Back to Journals » Psychology Research and Behavior Management » Volume 19
Psychological Flexibility and Mental Health: Theoretical Foundations, Empirical Support, and Applications Across Clinical Contexts
Authors Chalghaf N ![]() , Chokri I
, Chokri I ![]() , Boukari S, Dergaa MA, Dhahbi W
, Boukari S, Dergaa MA, Dhahbi W ![]() , Ceylan HI
, Ceylan HI ![]() , Maamri ME, Solmi S
, Maamri ME, Solmi S ![]() , Muntean RI
, Muntean RI ![]() , Guelmami N, Dergaa I
, Guelmami N, Dergaa I ![]()
Received 14 January 2026
Accepted for publication 28 March 2026
Published 30 June 2026 Volume 2026:19 596070
DOI https://doi.org/10.2147/PRBM.S596070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Igor Elman
Nasr Chalghaf1, Imed Chokri1,2, Samia Boukari3, Mohamed Amine Dergaa4, Wissem Dhahbi4,5, Halil Ibrahim Ceylan6, Mohamed Elaid Maamri1, Sana Solmi1, Raul Ioan Muntean7, Noomen Guelmami4,*, Ismail Dergaa3,4,8,*
1High Institute of Sport and Physical Education of Gafsa, University of Gafsa, Gafsa, Tunisia; 2High Institute of Sport and Physical Education of Sfax, University of Sfax, Sfax, Tunisia; 3High Institute of Sport and Physical Education of Ksar Said, University of Manouba, Manouba, Tunisia; 4High Institute of Sports and Physical Education of Kef, University of Jendouba, El Kef, Tunisia; 5Training Department, Police College, Police Academy, Doha, Qatar; 6Physical Education and Sports Teaching Department, Faculty of Sports Sciences, Ataturk University, Erzurum, Turkey; 7Department of Physical Education and Sport, Faculty of Law and Social Sciences, University “1 Decembrie 1918” of Alba Iulia, Alba Iulia, Romania; 8Physical Activity, Sport and Health Research Unit, UR18JS01, National Observatory of Sport, Tunis, Tunisia
*These authors contributed equally to this work
Correspondence: Halil Ibrahim Ceylan, Email [email protected]
Raul Ioan Muntean, Email [email protected]
Abstract: A key transdiagnostic process in modern mental health science is psychological flexibility, defined as the ability to remain freely engaged with present-moment experience while pursuing valued goals, even in the context of suffering. The construct, which is based on Relational Frame Theory and operationalised within the framework of Acceptance and Commitment Therapy (ACT), consists of six interconnected processes: self-as-context, values clarity, acceptance, cognitive defusion, present-moment awareness, and committed action. This narrative review, based on systematic searches of PubMed, PsycINFO, and Web of Science covering publications from 1987 to 2024, synthesizes theoretical foundations, measurement approaches, mechanistic evidence, and clinical applications of psychological flexibility across diverse populations and conditions. Meta-analytic findings consistently demonstrate small-to-medium effects of flexibility-based interventions on anxiety, depression, chronic pain, substance use disorders, and workplace functioning, with converging evidence that psychological flexibility mediates treatment outcomes. The Acceptance and Action Questionnaire-II (AAQ-II) remains the most widely used assessment tool; however, concerns persist regarding its discriminant validity from general negative affect. Key limitations include predominantly cross-sectional research designs, cultural homogeneity in study samples, and methodological weaknesses in mediation research that constrain causal inference. Ten research priorities are proposed, with particular urgency around prospective longitudinal designs to establish causal precedence, the development of culturally sensitive assessment instruments, and systematic cross-cultural adaptation research. Current evidence supports psychological flexibility as a clinically accessible, theoretically coherent construct with demonstrated utility across a wide range of conditions. For practitioners, this translates into a process-based intervention target that is applicable across diagnostic categories and that does not require disorder-specific protocol switching. It can be reduced to specific clinical techniques like acceptance exercises, defusion strategies, and values-guided behavioural activation.
Keywords: experiential avoidance, mindfulness, behavior therapy, committed action, psychopathology, cognitive defusion
Introduction
Mental health disorders collectively affect approximately one in eight individuals worldwide, with the World Health Organization estimating that over 970 million people are currently living with a mental or substance use disorder.1 This global burden is compounded by high rates of diagnostic comorbidity, limited treatment uptake, and the inherent constraints of disorder-specific therapeutic models. The search for transdiagnostic mechanisms capable of addressing this complexity is therefore a scientific and clinical priority of considerable urgency.
Clinical psychology has shifted toward process-based approaches targeting underlying mechanisms rather than discrete symptom reduction.2 Psychological flexibility stands as a central construct in this evolution.3 Hayes et al defined psychological flexibility as the ability to contact the present moment fully as a conscious human being and to change or persist in behavior when doing so serves valued ends.4 This definition emphasizes functional contextualism, in which psychological processes acquire meaning through their relationship to valued outcomes rather than their content or frequency.
Traditional cognitive-behavioral approaches emphasized changing or eliminating problematic thoughts and feelings.5 The psychological flexibility model offers a different perspective: psychological suffering stems less from difficult internal experiences themselves than from inflexible attempts to control or avoid such experiences when doing so compromises valued living.6 A person experiencing anxiety about public speaking might avoid presentations entirely, sacrificing career advancement. Alternatively, they might acknowledge anxiety while speaking anyway, guided by professional values.
Acceptance and Commitment Therapy emerged in the late 1980s as the primary intervention targeting psychological flexibility.7 Hayes et al articulated ACT’s core principles in their foundational text.6 Since then, research has expanded substantially. The Society of Clinical Psychology designates ACT as empirically supported for chronic pain, depression, anxiety disorders, and substance use.8
It is important to note that psychological flexibility is not exclusively an ACT construct. In Dialectical Behaviour Therapy (DBT), flexibility-adjacent processes are cultivated through mindfulness and distress tolerance skills, enabling individuals to respond to emotional crises without rigid avoidance or impulsive reactivity.9 Similarly, Mindfulness-Based Cognitive Therapy (MBCT) addresses inflexible ruminative processing through non-judgmental present-moment awareness, directly analogous to the present-moment awareness component of the hexaflex.10 This broader therapeutic context positions psychological flexibility as a transtherapeutic mechanism rather than a model-specific construct.
Research demonstrates the relevance of psychological flexibility across clinical presentations, organizational contexts, health behaviors, and normative populations. Studies link the construct to depression, anxiety disorders, chronic pain, substance use, eating disorders, workplace functioning, academic performance, and relationship quality.11 Kashdan and Rottenberg argued that psychological flexibility represents a fundamental aspect of health, proposing it as a unifying framework for understanding adaptive human functioning.3
Despite widespread interest, important questions persist.12 Concerns exist regarding construct specificity, measurement adequacy, mechanism clarity, and cultural generalizability.13–15 Arch et al raised methodological concerns about mediation research, noting inadequate sample sizes and analytical approaches.12 Critics question whether psychological flexibility processes are unique to ACT or shared across evidence-based interventions.16 The causal status of flexibility remains incompletely established. Longitudinal research examining whether flexibility precedes mental health outcomes or vice versa remains limited.17 Most recently, Macri et al published a comprehensive systematic and meta-analytic review examining all six hexaflex domains as treatment mechanisms, providing the most granular process-level evidence to date and identifying specific patterns in how individual flexibility components contribute to ACT outcomes.18 Furthermore, this review explicitly evaluates the challenges of generalizing the psychological flexibility construct and its associated interventions to non-Western cultural contexts, which remain significantly underrepresented in the empirical literature and constitute a critical barrier to the construct’s global clinical utility.
Despite over three decades of research, no single synthesis has simultaneously addressed the theoretical architecture, the state-of-the-art in psychometrics, the mechanistic evidence base, cross-domain clinical applications, and the cultural generalizability of psychological flexibility within a single integrated framework. Existing reviews have addressed ACT efficacy within specific clinical populations or have examined individual measurement instruments in isolation. The present narrative review addresses this gap by providing the integrative, transdiagnostic account needed to guide both research design and evidence-based clinical practice. The central argument threading through this review is that psychological flexibility functions as a transdiagnostic regulatory capacity whose theoretical coherence and empirical support are well-established, but whose full scientific potential remains constrained by specific, addressable methodological and conceptual limitations, constraints that each subsequent section progressively analyses.
Based on these identified gaps in the literature, this narrative review aimed to: (i) synthesize theoretical foundations of psychological flexibility within Relational Frame Theory and the hexaflex model; (ii) evaluate measurement approaches and their psychometric properties; (iii) examine meta-analytic evidence across clinical, workplace, and health behavior domains; (iv) analyze mechanisms of change and mediational pathways; (v) assess applications across diverse populations and conditions; (vi) critically evaluate methodological limitations and construct validity concerns; and (vii) propose future research directions to address current knowledge gaps. Unlike prior reviews that have addressed ACT efficacy within single disorder categories or examined isolated measurement instruments, the present review uniquely integrates all seven of these dimensions within a single coherent synthesis, designed to serve both researchers consolidating their knowledge base and clinicians seeking a theoretically grounded and practically applicable overview of the construct.
Literature Search and Selection
This narrative review was conducted through systematic searches of PubMed, PsycINFO, and Web of Science using the following terms: psychological flexibility, acceptance and commitment therapy, experiential avoidance, hexaflex model, relational frame theory, mindfulness-based interventions, cognitive defusion, valued action, and related constructs. Publications from 1987 to 2024 were considered, encompassing empirical studies, meta-analyses, systematic reviews, randomized controlled trials, and foundational theoretical texts. Priority was given to peer-reviewed sources published in or after 2020. Foundational works published prior to 2020 were retained where they represent the theoretical or psychometric basis of the field and cannot be replaced by more recent equivalents without misrepresenting the intellectual history of the construct. Studies were selected to provide comprehensive coverage of the theoretical, measurement, mechanistic, and applied dimensions of psychological flexibility across clinical and non-clinical contexts. All selected sources were reviewed by the lead authors; disagreements about inclusion were resolved through discussion and consensus.
Theoretical Foundations
Relational Frame Theory as Philosophical Foundation
Relational Frame Theory provides the scientific foundation for psychological flexibility.19 Developed by Hayes, Barnes-Holmes et al, RFT extends behavioral principles to explain uniquely human psychological phenomena, including language, cognition, and abstract reasoning. Understanding RFT is essential to understanding why flexibility developed as a therapeutic target.20
RFT proposes that human language involves arbitrarily applicable relational responding. Unlike simple associations, relational framing derives relations among stimuli from contextual cues rather than from physical properties.21 Humans learn that if A exceeds B and B exceeds C, then A must exceed C without directly comparing A and C.22 This derived relational responding underlies language comprehension, mathematical reasoning, and symbolic thought.
While relational framing provides adaptive advantages, it creates vulnerabilities to psychological suffering. Language processes allow humans to relate past negative experiences to current situations, anticipate threats that may never materialize, and construct negative self-evaluations.23 The statement “I am worthless” illustrates how language creates relations between oneself and negative evaluations that persist despite contradictory evidence. Once established, verbal relations exert powerful behavioral control, often limiting flexibility and undermining valued aspects of life.
