Back to Journals » Drug Design, Development and Therapy » Volume 20
Psychiatric, Cardiovascular and Skeletal Risks of Codeine versus Oxycodone in Hip Osteoarthritis: A Population-Based Cohort Study
Authors Lee J ![]() , Kim Y, Choo E, Shin S
, Kim Y, Choo E, Shin S ![]() , Choi YJ
, Choi YJ ![]()
Received 4 October 2025
Accepted for publication 27 January 2026
Published 10 February 2026 Volume 2026:20 572083
DOI https://doi.org/10.2147/DDDT.S572083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Anastasios Lymperopoulos
Jeongmin Lee,1– 3,* Yujin Kim,1– 3,* Eunjung Choo,4 Sooyoung Shin,4,5 Yeo Jin Choi1– 3
1Department of Regulatory Science, Graduate School, Kyung Hee University, Seoul, Korea; 2Institute of Regulatory Innovation through Science (IRIS), Kyung Hee University, Seoul, Korea; 3Department of Pharmacy, College of Pharmacy and Institute of Integrated Pharmaceutical Sciences, Kyung Hee University, Seoul, Korea; 4Department of Pharmacy, College of Pharmacy, Ajou University, Suwon, Korea; 5Research Institute of Pharmaceutical Science and Technology (RIPST), Ajou University, Suwon, Korea
*These authors contributed equally to this work
Correspondence: Yeo Jin Choi, Department of Pharmacy, College of Pharmacy and Institute of Integrated Pharmaceutical Sciences, Kyung Hee University, 26 Kyungheedae-ro, Dongdamun-gu, Seoul, 02447, Korea, Tel +82 2 961 0532, Fax +82 2 961 9580, Email [email protected] Sooyoung Shin, Department of Pharmacy, College of Pharmacy, Ajou University, Suwon, 16488, Korea, Tel +82 31 219 3456, Fax +82 31 219 3435, Email [email protected]
Background/Objectives: Hip osteoarthritis (OA) induces chronic pain and disability in aging populations. Opioids are increasingly prescribed for refractory hip OA pain; however, comparative safety data are limited. This study aimed to compare the psychiatric, cardiovascular and skeletal outcomes between codeine and oxycodone in patients with hip OA.
Methods: A population-based retrospective cohort using Korean Health Insurance Review and Assessment Service (HIRA) claims data was performed in hip OA (M16) patients who initiated codeine or oxycodone. Propensity score matching (PSM) was applied with sensitivity analyses performed using inverse probability of treatment weighting (IPTW). Outcomes included composite psychiatric outcomes (depression, anxiety, bipolar disorder, sleep disorders, and schizophrenia), major adverse cardiovascular outcomes (MACE; myocardial infarction, stroke, cardiovascular death/arrest, heart failure hospitalization), and fractures. Hazard ratios (HR) with 95% confidence intervals (CIs) were estimated using Cox proportional hazard models.
Results: A total of 16,162 patients were included in the cohort after 1:1 PSM. Codeine was associated with a higher risk of psychiatric disorders (HR 1.11, 95% CI 1.04– 1.19), particularly anxiety (HR 1.14, 95% CI 1.03– 1.26) and sleep disorders (HR 1.15, 95% CI 1.02– 1.30). Risks of MACE (HR 1.02, 95% CI 0.92– 1.14) and death (HR 1.03, 95% CI 0.92– 1.14) were comparable between groups. Codeine was associated with a higher risk of non-femoral fractures (HR 1.10, 95% CI 1.04– 1.16). Subgroup analyses revealed differentiated risks across age, sex, comorbidities, and concomitant medications.
Conclusion: Codeine use in patients with hip osteoarthritis was associated with a higher risk of psychiatric disorders and distinct fracture patterns. The observed risks varied according to patient characteristics, comorbidities, and concomitant medications, emphasizing the need for individualized opioid prescribing strategies that incorporate psychiatric monitoring, fracture risk assessment, and patient-specific factors. Further controlled studies integrating clinical, lifestyle, and genetic data are warranted to confirm these findings and refine personalized opioid therapy in hip osteoarthritis.
