Back to Journals » Patient Preference and Adherence » Volume 16
Psychometric Evaluation of the Chinese Version of Decisional Conflict Scale in Chinese Young Women Making HPV Vaccination Decisions
Authors Zhai ZH, Ning JH, Wang LDL
Received 16 January 2022
Accepted for publication 11 March 2022
Published 24 March 2022 Volume 2022:16 Pages 761—769
DOI https://doi.org/10.2147/PPA.S358292
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Zi Han Zhai,1,2 Jun Hao Ning,1,2 Linda Dong-Ling Wang1,3
1Institute of Translational Medicine, Medical College, Yangzhou University, Yangzhou, 225001, People’s Republic of China; 2Jiangsu Key Laboratory of Experimental & Translational Non-Coding RNA Research, Yangzhou, 225001, People’s Republic of China; 3Centre for Psycho-Oncology Research & Training, School of Public Health, The University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China
Correspondence: Linda Dong-Ling Wang, Institute of Translational Medicine, Medical College, Yangzhou University, Yangzhou, 225001, People’s Republic of China, Tel +86-051487978925, Email [email protected]
Purpose: The Decisional Conflict Scale (DCS) is a well-known scale for measuring personal decisional conflict, particularly when a person feels uninformed about the risks/benefits of choices, is unclear about personal values, and feels unsupported in making a choice. Higher scores of DCS indicate higher decisional conflict. In the present study, we aimed to assess the psychometric properties of the Chinese version of the DCS among Chinese young women making HPV vaccination decisions.
Methods: A total of 107 HPV-unvaccinated Chinese women aged 18– 26 completed the survey assessing decisional conflict, knowledge and decision of HPV vaccination. Factorial validity, construct validity, and reliability of the DCS were examined.
Results: The mean score of the DCS-16 was 41.5 (SD=20.0). Principal component analysis extracted a 3-factor model of DCS containing 13 items (DCS-13), but both the original DCS-16 and extracted DCS-13 showed poor factorial validity. An alternative DCS-10 revealed a good fit to the data with Cronbach’s alpha 0.86. Some subscales of the three versions of DCS showed inconsistent correlation.
Conclusion: The DCS-10 demonstrated good model fit to the data. By using the DCS-10 total score rather than sub-scores to measure Chinese young women’s HPV vaccination decisional conflict a more valid assessment can be obtained.
Keywords: decisional conflict, validation, HPV vaccination, decision making
Introduction
Human Papillomavirus (HPV) is the primary cause of cervical cancer which ranked the second most common cancer in females living in less developed regions.1 The establishment of HPV vaccination can effectively prevent HPV infection and related diseases. HPV vaccination in free-market Hong Kong is promoted mainly by the pharmaceutical industry through mass media. In the absence of government-organized promotion programmes, producer HPV vaccination promotion and advocacy are of limited effectiveness. The uptake rate of HPV vaccination has been lower than expected, ranging from less than 10% among adolescent girls aged 9–18 years to 47.2% among 18–24 years old local undergraduate female students where the universities provided discounted HPV vaccines for female students, and only 3% adult women have received HPV vaccination.2–6 A number of predictors have been identified to explain vaccinating behaviours, for instance attitude, knowledge, endorsement from physicians.7 However, very few studies have investigated respondents’ decisional conflict during HPV vaccination decision making, a new vaccine class embodying considerable uncertainty surrounding the outcomes of health decision.