From this perspective, psychological inflexibility arises when verbal constructions dominate behavioral regulation at the expense of direct contingencies and personal values.6 Experiential avoidance exemplifies this process: verbal rules like “I cannot tolerate anxiety” may lead to avoiding anxiety-provoking situations even when avoidance prevents valued activities.24 Cognitive fusion occurs when individuals become entangled with literal thought content, treating verbal constructions as objective truths rather than ongoing mental events.25
The Hexaflex Model
Building on RFT, ACT articulates a six-process model of psychological flexibility, commonly represented in the hexaflex diagram (see Table 1).4 These processes organize into two categories: mindfulness and acceptance processes (acceptance, cognitive defusion, present-moment awareness, self-as-context) and commitment and behavior change processes (values clarification, committed action).
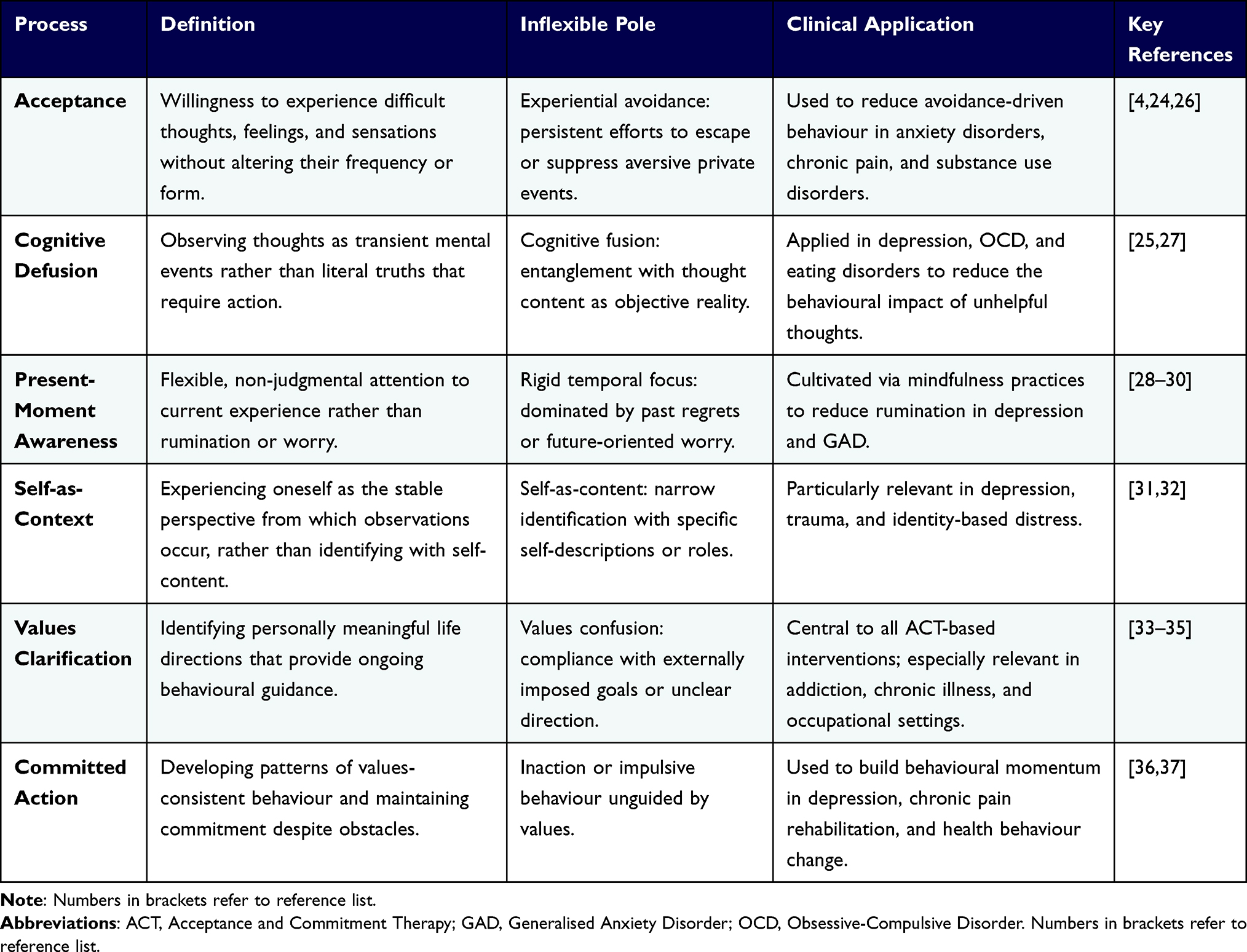 |
Table 1 The Six Core Processes of Psychological Flexibility and Their Clinical Applications |
Acceptance involves willingness to experience difficult thoughts, feelings, and sensations without attempting to change their frequency or form. Rather than suppressing anxiety or controlling sadness, acceptance means allowing these experiences while engaging in valued behavior. Research demonstrates that experiential avoidance, the opposite of acceptance, correlates with numerous forms of psychopathology.26 Bond and Bunce found that acceptance predicted mental health outcomes better than attempts to control internal experiences in workplace samples.38
Cognitive defusion refers to observing thoughts as transient mental events rather than as literal truths that require action. Techniques help individuals recognize “I am a failure” as a thought rather than an objective fact about oneself.27 Defusion creates distance from thought content without changing the thoughts themselves.25 This process contrasts with cognitive restructuring, which challenges and modifies thought content.
Present-moment awareness involves flexible attention to current experience rather than dwelling on past regrets or future worries.28 Mindfulness practices cultivate this capacity.29 Research indicates that present-moment awareness associates with reduced rumination and worry, two cognitive processes implicated in depression and anxiety disorders.30
Self-as-context refers to experiencing oneself as the perspective from which observations occur, rather than identifying with specific self-content. Through deictic framing (I-you, here-there, now-then), humans develop a transcendent sense of self that remains constant despite changing thoughts, feelings, and experiences.31 This process allows individuals to observe difficult experiences without becoming defined by them. Research on self-as-context remains limited compared to other processes.32
Values clarification involves identifying personally meaningful life directions rather than socially prescribed goals. Values differ from goals in that they are not ends in themselves but rather provide ongoing direction for behavior.33 A systematic review found that higher levels of valued living correlated negatively with depression and anxiety across populations, underscoring the central role of values engagement in psychological health.34 The value of being a supportive friend differs from the goal of calling a friend on Tuesday; the value provides continuous guidance as the goal is accomplished and completed.
Committed action is taking practical steps guided by values, even when obstacles arise. This process involves developing patterns of values-consistent behavior, accepting setbacks, and maintaining commitment in the face of difficulties.36 Research indicates that committed action mediates relationships between other flexibility processes and behavioral outcomes.
These six processes function interdependently rather than independently.37 Changes in one process often affect others.39 Acceptance facilitates present-moment awareness. Cognitive defusion enables contact with values beyond verbal constructions about what one “should” want. The model proposes that interventions targeting any process can enhance overall flexibility, though comprehensive interventions address multiple processes.
Psychological Inflexibility
The obverse of flexibility, psychological inflexibility, comprises six corresponding processes. Experiential avoidance refers to an unwillingness to remain in contact with difficult private events, accompanied by efforts to alter their form, frequency, or situational sensitivity.24 Cognitive fusion involves entanglement with literal thought content.25 A lack of present-moment awareness manifests as rumination, worry, or dissociation.40 Self-as-content occurs when individuals identify narrowly with particular self-descriptions. Confusion about values, or compliance with externally imposed goals rather than personally meaningful directions, characterizes value problems. Inaction or impulsive behavior unguided by values represents the opposite of committed action.
Research demonstrates associations between inflexibility and diverse forms of psychopathology. Hayes et al conducted correlational studies and found that psychological flexibility accounted for substantial variance in psychopathology measures at baseline.4 Subsequent studies have replicated these relationships across clinical and non-clinical samples.41
Measurement and Assessment
The Acceptance and Action Questionnaire Series
Measuring psychological flexibility presents unique challenges given its multi-faceted nature and emphasis on function over form. The Acceptance and Action Questionnaire is the primary instrument for assessing global psychological flexibility and its opposite, experiential avoidance.24
Hayes et al developed the original AAQ to assess unwillingness to experience unpleasant thoughts and feelings, inability to pursue valued directions in the presence of psychological obstacles, and behavioral ineffectiveness in the presence of difficult internal experiences. Initial validation studies demonstrated acceptable reliability and validity across samples. The AAQ correlated significantly with measures of psychopathology, quality of life, and behavioral outcomes.24
However, the original AAQ faced psychometric challenges. Internal consistency proved variable across studies. Item complexity sometimes confused respondents. The factor structure remained unclear, with some studies identifying multiple factors rather than a unitary construct. These limitations prompted the development of a revised measure.
Bond et al introduced the Acceptance and Action Questionnaire-II to address these concerns.42 The AAQ-II comprises items with simplified wording and a more explicit focus on psychological inflexibility. Sample items include “My painful experiences and memories make it difficult for me to live a life that I would value” and “I’m afraid of my feelings.” Higher scores indicate greater inflexibility.
Extensive validation studies support the AAQ-II.42 Bond et al reported good internal consistency (Cronbach’s alpha.84-0.93 across independent samples), acceptable test-retest reliability (r =0.81 at three-month intervals), and significant convergent validity with measures of depression and anxiety. The AAQ-II demonstrated incremental validity beyond Big Five personality traits in predicting mental health outcomes. Factor analyses supported a single underlying factor structure. However, discriminant validity from general negative affect is less robust, with correlations with the PHQ-9 and GAD-7 sometimes exceeding r =0.60, raising concerns that the instrument captures psychological flexibility specifically or broader psychological distress.
Despite these improvements, concerns about the AAQ-II persist.13 Some researchers question whether the measure assesses psychological flexibility specifically or general distress more broadly. High correlations with depression and anxiety measures raise concerns about discriminant validity.43 The measure may conflate process with outcome. Wolgast argued that several AAQ-II items assess negative outcomes rather than experiential avoidance per se.13
Context-Specific Measures
Recognizing that flexibility may vary across life domains, researchers developed context-specific measures. Bond et al developed the Work-related Acceptance and Action Questionnaire (WAAQ) to assess workplace flexibility.44 The WAAQ demonstrated superior predictive validity for work outcomes compared with the general AAQ-II, supporting the utility of domain-specific assessment.
Similar measures address flexibility in chronic pain,45 parenting,46 body image,47 and other domains. These instruments typically show stronger relationships with domain-specific outcomes than global flexibility measures, suggesting context matters in assessing and intervening on flexibility processes.
Process-Specific Measures
Rather than assessing global flexibility, some instruments target specific processes within the hexaflex. The Cognitive Fusion Questionnaire measures the degree to which individuals are entangled with thought content.25 The Valued Living Questionnaire assesses value clarity and consistency of actions with values across life domains.35 The Five Facet Mindfulness Questionnaire includes subscales assessing present-moment awareness, non-reactivity, and other mindfulness components related to flexibility processes.48
These process-specific measures facilitate more precise examination of mechanisms. Research can determine whether interventions affect particular processes and whether changes in specific processes mediate outcomes.49 However, the proliferation of measures creates challenges for literature synthesis and theory evaluation.
