Back to Journals » Psychology Research and Behavior Management » Volume 18
Psychological Positive Energy in Medical Students: Framework, Influencing Factors and Mental Health Implications
Authors Li Y, Feng X, Ju W, Su Y, Cheng X, Xu T, Cui L
Received 9 April 2025
Accepted for publication 17 October 2025
Published 25 October 2025 Volume 2025:18 Pages 2207—2224
DOI https://doi.org/10.2147/PRBM.S533465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Yueqin Li,1,* Xiaofang Feng,1,* Weifang Ju,1 Yanyan Su,1 Xia Cheng,2 Tao Xu,2 Liping Cui3
1Department of General Medical, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China; 2Nursing College, Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 3Department of Nursing, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liping Cui, Department of Nursing, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, No. 99, Longcheng Street, Xiaodian District, Taiyuan, Shanxi, 030032, People’s Republic of China, Tel +8613934154909, Email [email protected]
Objective: This study aimed to explore the structure, developmental characteristics and influencing factors of psychological positive energy (PPE) in medical students as well as its relationship with mental health. Psychological positive energy refers to a positive mindset comprising optimism, emotional resilience and proactive behaviours, which contribute to overall well-being.
Methods: A mixed-methods design was adopted. Semi-structured interviews (n=650, stratified by year/gender/speciality) were analysed via grounded theory to construct a PPE framework (theoretical saturation reached). A cross-sectional survey (n=650, 562 valid) used a self-developed PPE scale (Cronbach’s α=0.89, good fit) and three validated scales. Data were analysed via SPSS 26.0 with Pearson correlation and multiple linear regression.
Results: Qualitative analysis identified a four-dimensional PPE framework: positive cognitive orientation (tendency to interpret life events optimistically), emotional feelings (experience of stable positive emotions such as hope), behavioural patterns (proactive engagement in problem-solving) and self-development (intrinsic motivation for professional/personal growth). This framework was confirmed after reaching data saturation The quantitative results showed the following: (1) Medical students’ PPE levels were high (M = 5.5– 6.0/7-point scale), with significant demographic patterns (higher in men than in women; increasing with academic seniority). (2) Perceived social support, family care and trait self-control were key predictors of PPE, collectively explaining 72.1% of its variance (with social support as the strongest predictor). (3) Psychological positive energy was positively associated with adaptive psychological outcomes (meaning in life, cognitive reappraisal) and negatively associated with mental health risks (anxiety, depression, aggression) (all p < 0.001), indicating the protective role of PPE.
Conclusion: This study clarifies the four-dimensional structure of PPE in medical students and confirms its critical protective role in mental health (eg reducing anxiety/depression). Key influencing factors – perceived social support (strongest predictor), family care and trait self-control – provide actionable targets for universities to design targeted interventions.
Keywords: psychological positive energy, medical students, influencing factors, mental health
Introduction
Conceptualisation of Psychological Positive Energy
The term “positive energy” initially emerged in the field of physics. British psychologist Richard Wiseman redefined the concept, transforming it from a physical term into one associated with human emotion. In his book Rip It Up, he described positive energy as anything that provides uplift and hope, motivates ongoing pursuit and makes life fulfilling and happy.1 Compared with its academic meaning in physics, the concept of positive energy is now more widely accepted and commonly used in psychology.2
Psychological positive energy (PPE)3 refers to an individual’s capacity to generate and sustain positive psychological states (eg, optimism, resilience, gratitude) that enhance well-being and support adaptive functioning. It encompasses emotional, cognitive and behavioural dimensions, aligning with the broaden-and-build theory and frameworks within positive psychology.4 In this study, PPE is conceptualised as a multidimensional construct that integrates trait-like components (eg, stable optimism as a long-term personal quality), state-like features (eg, context-dependent positive psychological states triggered by specific situations) and transient emotional experiences (eg, momentary feelings of hope or gratitude). This operationalisation reflects the dynamic nature of PPE, capturing both its stable and situational aspects to better align with the complexity of positive psychological functioning in medical students. In psychology, PPE is expressed in various ways: as positive emotional experiences,2 as an inherent trait or mental state5,6 and through spoken words and outward actions that benefit others.2 Research suggests that PPE may serve as a protective factor against mental health conditions such as anxiety, depression and stress. For instance, positive emotions – a core component of PPE – have been shown to promote psychological well-being and alleviate mental health difficulties.7 A study by Fredrickson4 indicates that positive emotions are associated with a broadened mindset, which enhances resilience and adaptive coping strategies. Given the potential mental health benefits of PPE, understanding how it is cultivated and its subsequent impact is crucial.
Research Gaps in PPE Measurement
Currently, research on the comprehensive measurement of PPE remains limited. Existing PPE-related scales have critical limitations: Lu Hongzhen’s8 questionnaire focuses only on the “awareness and cultivation status” of PPE, not its structural dimensions; Ren Qihan’s6 study lacks a standardised measurement tool. Other relevant scales9 assess overlapping constructs but omit PPE’s behavioural and self-development dimensions. Thus, a new scale tailored to medical students is necessary to capture PPE comprehensively. This gap is critical because, without a clear framework, it is impossible to accurately assess PPE in high-stress groups such as medical students or to identify targeted strategies to enhance their PPE. As a result, existing research cannot effectively guide mental health interventions for this population, which highlights the need for the present study.
Medical students are particularly vulnerable to high levels of academic and emotional stress,10 making them a key population for the study of PPE. Their unique stressors (eg, clinical training pressure) may interact with PPE to affect mental health, highlighting the need to explore PPE in this group. Their rigorous training often results in burnout, anxiety and depression, which can substantially affect their mental health and overall well-being.11 Research has shown that positive psychological states such as optimism and resilience – core components of PPE – can serve as protective factors against mental health issues. A study by Mamyrova et al12 found that medical students with higher levels of positive psychological capital (including optimism and resilience) reported lower levels of burnout and depression. Therefore, cultivating PPE in medical students is essential to help them better manage these challenges and maintain resilience.
Rationale for Focusing on Medical Students
The university setting plays a pivotal role in fostering PPE, as it is where medical students’ daily experiences (eg, academic interactions, campus culture) primarily occur, serving as the primary environment for fostering PPE. Chen et al13 emphasise the importance of integrating positive psychology into educational curricula, highlighting how such courses can offer students cognitive experiences of PPE that contribute to personal growth and self-worth. Moreover, a positive environmental atmosphere, including a harmonious and united campus culture, can enhance the development of PPE.12
In addition, demographic characteristics (eg, gender and age) can influence PPE development; for example, female medical students may report different PPE levels due to gender-specific stressors, which, in turn, affects intervention effectiveness.14,15 Moreover, social discourse and cultural values (eg, collective well-being in China) shape PPE by defining societal expectations for positive behaviours, creating a context that interacts with demographic factors to influence PPE in medical students.16 In China, for instance, universities play a crucial role in guiding public opinion and promoting a positive social environment, which is vital for students’ mental health.16 This context underscores the relevance of studying PPE in medical students within a university setting.
This study is guided by the frameworks of positive psychology and social cognitive theory. Positive psychology emphasises the importance of fostering individual strengths and virtues, suggesting that PPE plays a vital role in enhancing mental well-being.17 Social cognitive theory highlights the interaction between individuals and their social environments, which is essential for understanding how PPE develops and is sustained. The influence of external factors, such as social discourse and the educational environment, is particularly great in this context.18 For example, a supportive social environment can strengthen individual resilience, whereas a positive educational atmosphere can nurture PPE in students. These external influences form critical components of the study’s framework, positioning the research within a broader social and educational context.
Study Objectives and Hypotheses
The existing literature on PPE has largely focused on isolated aspects, such as emotional traits or cognitive orientations. However, a comprehensive framework for understanding PPE – particularly in medical students – is lacking. Although previous studies have examined individual factors influencing mental health, few have connected PPE to a multidimensional framework that addresses both personal development and mental health outcomes. Psychological positive energy is a referential term that represents valuable spiritual qualities and virtues; however, its specific cultivation strategies have typically been explored at a macro level.
Based on the literature, this study proposes the following hypotheses:
H1: Psychological positive energy in medical students consists of multiple dimensions (derived from qualitative analysis). H2: Medical students’ PPE levels differ by gender and grade (men > women; final year > first year). H3: Perceived social support, family care and trait self-control positively predict PPE. H4: Psychological positive energy is positively correlated with adaptive outcomes (eg meaning in life) and negatively correlated with mental health risks (eg, anxiety).
This study aims to address the abovementioned gap in the existing literature on PPE by developing a comprehensive framework of PPE in medical students, exploring its developmental characteristics, influencing factors and relationship with mental health. Prior research has shown that perceived social support,19 family care20 and trait self-control21 are important variables that can influence psychological well-being. For instance, social support has been identified as a key protective factor against stress and mental health difficulties,19 whereas family care can offer a stable and nurturing environment that promotes resilience.20 Trait self-control, meanwhile, has been linked to improved emotional regulation and adaptive coping strategies.21 Given that PPE encompasses optimism, resilience and proactive behaviours, it is essential to examine how these factors interact with PPE and, in turn, influence mental health.