Decisional conflict is “a state of uncertainty about the course of action to take”, particularly when a person feels uninformed about the risks/benefits of choices/alternatives, is unclear about personal values, and feels unsupported in making a choice or pressured to choose on course of action.8,9 The manifestations of such conflict include verbalized uncertainty about choices and undesired consequences of alternatives, hesitation among choices, delayed decision making, and questioning personal beliefs and value while trying to make decisions.8 Decisional conflict is commonly found in preference sensitive decisions where the uncertainty arises from the complexity of choices that involve value trade-offs between perceived benefits and harms, and modifiable factors like level of knowledge and adequacy of support.8 Individuals with high levels of decisional conflict about the choice at hand will most likely delay making a decision. Ultimately, high decisional conflict compromises one’s quality of life.10
The Decisional Conflict Scale (DCS) was developed in 1990s by O’Connor to measure individual perceptions of a) uncertainty in choosing options; b) factors contributing to uncertainty such as feeling uninformed, unclear about personal values and unsupported in decision-making; and c) effective decision making such as feeling the choice is informed, values-based, likely to be implemented and expressing satisfaction with the choice.9 The original DCS was psychometrically tested with individuals who were making a decision on influenza immunizations and breast cancer screening.8 The initial DCS included three subscales when it was developed derived from the decisional conflict construct, namely Decision Uncertainty (3 items), Factors Contributing to Uncertainty (9 items), and Perceived Efficacy in Decision Making (3 items). Initial psychometric testing of the DCS elicited a test-retest coefficient of 0.81 and reliability coefficients of 0.58–0.92.8
The standard forms of the DCS comprises 16 self-administrated items in statement and question format. The Statement format DCS is traditional with 5-point Likert Scale (from 0=Strongly Agree to 4=Strongly Disagree), which has been widely used in most studies to date, but many participants reportedly found it hard to respond to.9 The Question format DCS uses 5 response categories (from 0=Yes, 1=Probably yes, 2=Unsure, 3=Probably no, to 4=No), which is reportedly easier to respond to.9 Overall, the 16 items were categorized into 5 subscales: Informed subscale (3 items), Values Clarity subscale (3 items), Support subscale (3 items), Uncertainty subscale (3 items), and Effective Decision subscale (4 items).9 The total score is calculated by adding up these five sub-scores, then convert the score by using 100 as the full mark. Higher scores indicate higher decisional conflict.9
DCS has been used in different decision-making contexts: influenza immunization,8 breast cancer screening,9 genetic testing,11,12 breast cancer surgery,13 oncology treatment,14,15 end-of-life decision making,16 and asthma treatment.17 It has also been assessed in decision of continuing studies among nursing students.18 DCS is available in multiple languages including English, Spanish, French, Chinese, Dutch and Japanese.7,11–16,18
One validation study of Chinese version DCS which was conducted on breast cancer surgery decision-making among Hong Kong Chinese women with breast cancer, and revealed that the original 5-factor structure of 16-item DCS had poor fit to the sample data.13 The study suggested an alternative 3-factor structure of the Chinese DCS version with 14 items gave better data fit. The possible total scores range from 0 to 64, with higher scores indicating greater decisional conflict. The overall internal consistency for the alternative 3-factor structure of 14-item DCS is high (Cronbach’s α=0.81), and comprises Informed and Values Clarity (Cronbach’s α=0.87), Uncertainty and Effective Decision (Cronbach’s α=0.71), and Support (Cronbach’s α=0.51).13
Unlike in oncology studies,8,11–15 there is very limited study on vaccination decision conflict.19 Meanwhile, the validity and reliability of DCS, and hence its utility when applied to HPV vaccination decision-making among Chinese populations is unclear. The objective of this study was to assess the decisional conflict level and to evaluate the psychometric properties of the Chinese version of the DCS among young Chinese women making HPV vaccination decisions.
Materials and Methods
Participants
Chinese women aged 18–26 years resident in Hong Kong, who were able to communicate in Cantonese or Mandarin, have no history of HPV vaccination were invited to respond to a self-administered questionnaire. Women of this age range were chosen because they can make vaccination decisions by themselves and USA Advisory Committee on Immunization Practices (ACIP) recommends young adult women through age 26 should receive HPV vaccination.20 The study complied with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (HKU/HA HKW IRB, reference number: UW 13-397). All participants were informed about the purpose of the study, and written consent from all participants was obtained at initial contact. Bryant and Yarnold suggest the subjects-to-variables ratio should be five or greater and every analysis should be based on a minimum of 100 observations.21 By using convenience sampling method, 109 young Chinese women recruited by snowball sampling from local universities and community centres were invited and completed the assessment.