Alternative Flexibility Measures
Dissatisfaction with the limitations of the AAQ prompted the development of alternative measures. Kashdan et al introduced the Personalized Psychological Flexibility Index, which assesses flexibility in relation to individually specified valued goals.50 Respondents identify personal goals and then rate tendencies to avoid, accept, or harness discomfort when pursuing those goals. This idiographic approach addresses concerns about decontextualized assessment.
Gloster et al developed the Multidimensional Psychological Flexibility Inventory to provide a comprehensive assessment across all hexaflex processes.51 The MPFI includes subscales for each of the six flexibility processes, along with their inflexible counterparts. Preliminary validation supports the measure’s reliability and validity, though more research is needed.
Behavioral and Laboratory Measures
Beyond self-report, researchers have developed behavioral and laboratory methods for assessing flexibility. These tasks typically involve exposing participants to aversive experiences while measuring persistence in valued activities.52 The cold pressor task, in which participants immerse their hand in ice water, has been used alongside measures of pain tolerance and willingness to experience discomfort. Studies demonstrate that individuals higher in psychological flexibility show greater pain tolerance and faster recovery to baseline distress.
Mirror tracing tasks, in which participants trace shapes while viewing only their hand in a mirror, provide another laboratory assessment. Performance requires accepting frustration while persisting with the task.39 These behavioral measures reduce reliance on self-report and may mitigate standard method variance.
Understanding the theoretical architecture of psychological flexibility is only scientifically useful if the construct can be reliably and validly operationalized; the section above has evaluated the current state of measurement and highlighted where psychometric limitations constrain theoretical conclusions. The review now turns to the empirical evidence base, evaluating whether the flexibility construct, as currently measured, predicts and mediates treatment outcomes across clinical conditions with sufficient consistency to justify its transdiagnostic claims.
Empirical Evidence BASE
Meta-Analytic Findings on Clinical Outcomes
Multiple meta-analyses have evaluated the efficacy of ACT in promoting psychological flexibility and improving clinical outcomes (see Table 2).11 A-Tjak et al conducted a comprehensive meta-analysis of randomized controlled trials examining ACT for clinically relevant mental and physical health problems.53 Results indicated ACT produced medium effect sizes for anxiety, depression, addiction, and somatic health problems compared to control conditions. Effects remained significant, though smaller, when comparing ACT to established treatments.
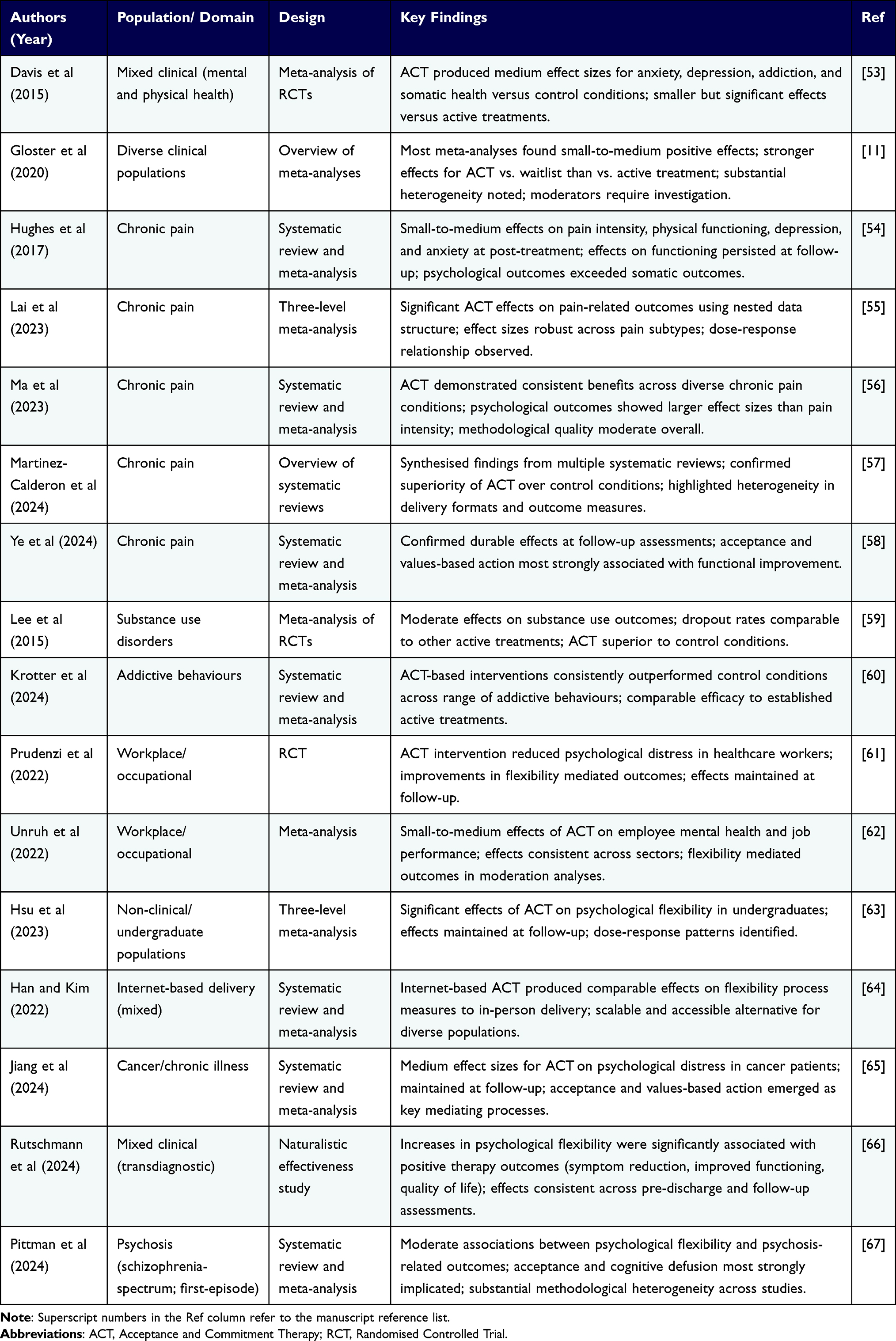 |
Table 2 Summary of Major Meta-Analyses and Systematic Reviews Examining Psychological Flexibility-Based Interventions |
Gloster et al provided an overview of meta-analyses examining ACT across diverse populations and outcomes.11 Most meta-analyses found small to medium positive effects, with stronger effects typically emerging for ACT versus waitlist or treatment-as-usual conditions than for active treatment comparisons. The authors noted substantial heterogeneity across studies and called for more rigorous investigation of moderators affecting outcomes.
The most recent overview of ACT research by Levin et al confirmed that ACT evidence continues to grow rapidly across clinical domains, with an expanding evidence base across new populations and delivery modalities.68
Domain-specific meta-analyses provide additional detail. Hughes et al examined ACT for chronic pain across multiple studies, finding small to medium effects on pain intensity, physical functioning, depression, and anxiety at post-treatment.54 Effects on functioning persisted at follow-up. Lee et al meta-analyzed ACT for substance use disorders, finding moderate effects on substance use outcomes and dropout rates similar to comparison treatments.59
Most recently, Pittman et al documented moderate associations between psychological flexibility and psychosis-related outcomes across schizophrenia-spectrum and first-episode psychosis populations, with acceptance and cognitive defusion emerging as the most strongly implicated processes.67
A naturalistic effectiveness study by Rutschmann et al further confirmed that increases in psychological flexibility were significantly associated with positive therapy outcomes following transdiagnostic ACT treatment across diverse clinical presentations.66
Comparing across these bodies of meta-analytic evidence reveals several consistent and instructive patterns. First, effect sizes are systematically larger when flexibility-based interventions are compared to waitlist or treatment-as-usual controls than when compared to active psychological treatments, suggesting that a meaningful proportion of ACT’s benefit may reflect common therapeutic factors rather than flexibility-specific processes. Second, effects on psychological outcomes such as depression, anxiety, and quality of life reliably exceed those on somatic or behavioral outcomes such as pain intensity ratings and substance use frequency, a finding consistent with the model’s theoretical emphasis on psychological functioning over symptom elimination. Third, methodological quality varies substantially across clinical domains: chronic pain and workplace research draw on higher-quality randomized controlled trial evidence with longer follow-up periods, whereas evidence for eating disorders and health behavior change largely remains confined to small pilot trials. These contrasts carry direct implications for the degree of confidence with which clinical recommendations can be made across condition categories, and highlight precisely where research investment is most urgently needed.
Psychological Flexibility as Mediator
Understanding whether interventions work through theorized mechanisms is crucial for evaluating theories and refining treatments.69 Numerous studies have examined whether changes in psychological flexibility mediate ACT’s effects on outcomes.
Fledderus et al conducted a randomized trial of guided self-help ACT for psychological distress, measuring flexibility at multiple timepoints.70 Multilevel modeling demonstrated that improvements in flexibility mediated reductions in depression and anxiety. Participants with higher baseline flexibility showed stronger treatment effects. Similar findings have arisen from studies of ACT for social anxiety, generalized anxiety disorder, chronic pain, and workplace stress.38,71–73
However, Arch et al provided a critical evaluation of ACT mediation research, identifying substantial methodological limitations. Many studies lacked adequate sample sizes to detect mediation effects. Few studies have assessed temporal precedence, measuring whether changes in flexibility precede changes in outcomes, as causal mediation requires. Studies often failed to demonstrate treatment specificity, showing that psychological flexibility also changed in non-ACT comparison conditions.
Stockton et al conducted a systematic review of mediation studies examining whether ACT processes mediate outcomes.49 While many studies found evidence for mediation, most suffered from methodological weaknesses, including cross-sectional designs, inadequate statistical approaches, and failure to test competing models. The authors concluded that stronger evidence requires longitudinal designs with multiple assessment points and comparisons of ACT processes with those targeted in alternative treatments.
Workplace and Organizational Research
Bond et al have extensively examined psychological flexibility in workplace contexts. Bond and Bunce randomly assigned employees to worksite stress management interventions based on ACT principles or traditional problem-focused approaches.74 ACT proved more effective in improving mental health, with changes mediated by acceptance rather than problem-solving. The ACT condition showed sustained benefits at follow-up.
Bond and Flaxman demonstrated that psychological flexibility and job control interact to predict workplace outcomes.71 Flexibility proved particularly beneficial under conditions of low job control, suggesting it buffers stress when situational control proves limited. This finding aligns with ACT’s emphasis on accepting what cannot be changed while pursuing valued directions.
Bond et al examined the role of flexibility in organizational change.75 During a work reorganization intervention, employee flexibility moderated relationships between job redesign and outcomes. Those with higher flexibility showed greater learning, innovation, and improvements in mental health following reorganization.
Further research has linked workplace flexibility to job performance, absenteeism, turnover intentions, and innovation. Bond et al developed the Work-related Acceptance and Action Questionnaire and demonstrated its utility in predicting employment outcomes beyond general flexibility measures.44 Meta-analytic evidence indicates that workplace ACT interventions produce small to medium effects on employee mental health.61
More recently, a meta-analytic examination by Unruh et al confirmed small-to-medium effects of ACT-based interventions on employee mental health and job performance across organizational settings, providing an updated and comprehensive evidence base for workplace applications.62
Health Behavior Applications
Psychological flexibility has been applied to health behavior change with promising results. Lillis et al tested an ACT-based weight-management intervention, hypothesizing that accepting food-related thoughts and feelings while pursuing health values would improve outcomes compared with traditional weight-loss approaches.76 Results supported the model: acceptance and values-based action mediated weight loss and psychological outcomes.