The quantitative component of this study examines how perceived social support, family care and trait self-control predict PPE and its correlation with mental health, whereas qualitative interviews offer deeper insight into students’ lived experiences. The findings can inform educational policies and practices, supporting universities in fostering positive and supportive environments that enhance psychological well-being. Moreover, the development of tailored interventions based on PPE cultivation could offer a practical means of improving students’ mental health and resilience, particularly in high-stress fields such as medicine.
Study Participants and Methods
Study Participants
This study was conducted between March and August 2023. Data collection for semi-structured interviews (qualitative component) occurred between March and June 2023, and the questionnaire survey (quantitative component) was administered between July and August 2023. Medical students from different academic years (first year to final year) were selected using proportional sampling: the number of participants in each year group was determined based on the university’s official year-group distribution (first year 23%, second year 31%, third year 30%, final year 16%), and specific participants within each year group were selected through random sampling to ensure representativeness. Participants were contacted via the education office and their academic advisors to ensure effective communication. Incentives in the form of research memorabilia were provided to those who participated in the survey to encourage involvement. The inclusion criteria were as follows: (1) medical students who volunteered to participate; (2) students without serious physiological or psychological disorders and with the literacy skills to complete the questionnaire assessment independently. This study was approved by the hospital ethics committee, and all participants provided informed consent.
Study 1: Qualitative Development of the PPE Framework
This study adopted an exploratory sequential mixed-methods design, where qualitative and quantitative components were integrated in a sequential and complementary manner.22 The qualitative component (semi-structured interviews) was conducted first to explore and inductively construct the dimensional framework of PPE, whereas the quantitative component (questionnaire survey) subsequently validated this framework, analysed its developmental characteristics and examined its relationships with influencing factors and mental health outcomes. This design ensured that the theoretical insights from the qualitative data directly informed the measurement and analysis of the quantitative phase.
Investigation of the PPE Framework in Medical Students
Qualitative data on PPE among medical students were collected through one-on-one semi-structured interviews with a total of 650 participants. These 650 participants constituted the entire qualitative sample, covering all year groups (first year to final year), both genders and the major medical disciplines. The sample size was determined based on the principle of data saturation – no new dimensions or categories emerged after the 620th interview, confirming that theoretical saturation had been reached. Sampling was halted when data saturation was achieved, confirming that this sample size sufficiently captured the range of perspectives needed to construct the PPE framework. The interviews comprised a total of 12 questions, which were selected to ensure a comprehensive exploration of the key dimensions of PPE while maintaining a manageable interview length. Details of the interview questions are provided in Appendix 1. Notably, the questions were designed to elicit concrete lived experiences rather than general opinions. For instance, instead of asking in an abstract way about optimism, questions focused on specific scenarios: “Can you recall a time when you faced academic failure (eg, a low exam score) and responded with a positive attitude?” “What thoughts or actions characterised your response, and how did you feel afterwards?” This design aligns with grounded theory’s emphasis on deriving insights from participants’ actual experiences, ensuring the resulting framework is rooted in real-world contexts. Interviews were conducted in private settings to ensure confidentiality and lasted approximately 30–40 minutes. A purposive sampling method was used to select participants from diverse academic years, genders and psychological well-being statuses, ensuring a broad range of perspectives.
Qualitative data from the semi-structured interviews were analysed using the comprehensive analytical techniques summarised by Sun et al,23 based on grounded theory. Specifically, we adopted Strauss and Corbin’s version of grounded theory, which is rooted in a constructivist epistemology. This perspective holds that knowledge is not fixed but emerges through social interactions and contextual experiences, making it well suited to exploring dynamic constructs such as PPE. This epistemological stance aligns with our focus on understanding PPE as a context-dependent phenomenon shaped by medical students’ unique academic, clinical and interpersonal environments. Unlike approaches that impose predefined theoretical frameworks, Strauss and Corbin’s method allows categories to emerge inductively from participants’ narratives, ensuring the resulting PPE framework is grounded in their lived experiences, which emphasises a systematic three-stage coding process (open, axial and selective coding) to develop theoretical constructs. Open coding example: From the interview statement “When I encountered difficulties in clinical practice, I always thought about how to solve them instead of complaining”, the initial concept of “problem-oriented thinking” was extracted, which was then categorised under “positive cognitive orientation”. Axial coding example: The concept of “active help-seeking from peers” (from behavioural descriptions) was linked to “emotional stability when facing pressure” (from emotional expressions) to form the axial category “behavioural–emotional interaction in stress response”. Selective coding example: The core category of “adaptive development of PPE” was identified, integrating all four dimensions (positive cognitive orientation, emotional feelings, behavioural patterns, self-development) as interconnected elements. All interviews were initially transcribed verbatim, and the data were manually coded to identify patterns and themes. The coding process was iterative, with initial codes grouped into broader categories and later refined into themes. To ensure methodological rigor, several strategies were implemented: intercoder reliability was assessed by having a second researcher independently code 15% of the interviews (n = 98), yielding an agreement rate of 82%; discrepancies were resolved through discussion to ensure coding consistency. Additionally, data saturation was verified by analysing 30 additional interviews after the 620th interview, with no new dimensions or categories emerging, confirming the stability of the identified framework. Methodological triangulation was employed by cross-referencing qualitative themes (eg, descriptions of proactive problem-solving in interviews) with preliminary quantitative findings from pilot surveys (eg, high scores on behavioural pattern items), enhancing the validity of the results. Finally, an audit trail was maintained, documenting all coding decisions, memos and revisions to ensure transparency and reproducibility of the analytical process.
Participants for the semi-structured interviews were selected according to the principle of data saturation. In qualitative research, saturation is reached when no new themes or information emerge from additional interviews. Based on prior studies and the complexity of the research questions, the sample size was deemed sufficient to achieve data saturation.
Study 2: Quantitative Validation of the PPE Scale
For the quantitative component, a sample size of 650 questionnaires was determined based on the proportion of medical students across different academic years. This proportional sampling approach ensured that each year group was adequately represented, reflecting the overall student population. Proportional sampling was implemented based on the official year-group distribution of the target university, where first-year, second-year, third-year and final-year students accounted for approximately 23%, 31%, 30% and 16% of the total medical student population, respectively. This sampling strategy aimed to ensure the sample’s representativeness of the real population structure. Within each year group, participants were randomly selected to avoid selection bias, ensuring the sample reflected the overall population structure. Specifically, random selection was conducted using a computer-generated random number sequence: all eligible students in each year group were assigned unique identifiers, and participants were selected by randomly drawing these identifiers until the target sample size for the year group was achieved. This method ensured equal probability of selection for all students in each year group. A power analysis was conducted; based on an expected medium effect size (Cohen’s f² = 0.15), a significance level of 0.05 and a power of 0.80, the analysis indicated that a minimum of 129 participants was required. The final sample size of 650 exceeded this threshold, ensuring adequate statistical power. The survey was administered online to facilitate easy access and completion. It required approximately 15–20 minutes to complete.