Keywords: oxycodone, codeine, MACE, anxiety, sleep disorder, fracture
Introduction
Hip osteoarthritis (OA) is a highly prevalent musculoskeletal disorder and a leading cause of chronic pain, disability, and reduced quality of life in aging populations worldwide, with an estimated global prevalence of 8.55%.1,2 As symptoms progress, many patients usually require pharmacological interventions beyond nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen, and current treatment guidelines recommend reserved opioid use for short-term management of severe, refractory pain.3 In particular, guidelines generally recommend the use of weak opioids, such as codeine or tramadol, before considering strong opioids such as oxycodone.3 However, recent epidemiological studies have reported increasing oxycodone use among patients with OA, raising concerns regarding potential differences in safety profiles between weak and strong opioids.4
Opioids not only carry elevated risk of dependence, misuse, or abuse, but also contribute to a wide range of systemic adverse events affecting the gastrointestinal, neurological, cardiovascular, and psychiatric systems.3,5 Previous studies have reported an association between opioid use and an increased risk of mood and anxiety disorders, particularly with long-term exposure, and similar findings have also been observed among individuals using opioid for non-medical purposes.6–8 Moreover, the duration of opioid use appears to be a stronger predictor of opioid-induced depression than the prescribed opioid dose.9 In addition, the risk of opioid misuse is substantially elevated in patients with preexisting psychiatric disorders such as attention-deficit disorders, bipolar disorder, depression and schizophrenia, as implied by the Opioid Risk Tool (ORT), a validated screening instrument developed to predict opioid misuse in patients with chronic nonmalignant pain.10 These findings suggest a potential mutual relationship between psychiatric disorders and opioid use, whereby psychiatric vulnerability predisposes patients to opioid misuse, while prolonged opioid exposure may exacerbate or induce psychiatric morbidity.
Beyond psychiatric outcomes, opioids have also been associated with adverse cardiovascular events, with studies reporting up to a 74% increased risk of major adverse cardiovascular events (MACE) associated with chronic opioid use.8,11,12 Furthermore, opioid use has been consistently associated with an increased risk of falls and fractures, especially among the elderly.13,14 Opioid has been associated with reduced bone mineral density (BMD), while additional factors such as opioid-related sedation, impaired balance, dizziness, and orthostatic hypotension, may further contribute to increased fall risk and fracture susceptibility.15,16 Emerging evidence has further expanded the scope of opioid-related safety concerns to included neurodegenerative impacts, such as exacerbation of cognitive decline and neuroinflammation, particularly in vulnerable, older populations.17 Despite known risks, direct comparative evidence of the safety profiles of commonly prescribed opioids remains limited. Although codeine is generally recommended before the use of oxycodone, recent epidemiological evidence indicate increasing oxycodone use among patients with OA.4 However, comparative evidence on safety outcomes, particularly psychiatric disorders, MACE, and fractures, between codeine and oxycodone, is limited. Therefore, this study aimed to compare the risks of psychiatric disorders, MACE, and fractures between codeine and oxycodone in patients with hip OA and to stratify these risks by patient characteristics to inform individualized opioid prescribing and enhance patient safety.
Methods
Data Source and Study Population
This was a nationwide, population-based retrospective cohort study using the Health Insurance Review and Assessment Service (HIRA) National Claims Data (M20230724004), conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.18 The HIRA database contains administrative data from the National Health Insurance (NHI), including patient demographics, diagnoses, prescription records, healthcare services, type of healthcare institution, outpatient and inpatient encounters, and details on hospitalizations.19 Diagnoses were coded using the Korean Standard Classification of Diseases 8th Revision, which was adapted from the International Classification of Diseases, 10th Revision (ICD-10).