A systematic review by Iturbe et al further supported the use of ACT for overweight and obesity management, demonstrating that acceptance-based strategies produced clinically meaningful improvements in weight-related outcomes and psychological well-being.77
Gifford et al developed acceptance-based smoking cessation treatment emphasizing willingness to experience cravings while committing to quit-related values.78 A randomized trial found ACT comparable to nicotine replacement therapy at post-treatment, with superior outcomes at follow-up. Subsequent trials have replicated these findings using telephone-delivered and smartphone-delivered ACT interventions.79
Butryn et al examined the use of ACT for physical activity promotion.80 The intervention targeted acceptance of exercise-related discomfort and valued directions related to health and vitality. Participants showed increased physical activity at post-treatment maintained at follow-up. Changes in psychological flexibility mediated increases in activity.
Graham et al systematically reviewed ACT for chronic illness and long-term conditions, examining studies across diabetes, cancer, epilepsy, and other conditions.81 Results indicated ACT improved the quality of life and reduced distress related to chronic illness. Effects on medical outcomes were mixed, with some conditions showing improvement and others not.
A meta-analysis by Jiang et al provided strong evidence that ACT significantly reduces psychological distress in cancer patients, with medium effect sizes maintained at follow-up assessments.65
Non-Clinical Populations
Research has extended beyond clinical samples to examine flexibility in general populations. Studies demonstrate that flexibility correlates with life satisfaction, positive affect, and psychological well-being even among non-distressed individuals.3,4 Kashdan and Rottenberg reviewed evidence positioning flexibility as a fundamental aspect of health rather than merely the absence of pathology.3
Academic settings have received particular attention. College student samples show that flexibility predicts academic performance, retention, and adjustment to university life.82 Levin et al demonstrated the feasibility and preliminary efficacy of web-based ACT prevention programs for college students.
A three-level meta-analysis by Hsu et al confirmed significant effects of ACT on psychological flexibility in undergraduate populations, with effects maintained at follow-up and evidence of dose-response patterns.63
Parenting represents another non-clinical application domain. Research indicates that parental psychological flexibility predicts parenting stress, parent-child relationship quality, and child adjustment.83 Blackledge and Hayes developed an ACT workshop for parents of children with autism, finding significant reductions in parental distress and improvements in acceptance maintained at follow-up.84
Mechanisms of Change
Demonstrating that flexibility-based interventions work is a necessary but insufficient scientific foundation; understanding the processes through which they work is essential for theory refinement and treatment optimization. The following section examines process-level evidence with this goal in mind.
Process Research Examining How ACT Works
Understanding therapeutic mechanisms requires investigating not only whether treatments work but also how they work.69 Process research examines relationships among interventions, theorized change processes, and outcomes. For ACT, this means testing whether interventions affect psychological flexibility and whether changes in flexibility produce changes in symptoms.
McCracken and Gutierrez-Martinez examined processes of change in an interdisciplinary ACT-based treatment for chronic pain.72 They assessed flexibility processes weekly throughout treatment and examined relationships with pain-related functioning. Results indicated that changes in acceptance and values-based action during early treatment sessions predicted later improvements in functioning. Changes in pain catastrophizing and pain-related fear proved less consistent as predictors.
Hayes et al investigated processes of change in acceptance-based behavior therapy for generalized anxiety disorder.73 They measured worry, mindfulness, and psychological flexibility before each session throughout treatment. Time-lagged analyses indicated that session-to-session increases in flexibility preceded subsequent decreases in worry, supporting the hypothesized causal sequence. Traditional cognitive therapy processes did not exhibit similar temporal patterns in this treatment.
However, not all process research supports clear mediation. Bilich and Ciarrochi found that ACT improved mental health and values-based living in police officers, but AAQ scores did not change during intervention.85 This null finding on the primary process measure raises questions about whether measured flexibility actually captured the therapeutic change process or whether ACT operated through unmeasured mechanisms.
Component Studies
Component studies systematically vary intervention elements to determine which components contribute to outcomes. Levin et al conducted a meta-analysis of laboratory-based component studies examining psychological flexibility processes.39 Brief exercises targeting acceptance, defusion, values, and present-moment awareness produced medium-sized effects on behavioral outcomes like pain tolerance, distress tolerance, and task persistence.
However, translating laboratory findings to clinical contexts remains challenging. Brief exercises showing effects in controlled settings may function differently when embedded in comprehensive treatment protocols. The ecological validity of laboratory behavioral outcomes compared to real-world functioning remains uncertain.
Arch et al have compared complete ACT protocols with versions that emphasize particular processes.86 In one study comparing cognitive behavioral therapy to ACT for anxiety disorders, they found both treatments equally effective but operating through different processes. ACT produced greater increases in mindfulness and acceptance, while CBT showed larger changes in cognitive reappraisal. Both process changes predicted outcomes within their respective treatments, suggesting multiple pathways to symptom reduction exist.
Boundary Conditions and Moderators
Identifying who benefits most from flexibility-based interventions and under what conditions proves critical for personalized treatment. Research has begun examining moderators of ACT effects.87
Some evidence suggests baseline flexibility moderates treatment response. Fledderus et al found that participants with higher initial flexibility showed stronger reactions to guided self-help ACT.70 This finding seems counterintuitive: if flexibility is what ACT targets, those low in flexibility should benefit most. However, the result may indicate that some minimal level of flexibility is necessary to engage effectively with ACT exercises and principles.
Personality characteristics may moderate ACT effects. Preliminary evidence suggests that openness to experience is positively associated with ACT engagement and outcomes.87 Individuals high in neuroticism may benefit particularly from acceptance-based approaches, though findings remain mixed across studies.
Condition-specific factors also moderate outcomes. ACT appears particularly effective for conditions characterized by experiential avoidance, such as chronic pain, generalized anxiety disorder, and substance use disorders. Conditions in which cognitive content is central to pathology may benefit from approaches that address thought content more directly.16
Cultural factors require consideration. Most ACT research has occurred in Western, educated, industrialized, prosperous, and democratic societies.88 The relevance and optimal cultivation methods of psychological flexibility may differ across cultural contexts.14 Preliminary cross-cultural research suggests that flexibility predicts well-being across diverse cultures, but specific processes may function differently.89 For example, the emphasis on individual values in ACT may require adaptation in collectivist cultures where family and community values take precedence.
Internet-based ACT has shown effects on psychological flexibility processes comparable to those of in-person delivery, opening new avenues for scalable, equitable access to flexibility-based interventions across diverse populations.64
Applications Across Populations
Anxiety Disorders
Anxiety disorders represent one of the most extensively studied applications of ACT and psychological flexibility. The model proposes that anxiety becomes problematic less through its presence than through attempts to suppress or avoid it. Experiential avoidance of anxiety often maintains the disorder by preventing corrective learning and interfering with valued living.26
Arch et al conducted a randomized trial comparing ACT to cognitive behavioral therapy for mixed anxiety disorders.86 Both treatments produced significant improvements with large effect sizes and no differences in efficacy. However, treatments operated through different processes: ACT showed greater effects on experiential avoidance while CBT produced larger changes in worry and cognitive reappraisal.
Specific anxiety disorders have received targeted attention. Dalrymple and Herbert tested ACT for social anxiety disorder, finding large pre-post effect sizes on social anxiety and quality of life maintained at follow-up.90 Treatment emphasized accepting anxiety sensations and anxious thoughts while engaging in valued social activities.
For generalized anxiety disorder, ACT targets the function of worry rather than its content. Rather than challenging specific worry content, ACT helps individuals recognize worry as a mental behavior that serves avoidance functions.91 Treatment cultivates mindfulness of present-moment experience as an alternative to future-focused worry, while values work motivates behavioral activation despite uncertainty about future outcomes.
Obsessive-compulsive disorder presents unique challenges given the condition’s focus on intrusive thoughts and compulsive rituals.92 ACT approaches involve exposing clients to obsessive content while preventing compulsions, framing this practice differently from standard ERP: rather than promoting habituation to feared content, ACT emphasizes willingness to experience obsessions as mental events while refraining from compulsions, as doing so better serves values.
Depressive Disorders
Depression involves not only a sad mood but also behavioral withdrawal, rumination, and difficulty engaging in previously enjoyed activities. Psychological inflexibility contributes to depression through multiple pathways: experiential avoidance of negative emotions, cognitive fusion with depressive thoughts, loss of present-moment awareness through rumination, identification with a depressed self-concept, disconnection from values, and behavioral inaction.4
Forman et al compared ACT to cognitive therapy for anxiety and depression in a community mental health setting.93 Both treatments produced equivalent improvements in depression and anxiety with large effect sizes. Results supported the effectiveness of ACT in real-world clinical settings across diagnostically heterogeneous samples.
ACT interventions for depression typically emphasize values-guided behavioral activation rather than mood.94 Traditional behavioral activation instructs clients to engage in pleasant activities to improve mood. Values-based behavioral activation asks clients to engage in meaningful activities regardless of current mood, accepting that initial activation may occur without mood improvement.95 This approach addresses the common clinical observation that depressed clients often wait to feel motivated before acting, perpetuating inactivity.
Rumination represents a key maintaining factor in depression.40 From a flexibility perspective, rumination constitutes a form of cognitive fusion where individuals become entangled with depressive thinking patterns. Defusion techniques help clients observe ruminative thoughts without becoming absorbed in their content. Mindfulness practices shift attention from mental time travel to present-moment experience.
Self-as-context proves particularly relevant for depression, given that depressed individuals often identify strongly with negative self-concepts. ACT helps clients distinguish between self-as-content (eg., “I am worthless”) and self-as-context (eg., “I am having the thought that I am worthless”). This distinction creates flexibility: thoughts about oneself become observations rather than definitions.
Chronic Pain
Chronic pain has been described as an exemplar application for psychological flexibility.96 Traditional pain management often emphasizes pain reduction as the primary goal. However, many chronic pain conditions prove resistant to complete pain elimination. Continued pursuit of pain relief through medical interventions, activity avoidance, and medication can paradoxically worsen functioning and quality of life.
ACT for chronic pain shifts the goal from pain elimination to valued living despite pain. The approach distinguishes between clean pain (unavoidable physical sensations) and dirty pain (additional suffering created by struggling against pain). Treatment targets experiential avoidance of pain, cognitive fusion with pain-related thoughts, and behavioral withdrawal.96
McCracken et al have extensively studied psychological flexibility in chronic pain populations.96,97 Their research demonstrates that pain acceptance predicts functioning better than pain intensity. Patients who accept pain as a part of their experience while engaging in valued activities show better outcomes than those who achieve slightly lower pain levels through avoidance.
The Chronic Pain Acceptance Questionnaire assesses two dimensions: pain willingness (readiness to experience pain) and activities engagement (pursuing valued activities despite pain).45 Both dimensions predict functioning, disability, and psychological adjustment. Interventions targeting acceptance show medium to large effects on pain-related disability and psychological distress, with smaller effects on pain intensity itself.