Measures
Decisional conflict was measured using the Chinese version of the 16-item question format DCS (Appendix-1) originally translated by Lam et al for Chinese women making decision for breast cancer surgery.13 (The full version of Chinese DCS-16 is available from https://decisionaid.ohri.ca/docs/develop/Tools/DCS_Question_Chinese.pdf). Only the decision was modified to HPV vaccination uptake. Five-point Likert scales, with coding of 0=Yes, 1=Probably yes, 2=Unsure, 3=Probably no, and 4=No were the response format. Each sub-score was calculated by averaging the sum of the corresponding subscale then multiplying by 25 so the sub-score ranged from 0 to 100. The higher the sub-score in uncertainty subscale, informed subscale, values clarity subscale, support subscale and effective decision subscale, the more participants felt uncertain, uninformed, unclear about personal values, unsupported and ineffective decision making, respectively.9 Total score was calculated by averaging the sum of 16 items then multiplying by 25 so it also ranged from 0 (no decisional conflict) to 100 (extremely high decisional conflict).9
Knowledge about HPV and HPV vaccination was evaluated using five True/False statements regarding prevalence and routes of HPV transmission, vaccination administration, recommended age of vaccination, and perceived causation of cervical cancer, as well as knowledge about Pap smears. Total scores ranged from 0 to 10, with higher scores indicating greater knowledge (Appendix-2).
Decision on HPV vaccination was measured by asking participants “Now that you have had a chance to consider your options for HPV vaccination, which choice looks the best to you?” The responses (Receive HPV vaccination/Do not receive HPV vaccination/Unsure) were classified as accept, reject, or unsure about the decision of HPV vaccination.
Data Analysis
Descriptive statistics summarized participants’ socio-demographic characteristics, scores of DCS, HPV vaccination-related knowledge, and HPV vaccination decision. Confirmatory factor analysis (CFA) was performed to examine the factorial validity of the original 5-factor model of the DCS. Since DCS scores can utilize all-items total or individual subscale scores to assess decisional conflict, both hierarchical and correlated models of the DCS were compared to determine which gave the best data fit. Multiple model fit indices were used, including chi-squared statistic, the comparative fit index (CFI), root mean square error of approximation (RMSEA) with 90% confidence interval, Tucker-Lewis Index (TLI), and standardized root mean square residual (SRMR). CFI and TLI values ≥0.90, RMSEA values ≤0.10 with 90% confidence interval, and SRMR values ≤0.08 suggest acceptable model fit.22 If the original 5-factor model of the DCS-16 was unsupported, exploratory factor analysis (EFA) would be conducted to explore the potential factorial structure. Cronbach’s alpha coefficients of the scale and sub-scales were calculated examining the internal consistency of the scale. Minimal acceptable alpha was specified at 0.70.23
Construct validity was tested by correlating the DCS with the knowledge of HPV vaccination. We hypothesized that the DCS would be inversely correlated to knowledge of HPV vaccination. All correlation was performed using Pearson’s correlation analysis. In addition, construct validity was tested using the known-groups comparison approach. DCS total scores and subscores were compared between groups of participants who indicated certain (accept/reject) and uncertain (unsure) decisions to HPV vaccination. According to the decisional conflict construct, individuals who were unsure about their decisions were expected to have higher decisional conflict scores than their counterparts.
Furthermore, since the 4 factor 10 items of DCS (DCS-10) (Appendix-3) use the same items drawn from DCS-16 and the response (Yes, Unsure, and No) is similar to the DCS-16 (Yes/Probably yes/Unsure/ Probably no/No) after combining the 5 responses to 3 responses, we took a further step using abovementioned method to examine the factorial validity, construct validity and reliability of the DCS-10 in the same sample of Chinese young women considering HPV vaccination decisions.
Excepting that CFA was performed using Mplus version 6 software, all data analyses were carried out using SPSS version 24.0 and p<0.05 was considered statistically significant.
Results
Study Participants
Among the 109 participants approached, two did not fully complete the DCS and were excluded from the final analysis. Socio-demographic characteristics of the final 107 participants are summarized in Table 1. The mean age of respondents was 22.9 years (SD: 2.5; range: 18–26). The mean total scores of DCS-16 and HPV vaccination knowledge were 41.5 (SD=20.0) and 8 (SD=1.8), respectively. In terms of HPV vaccination decision, 56.1% (60/107) of the participants tended toward accepting vaccination, 13.1% (14/107) rejected the idea of vaccination, and 30.8% (33/107) were unsure about the choice.