Patients diagnosed with hip OA (ICD-10 code M16) between January 1, 2014 and December 31, 2017 who received at least one prescription of either oxycodone or codeine were included in the cohort (Figure 1). The index date was defined as the date of the first prescription of codeine or oxycodone following the initial diagnosis of hip OA. Opioid exposure was treated as a time-fixed variable defined at the index date to ensure clinical interpretability and minimize exposure misclassification, particularly given the intermittent and short-term prescribing patterns observed in our data. After cohort entry, patients were followed longitudinally from the index date until the occurrence of the outcome of interest, or December 31, 2022, whichever came first. Exclusion criteria were as follows: (1) age <20 or ≥85 years, (2) history of codeine or oxycodone use within 1 year prior to index date, (3) diagnoses of psychiatric disorders (F13, F20-F42, F51) within 1 year prior to the index date, defined as the date of the first codeine or oxycodone prescription following an M16 diagnosis, (4) diagnosis of cancer (C00-D48), (5) history of opioid-related disorders (F11), (6) medication history of buprenorphine or naloxone injection,(7) history of orthopedic joint implants (Z96.6), burns injuries, traffic crashes, and (8) use of low-dose (<50mg) dihydrocodeine, typically prescribed as an antitussive. The study protocol was approved by Institutional Review Board (IRB) of Kyung Hee University (KHSIRB-23-272-1(EA)), and requirement for informed consent was waived owing to the retrospective study design using anonymized data.
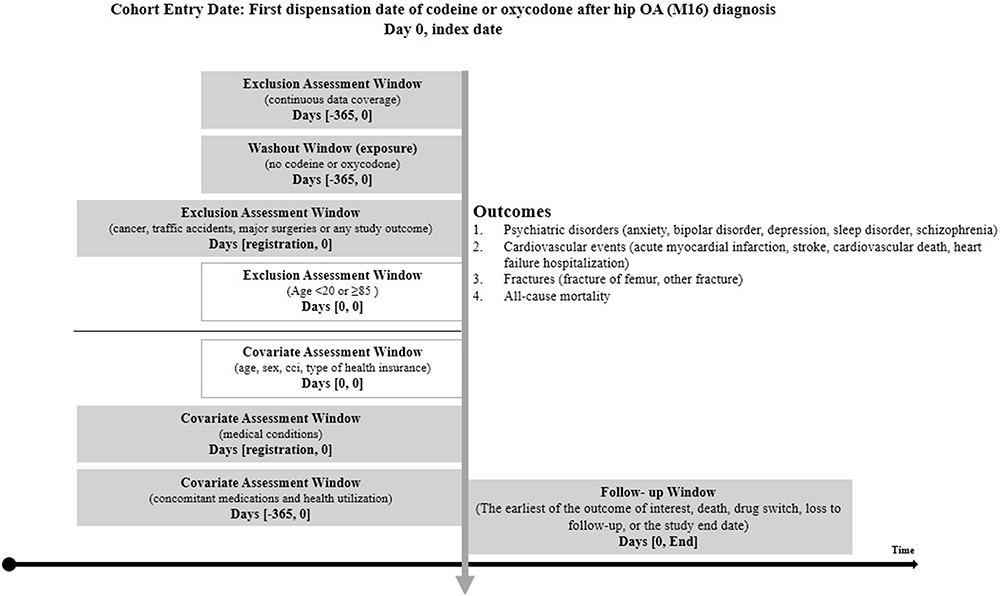 |
Figure 1 Study design. |
Study Outcomes and Covariates
The primary study outcome was the incidence of composite psychiatric disorders, defined as depression (F32-F33), anxiety disorder (F41), bipolar disorder (F30-F31), sleep disorder (F51) or schizophrenia (F20-F25). Secondary study outcomes were MACE, fractures, and mortality after initiation of either oxycodone or codeine. MACE was defined as myocardial infarction (I21-I22), stroke (I60-I64, I69), cardiovascular death/arrest (I40, I46), or hospitalization for heart failure (I11, I13, I13.2, I50). Fractures were identified using prespecified diagnostic codes: S22, S32, S42, S52, S62, S72, S82, S92, T02, T08, T10-13, T142, M80. Patients were followed from the index date until the earliest of the following events: outcome occurrence, medication switch, or December 31, 2022, with a maximum follow-up of nine years. Baseline characteristics, including demographics, (age, sex), Charlson Comorbidity Index (CCI), comorbidities, and concomitant medications, were assessed during the 12 months prior to the index date.