Recent meta-analyses support the efficacy of ACT for chronic pain. Hughes et al found that ACT was superior to control conditions across various outcomes, with effects larger for psychological than somatic outcomes.54 Multiple recent meta-analyses have further confirmed and extended this evidence base: Lai et al demonstrated efficacy using three-level meta-analytic methods,55 Ma et al reported consistent benefits across diverse chronic pain conditions,56 Martinez-Calderon et al synthesized findings across systematic reviews,57 and Ye et al confirmed durable effects at follow-up.58 Collectively, these studies establish ACT as one of the most well-evidenced psychological interventions for chronic pain.
Substance Use Disorders
Substance use involves complex interactions between physiological dependence, environmental triggers, and psychological processes.98 Psychological inflexibility contributes through experiential avoidance of negative emotions and cravings, cognitive fusion with addiction-related thoughts, values confusion or disconnection, and difficulty maintaining committed action toward recovery.
Lee et al meta-analyzed ACT for substance use across randomized trials.59 Results indicated moderate effects on substance use outcomes, with ACT showing advantages over control conditions and comparable outcomes to established treatments. Dropout rates did not differ between ACT and comparison interventions.
ACT interventions for substance use typically emphasize accepting cravings and negative emotions without using substances.78 Rather than attempting to eliminate cravings through avoidance or distraction, clients practice observing cravings as temporary physiological states while choosing not to use.
Values work proves particularly important in addiction treatment. Substance use often develops as a means of coping with experiential avoidance, providing temporary relief from difficult emotions. However, continued use increasingly conflicts with important values related to health, relationships, work, and self-respect.99 ACT helps clients reconnect with these values and use them as motivation for behavioral change.
Defusion techniques address cognitive triggers for use. Thoughts like “I deserve a drink after this stressful day” or “One time won’t hurt” can precipitate relapse when taken literally. Defusion creates distance from such thoughts, allowing clients to recognize them as mental events rather than commands requiring action.
Research specifically examining psychological flexibility mechanisms in addiction treatment remains limited. Ii et al conducted a systematic review, finding that flexibility-based interventions showed promise but noted the need for more rigorous process research.100 A recent meta-analysis by Krotter et al confirmed these findings across a range of addictive behaviors, demonstrating that ACT-based interventions consistently outperformed control conditions and showed comparable efficacy to other active treatments.60
Eating Disorders and Body Image
Eating disorders involve both behavioral symptoms (restriction, binge eating, purging) and psychological processes, including experiential avoidance of negative body-related emotions, cognitive fusion with appearance-related thoughts, values confusion, and rigid rule-following regarding eating.101
Juarascio et al adapted ACT for binge eating disorder, emphasizing acceptance of food cravings and negative emotions while choosing eating behaviors consistent with health values.101 A pilot randomized trial found preliminary support for the intervention’s feasibility and acceptability. Participants showed reductions in binge eating frequency and improvements in psychological flexibility.
Body image represents another application area. The Body Image Acceptance and Action Questionnaire assesses willingness to experience body-related discomfort while engaging in valued activities.47 Research indicates that body image flexibility predicts quality of life and psychological adjustment better than body dissatisfaction itself.
ACT interventions for body image target cognitive fusion with appearance-related thoughts and experiential avoidance of situations where body concerns arise.102 Rather than attempting to improve body satisfaction or challenge negative body thoughts, interventions emphasize willingness to have body concerns while pursuing meaningful social connections, physical activity, and self-care.
Research evidence remains preliminary compared to other disorder categories. More randomized controlled trials with adequate sample sizes and follow-up assessments are needed.103 Questions remain about whether flexibility-based approaches add value beyond established treatments for eating disorders.
A systematic review by Onnink et al provided an updated evidence base for ACT in eating disorders, noting promising results across a range of diagnostic presentations while highlighting the need for methodologically stronger trials.104
Critical Evaluation
The accumulated theoretical, measurement, and empirical evidence reviewed above provides the basis for a balanced critical appraisal of the flexibility model’s genuine strengths and the methodological constraints that currently limit its explanatory scope.
Strengths of the Psychological Flexibility Model
The psychological flexibility model offers several advantages as a framework for understanding psychopathology and treatment. First, the transdiagnostic nature proves conceptually and practically valuable.37 Rather than developing separate models for each disorder, psychological flexibility provides a unified account of diverse conditions.105 This parsimony is theoretically elegant and clinically valuable, as many clients present with multiple comorbid conditions that are better addressed through common processes than through disorder-specific protocols.106
Second, the model’s grounding in basic behavioral science through Relational Frame Theory provides theoretical coherence. Unlike some therapeutic approaches developed primarily through clinical observation, ACT derives from an explicit account of language and cognition.19 This foundation allows for systematic investigation of hypothesized mechanisms through both laboratory and clinical research.
Third, the emphasis on functional contextualism proves clinically valuable. By focusing on workability rather than symptom frequency, the model avoids the trap of evaluating thoughts and feelings as inherently good or bad. This perspective reduces shame and self-criticism that often accompany psychological difficulties, as clients learn that uncomfortable experiences can be had while still moving in valued directions.107
Fourth, the extensive empirical literature supporting ACT demonstrates the model’s heuristic value. The exponential growth in research output indicates that psychological flexibility generates productive lines of investigation across diverse populations and contexts. Meta-analytic evidence consistently supports relationships between flexibility and adaptive outcomes.11,53
Fifth, the model’s clinical accessibility benefits practitioners. The hexaflex provides clear targets for intervention, and numerous treatment manuals and resources support implementation.6,37 Metaphors and experiential exercises make abstract concepts tangible for clients.108 Training programs have successfully disseminated ACT to diverse provider groups.109
Flexibility-related constructs have independent histories in cognitive psychology and personality science. Cognitive flexibility, as studied in executive function research, refers to the capacity to shift mental sets and adapt strategies in response to changing task demands.110 In personality psychology, openness to experience overlaps conceptually with the capacity for flexible responding to novel stimuli.111 Neuropsychologically, flexibility processes implicate prefrontal-mediated response inhibition and cognitive set-shifting, providing a biological substrate that partially converges with the ACT model.112 Contrasting these perspectives with the clinical ACT framework reveals an important divergence: while neuropsychological models emphasize structural-executive capacities, ACT emphasizes the functional context of behavioral responding and the role of verbal-regulatory processes in sustaining inflexibility. Both levels of analysis are necessary for a complete account of the construct.
Limitations and Methodological Concerns
Despite its strengths, significant limitations warrant consideration. Measurement challenges pose the most prominent concern. The AAQ-II exhibits problematic psychometric properties in some studies, including high correlations with general distress measures, raising questions about its discriminant validity.13,43 Whether the measure assesses flexibility specifically or captures broader negative affect remains a matter of debate.
The issue of construct specificity extends beyond measurement. Do psychological flexibility processes uniquely characterize ACT, or do other evidence-based treatments target similar processes under different names16? Research comparing ACT to cognitive-behavioral therapy often finds both treatments similarly effective with overlapping process changes.86 This raises questions about whether theoretical distinctions between approaches prove more semantic than substantive.
Mediation research faces substantial methodological limitations. Arch et al comprehensively reviewed these concerns: inadequate sample sizes to detect mediation effects, cross-sectional designs that cannot establish temporal precedence, failure to demonstrate the treatment specificity of process changes, and statistical approaches that do not adequately test causal mediation.12 Much existing mediation research may overestimate the certainty of causal conclusions.
The causal status of psychological flexibility remains incompletely established. Most research demonstrates correlational relationships between flexibility and outcomes.41 Longitudinal studies examining whether flexibility precedes and predicts later mental health outcomes while controlling for baseline mental health remain rare.17 Without such evidence, the direction of causality remains ambiguous: does inflexibility cause psychopathology, does psychopathology produce inflexibility, or do reciprocal relationships exist?
Publication bias likely affects the literature. Studies reporting null or negative results for ACT interventions may be less likely to be published than those reporting positive findings.113 Meta-analyses attempt to assess publication bias through funnel plots and related techniques, but these methods cannot fully account for missing data. The actual effect sizes for ACT may be smaller than those reported in published meta-analyses.114
Cultural limitations require acknowledgment. Most research occurs in Western contexts with predominantly white, educated samples.88 Whether psychological flexibility operates similarly across cultural contexts remains uncertain. The emphasis on individual values may prove less relevant in collectivist cultures.89 More research in diverse cultural settings is needed.
Questions arise about the clinical significance versus statistical significance. Many meta-analyses report small to medium effect sizes.53 While statistically significant, whether such effects represent clinically meaningful improvements for individual clients remains unclear.114 More research reporting clinical significance metrics, including responder analyses and reliable change indices, would strengthen the literature.115
The relationship between ACT and traditional cognitive-behavioral therapy remains contested. Some researchers view ACT as a distinct approach with unique theoretical foundations and therapeutic processes.4 Others consider ACT a variant of cognitive-behavioral therapy that shares more similarities than differences with established CBT approaches.16 This ongoing debate has generated productive scientific discourse but also confusion among practitioners and researchers about how to categorize and study ACT.
A further concern is the concentration of authorship in the psychological flexibility literature, where a disproportionate share of influential empirical and theoretical work originates with ACT’s core developers. Researchers from the broader cognitive-behavioral tradition have demonstrated that CBT achieves clinically equivalent outcomes through partially overlapping process changes,2 suggesting that flexibility may not be uniquely catalytic. DBT researchers have similarly documented sustained improvements in behavioral flexibility through acceptance-based distress tolerance training in borderline personality disorder, with outcomes maintained at multi-year follow-up.116 Integrating these perspectives more systematically would sharpen understanding of what is uniquely attributable to ACT-specific flexibility processes versus common therapeutic factors shared across evidence-based interventions.
Research Gaps and Future Directions
Despite substantial progress in psychological flexibility research, several critical gaps remain that limit a comprehensive understanding of the construct and its applications. First, the field lacks adequate longitudinal research establishing the temporal precedence of flexibility with respect to mental health outcomes. Most existing studies employ cross-sectional or short-term designs that cannot determine whether inflexibility represents a causal risk factor, a consequence of psychopathology, or a bidirectional relationship.17 Prospective studies following individuals before disorder onset would clarify whether inflexibility predicts first-episode psychopathology. Ecological momentary assessment approaches that capture real-time relationships between flexibility processes and valued behavior in natural contexts would provide rich data on dynamic within-person processes.117
Second, measurement limitations continue to constrain research progress. The AAQ-II’s questionable discriminant validity raises concerns about whether studies assess psychological flexibility specifically or general distress more broadly.13,43 Developing measures with stronger psychometric properties that clearly distinguish flexibility from overlapping constructs is a priority. Behavioral and physiological measures, when used alongside self-report, would reduce common method variance and provide converging evidence. Idiographic assessment approaches that capture person-specific flexibility relative to individualized values show promise but require further validation.50,51
Third, mediation research suffers from methodological weaknesses that undermine causal inferences.12 Studies typically lack adequate sample sizes for detecting mediation effects with sufficient statistical power. Cross-sectional designs dominate despite their inability to establish temporal precedence. Advanced statistical approaches, including cross-lagged panel models, latent growth curve modeling, and dynamic systems methods, could strengthen causal inference.