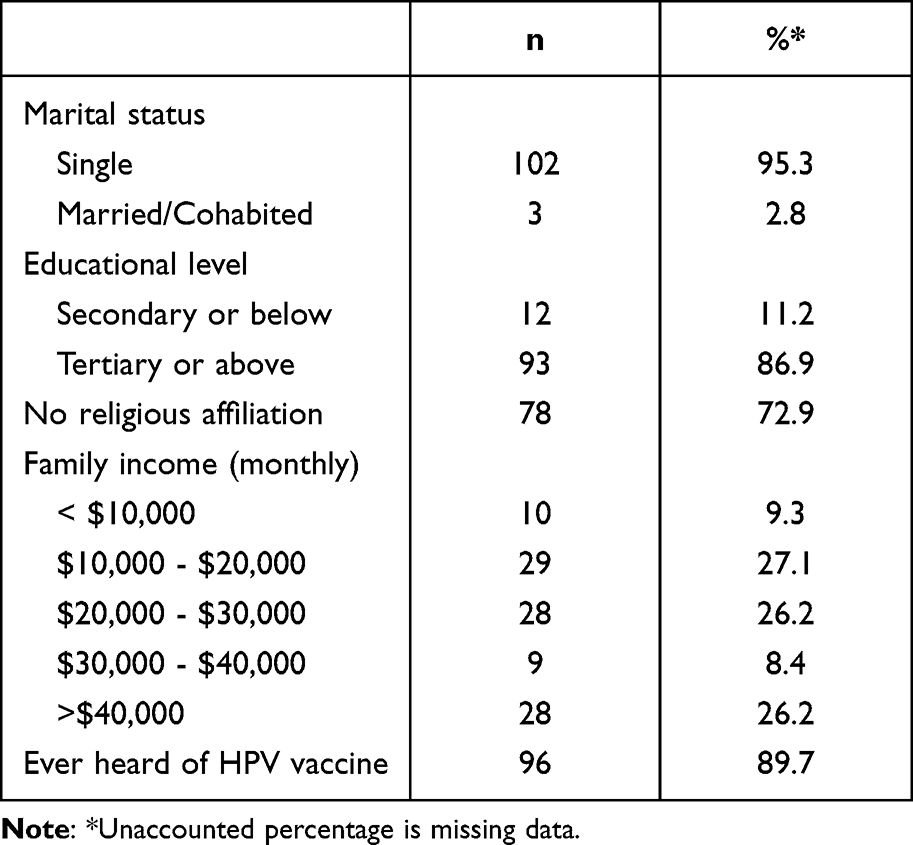 |
Table 1 Demographic Characteristics of Participants (N=107 Young Women) |
Factorial Validity
Using confirmatory factor analysis (CFA), both hierarchical and correlated five-factor models of the DCS-16 were tested. Table 2 summarizes the goodness-of-fit indices of the models, indicating both hierarchical and correlated DCS-16 5-factor models failed to meet the minimum fit criteria. Consequently, an exploratory factor analysis was performed.
 |
Table 2 Goodness-of-Fit Indices of Confirmatory Factor Analyses of the DCS |
The sampling adequacy for factor analysis was supported by the Kaiser-Meyer-Olkin (KMO) test of 0.88, exceeding the minimum adequacy level of 0.50. Bartlett’s Test of Sphericity for the significance of the correlation matrix was 1200.77 (p<0.0001), indicating appropriateness for factor analysis. Using latent root criteria with an eigenvalue >1 and scree plots to identify the optimal number of factors, exploratory factor analysis suggested a 3-factor model. As suggested by Hair et al, a factor loading cut-off of 0.55 was adopted with sample size of 100 subjects needed for significance.24 Principal component analysis (PCA) with Oblimin rotation method extracted a 3-factor model comprising 13 items (DCS-13) (Table 3). Items from Uncertainty subscale (item 11, 12) and Effective Decision subscale (item 14, 15, 16) loaded on Factor 1 (labelled Uncertainty and Effective Decision subscale). Items from Informed subscale (item 1, 2, 3) and Value Clarity subscale (item 4, 5, 6) loaded on Factor 2 (labelled Informed and Value Clarity subscale). Items from Support subscale (item 7, 8) loaded on Factor 3 (labelled Support subscale). Three items (item 9, 10 and 13) were excluded since did not load on any of the three extracted factors with cut-off above 0.55. The 3-factor model explained 70.5% of total variance, allocated across Factor 1 (45.9%), Factor 2 (18.2%), and Factor 3 (6.4%). This extracted 3-factor DCS-13 was further examined using CFA. However, the 3-factor DCS-13 again showed poor model fit (Table 2).