Questionnaire for PPE in Medical Students
An author-developed questionnaire was used to assess PPE in medical students, comprising four dimensions: positive cognitive orientation, positive emotional feelings, positive behavioural patterns and self-development. It employed a 7-point Likert scale and contained 51 items, detailed in Appendix 2. First, the dimensions were clearly defined on the first page of the questionnaire as follows: (1) positive cognitive orientation: an individual’s habitual positive, optimistic and constructive way of perceiving and interpreting events, such as seeing growth opportunities in difficulties; (2) positive emotional feelings: the experience of positive emotions, such as joy, happiness and hope in daily life, reflecting overall emotional well-being; (3) positive behavioural patterns: actions beneficial to physical and mental health, social relationships and personal development, such as regular exercise and healthy eating; (4) positive self-development: an individual’s continuous self-improvement efforts, including skill and knowledge development and goal-oriented actions for self-actualisation. The questionnaire was designed based on established theories and expert consultation. After drafting the initial items based on the qualitative framework, the questionnaire was reviewed by five experts (three professors in medical education and two associate professors in clinical psychology) to assess content validity. The experts rated the relevance of each item to the PPE dimensions, with a content validity index (CVI) of 0.92. Six items with low relevance (CVI < 0.8) were revised based on expert feedback, focusing on clarifying ambiguous phrases (eg replacing “positive attitude” with “specific positive coping behaviours in clinical scenarios”). To streamline the logic of validity assurance, the three key steps in the development process and the comprehensive validity evaluation were integrated as follows: First, cognitive interviews were conducted with 10 medical students to assess item comprehension, leading to revisions of eight ambiguous phrases. Second, a pilot study was administered to 80 medical students (not in the final sample), with item–total correlations used to remove seven items with low discriminability. Third, factor analysis was performed: exploratory factor analysis (EFA) with 200 participants extracted four factors (eigenvalues >1) explaining 67.2% of the variance, and confirmatory factor analysis (CFA) with 362 participants confirmed good model fit (χ²/df = 2.31, CFI = 0.92, RMSEA = 0.05). These results, together with the theoretical alignment with the qualitative framework and expert consultation (CVI = 0.92), comprehensively verified the questionnaire’s content validity and construct validity (construct validity confirmed by EFA [factor loadings > 0.6, four factors explaining 67.2% of the variance] and CFA [χ²/df = 2.31, CFI = 0.92, RMSEA = 0.05]), indicating that the scale structure matches the theoretical framework. Prior to factor analysis, the questionnaire underwent two key optimization steps to ensure item quality: first, cognitive interviews with 10 medical students were conducted to revise 8 ambiguous items (eg, specifying “positive attitude” as “specific coping behaviours in clinical settings”); second, a pilot study was administered to 80 medical students (not in the final sample), and 7 items with low item–total correlations (<0.3) were removed. Additionally, the questionnaire showed high internal consistency: the overall Cronbach’s α coefficient was 0.965, with α coefficients for the four dimensions ranging from 0.869 (positive self-development) to 0.930 (positive behavioural patterns), all exceeding the acceptable threshold of 0.7. No statistically significant differences were observed in the scores for PPE and its four dimensions across different year groups, confirming the questionnaire’s consistent applicability. In this study, the questionnaire showed high internal consistency: the internal consistency coefficient for the overall questionnaire was 0.965. The internal consistency coefficients for the four dimensions – positive cognitive orientation, positive emotional feelings, positive behavioural patterns and positive self-development – were 0.924, 0.916, 0.930 and 0.869, respectively, all exceeding the acceptable threshold of 0.7 for internal consistency.
Exploration of Influencing Factors of PPE
To explore the factors influencing the formation and development of PPE among medical students, a questionnaire survey was conducted using the Perceived Social Support Scale (Cronbach’s alpha [α]: 0.88),19 the Family APGAR Scale (Cronbach’s α: 0.84)23 and the Self-Control Scale for Medical Students (Cronbach’s α: 0.88).21 These scales were selected to test H3 (“Perceived social support, family care and trait self-control positively predict PPE”). Specifically, the Perceived Social Support Scale19 was chosen because social support provides external resources that foster positive psychological states, which aligns with our focus on contextual factors influencing PPE. The Family APGAR Scale24 was selected to measure family care, as family functioning is a key environmental factor that shapes psychological traits in young adults, which is directly relating to PPE development. The Self-Control Scale for Medical Students21 was used because self-control is linked to proactive behaviours (a core dimension of PPE), making it a critical personal predictor of PPE. The Perceived Social Support Scale has been widely validated across various populations, including students, to assess social support.25 The Family APGAR Scale – measuring adaptation, partnership, growth, affection and resolve – has been used extensively to evaluate family functioning and its impact on psychological well-being, especially in educational contexts.26 The Self-Control Scale for Medical Students has been validated for use in this specific population to assess traits related to behavioural regulation and self-discipline.21
Exploration of Mental Health
To examine the relationship between PPE and mental health, five representative mental health factors were selected: the sense of meaning in life, emotion regulation strategies, anxiety, depression and aggressive behaviour. A questionnaire survey was utilised, incorporating the Cognitive Reappraisal Strategy Questionnaire (Cronbach’s α: 0.73),27 the Meaning in Life Questionnaire (Cronbach’s α: 0.9),28 the Self-Rating Anxiety Scale (Cronbach’s α: 0.85),29 the Self-Rating Depression Scale (Cronbach’s α: 0.82)30 and the Proactive–Reactive Aggression Questionnaire (Cronbach’s α: 0.75)31 to assess the mental health status of the medical students who participated in this study. These tools were selected to test H4, which explores the relationship between PPE and mental health outcomes. Specifically, the Cognitive Reappraisal Strategy Questionnaire27 and the Meaning in Life Questionnaire28 were chosen because they measure adaptive outcomes (cognitive reappraisal, life meaning) that are hypothesised to correlate positively with PPE, as they reflect psychological resilience. The Self-Rating Anxiety Scale29 and the Self-Rating Depression Scale30 were selected due to their wide use in assessing mental health risks in medical students,12 aligning with our focus on negative outcomes hypothesised to correlate negatively with PPE. The Proactive–Reactive Aggression Questionnaire31 was chosen to measure interpersonal difficulties, which are a potential indicator of low PPE in high-pressure academic environments.
The Cognitive Reappraisal Strategy Questionnaire was selected due to the central role of emotion regulation, particularly in medical students who often experience substantial stress.8,11 The Meaning in Life Questionnaire was included to assess how a sense of purpose may offer protection against mental health challenges in this population.32 The Self-Rating Anxiety Scale and Self-Rating Depression Scale are widely validated in student populations and are effective tools for measuring stress-related psychological issues.10 Lastly, the Proactive–Reactive Aggression Questionnaire was employed to assess aggression,33 which is pertinent for understanding interpersonal and emotional difficulties in high-pressure academic environments.
Informed consent was obtained from all participants prior to data collection, with clear explanations provided regarding the study’s purpose and procedures. Confidentiality was maintained by the anonymisation of all personal data. Participants were assured that their involvement was voluntary and that they could withdraw at any time without consequence.
Statistical Methods
For data processing, SPSS 26.0 software (IBM, Armonk, NY, USA) was used. Quantitative data following normal distribution were expressed as mean ± standard deviation, whereas count data were expressed as frequency (rate) (n [%]). Prior to conducting the parametric tests, the assumption of normality was tested using the Shapiro–Wilk test, and homogeneity of variance was assessed using Levene’s test. If either assumption was violated, non-parametric alternatives were considered.
The independent samples t-test was used for intergroup comparisons of the quantitative data, specifically to compare means between two groups, such as gender differences in PPE scores. For multigroup comparisons, analysis of variance (ANOVA) was performed, followed by Bonferroni post hoc tests to adjust for multiple comparisons when significant differences were detected. To compare PPE scores across different year groups, ANOVA was applied.
Pearson correlation analysis and multiple linear regression analysis were conducted to examine relationships between variables.34 Pearson correlation was used to assess the strength and direction of linear relationships between PPE, its dimensions and other variables such as perceived social support and mental health indicators. Multiple linear regression analysis was used to evaluate the combined and unique predictive power of variables (perceived social support, family care, and trait self-control) on PPE and its dimensions, with all three predictor variables included simultaneously in the regression model to account for potential overlapping explained variance among them. The adjusted R-squared value was reported to indicate the proportion of variance explained by the predictor variables in the regression models. The significance level was set at α = 0.05.
Results
Study 1: Qualitative Results of the PPE Framework
Qualitative research was conducted following a rigorous grounded theory methodology, which involved an iterative process of open coding, axial coding and selective coding.35 This study adopted Strauss and Corbin’s constructivist version of grounded theory, which emphasises knowledge co-construction through interactions between researchers’ and participants’ lived experiences.26 A total of 650 medical students (covering all year groups, genders and major medical disciplines) were included in the qualitative sample. The sample size was determined by data saturation – no new dimensions or categories emerged after the 620th interview, and 30 additional interviews confirmed theoretical saturation. The analytical process followed three-stage coding: (1) open coding extracted 327 initial concepts (eg, “problem-oriented thinking” from clinical failure scenarios); (2) axial coding integrated these into 12 categories (eg, “behavioural–emotional interaction in stress response”); (3) selective coding identified the core category of “adaptive development of PPE”, integrating the four dimensions. Methodological rigor was ensured by inter-coder reliability (82% agreement on 15% of interviews, n = 98) and triangulation with preliminary quantitative pilot data (eg, consistency between interview themes of “proactive problem-solving” and high scores on behavioural pattern items in pilot surveys). This approach allowed us to identify a comprehensive framework of PPE in medical students, as depicted in Figure 1. The framework is structured around four primary dimensions: positive cognitive orientation, positive emotional feelings, positive behavioural patterns and positive self-development.
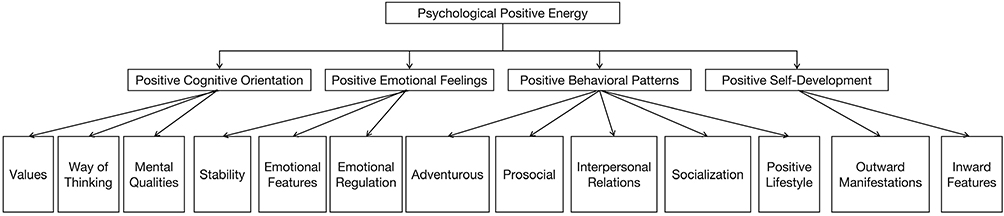 |
Figure 1 The Framework of PPE in Medical Students. |
Each dimension is further elaborated with specific coding categories that capture the essence of PPE in medical students (as shown in Table 1). The positive cognitive orientation dimension encompasses 11 categories that reflect values, mental qualities, stability and emotional features. These include “altruistic orientation”, “awareness of the bigger picture”, “positive transmission”, “alignment with social culture”, “openness and flexibility”, “independence”, “positive thinking patterns”, “responsibility”, “gratitude”, “hope” and “kindness”.