Fourth, systematic dismantling studies examining which ACT components are essential versus peripheral remain rare.39 The field lacks clarity about whether all six hexaflex processes contribute equally to outcomes, or whether some processes are more potent under specific conditions or populations. Component research could inform more efficient interventions targeting core active ingredients.
Fifth, research on personalization that identifies who benefits most from flexibility-based approaches and under what conditions remains limited.87 Machine learning approaches that analyze patterns across multiple variables may identify profiles that predict differential responses to ACT versus alternative treatments, supporting precision intervention and treatment matching.
Sixth, research on cultural adaptation in diverse global contexts remains insufficient.14,88 Whether core assumptions about selfhood, emotion regulation, and values hold across cultures remains to be investigated. The emphasis on individual values may require substantial modification in collectivist cultures. Indigenous psychology approaches might identify culture-specific manifestations of flexibility.
Seventh, implementation research examining effective dissemination of psychological flexibility interventions in community settings would enhance public health impact.118 Scalable delivery methods, including digital and internet-based interventions, group formats, and brief interventions, deserve investigation.64 Training models that successfully teach practitioners to deliver flexibility-based interventions competently require evaluation.
Eighth, the field needs research examining psychological flexibility across the lifespan. Most studies focus on adults, with limited research on children, adolescents, and older adults.119 Research on ACT for adolescents remains particularly limited, though recent reviews suggest promising applications across school-based, clinical, and community settings.120 Developmental trajectories of flexibility processes remain poorly understood. Age-appropriate assessment methods and interventions require development and validation.
Ninth, neurobiological research linking psychological flexibility to brain structure and function remains nascent. Neuroimaging studies examining neural correlates of flexibility processes could validate theoretical models and identify neural mechanisms. Research on how flexibility-based interventions alter brain function would strengthen understanding of therapeutic mechanisms.
Tenth, economic evaluation research assessing the cost-effectiveness of flexibility-based interventions compared to established treatments remains limited. Health economic analyses examining treatment costs, healthcare utilization, work productivity, and quality-adjusted life years would inform resource allocation decisions and policy recommendations.
Among these priorities, three are most urgently required. First, prospective longitudinal designs with multiple assessment points are needed to determine whether psychological inflexibility is a causal antecedent of psychopathology, a consequence, or part of a bidirectional feedback process. Second, the development of psychometrically robust, transculturally validated assessment instruments is essential to advance both scientific inquiry and equitable clinical application. Third, systematic cultural adaptation research is required to determine whether the psychological flexibility construct and its associated interventions are genuinely generalisable beyond predominantly Western, WEIRD samples, or whether fundamental reconceptualization is needed in non-Western cultural frameworks.
Our ten proposed directions substantially converge with the six priorities advanced by Macri et al,18 particularly regarding process-specific investigation, longitudinal methodology, and measurement refinement. Our review extends their agenda by incorporating additional priorities specific to cultural generalizability, neurobiological underpinnings, lifespan development, implementation science, and health economic evaluation, reflecting the broader transdiagnostic and global scope of the present synthesis.
Conclusion
Psychological flexibility has established itself as a significant construct in contemporary psychological science. The capacity to remain present with difficult experiences while pursuing valued directions represents a fundamental aspect of adaptive human functioning. The theoretical foundation in Relational Frame Theory provides a coherent account of how language and cognition create both possibilities and vulnerabilities. The six-process hexaflex model offers clinically useful targets spanning acceptance, cognitive defusion, present-moment awareness, self-as-context, values, and committed action.
Measurement approaches have facilitated systematic investigation despite ongoing psychometric concerns. Meta-analytic evidence demonstrates relationships between flexibility and diverse outcomes, including depression, anxiety, chronic pain, substance use, and workplace functioning. Effect sizes typically range from small to medium, with variation across populations and outcome domains. Process research provides preliminary support for flexibility as a mechanism of change, though methodological limitations temper certainty about causal conclusions.
Applications span clinical conditions, organizational settings, health behaviors, and non-clinical populations. Evidence proves strongest for chronic pain, where accepting pain while engaging in valued activities produces better functioning than the single-minded pursuit of pain elimination. Anxiety and depressive disorders show good response to flexibility-based interventions, with outcomes comparable to established treatments. Substance use disorders, eating pathology, and other conditions show promise, though they require more research.
Critical evaluation reveals both strengths and limitations. The transdiagnostic nature of the concept proves conceptually elegant and clinically useful. Grounding in basic science provides theoretical coherence. Clinical accessibility facilitates dissemination. However, measurement challenges, questions about construct specificity, limitations in mediation research, uncertainty about causal status, and cultural constraints require acknowledgment.
Beyond cataloguing existing evidence, this review supports a substantive reconceptualization of psychological flexibility as a dynamic, context-sensitive regulatory capacity rather than a stable individual trait. This reframing is not merely semantic; it carries direct and concrete implications. If flexibility is inherently context-dependent rather than dispositional, then its measurement must be idiographic and ecologically sensitive rather than reliant exclusively on decontextualized global self-report instruments. If it is malleable and cultivable at any point across the lifespan, then intervention timing and intensity may be calibrated more precisely than current protocol-based approaches allow. And if its expression reflects the interaction between individual regulatory tendencies and situational demands, then understanding its variability across cultural contexts becomes a central scientific priority rather than a peripheral refinement. This integrative perspective aligns the ACT flexibility model with contemporary regulatory science, developmental psychology, and cross-cultural behavioral science, offering a theoretically coherent organizing framework for the next generation of research in this domain.
Multiple research gaps constrain a comprehensive understanding of psychological flexibility. The field needs longitudinal research establishing temporal precedence, refined measurement tools with stronger discriminant validity, methodologically rigorous mediation research with adequate power and temporal assessment, dismantling studies identifying essential components, personalization research supporting treatment matching, cultural adaptation studies in diverse contexts, implementation research facilitating dissemination, developmental research across the lifespan, neurobiological research examining neural mechanisms, and economic evaluation research assessing cost-effectiveness. Among these, longitudinal causal designs, culturally validated measurement, and systematic cross-cultural adaptation research are most urgently needed.
Despite limitations, psychological flexibility demonstrates sufficient empirical support and clinical utility to warrant continued investigation and application. For clinicians, the most immediate and actionable implication of this body of evidence is that targeting psychological flexibility through values-guided, acceptance-based interventions offers a unifying and empirically grounded pathway to improving mental health outcomes across a broad range of clinical presentations, without the need for disorder-specific protocol switching, making psychological flexibility one of the most versatile, theoretically coherent, and clinically accessible constructs available to contemporary practice.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
Ethics Statement
Ethical review and approval were not required for this study, as it is a narrative review based solely on previously published, publicly available literature. No primary data were collected from human or animal subjects.
Acknowledgments
The authors wish to thank the Reviewers and the Editors for their constructive and detailed feedback, which substantially improved the quality and clarity of this manuscript.
Author Contributions
Noomen Guelmami and Ismail Dergaa share co-last authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this study.
Disclosure
The authors declare that this research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. World Mental Health Report: Transforming Mental Health for All. Geneva: WHO; 2022.
2. Hayes SC, Hofmann SG. Process-Based CBT: The Science and Core Clinical Competencies of Cognitive Behavioral Therapy. New Harbinger Publications; 2018.
3. Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. 2010;30(7):865–23. doi:10.1016/j.cpr.2010.03.001
4. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44(1):1–25. doi:10.1016/j.brat.2005.06.006
5. Rush AJ. At the research front: cognitive therapy for depression. Aust N Z J Psychiatry. 1979;13(1):13–16. doi:10.3109/00048677909159104
6. Hayes SC, Strosahl K, Wilson KG. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change. New York: Guilford Press; 1999.
7. Hayes SC. A contextual approach to therapeutic change. In: Psychotherapists in Clinical Practice: Cognitive and Behavioral Perspectives. New York: Guilford Press; 1987:327–387.
8. Bluett EJ, Homan KJ, Morrison KL, Levin ME, Twohig MP. Acceptance and commitment therapy for anxiety and OCD spectrum disorders: an empirical review. J Anxiety Disord. 2014;28(6):612–624. doi:10.1016/j.janxdis.2014.06.008
9. Linehan MM. Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: Guilford Press; 1993.
10. Segal ZV, Williams JMG, Teasdale JD. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse. New York: Guilford Press; 2002.
11. Gloster AT, Walder N, Levin ME, Twohig MP, Karekla M. The empirical status of acceptance and commitment therapy: a review of meta-analyses. J Context Behav Sci. 2020;18:181–192. doi:10.1016/j.jcbs.2020.09.009
12. Arch JJ, Fishbein JN, Finkelstein LB, Luoma JB. Acceptance and commitment therapy processes and mediation: challenges and how to address them. Behav Ther. 2023;54(6):971–988. doi:10.1016/j.beth.2022.07.005
13. Wolgast M. What does the Acceptance and Action Questionnaire (AAQ-II) really measure? Behav Ther. 2014;45(6):831–839. doi:10.1016/j.beth.2014.07.002
14. Masuda A, Wendell JW. Mindfulness mediates the relation between disordered eating-related cognitions and psychological distress. Eat Behav. 2010;11(4):293–296. doi:10.1016/j.eatbeh.2010.07.001
15. Gaudiano BA. A review of acceptance and commitment therapy (ACT) and recommendations for continued scientific advancement. Sci Rev Ment Health Pract. 2011;8(2):5–22.
16. Hofmann SG, Asmundson GJ. Acceptance and mindfulness-based therapy: new wave or old hat? Clin Psychol Rev. 2008;28(1):1–16. doi:10.1016/j.cpr.2007.09.003
17. Spinhoven P, Drost J, De Rooij M, Van Hemert AM, Penninx BWJH. Is experiential avoidance a mediating, moderating, independent, overlapping, or proxy risk factor in the onset, relapse and maintenance of depressive disorders? Cognit Ther Res. 2016;40(2):150–163. doi:10.1007/s10608-015-9747-8
18. Macri JA, Ong CW, Levin ME, Hayes SC, Gershkovich M. Examining domains of psychological flexibility and inflexibility as treatment mechanisms in acceptance and commitment therapy: a comprehensive systematic and meta-analytic review. Clin Psychol Rev. 2024;110:102432. doi:10.1016/j.cpr.2024.102432
19. Hayes SC, Barnes-Holmes D, Roche B. Relational Frame Theory: a Post-Skinnerian Account of Human Language and Cognition. In: Hayes SC, Barnes-Holmes D, Roche B, editors. Relational Frame Theory: A Precis. New York: Kluwer Academic/Plenum; 2001:141–154.
20. Torneke N. Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Oakland: New Harbinger Publications; 2010.
21. Barnes-Holmes Y, Hayes SC, Barnes-Holmes D, Roche B. Relational frame theory: a post-Skinnerian account of human language and cognition. Adv Child Dev Behav. 2001;28:101–138.