 |
Table 3 Exploratory Factor Analysis of Decisional Conflict Scale (DCS; Principal Components Analysis, Oblimin Rotation) |
Since both the original 5-factor DCS-16 and extracted 3-factor DCS-13 showed poor factorial validity, we next examined the short form version of the DCS which has 10 items, originally distributed across four factors.10 Both hierarchical and correlated 4-factor models of the DCS-10 were tested using CFA. The 4-factor correlated model of DCS-10 revealed a good fit to the data (CFI and TLI >0.90, RMSEA with 90% confidence interval <0.10, and SRMR <0.08; Table 2).
Reliability
Table 4 summarizes the Cronbach’s alphas for the DCS-16, DCS-13, and DCS-10 overall scales and subscales. The overall internal consistency of the three scales was high, with Cronbach’s alpha ranging from 0.86 (DCS-10) to 0.92 (DCS-16). However, the Support subscale showed consistently poor internal consistency (Cronbach’s alpha <0.70).
 |
Table 4 Reliability of Decisional Conflict Scale (DCS) |
Construct Validity
The overall scores of DCS-16, DCS-13, and DCS-10 consistently demonstrated moderate negative correlations with knowledge of HPV vaccination (correlation coefficients r ranging from −0.243 to −0.299; Table 5). Those respondents who had less knowledge about HPV vaccination had higher decisional conflict about HPV vaccination. It is noteworthy that some of the subscales showed inconsistent correlation. In the original 5-factor DCS-16 and original 4-factor DCS-10, Values Clarity subscale significantly inversely correlated to knowledge of HPV vaccination, while in the extracted 3-factor DCS-13 when Values Clarity combined with Informed subscale there was no significant correlation observed. Moreover, the Informed subscale and Support subscale consistently showed no correlation with knowledge of HPV vaccination.
 |
Table 5 Correlation Matrix for Construct Validity |
Table 6 illustrates that total DCS scores consistently significantly discriminate groups who were certain (accept/reject) from those uncertain of the decision regarding HPV vaccination. Higher scores, indicating higher decisional conflict, were observed among participants who were unsure about whether to be immunized against HPV. Similar patterns were observed with most of the subscales. The notable exception was the failure of the Informed subscale and Values Clarity subscale.
 |
Table 6 Summary of Known-Groups Comparisons |
Discussion
The psychometric properties of DCS were first evaluated in respect to preventive measures like influenza vaccination and breast cancer screening and reported to be highly reliable and valid.8 Later study also examined treatment decision-making.13,14 Our study echoed O’Conner’s work that decisional conflict in vaccination could be measured by DCS.8
The present study assessed the factorial validity, construct validity, and reliability of the Chinese version of the decisional conflict scale (DCS) measuring Chinese young women’s HPV vaccination decision conflict. Confirmatory factor analysis (CFA) revealed that the original five-factor structure of the DCS-16 poorly fitted the sample of Chinese young women. Exploratory factor analysis revealed a 3-factor 13-item of DCS model: a) Uncertainty & Effective Decision, b) Informed & Values Clarity, and c) Support, which differed from previous DCS validation studies.8,13,25,26 One explanation for these differences may lie in the difference in the type of decision to be made. Most previous studies have focused on screening and treatment of cancer, particularly breast cancer. Only O’Connor ever studied influenza vaccination decision conflict, with the decision studied being one of low-risk, unlike HPV vaccination decisions involving higher stakes and value tradeoffs. Another explanation may be the difference in ethnicity since a majority of previous studies recruited Hispanics. The only other study conducted on Hong Kong Chinese showed a similar result as ours, with items 1–6 loading onto one factor.13 This suggests that the Informed subscale (item 1–3) and Values Clarity subscale (item 4–6) is poorly differentiated among Hong Kong Chinese, most likely because both subscales assess participants’ knowledge of the options.