Statistical Analysis
To compare the risks of psychiatric disorders, MACE, fracture, and death between codeine and oxycodone users, a 1:1 nearest neighbor propensity score-matching (PSM) without replacement was performed using a caliper width of 0.1. Covariate balance was assessed using standardized mean differences (SMD), with values <0.1 indicating adequate balance. All baseline covariates were complete, with no missing values. Patients with medication use exceeding the 99th percentile of the overall distribution were excluded to minimize the influences of outliers. Cumulative incidence rates were estimated using Kaplan-Meier curves and compared with the Log rank test. Multivariable Cox proportional hazard models were used to estimate hazard ratios (HR) with 95% confidence intervals (CIs), adjusted for age, sex, CCI, baseline comorbidities (diabetes mellitus (DM), cardiovascular disorders (CVD), chronic kidney disease (CKD), neurological disease, thyroid disease, liver disease, gastrointestinal disease, osteoporosis, and asthma), and concomitant medications (benzodiazepines, antidepressants, antipsychotics, anticonvulsants, non-steroidal anti-inflammatory drugs [NSAIDs], and tramadol). The proportional hazards assumption was assessed using the Schoenfeld residual test. Subgroup analyses were performed within the PSM cohort according to sex, age group (20–39 years, 40–64 years and ≥65 years), CCI index, type of health insurance, comorbidities, and concomitant medications. To assess the robustness of the primary findings, we conducted sensitivity analyses using inverse probability of treatment weighting (IPTW). In addition, to evaluate potential duration-dependent effects, we performed a prespecified sensitivity analysis stratifying patients into short-term (<30 days) and relatively sustained (≥30 days) opioid use groups. All statistical analyses were performed using SAS version 7.14 (SAS Institute, Inc., Cary, NC, USA) and R version 3.5.1 (R Core Team). A two-sided P-value <0.05 was considered statistically significant.
Results