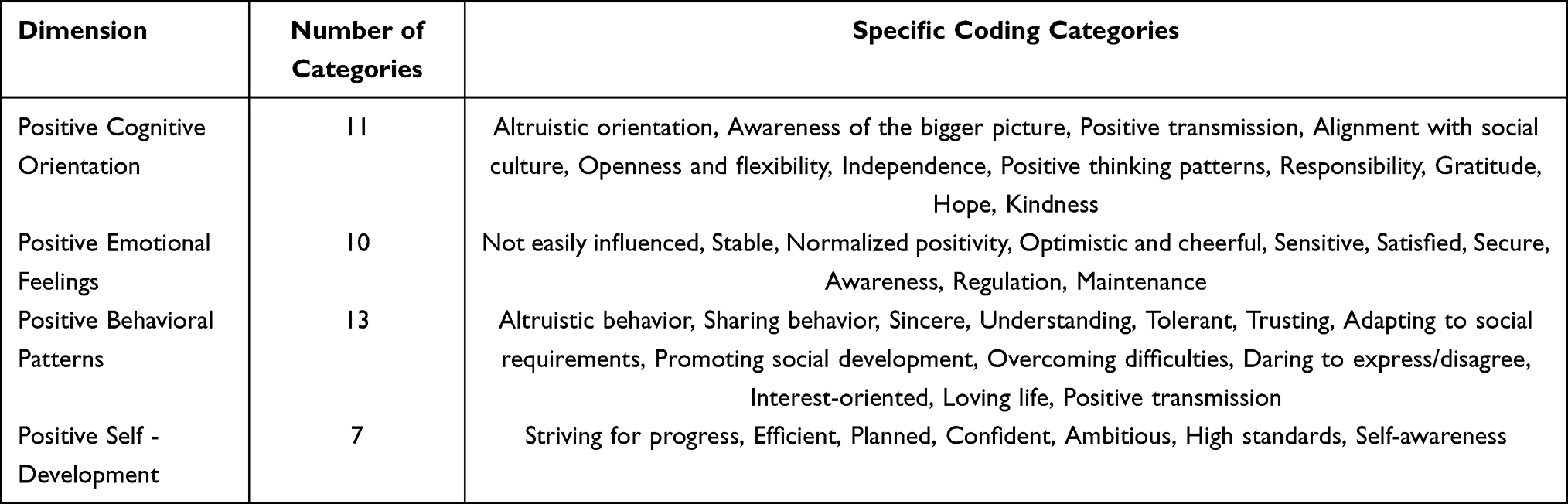 |
Table 1 Coding Categories for Each Dimension |
The positive emotional feelings dimension is characterised by 10 categories that highlight emotional regulation and adventurousness. These categories are “not easily influenced”, “stable”, “normalised positivity”, “optimistic and cheerful”, “sensitive”, “satisfied”, “secure”, “awareness”, “regulation” and “maintenance”.
The positive behavioural patterns dimension includes 13 categories that illustrate prosocial and interpersonal relations. These categories are “altruistic behaviour”, “sharing behaviour”, “sincerity” “tolerance” “trust”, “adapting to social requirements”, “promoting social development”, “overcoming difficulties”, “daring to express/disagree”, “interest-oriented”, “loving life” and “positive transmission”.
Finally, the positive self-development dimension is composed of seven categories that represent socialisation, positive lifestyle, outward manifestations and inward features. These categories include “striving for progress”, “efficiency” “planning” “confidence”, “ambitious”, “high standards” and “self-awareness”. Through selective coding, the core category “adaptive development of PPE” was identified, integrating these four dimensions as dynamically interconnected components. Positive cognitive orientation forms the foundation for interpreting experiences optimistically, which, in turn, shapes stable positive emotional feelings. These emotional states drive proactive behavioural patterns, such as seeking solutions or supporting peers, whereas consistent engagement in such behaviours fosters self-development – reinforcing cognitive optimism in a reciprocal cycle. This theoretical framework reflects how PPE evolves through interaction with academic challenges, clinical experiences and social contexts, aligning with the inductive logic of grounded theory.
Study 2: Quantitative Results
General Data
As shown in Table 2, the questionnaire was distributed and collected via an online platform targeting medical students. A total of 650 questionnaires were completed. After review, 88 were excluded due to response patterns indicating carelessness, such as inconsistent or contradictory answers, and patterns, such as straight-lining (selecting the same response for all questions). This resulted in 562 valid questionnaires, yielding a response rate of 86.46%. The mean age of the participants was 21.01 ± 1.54 years, with 237 men accounting for 42.17%. The year-group distribution was as follows: 131 first-year (23.31%), 174 second-year (30.96%), 167 third-year (29.72%) and 90 final-year (16.01%) students. This distribution is consistent with the official year-group proportion of medical students in the target university, confirming the representativeness of the sample in reflecting the actual population structure. All year-group sample sizes exceeded the minimum threshold for ANOVA and regression analyses (n > 30 per group) and were supported by the overall power analysis (total sample n = 650 > required 129), ensuring statistical robustness.
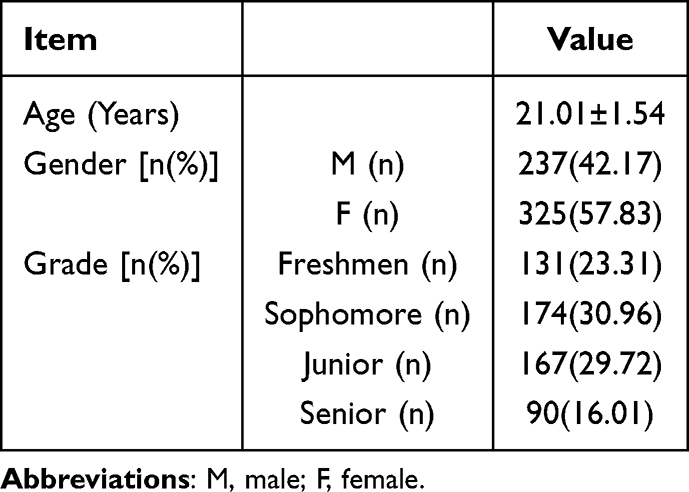 |
Table 2 General Data of the Study Population |
Psychometric Properties of the Researcher-Developed PPE Questionnaire
To ensure the reliability and validity of the measurement tool for subsequent analyses, the researcher-developed PPE questionnaire underwent rigorous psychometric testing. For content validity, expert reviews (three professors of medical education and two associate professors of clinical psychology) confirmed high item relevance to PPE dimensions (CVI = 0.92), with 6 items (CVI < 0.8) revised to clarify ambiguity (eg, replacing “positive attitude” with “specific positive coping behaviours in clinical scenarios”). For construct validity, EFA (200 participants) extracted 4 factors (eigenvalues >1, 67.2% variance explained, loadings >0.6) matching the four-dimensional structure, and CFA (362 participants) showed good fit (χ²/df=2.31, CFI=0.92, RMSEA=0.05). The questionnaire also had high internal consistency (overall Cronbach’s α=0.965; dimensional α=0.869–0.930, all >0.7), confirming its reliability and validity for subsequent quantitative analyses.
Developmental Characteristics of PPE
Descriptive Analysis of PPE and Its Variables in Medical Students
Table 3 shows a good overall level of PPE and its dimensions among medical students, with mean scores ranging from 5.5 to 6.0. The scores for perceived social support, the degree of family care and trait self-control were 5.358 ± 0.977, 6.493 ± 1.340 and 3.338 ± 0.724, respectively, indicating a satisfactory overall level.
 |
Table 3 Descriptive Analysis of PPE and Variables in Medical Students |
Development Characteristics of PPE in Medical Students
Table 4 indicates statistically significant gender differences in the total average score of PPE and the scores for each dimension. The total PPE score was 6.02 ± 0.60 vs 5.76 ± 0.46 (t = 5.712, p < 0.001); positive cognitive orientation: 5.95 ± 0.74 vs 5.80 ± 0.73 (t = 2.367, p = 0.018); positive emotional feelings: 5.85 ± 0.80 vs 5.50 ± 0.77 (t = 5.270, p < 0.001); positive behavioural patterns: 6.23 ± 0.77 vs 5.89 ± 0.68 (t = 5.554, p < 0.001); and positive self-development: 5.92 ± 0.71 vs 5.69 ± 0.72 (t = 3.731, p = 0.001).