22. Dymond S, Rehfeldt RA. Understanding complex behavior: the transformation of stimulus functions. Behav Anal. 2000;23(2):239–254. doi:10.1007/BF03392013
23. Barnes-Holmes Y, Barnes-Holmes D, McHugh L, Hayes SC. Relational frame theory: some implications for understanding and treating human psychopathology. Int J Psychol Psychol Ther. 2004;4(2):355–375.
24. Hayes SC, Strosahl K, Wilson KG, et al. Measuring experiential avoidance: a preliminary test of a working model. Psychol Rec. 2004;54(4):553–578. doi:10.1007/BF03395492
25. Gillanders DT, Bolderston H, Bond FW, et al. The development and initial validation of the Cognitive Fusion Questionnaire. Behav Ther. 2014;45(1):83–101. doi:10.1016/j.beth.2013.09.001
26. Chawla N, Ostafin B. Experiential avoidance as a functional dimensional approach to psychopathology: an empirical review. J Clin Psychol. 2007;63(9):871–890. doi:10.1002/jclp.20400
27. Masuda A, Hayes SC, Sackett CF, Twohig MP. Cognitive defusion and self-relevant negative thoughts: examining the impact of a ninety year old technique. Behav Res Ther. 2004;42(4):477–485. doi:10.1016/j.brat.2003.10.008
28. Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822–848. doi:10.1037/0022-3514.84.4.822
29. Kabat-Zinn J. Full Catastrophe Living: The Program of the Stress Reduction Clinic at the University of Massachusetts Medical Center. New York: Delta; 1990.
30. Raes F, Williams JMG. The relationship between mindfulness and uncontrollability of ruminative thinking. Mindfulness. 2010;1(4):199–203. doi:10.1007/s12671-010-0021-6
31. McHugh L, Barnes-Holmes Y, Barnes-Holmes D. Perspective-taking as relational responding: a developmental profile. Psychol Rec. 2004;54(1):115–144. doi:10.1007/BF03395465
32. Godbee M, Kangas M. The relationship between flexible perspective taking and emotional well-being: a systematic review of the “self as context” component of acceptance and commitment therapy. Behav Ther. 2020;51(6):917–932. doi:10.1016/j.beth.2019.12.010
33. Dahl J, Plumb JC, Lundgren T, Stewart I. The Art and Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Commit to Valued Action Using Acceptance and Commitment Therapy. Oakland: New Harbinger; 2009.
34. Tunc H, Morris PG, Kyranides MN, McArdle A, McConachie D, Williams J. The relationships between valued living and depression and anxiety: a systematic review, meta-analysis, and meta-regression. J Context Behav Sci. 2023;28:102–126. doi:10.1016/j.jcbs.2023.02.004
35. Wilson KG, Sandoz EK, Kitchens J, Roberts M. The valued living questionnaire: defining and measuring valued action within a behavioral framework. Psychol Rec. 2010;60(2):249–272. doi:10.1007/BF03395706
36. McCracken LM. Committed action: an application of the psychological flexibility model to activity patterns in chronic pain. J Pain. 2013;14(8):828–835. doi:10.1016/j.jpain.2013.02.009
37. Hayes SC, Pistorello J, Levin ME. Acceptance and commitment therapy as a unified model of behavior change. Couns Psychol. 2012;40(7):976–1002. doi:10.1177/0011000012460836
38. Bond FW, Bunce D. The role of acceptance and job control in mental health, job satisfaction, and work performance. J Appl Psychol. 2003;88(6):1057–1067. doi:10.1037/0021-9010.88.6.1057
39. Levin ME, Hildebrandt MJ, Lillis J, Hayes SC. The impact of treatment components suggested by the psychological flexibility model: a meta-analysis of laboratory-based component studies. Behav Ther. 2012;43(4):741–756. doi:10.1016/j.beth.2012.05.003
40. Nolen-Hoeksema S. The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J Abnorm Psychol. 2000;109(3):504–511. doi:10.1037/0021-843X.109.3.504
41. Ruiz FJ. A review of acceptance and commitment therapy (ACT) empirical evidence: correlational, experimental psychopathology, component and outcome studies. Int J Psychol Psychol Ther. 2010;10(1):125–162.
42. Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42(4):676–688. doi:10.1016/j.beth.2011.03.007
43. Rochefort C, Baldwin AS, Chmielewski M. Experiential avoidance: an examination of the construct validity of the AAQ-II and MEAQ. Behav Ther. 2018;49(3):435–449. doi:10.1016/j.beth.2017.08.008
44. Bond FW, Lloyd J, Guenole N. The work-related acceptance and action questionnaire: initial psychometric findings and their implications for measuring psychological flexibility in specific contexts. J Occup Organ Psychol. 2013;86(3):331–347. doi:10.1111/joop.12001
45. McCracken LM, Vowles KE, Eccleston C. Acceptance of chronic pain: component analysis and a revised assessment method. Pain. 2004;107(1–2):159–166. doi:10.1016/j.pain.2003.10.012
46. Cheron DM, Ehrenreich JT, Pincus DB. Assessment of parental experiential avoidance in a clinical sample of children with anxiety disorders. Child Psychiatry Hum Dev. 2009;40(3):383–403. doi:10.1007/s10578-009-0135-z
47. Sandoz EK, Wilson KG, Merwin RM, Kellum KK. Assessment of body image flexibility: the body image-acceptance and action questionnaire. J Context Behav Sci. 2013;2(1–2):39–48. doi:10.1016/j.jcbs.2013.03.002
48. Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006;13(1):27–45. doi:10.1177/1073191105283504
49. Stockton D, Kellett S, Berrios R, Sirois F, Wilkinson N, Miles G. Identifying the underlying mechanisms of change during acceptance and commitment therapy (ACT): a systematic review of contemporary mediation studies. Behav Cogn Psychother. 2019;47(3):332–362. doi:10.1017/S1352465818000553
50. Kashdan TB, Disabato DJ, Goodman FR, Doorley JD, McKnight PE. Understanding psychological flexibility: a multimethod exploration of pursuing valued goals despite the presence of distress. Psychol Assess. 2020;32(9):829–850. doi:10.1037/pas0000834
51. Gloster AT, Block VJ, Klotsche J, et al. Psy-Flex: a contextually sensitive measure of psychological flexibility. J Context Behav Sci. 2021;22:13–23. doi:10.1016/j.jcbs.2021.09.001
52. Feldner MT, Hekmat H, Zvolensky MJ, Vowles KE, Secrist Z, Leen-Feldner EW. The role of experiential avoidance in acute pain tolerance: a laboratory test. J Behav Ther Exp Psychiatry. 2006;37(2):146–158. doi:10.1016/j.jbtep.2005.03.002
53. A-Tjak JGL, Davis ML, Morina N, Powers MB, Smits JAJ, Emmelkamp PMG. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychother Psychosom. 2015;84(1):30–36. doi:10.1159/000365764
54. Hughes LS, Clark J, Colclough JA, Dale E, McMillan D. Acceptance and commitment therapy (ACT) for chronic pain: a systematic review and meta-analyses. Clin J Pain. 2017;33(6):552–568. doi:10.1097/AJP.0000000000000425
55. Lai L, Liu Y, McCracken LM, Li Y, Ren Z. The efficacy of acceptance and commitment therapy for chronic pain: a three-level meta-analysis and a trial sequential analysis of randomized controlled trials. Behav Res Ther. 2023;165:104308. doi:10.1016/j.brat.2023.104308
56. Ma TW, Yuen AS, Yang Z. The efficacy of acceptance and commitment therapy for chronic pain: a systematic review and meta-analysis. Clin J Pain. 2023;39(3):147–157. doi:10.1097/AJP.0000000000001096
57. Martinez-Calderon J, Garcia-Munoz C, Rufo-Barbero C, Matias-Soto J, Cano-Garcia FJ. Acceptance and commitment therapy for chronic pain conditions: an overview of systematic reviews. J Pain. 2024;25(3):595–617. doi:10.1016/j.jpain.2023.09.013
58. Ye L, Li Y, Deng Q, Zhao X, Zhong L, Yang L. Acceptance and commitment therapy for patients with chronic pain: a systematic review and meta-analysis on psychological outcomes and quality of life. PLoS One. 2024;19(6):e0301226. doi:10.1371/journal.pone.0301226
59. Lee EB, An W, Levin ME, Twohig MP. An initial meta-analysis of acceptance and commitment therapy for treating substance use disorders. Drug Alcohol Depend. 2015;155:1–7. doi:10.1016/j.drugalcdep.2015.08.004
60. Krotter A, Aonso-Diego G, Gonzalez-Menendez A, Gonzalez-Roz A, Secades-Villa R, Garcia-Perez A. Effectiveness of acceptance and commitment therapy for addictive behaviors: a systematic review and meta-analysis. J Context Behav Sci. 2024;32:100773. doi:10.1016/j.jcbs.2024.100773
61. Prudenzi A, Graham CD, Flaxman PE, Wilding S, Day F, O’Connor DB. A workplace acceptance and commitment therapy (ACT) intervention for improving healthcare staff psychological distress: a randomised controlled trial. PLoS One. 2022;17(4):e0266357. doi:10.1371/journal.pone.0266357
62. Unruh I, Neubert M, Wilhelm M, Euteneuer F. ACT in the workplace: a meta-analytic examination of randomized controlled trials. J Context Behav Sci. 2022;26:114–124. doi:10.1016/j.jcbs.2022.09.003
63. Hsu T, Adamowicz JL, Thomas EBK. The effect of acceptance and commitment therapy on the psychological flexibility and inflexibility of undergraduate students: a systematic review and three-level meta-analysis. J Context Behav Sci. 2023;30:169–180. doi:10.1016/j.jcbs.2023.10.006
64. Han A, Kim TH. Effects of internet-based acceptance and commitment therapy on process measures: a systematic review and meta-analysis. J Med Internet Res. 2022;24(8):e39182. doi:10.2196/39182
65. Jiang X, Sun J, Song R, Wang Y, Li J, Shi R. Acceptance and commitment therapy reduces psychological distress in patients with cancer: a systematic review and meta-analysis of randomized controlled trials. Front Psychol. 2024;14:1253266. doi:10.3389/fpsyg.2023.1253266
66. Rutschmann R, Romanczuk-Seiferth N, Gloster A, Richter C. Increasing psychological flexibility is associated with positive therapy outcomes following a transdiagnostic ACT treatment. Front Psychiatry. 2024;15:1403718. doi:10.3389/fpsyt.2024.1403718
67. Pittman L, Krafft J, Levin ME, Twohig MP. The relationship between psychosis and psychological flexibility and other acceptance and commitment therapy processes: a systematic review and meta-analysis. J Context Behav Sci. 2024;31:100726.
68. Levin ME, Krafft J, Twohig MP. An overview of acceptance and commitment therapy research: concepts, components, and clinical applications. Psychiatr Clin North Am. 2024;47(2):419–431. doi:10.1016/j.psc.2024.02.007
69. Kazdin AE. Mediators and mechanisms of change in psychotherapy research. Annu Rev Clin Psychol. 2007;3(1):1–27. doi:10.1146/annurev.clinpsy.3.022806.091432
70. Fledderus M, Bohlmeijer ET, Pieterse ME, Schreurs KMG. Acceptance and commitment therapy as guided self-help for psychological distress and positive mental health: a randomized controlled trial. Psychol Med. 2012;42(3):485–495. doi:10.1017/S0033291711001206
71. Bond FW, Flaxman PE. The ability of psychological flexibility and job control to predict learning, job performance, and mental health. J Organ Behav Manag. 2006;26(1–2):113–130.