This is the first study that evaluated decisional conflict regarding HPV vaccination decision-making among a Chinese population. Given the suboptimal vaccination uptake rate, this study facilitates understanding of factors influencing Chinese young women’s HPV vaccination decision-making to allowing subsequent interventions to take place.
Study Limitation
The current analysis is based on an experimental study design rather than a randomized controlled trial, therefore, selection bias and some potential confounders might exist. Test-retest reliability and predictive validity were not assessed in the present study due to the cross-sectional study design. The study was also limited to small (although sufficient) sample size and Hong Kong women aged 18–26 years only. Future studies should be conducted with larger sample sizes and in different samples to further verify the validity and reliability of the decisional conflict scale.
Conclusion
In conclusion, the present study found that the total score of DCS (Chinese version) showed consistently good reliability and ability to differentiate participants who were certain vs uncertain about HPV vaccination decision. It is suggested to use the total score rather than subscores to measure Chinese young women’s HPV vaccination decisional conflict. In particular, the 4-factor 10 item DCS with 3 response options demonstrated good model fit to the data and may be a more suitable tool to quickly assess young Chinese women’s HPV vaccination decisional conflict enabling a reduced survey workload. Future studies should be considered to examine the psychometric properties of DCS (Chinese version) among other Chinese samples with larger sample size.
Abbreviations
DCS, The Decisional Conflict Scale; HPV, Human Papillomavirus; ACIP, Advisory Committee on Immunization Practices; HKU/HA HKW IRB, Hong Kong/Hospital Authority Hong Kong West Cluster; CFA, Confirmatory factor analysis; CFI, the comparative fit index; RMSEA, root mean square error of approximation; TLI, Tucker-Lewis Index; SRMR, standardized root mean square residual; EFA, exploratory factor analysis; CFA, confirmatory factor analysis; KMO, the Kaiser-Meyer-Olkin; PCA, Principal component analysis.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Funding
This study was funded by a grant from the Health and Medical Research Fund (HMRF, #12132931) of the Food and Health Bureau, the Hong Kong SAR government.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization. Human papillomavirus (HPV) and cervical cancer; 2020. Available from: http://www.who.int/mediacentre/factsheets/fs380/en/.
2. Choi HC, Leung GM, Woo PP, Jit M, Wu JT. Acceptability and uptake of female adolescent HPV vaccination in Hong Kong: a survey of mothers and adolescents. Vaccine. 2013;32(1):78–84. doi:10.1016/j.vaccine.2013.10.068
3. Li SL, Lau YL, Lam TH, Yip PS, Fan SY, Ip P. HPV vaccination in Hong Kong: uptake and reasons for non-vaccination amongst Chinese adolescent girls. Vaccine. 2013;31:5785–5788. doi:10.1016/j.vaccine.2013.10.027
4. Wang DL, Lam WWT, Fielding R. Parental decision-making with regards to vaccination against human papilloma virus in adolescent girls in Hong Kong, China: a prospective cohort study. Lancet. 2016;388(Special Issue, S78):S78. doi:10.1016/S0140-6736(16)32005-0
5. Leung JTC, Law CK. Revisiting knowledge, attitudes and practice (KAP) on human papillomavirus (HPV) vaccination among female University students in Hong Kong. Hum Vaccin Immunother. 2018;14(4):924–930. doi:10.1080/21645515.2017.1415685
6. Wang LDL, Lam WWT, Fielding R. Cervical cancer prevention practices through screening and vaccination: a cross-sectional study among Hong Kong Chinese women. Gynecol Oncol. 2015;138:311–316.