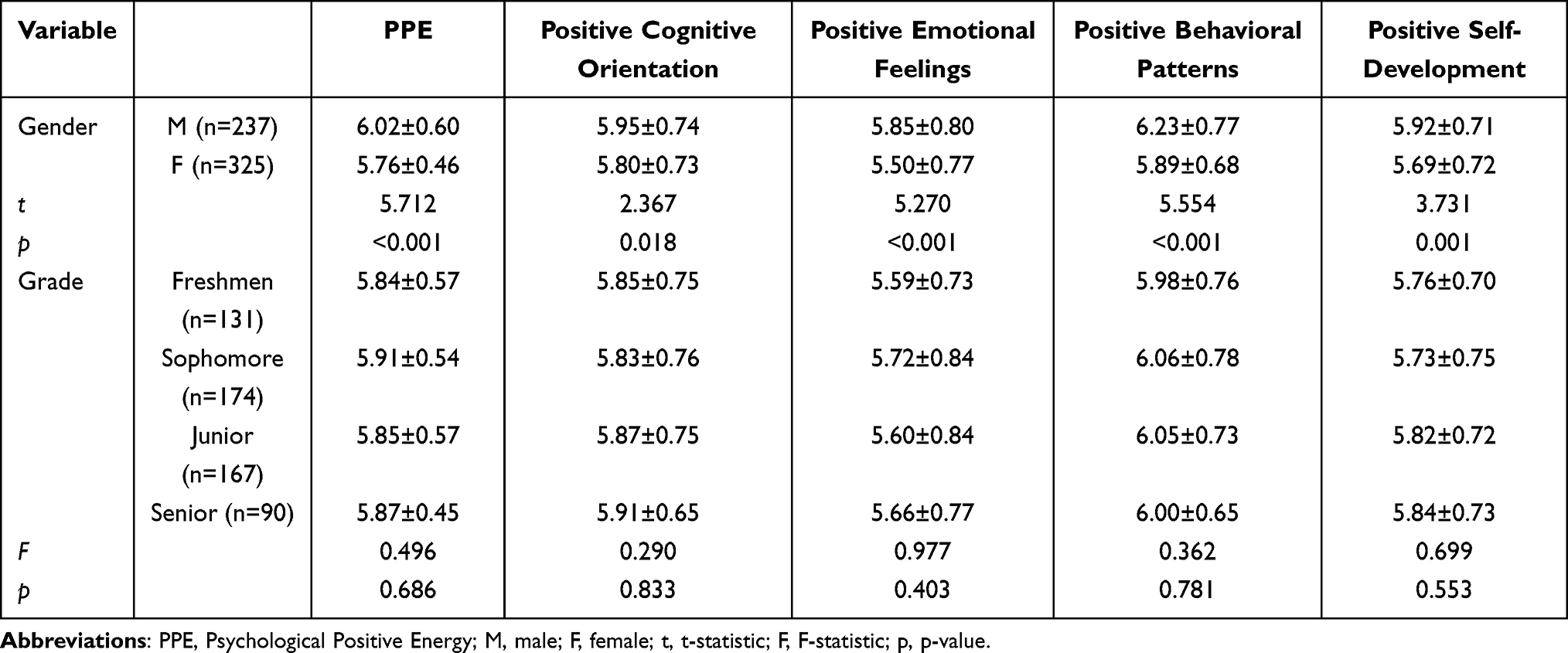 |
Table 4 Analysis of Differences in PPE Levels Between Medical Students by Genders and Grades |
Regarding the differences between year groups, no statistically significant differences were observed in the scores for positive psychological energy, positive cognitive orientation, positive emotional feelings and positive behaviour patterns.
Influencing Factors of PPE
Correlation Analysis of PPE and Its Variables in Medical Students
Table 5 shows the results of the Pearson correlation analysis between PPE and its four dimensions, as well as perceived social support and its dimensions, family care and trait self-control. The analysis revealed significant positive correlations between PPE and its four dimensions and perceived social support, family care and trait self-control (p < 0.05).
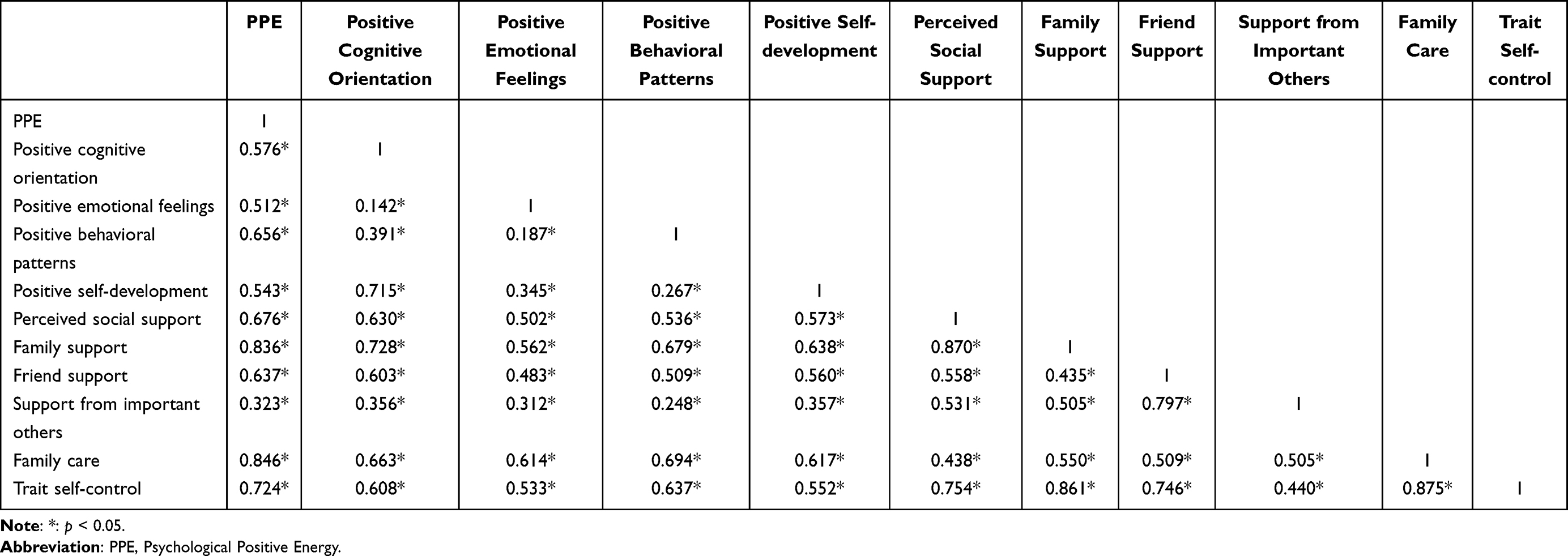 |
Table 5 Correlation Analysis of PPE with Perceived Social Support, Family Care and Trait Self-Control in Medical Students |
Regression Analysis of PPE in Medical Students and Various Variables
Multiple linear regression analyses were performed to evaluate the predictive roles of perceived social support, family care and trait self-control in PPE and its dimensions (positive cognitive orientation, positive emotional feelings, positive behavioural patterns and positive self-development) among medical students.
As shown in Table 6, the combined effect of the three predictors significantly explained the variance in all outcomes. For the total PPE score, the regression model accounted for 72.1% of the variance (f = 480.734, p < 0.001). For positive cognitive orientation, the predictors explained 46.0% of the variance (f = 158.705, p < 0.001). The model for positive emotional feelings explained 37.8% of the variance (f = 113.051, p < 0.001). For positive behavioural patterns, 49.3% of the variance was accounted for by the predictors (f = 180.894, p < 0.001). In the regression model for positive self-development, the three predictors collectively explained 39.2% of the variance (f = 119.766, p < 0.001).