72. McCracken LM, Gutierrez-Martinez O. Processes of change in psychological flexibility in an interdisciplinary group-based treatment for chronic pain based on acceptance and commitment therapy. Behav Res Ther. 2011;49(4):267–274. doi:10.1016/j.brat.2011.02.004
73. Hayes SA, Orsillo SM, Roemer L. Changes in proposed mechanisms of action during an acceptance-based behavior therapy for generalized anxiety disorder. Behav Res Ther. 2010;48(3):238–245. doi:10.1016/j.brat.2009.11.006
74. Bond FW, Bunce D. Mediators of change in emotion-focused and problem-focused worksite stress management interventions. J Occup Health Psychol. 2000;5(1):156–163. doi:10.1037/1076-8998.5.1.156
75. Bond FW, Flaxman PE, Bunce D. The influence of psychological flexibility on work redesign: mediated moderation of a work reorganization intervention. J Appl Psychol. 2008;93(3):645–654. doi:10.1037/0021-9010.93.3.645
76. Lillis J, Hayes SC, Bunting K, Masuda A. Teaching acceptance and mindfulness to improve the lives of the obese: a preliminary test of a theoretical model. Ann Behav Med. 2009;37(1):58–69. doi:10.1007/s12160-009-9083-x
77. Iturbe I, Echeburua E, Maiz E. Acceptance and commitment therapy for overweight and obesity: a systematic review. Clin Psychol Psychother. 2022;29(3):837–856. doi:10.1002/cpp.2695
78. Gifford EV, Kohlenberg BS, Hayes SC, et al. Acceptance-based treatment for smoking cessation. Behav Ther. 2004;35(4):689–705. doi:10.1016/S0005-7894(04)80015-7
79. Bricker JB, Mull KE, Kientz JA, et al. Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug Alcohol Depend. 2014;143:87–94. doi:10.1016/j.drugalcdep.2014.07.006
80. Butryn ML, Forman E, Hoffman K, Shaw J, Juarascio A. A pilot study of acceptance and commitment therapy for promotion of physical activity. J Phys Act Health. 2011;8(4):516–522. doi:10.1123/jpah.8.4.516
81. Graham CD, Gouick J, Krahe C, Gillanders D. A systematic review of the use of acceptance and commitment therapy (ACT) in chronic illness and long-term conditions. Clin Psychol Rev. 2016;46:46–58. doi:10.1016/j.cpr.2016.04.009
82. Levin ME, Pistorello J, Seeley JR, Hayes SC. Feasibility of a prototype web-based acceptance and commitment therapy prevention program for college students. J Am Coll Health. 2014;62(1):20–30. doi:10.1080/07448481.2013.843533
83. Brassell AA, Rosenberg E, Parent J, Rough JN, Fondacaro K, Seehuus M. Parent’s psychological flexibility: associations with parenting and child psychosocial well-being. J Context Behav Sci. 2016;5(2):111–120. doi:10.1016/j.jcbs.2016.03.001
84. Blackledge JT, Hayes SC. Using acceptance and commitment training in the support of parents of children diagnosed with autism. Child Fam Behav Ther. 2006;28(1):1–18. doi:10.1300/J019v28n01_01
85. Ciarrochi J, Bilich L, Godsell C. Psychological flexibility as a mechanism of change in acceptance and commitment therapy. In: Baer RA, editor. Assessing Mindfulness and Acceptance Processes in Clients: Illuminating the Theory and Practice of Change. Oakland: New Harbinger; 2010:51–75.
86. Arch JJ, Eifert GH, Davies C, Vilardaga JCP, Rose RD, Craske MG. Randomized clinical trial of cognitive behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for mixed anxiety disorders. J Consult Clin Psychol. 2012;80(5):750–765. doi:10.1037/a0028310
87. Wolitzky-Taylor KB, Arch JJ, Rosenfield D, Craske MG. Moderators and non-specific predictors of treatment outcome for anxiety disorders: a comparison of cognitive behavioral therapy to acceptance and commitment therapy. J Consult Clin Psychol. 2012;80(5):786–799. doi:10.1037/a0029418
88. Henrich J, Heine SJ, Norenzayan A. The weirdest people in the world? Behav Brain Sci. 2010;33(2–3):61–83. doi:10.1017/S0140525X0999152X
89. Masuda A, Anderson PL, Sheehan ST. Mindfulness and mental health among African American college students. Complement Health Pract Rev. 2009;14(2):115–127. doi:10.1177/1533210110363893
90. Dalrymple KL, Herbert JD. Acceptance and commitment therapy for generalized social anxiety disorder: a pilot study. Behav Modif. 2007;31(5):543–568. doi:10.1177/0145445507302037
91. Roemer L, Orsillo SM, Salters-Pedneault K. Efficacy of an acceptance-based behavior therapy for generalized anxiety disorder: evaluation in a randomized controlled trial. J Consult Clin Psychol. 2008;76(6):1083–1089. doi:10.1037/a0012720
92. Twohig MP, Hayes SC, Plumb JC, et al. A randomized clinical trial of acceptance and commitment therapy versus progressive relaxation training for obsessive-compulsive disorder. J Consult Clin Psychol. 2010;78(5):705–716. doi:10.1037/a0020508
93. Forman EM, Herbert JD, Moitra E, Yeomans PD, Geller PA. A randomized controlled effectiveness trial of acceptance and commitment therapy and cognitive therapy for anxiety and depression. Behav Modif. 2007;31(6):772–799. doi:10.1177/0145445507302202
94. Lewinsohn PM, Munoz RF, Youngren MA, Zeiss AM. Control Your Depression. Englewood Cliffs: Prentice-Hall; 1980.
95. Zettle RD, Rains JC. Group cognitive and contextual therapies in treatment of depression. J Clin Psychol. 1989;45(3):436–445. doi:10.1002/1097-4679(198905)45:3<436::AID-JCLP2270450314>3.0.CO;2-L
96. McCracken LM, Vowles KE. Acceptance and commitment therapy and mindfulness for chronic pain: model, process, and progress. Am Psychol. 2014;69(2):178–187. doi:10.1037/a0035623
97. McCracken LM. Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain. Pain. 1998;74(1):21–27. doi:10.1016/S0304-3959(97)00146-2
98. Marlatt GA, Donovan DM. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors.
99. Luoma JB, Kohlenberg BS, Hayes SC, Bunting K, Rye AK. Reducing self-stigma in substance abuse through acceptance and commitment therapy: model, manual development, and pilot outcomes. Addict Res Theory. 2008;16(2):149–165. doi:10.1080/16066350701850295
100. Ii T, Sato H, Watanabe N, et al. Psychological flexibility-based interventions versus first-line psychosocial interventions for substance use disorders: systematic review and meta-analyses of randomized controlled trials. J Context Behav Sci. 2019;13:109–120. doi:10.1016/j.jcbs.2019.07.003
101. Juarascio AS, Manasse SM, Espel HM, Kerrigan SG, Forman EM. Could training executive function improve treatment outcomes for eating disorders? Appetite. 2015;90:187–193. doi:10.1016/j.appet.2015.03.013
102. Pearson AN, Follette VM, Hayes SC. A pilot study of acceptance and commitment therapy as a workshop intervention for body dissatisfaction and disordered eating attitudes. Cogn Behav Pract. 2012;19(1):181–197. doi:10.1016/j.cbpra.2011.03.001
103. Hill ML, Masuda A, Latzman RD. Body image flexibility as a protective factor against disordered eating behavior for women with lower body mass index. Eat Behav. 2013;14(3):336–341. doi:10.1016/j.eatbeh.2013.06.003
104. Onnink CM, Konstantinidou Y, Moskovich AA, Karekla MK, Merwin RM. Acceptance and commitment therapy (ACT) for eating disorders: a systematic review of intervention studies and call to action. J Context Behav Sci. 2022;26:11–28. doi:10.1016/j.jcbs.2022.08.005
105. Mansell W, Harvey A, Watkins E, Shafran R. Conceptual foundations of the transdiagnostic approach to CBT. J Cogn Psychother. 2009;23(1):6–19. doi:10.1891/0889-8391.23.1.6
106. Barlow DH. Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Workbook. New York: Oxford University Press; 2011.
107. Luoma JB, Platt MG. Shame, self-criticism, self-stigma, and compassion in acceptance and commitment therapy. Curr Opin Psychol. 2015;2:97–101. doi:10.1016/j.copsyc.2014.12.016
108. Stoddard JA, Afari N. The Big Book of ACT Metaphors: A Practitioner’s Guide to Experiential Exercises and Metaphors in Acceptance and Commitment Therapy. Oakland: New Harbinger; 2014.
109. Varra AA, Hayes SC, Roget N, Fisher G. A randomized control trial examining the effect of acceptance and commitment training on clinician willingness to use evidence-based pharmacotherapy. J Consult Clin Psychol. 2008;76(3):449–458. doi:10.1037/0022-006X.76.3.449
110. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. 2000;41(1):49–100. doi:10.1006/cogp.1999.0734
111. McCrae RR, Costa PT. A contemplated revision of the NEO five-factor inventory. Pers Individ Dif. 2004;36(3):587–596. doi:10.1016/S0191-8869(03)00118-1
112. Dajani DR, Uddin LQ. Demystifying cognitive flexibility: implications for clinical and developmental neuroscience. Trends Neurosci. 2015;38(9):571–578. doi:10.1016/j.tins.2015.07.003
113. Ferguson CJ, Brannick MT. Publication bias in psychological science: prevalence, methods for identifying and controlling, and implications for the use of meta-analyses. Psychol Meth. 2012;17(1):120–128. doi:10.1037/a0024445
114. Ost LG. The efficacy of acceptance and commitment therapy: an updated systematic review and meta-analysis. Behav Res Ther. 2014;61:105–121. doi:10.1016/j.brat.2014.07.018
115. Jacobson NS, Truax P. Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol. 1991;59(1):12–19. doi:10.1037/0022-006X.59.1.12
116. Linehan MM, Armstrong HE, Suarez A, Allmon D, Heard HL. Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48(12):1060–1064. doi:10.1001/archpsyc.1991.01810360024003
117. Villatte JL, Vilardaga R, Villatte M, Vilardaga JCP, Atkins DC, Hayes SC. Acceptance and commitment therapy modules: differential impact of values clarification and committed action during the treatment of major depression. Behav Res Ther. 2016;77:139–147. doi:10.1016/j.brat.2015.12.001
118. McHugh RK, Barlow DH. The dissemination and implementation of evidence-based psychological treatments: a review of current efforts. Am Psychol. 2010;65(2):73–84. doi:10.1037/a0018121
119. Coyne L, Kelly GW. The role of cognitive fusion in impaired parenting. Int J Psychol Psychol Ther. 2004;4(3):469–486.
120. Petersen JM, Zurita Ona P, Twohig MP. A review of acceptance and commitment therapy for adolescents: developmental and contextual considerations. Cogn Behav Pract. 2024;31(1):72–89. doi:10.1016/j.cbpra.2022.08.002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.