7. Lee PWH, Kwan TTC, Tam FK, et al. Beliefs about cervical cancer and human papillomavirus (HPV) and acceptability of HPV vaccination among Chinese women in Hong Kong. Prev Med. 2007;45(2):130–134. doi:10.1016/j.ypmed.2007.07.013
8. O’Connor AM. Validation of a decisional conflict scale. Med Decis Making. 1995;15(1):25–30. doi:10.1177/0272989X9501500105
9. O’Connor AM. User manual - decision conflict scale; 1993. Available from: http://decisionaid.ohri.ca/docs/develop/User_Manuals/UM_Decisional_Conflict.pdf.
10. Eastwood JA, Doering L, Roper J, Hays RD. Uncertainty and health-related quality of life 1 year after coronary angiography. Am J Crit Care. 2008;17(3):
11. Katapodi MC, Munro ML, Pierce PF, Williams RA. Testing of the decisional conflict scale: genetic testing hereditary brest, ovarian cancer. Nurs Res. 2011;60(6):368–377. doi:10.1097/NNR.0b013e3182337dad
12. Mancini J, Santin G, Chabal F, Julian-Reynier C. Cross-cultural validation of the Decisional Conflict Scale in a sample of French patients. Qual Life Res. 2006;15(6):1063–1068. doi:10.1007/s11136-005-6003-9
13. Lam WW, Kwok M, Liao Q, et al. Psychometric assessment of the Chinese version of the decisional conflict scale in Chinese women making decision for breast cancer surgery. Health Expect. 2015;18(2):210–220. doi:10.1111/hex.12021
14. Koedoot N, Molenaar S, Oosterveld P, et al. The decisional conflict scale: further validation in two samples of Dutch oncology patients. Patient Educ Counsel. 2001;45(3):187–193. doi:10.1016/S0738-3991(01)00120-3
15. Kawaguchi T, Azuma K, Yamaguchi T, et al. Development and validation of the Japanese version of the Decisional Conflict Scale to investigate the value of pharmacists’ information: a before and after study. BMC Med Inform Decis Mak. 2013;13:50. doi:10.1186/1472-6947-13-50
16. Song M-K, Sereika SM. An evaluation of the Decisional Conflict Scale for measuring the quality of end-of-life decision making. Patient Educ Counsel. 2006;61:397–404. doi:10.1016/j.pec.2005.05.003
17. Cormiers AD, Légaré F, Simard S, Boulet LP. Decisional conflict in asthma patients: a cross sectional study. J Asthma. 2015;52(10):1084–19091. doi:10.3109/02770903.2015.1047955
18. Urrutia M, Campos S, O’Connor A. Validation of a Spanish version of the Decisional Conflict Scale. Rev Med Chil. 2008;136(11):1439–1447. doi:10.4067/s0034-98872008001100010
19. Harper DM, Irons BB, Alexander NM, et al. Quantifying the decisional satisfaction to accept or reject the Human Papillomavirus (HPV) vaccine: a preference for cervical cancer prevention. PLoS One. 2014;9(2):e88493. doi:10.1371/journal.pone.0088493
20. Centers for Disease Control and Prevention USA. Vaccinating boys and girls; 2019. Available from: https://www.cdc.gov/hpv/parents/vaccine.html.
21. Bryant FB, Yarnold PR. Principal-components analysis and exploratory and confirmatory factor analysis. In: Grimm LG, Yamold PR, editors. Reading and Understanding Multivariate Statistics. Washington, DC: American Psychological Association; 1995.
22. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis: Pearson New International Edition.
23. Bland JM, Altman DG. Cronbach’s alpha. BMJ. 1997;314(7080):572. doi:10.1136/bmj.314.7080.572
24. Hair JF, Anderson RE, Tatham RL, Black WC. Multivariate Data Analysis.
25. Garvelink MM, Boland L, Klein K, et al. Decisional conflict scale use over 20 years: the anniversary review. Med Decis Making. 2019;39(4):301–314. doi:10.1177/0272989X19851345
26. Garvelink MM, Boland L, Klein K, et al. Decisional conflict scale findings among patients and surrogates making health decisions: part II of an anniversary review. Med Decis Making. 2019;39(4):315–326. doi:10.1177/0272989X19851346
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.