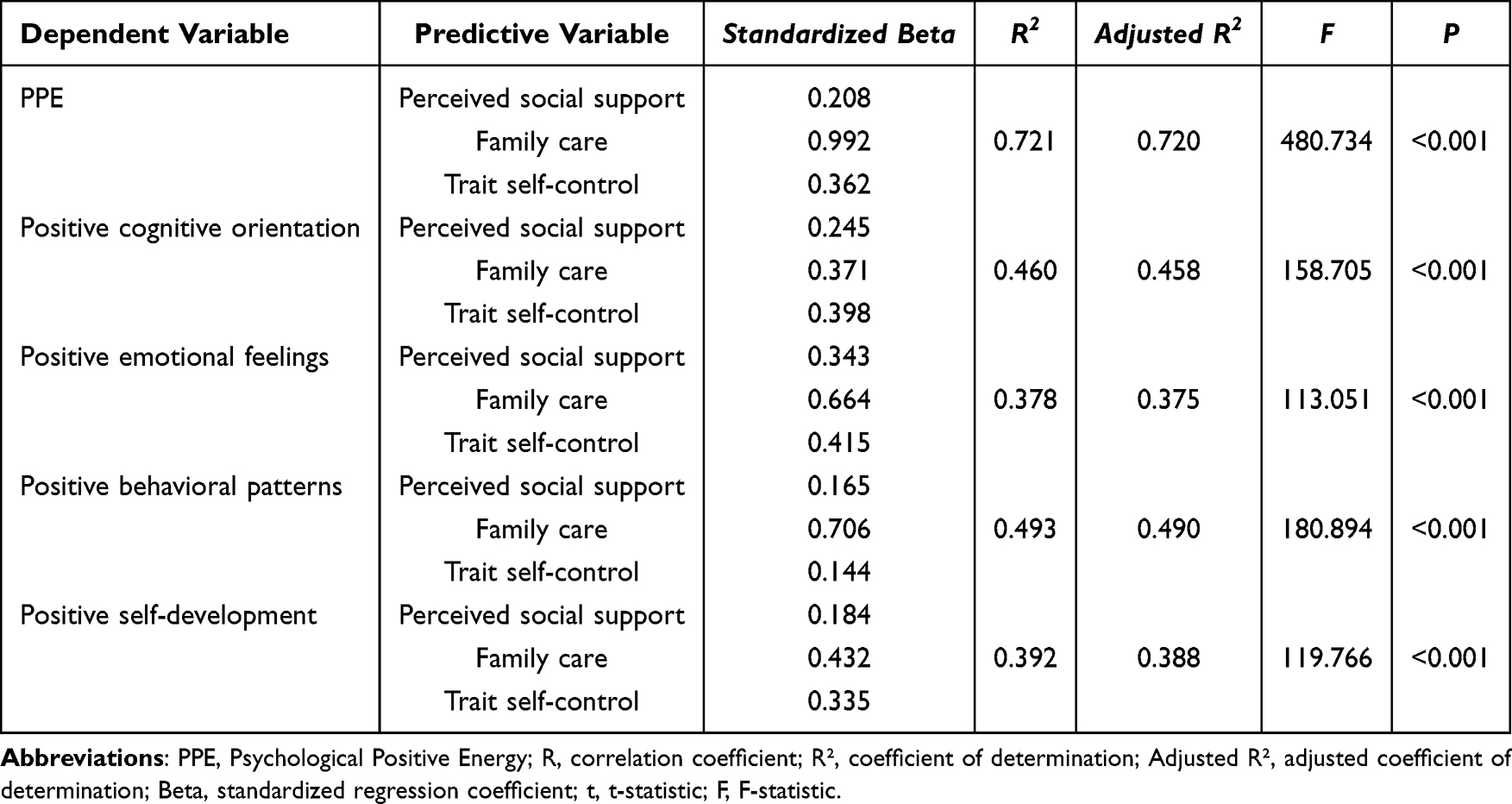 |
Table 6 Regression Analysis of PPE and Variables in Medical Students |
These findings indicate that perceived social support, family care and trait self-control jointly predict PPE and its dimensions in medical students.
Relationship Between PPE and Mental Health in Medical Students
Descriptive Analysis of PPE and Mental Health Variables in Medical Students
Table 7 shows a good overall level of the sense of meaning in life (5.117 ± 0.847) and cognitive reappraisal strategies (5.466 ± 0.785) among medical students. The standardised mean scores for anxiety and depression were 41.450 ± 7.712 and 48.021 ± 8.137, respectively, indicating well-controlled levels of anxiety and depression (the normal cut-off value for standard scores in the Chinese norm is 50). The mean scores for reactive and proactive aggression were 2.788 ± 1.031 and 1.817 ± 0.696, respectively, indicating low levels of aggression.
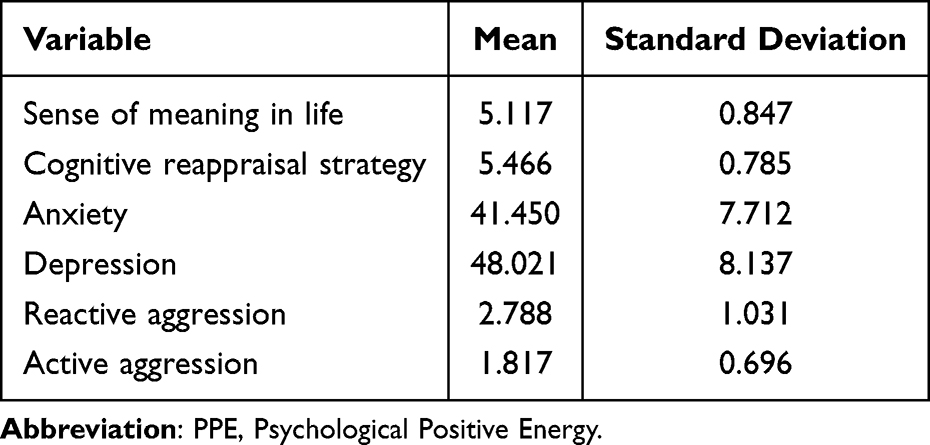 |
Table 7 Descriptive Analysis of PPE and Mental Health Variables in Medical Students |
Correlation Analysis of PPE and Mental Health Variables in Medical Students
As shown in Table 8, Pearson correlation analysis between PPE and its four dimensions and the sense of meaning in life, cognitive reappraisal strategies, anxiety, depression and aggressive behaviour revealed that PPE and its four dimensions were significantly positively correlated with the sense of meaning in life and cognitive reappraisal strategies (p < 0.05) and significantly negatively correlated with anxiety, depression and aggressive behaviour (p < 0.05).
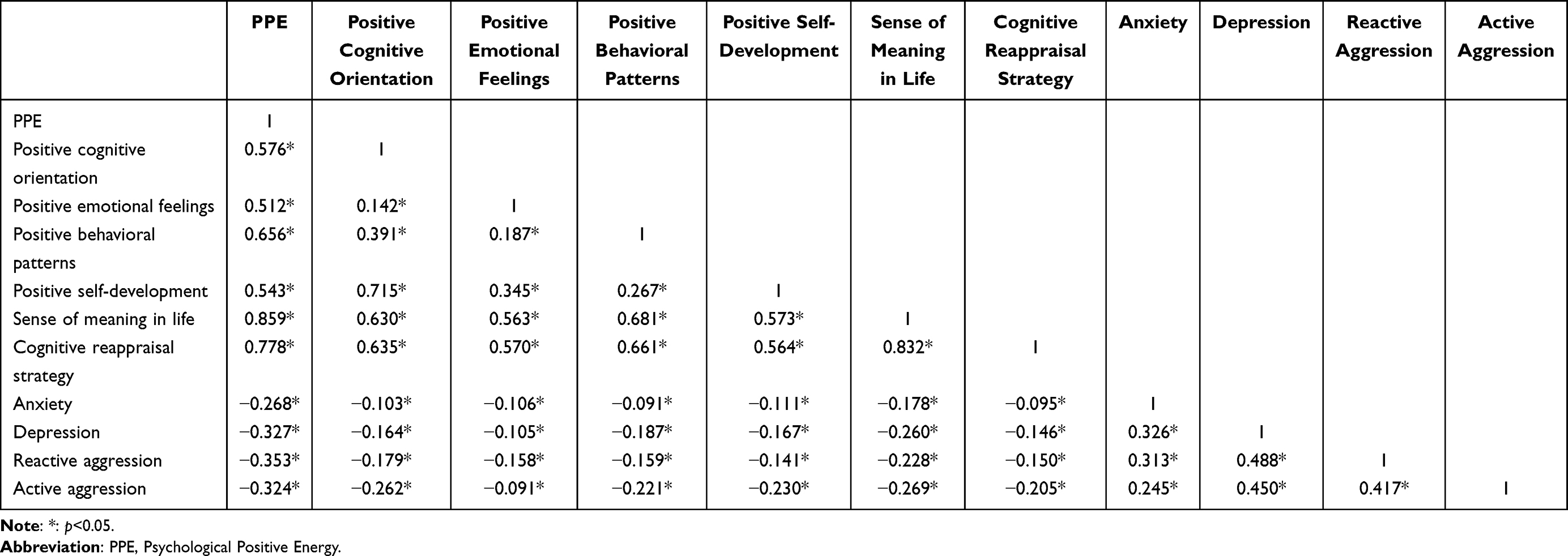 |
Table 8 Correlation Analysis of PPE and Mental Health Variables in Medical Students |
Discussion
Compared with previous research on PPE, which has often focused on a single aspect, this study presents a broader perspective. The reliability of the current findings is supported by the robust psychometric properties of the researcher-developed PPE questionnaire (detailed in General Data), including high content validity (CVI = 0.92), stable construct validity (confirmed by EFA and CFA) and excellent internal consistency (α = 0.965). These properties ensure that the measurement of PPE and its dimensions is accurate, addressing concerns about result credibility. Our four-dimensional PPE framework (positive cognitive orientation, emotional feelings, behavioural patterns, self-development) advances previous research: unlike Lu Hongzhen,9 who focused only on “awareness of PPE” without structural dimensions, and Ren Qihan,6 who lacked a standardised tool, our framework integrates cognitive, emotional, behavioural and developmental components, capturing the holistic nature of PPE in medical students.