Characteristics of Patients Before and After Matching
Among 487,994 patients diagnosed with hip OA between 2014 and 2017, 29,919 patients who received at least one prescription for either oxycodone or codeine were included in the cohort (Figure 2). A total of 16,162 patients were retained after 1:1 PSM. Baseline characteristics before and after PSM are summarized in Table 1. The age distribution was comparable between two groups, with more than 60% of patients aged ≥65 years. Comorbidities and concomitant medications use were well balanced between the two groups; however, residual imbalance remained for tramadol use (SMD = 0.381), asthma (SMD=0.130), and osteoporosis (SMD=0.101). In the matched cohort, the mean (± standard deviation) duration of opioid use was 59.57 ± 206.39 days in the oxycodone and 40.63±101.18 days in the codeine group, with median duration of 16 days (interquartile range [IQR] 37) and 14 days (IQR 28), respectively.
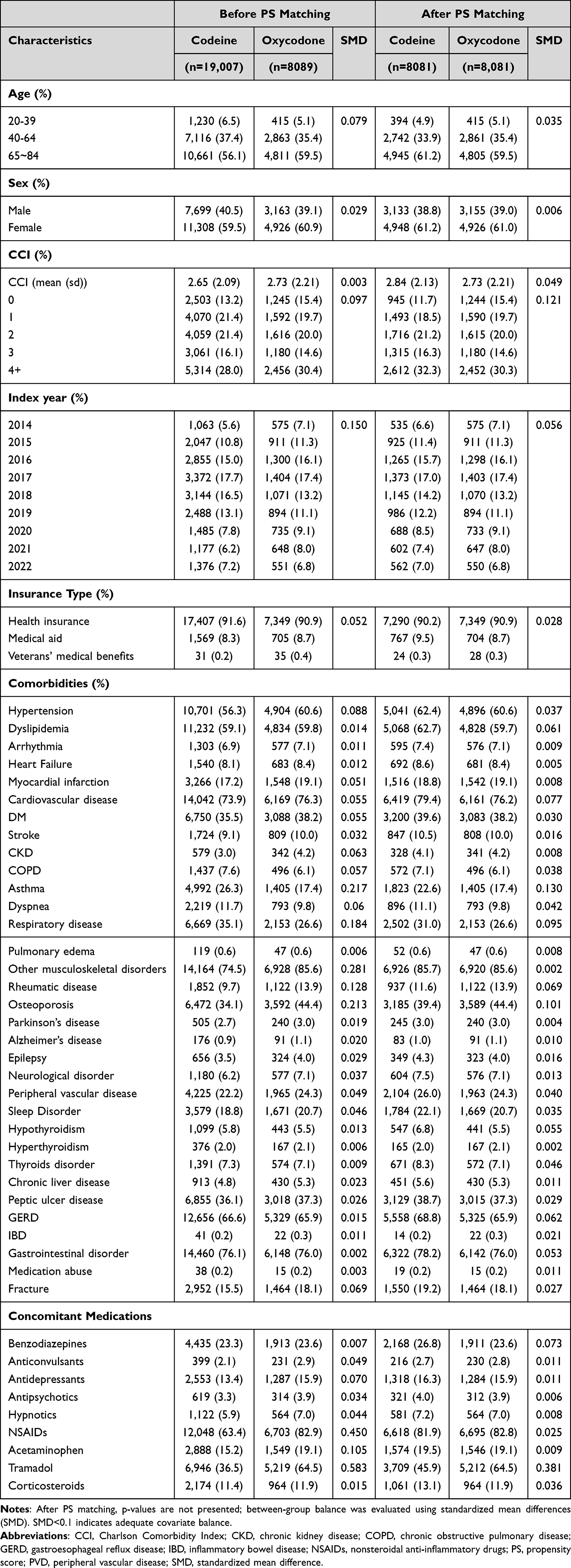 |
Table 1 Baseline Characteristics of the PS-Matched Cohort |
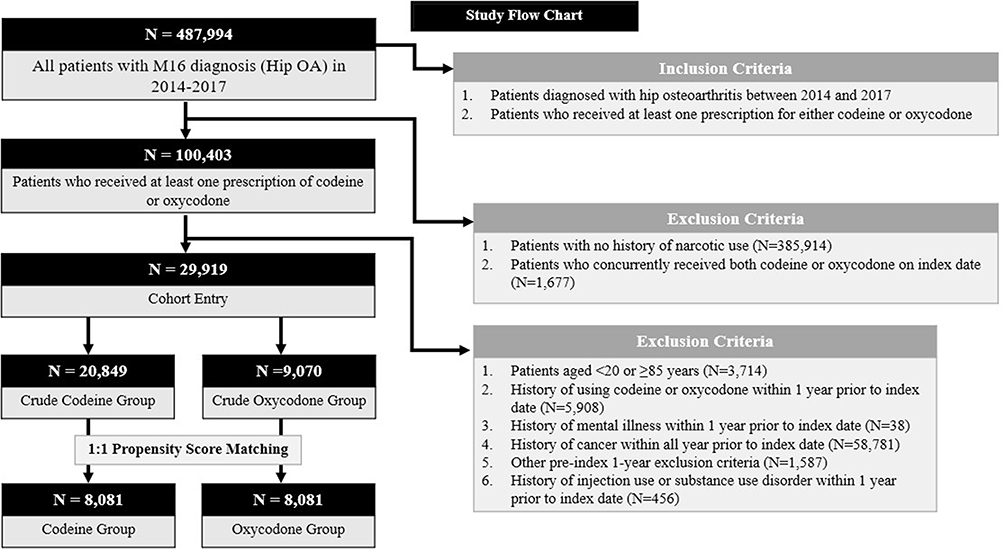 |
Figure 2 Flowchart of Patients from the HIRA Database (2014–2022) with exclusion and inclusion criteria. |
Risk of Psychiatric Disease
Kaplan–Meier survival analyses further illustrated the cumulative incidence of study outcomes between the two groups (Figure 3). Patients treated with codeine showed a significantly higher cumulative incidence of composite psychiatric outcomes (log-rank p = 0.027) and sleep disorders (log-rank p = 0.031). With respect to skeletal outcomes, the cumulative incidence of overall fracture (log-rank p = 0.032) and non-femoral fractures (log-rank p = 0.00042) was higher among codeine users, whereas a lower cumulative incidence of femoral fractures was observed in the codeine group (log-rank p < 0.0001). No significant difference was observed in the cumulative incidence of MACE or all-cause mortality between the two groups.
 |
Figure 3 Kaplan-Meier Curves for study outcomes. (A) Composite psychiatric outcomes, (B) Sleep disorders, (C) MACE, (D) Fracture, (E) