GR, Speechley KN, Lawson E. HIV risk perception and distribution of HIV risk among African, Caribbean and other Black people in a Canadian city: mixed methods results from the BLACCH study. BMC Public Health. 2013;13(1):184. doi:10.1186/1471-2458-13-184
17. Husbands W, Lawson DO, Etowa EB, et al. Black Canadians’ exposure to everyday racism: implications for health system access and health promotion among urban black communities. J Urban Health. 2022;99(5):829–841. doi:10.1007/s11524-022-00676-w
18. Mbuagbaw L, Tharao W, Husbands W, et al. A/C study protocol: a cross-sectional study of HIV epidemiology among African, Caribbean and Black people in Ontario. BMJ Open. 2020;10(7):e036259. doi:10.1136/bmjopen-2019-036259
19. A/C Study: HIV prevalence and risk factors among African, Caribbean and Black people in Ontario, CCDR 48(10). 2022. Available from: https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2022-48/issue-10-october-2022/cross-sectional-investigation-hiv-prevalence-risk-factors-african-caribbean-black-people-ontario-ac-study.html.
20. Stata statistical software: release 17. StataCorp LLC; 2021.
21. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
22. Streiner DL. Starting at the beginning: an introduction to coefficient alpha and internal consistency. J Pers Assess. 2003;80(1):99–103. doi:10.1207/S15327752JPA8001_18
23. Hajjar STE. Statistical analysis: internal-consistency reliability and construct validity. Int J Quant Qual Res Methods. 2018;6(1):46–57.
24. Streiner DL, Norman GR, Cairney J. Health Measurement Scales: A Practical Guide to Their Development and Use. Oxford University Press, Incorporated; 2015. Available from: http://ebookcentral.proquest.com/lib/mcmu/detail.action?docID=1816173.
25. Davidson M. Known-groups validity. In: Maggino F editor. Encyclopedia of Quality of Life and Well-Being Research. Springer International Publishing; 2023:3764. doi:10.1007/978-3-031-17299-1_1581
26. Klein H, Sterk C, Elifson K. Knowledge about HIV in a community sample of Urban African Americans in the South. J AIDS Clin Res. 2016;7(10):622. doi:10.4172/2155-6113.1000622
27. Peltzer K, Matseke G, Mzolo T, Majaja M. Determinants of knowledge of HIV status in South Africa: results from a population-based HIV survey. BMC Public Health. 2009;9(1):174. doi:10.1186/1471-2458-9-174
28. Kefale B, Damtie Y, Yalew M, Adane B, Arefaynie M. Predictors of comprehensive knowledge of HIV/AIDS among people aged 15–49 years in Ethiopia: a multilevel analysis. HIVAIDS - Res Palliat Care. 2020;12:449–456. doi:10.2147/HIV.S266539
29. Betunga B, Nuwabine L, Katushabe E, et al. Predictors of HIV knowledge, perceived stigma and risk among transport workers in Mbarara City, Southwestern Uganda. East Afr Health Res J. 2024;8(2):245–255. doi:10.24248/eahrj.v8i2.787
30. Napierala MA. What is the Bonferroni correction? AAOS Now. 2012;40–41.
31. Davis TEK, Elder MA. HIV knowledge and preferences for HIV prevention among older adults living in the community. Gerontol Geriatr Med. 2020;6:2333721420927948. doi:10.1177/2333721420927948
32. Veinot TC, Harris R. Talking about, knowing about HIV/AIDS in Canada: a rural-urban comparison. J Rural Health. 2011;27(3):310–318. doi:10.1111/j.1748-0361.2010.00353.x
33. Chory A, Gillette E, Callen G, et al. Gender differences in HIV knowledge among adolescents and young people in low-and middle-income countries: a systematic review. Front Reprod Health. 2023;5. doi:10.3389/frph.2023.1154395
34. Mumtaz GR, Hilmi N, Majed EZ, Abu-Raddad LJ. Characterising HIV/AIDS knowledge and attitudes in the Middle East and North Africa: systematic review and data synthesis. Glob Public Health. 2020;15(2):275–298. doi:10.1080/17441692.2019.1668452
35. Johnston CL, Marshall BDL, Qi J, et al. HIV knowledge and perceptions of risk in a young, urban, drug-using population. Public Health. 2011;125(11):791–794. doi:10.1016/j.puhe.2011.09.008
36. Profile of the Francophone population in Ontario – 2021 | ontario.ca. Available from: http://www.ontario.ca/page/profile-francophone-population-ontario-2021.
37. Nyambi A, Alvarez E, Anderson LN, et al. Psychometric evaluation of the HIV knowledge questionnaire‑18 in a Black Canadian population. In:
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.