All hypotheses were supported: (H1) the four-dimensional structure was confirmed by qualitative saturation and quantitative factor analysis; (H2) gender (men > women) and year-group (final year > first year) differences aligned with our predictions, consistent with the findings that academic experience and socialisation shape positive psychological traits;36 (H3) perceived social support, family care and trait self-control emerged as key predictors, with social support being the strongest (consistent with social cognitive theory18); (H4) PPE’s positive correlation with adaptive outcomes and negative correlation with mental health risks validated its protective role, extending Fredrickson’s broaden-and-build theory4 to medical contexts. This framework’s validity is strengthened by our methodological choices; we adopted an exploratory sequential mixed-methods design,22 where qualitative interviews (n = 650) first identified lived experiences of PPE, and quantitative analysis subsequently validated the structure. Specifically, Strauss and Corbin’s constructivist grounded theory was chosen for its emphasis on co-constructing knowledge from participants’ clinical and academic experiences,26 which aligns with PPE’s dynamic nature (integrating trait-like and state-like features). This approach ensured the four dimensions were not abstract constructs but rooted in real scenarios (eg, “positive behavioural patterns” derived from descriptions of clinical problem-solving), addressing reviewers’ concerns about epistemological clarity.
During the semi-structured interviews, some participants discussed the formation and development of PPE. Most believed that its formation is based on a genetic foundation and develops through interaction with the postnatal environment, consistent with the social–ecological system theory hypothesis. In this regard, the development of PPE results from the interaction between genetic factors and the environment, providing a certain level of explanation. For example, the framework of PPE includes the category of “prosocial behaviour”, which previous studies have confirmed as an outcome of gene–environment interaction.13
Research has also shown that cultures differ in how positive emotions and psychological traits are cultivated. In Eastern cultures, meaning in life and relational well-being are more highly valued, whereas Western cultures tend to emphasise individual happiness and personal achievement.16 This suggests that the development of PPE may be shaped by cultural frameworks that define what constitutes “positive energy” and how it is expressed. However, these explanations remain limited, and further research on the formation and development of PPE should consider it as a complete psychological variable and explore it through quantitative studies.
The scale used in this study is researcher-developed, with no reference to PPE levels in other medical student groups. Based on previous research, the mean positive energy level of medical students can be compared with the theoretical median, where a mean above the theoretical median indicates a good overall level.37 In this study, PPE and its dimensions scored between 5.5 and 6 points, exceeding the theoretical median of 4 (on a seven-point scale), suggesting a generally high level of PPE among medical students.
The analysis of gender and year-group differences revealed substantial variation in PPE between male and female students. In terms of year group, PPE and its dimensions followed similar developmental trends. The analysis of gender differences indicated that men exhibited substantially higher levels of PPE than women. This may be related to differing self-evaluation tendencies between men and women38 as well as broader societal and cultural factors that shape gender-specific psychological traits. Recent studies have shown that men are often socialised to display greater self-confidence and assertiveness, which may contribute to higher PPE levels. Research on gender differences in psychological resilience also suggests that men may adopt more proactive coping strategies in response to stress, further enhancing their PPE.36
The analysis of year-group differences in PPE among medical students indicated that the levels of PPE and its dimensions vary by year group, specifically demonstrating a consistent upward trend from the first year to the final year. This gradual enhancement of PPE across academic levels may be attributed to the cumulative effects of educational experiences, mentorship and exposure to clinical settings, which collectively foster psychological growth and adaptive functioning.39
The potential influencing factors of PPE in medical students were examined using a cross-sectional study design. Pearson correlation analysis and linear regression analysis revealed that perceived social support, family care and trait self-control substantially predicted PPE in medical students (72.1%). The strong predictive power of perceived social support, family care and trait self-control was robust to our instrument selection: (1) the Perceived Social Support Scale was chosen for its validation in student populations,25 ensuring alignment with PPE’s “external resource–internal energy” mechanism; (2) the Family APGAR Scale, validated for assessing family functioning in educational contexts,26 directly reflects the ecological influences on PPE development; (3) the Medical Student Self-Control Scale21 was selected for its focus on behavioural regulation, a core component of “positive behavioural patterns”. This targeted tool selection strengthens the validity of our regression findings.
These findings suggest that social support and family dynamics play a key role in fostering PPE, as they provide both emotional and practical support. Self-control, although important, had a relatively small influence. Each PPE dimension (behavioural patterns, emotional feelings, cognitive orientation and self-development) was influenced by these factors, indicating that a combination of social, familial and individual traits shapes PPE in medical students. Future interventions could focus on enhancing these factors to promote PPE.
Moreover, the sense of meaning in life, cognitive reappraisal strategies, anxiety, depression and aggressive behaviour are all representative factors of mental health, and the descriptive statistics of these variables indicate that medical students generally report a good overall level, suggesting a satisfactory mental health status. Furthermore, correlation analysis showed a statistically significant relationship between PPE and these representative mental health factors, indicating that PPE can predict an individual’s mental health level. In this regard, medical students with high PPE exhibit better mental health than those with low PPE, offering novel directions for future mental health interventions.
Theoretical value: This study clarifies the multidimensional structure of PPE in medical students, filling the gap in the existing literature that focused on isolated components (eg, emotional traits).5 It also validates the applicability of positive psychology frameworks in high-stress professional education, providing a theoretical basis for discipline-specific positive psychological research.
Practical value: The validated PPE questionnaire can serve as a tool for universities to assess students’ psychological status. Interventions targeting key influencing factors (eg, enhancing social support in clinical training, strengthening family–school collaboration) can be designed to improve PPE, thereby reducing anxiety and depression in medical students.
This study presents several key strengths. First, the use of a mixed-methods approach enabled a comprehensive understanding of PPE by combining quantitative data – used to assess the predictive power of various factors – with qualitative interviews that provided rich, in-depth perspectives. Methodological rigor further enhances result credibility: (1) qualitative analysis ensured trustworthiness via data saturation (620th interview), 82% inter-coder agreement and triangulation with quantitative pilot data; (2) the PPE scale’s validity was confirmed through expert review (CVI = 0.92), cognitive interviews and factor analysis (EFA/CFA); (3) sample size (n = 650) exceeded power analysis requirements (n = 129), ensuring statistical robustness. These steps address reviewers’ concerns about methodological transparency and replicability. Although the study offers valuable insights into the PPE framework among medical students, its findings may have broader applications. The cultivation of PPE could benefit students in other disciplines, particularly those facing high levels of academic pressure or emotional stress, such as law, engineering or nursing students. Additionally, the PPE framework may help in understanding mental well-being among non-student populations, including working professionals or individuals in high-stress occupations. By promoting PPE, interventions may enhance mental health outcomes, reduce burnout and foster resilience across diverse groups. Furthermore, this study contributes to the field of positive psychology by extending its application to a more targeted and culturally relevant framework, which may support the development of practical interventions in educational settings or workplace wellness programmes.
This study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design limits our ability to infer causal relationships between PPE and mental health. Although we observed significant correlations, we cannot determine whether PPE influences mental health, whether the reverse is true or whether other factors are involved. Second, the sample is limited to medical students from a single institution, which may affect the generalisability of the findings to other student populations or academic disciplines. Limitations include the following: (1) the cross-sectional design cannot establish causal relationships (eg whether increased PPE reduces anxiety or vice versa); (2) the single-institution sample may limit generalisability to other regions or education systems; (3) the researcher-developed questionnaire, although psychometrically sound, requires validation in multi-centre studies.
Future research could (1) adopt longitudinal designs to track PPE development and its long-term impact on mental health; (2) validate the PPE framework in diverse medical student populations (eg different year groups, specialities); (3) develop targeted interventions (eg social support workshops) and test their effectiveness in improving PPE and mental health.
Despite these limitations, the study provides a foundation for future research. Subsequent studies could track the development of PPE over several months or years to assess its long-term effects on mental health. Longitudinal designs would enable researchers to explore the temporal relationship between PPE and mental health outcomes. Furthermore, future research could implement PPE-based interventions in medical student populations, testing their effects through controlled designs. This would allow researchers to examine causal relationships between PPE and mental health more directly, addressing the limitations of cross-sectional data and offering more robust evidence for intervention strategies. Finally, future research should examine the PPE framework in diverse student populations and academic disciplines to explore its broader applicability across different contexts.
Conclusion
This study developed a framework for PPE in medical students, comprising four dimensions: positive cognitive orientation, emotional feelings, behavioural patterns and self-development.
The researcher-developed questionnaire used to measure PPE demonstrated robust psychometric properties, including high internal consistency (Cronbach’s α = 0.965 for the total scale and 0.869–0.930 for the subscales), good content validity (CVI = 0.92) and stable construct validity (confirmed by EFA and CFA), ensuring the reliability of subsequent findings. The findings indicate that PPE tends to improve as students progress through their studies, with perceived social support, family care and trait self-control emerging as key predictors. Psychological positive energy was also found to correlate positively with mental health, serving as a protective factor. However, limitations such as the cross-sectional design and the sample being drawn from a single institution highlight the need for further research across diverse populations to enhance generalisability.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki.This study was conducted with approval from the Ethics Committee of Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital. Written informed consent was obtained from all participants.
Consent for Publication
The manuscript is not submitted for publication or consideration elsewhere.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any funding support.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Wiseman R. Rip It Up: The Radical New Approach to Changing Your Life. Simon & Schuster; 2012.
2. Pan W, Han Y, Li J, Zhang E, He B. The positive energy of netizens: development and application of fine-grained sentiment lexicon and emotional intensity model. Curr Psychol. 2022;1–18. doi:10.1007/s12144-022-03876-4
3. Ryff CD. Positive psychology: looking back and looking forward. Front Psychol. 2022;13:840062. doi:10.3389/fpsyg.2022.840062
4. Fredrickson BL. The role of positive emotions in positive psychology: the broaden-and-build theory of positive emotions. Am Psychologist. 2001;56(3):218–226. doi:10.1037/0003-066X.56.3.218
5. Pang Z, Wang Z. “Positive energy”: a survey based on conceptual history. Media Forum. 2022;5(11):32–35. doi:10.3969/j.issn.2096-5079.2022.11.008
6. Ren Q. Do People Prefer to Interact with Those with Positive Energy? A Study on the Mechanism of Positive Energy on Interpersonal Communication. Hubei: Wuhan University; 2020.
7. Waters L, Algoe SB, Dutton J, et al. Positive psychology in a pandemic: buffering, bolstering, and building mental health. J Positive Psychol. 2022;17(3):303–323. doi:10.1080/17439760.2021.1871945
8. Lu H. Positive Energy Cultivation of Medical Students in the New Era. Guangxi: Guangxi University; 2021.
9. Luthans F, Broad JD. Positive psychological capital to help combat the mental health fallout from the pandemic and VUCA environment. Organ Dyn. 2022;51(2):100817. doi:10.1016/j.orgdyn.2020.100817
10. Mao Y, Zhang N, Liu J, He R, Wang X. A systematic review of depression and anxiety in medical students in China. BMC Med Educ. 2019;19:1–13. doi:10.1186/s12909-019-1744-2
11. Nair M, Moss N, Bashir A, et al. Mental health trends among medical students. Proc (Bayl Univ Med Cent). 2023;36(3):408–410. doi:10.1080/08998280.2023.2187207
12. Mamyrova G, Rider LG, Haagenson L, et al. Parvovirus B19 and onset of juvenile dermatomyositis. JAMA. 2005;294(17):2165–2171. doi:10.1001/jama.294.17.2170
13. Chen G, Wang J, Huang Q, et al. Social support, psychological capital, multidimensional job burnout, and turnover intention of primary medical staff: a path analysis drawing on conservation of resources theory. Hum Resour Health. 2024;22(1):42. doi:10.1186/s12960-024-00915-y
14. Matud MP, López-Curbelo M, Fortes D. Gender and psychological well-being. Int J Environ Res Public Health. 2019;16(19):3531. doi:10.3390/ijerph16193531
15. Benoit V, Gabola P. Effects of positive psychology interventions on the well-being of young children: a systematic literature review. Int J Environ Res Public Health. 2021;18(22):12065. doi:10.3390/ijerph182212065
16. Wood-Barcalow NL, Alleva JM, Tylka TL. Revisiting positive body image to demonstrate how body neutrality is not new. Body Image. 2024;50:101741. doi:10.1016/j.bodyim.2024.101741
17. Seligman MEP, Railton P, Baumeister RF, Sripada C. Homo Prospectus. Oxford University Press; 2016; doi:10.1093/acprof:oso/9780198746988.001.0001
18. Usher EL, Schunk DH. Social cognitive theoretical perspective of self-regulation. Handbook of self-regulation of learning and performance. In: Handbook of Self-Regulation of Learning and Performance. Routledge; 2017;19–35.
19. Dahlem NW, Zimet GD, Walker RR. The multidimensional scale of perceived social support: a confirmation study. J Clin Psychol. 1991;47(6):756–761. doi:10.1002/1097-4679(199111)47:6<756::AID-JCLP2270470605>3.0.CO;2-L
20. Castilla H, Caycho T, Shimabukuro M, et al. Perception of family functioning: psychometric analysis of family APGAR scale in adolescents in Lima. J Educ Psychol. 2014;2(1):65–78.
21. Unger A, Bi C, Xiao YY, et al. The revising of the Tangney self‐control scale for Chinese students. PsyCh Journal. 2016;5(2):101–116. doi:10.1002/pchj.128
22. Barroga E, Matanguihan GJ, Furuta A, et al. Conducting and writing quantitative and qualitative research. J Korean Med Sci. 2023;38(37):e291. doi:10.3346/jkms.2023.38.e291
23. Sun L, Sun LN, Sun YH, et al. Correlations between psychological symptoms and social relationships among medical undergraduates in Anhui Province of China. Int J Psychiatry Med. 2011;42(1):29–47. doi:10.2190/PM.42.1.c
24. Eaves YD. A synthesis technique for grounded theory data analysis. J Adv Nurs. 2001;35(5):654–663. doi:10.1046/j.1365-2648.2001.01897.x
25. Bruno TCV, Custódio IDD, de Menezes-Junior LAA, et al. Development and validity evidence on the scale of perceived social support for university students (EPSSEU) during the period of social restrictions. BMC Public Health. 2024;24(1):1474. doi:10.1186/s12889-024-18882-3
26. Castilla H, Caycho T, Shimabukuro M, Valdivia A. Perception of family functioning: psychometric analysis of family APGAR scale in adolescents in Lima. J Educ Psychol. 2020;8(2):e2007. doi:10.1007/s41649-020-00007-8
27. Perchtold CM, Weiss EM, Rominger C, et al. Humorous cognitive reappraisal: more benign humour and less “dark” humour is affiliated with more adaptive cognitive reappraisal strategies. PLoS One. 2019;14(1):e0211618. doi:10.1371/journal.pone.0211618
28. Naghiyaee M, Bahmani B, Asgari A. The psychometric properties of the meaning in life questionnaire (MLQ) in patients with life-threatening illnesses. Sci World J. 2020;2020:8361602. doi:10.1155/2020/8361602
29. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
30. Zung WW. A SELF-RATING DEPRESSION SCALE. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
31. Raine A, Dodge K, Loeber R, et al. The reactive-proactive aggression questionnaire: differential correlates of reactive and proactive aggression in adolescent boys. Aggress Behav. 2006;32(2):159–171. doi:10.1002/ab.20115
32. Al-Mahrouqi T, Al-Obeidani R, Elsherif M, et al. Predictors of presence of and search for meaning in life among Omani students during the COVID-19 pandemic: a cross-sectional study. Sci Rep. 2024;14(1):29685. doi:10.1038/s41598-024-80999-7
33. You X, Wang MC, Xia F, Liu T. Measurement invariance of the reactive and proactive aggression questionnaire (RPQ) across self-and other-reports. J Aggression Maltreat Trauma. 2021;30(2):261–277. doi:10.1080/10926771.2020.1806973
34. Roustaei N. Application and interpretation of linear-regression analysis. Med Hypothesis Discov Innov Ophthalmol. 2024;13(3):151–159. doi:10.51329/mehdiophthal1506
35. AtlaTi. What is Open Coding in Qualitative Research? 2025. Available from: https://atlasti.com/research-hub/open-coding.
36. Biswas A, Harbin S, Irvin E, et al. Sex and gender differences in occupational hazard exposures: a scoping review of the recent literature. Curr Environ Health Rep. 2021;8(4):267–280. doi:10.1007/s40572-021-00330-8
37. Liu Y, Cai H, Han T, et al. Network analysis of comorbid aggressive behavior and testosterone among bipolar disorder patients: a cross-sectional study. Transl Psychiatry. 2024;14(1):224. doi:10.1038/s41398-024-02957-1
38. Wilhelm RA, Lacey MF, Masters SL, et al. Greater weekly physical activity linked to left resting frontal alpha asymmetry in women: a study on gender differences in highly active young adults. Psychol Sport Exerc. 2024;74:102679. doi:10.1016/j.psychsport.2024.102679
39. Chim K, Lai JTC, Chan BTY. Embedding positive psychology into curriculum to promote posttraumatic growth, psychological flexibility, and socio-emotional competencies in higher education. Front Psychol. 2024;15:1450192. doi:10.3389/fpsyg.2024.1450192
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.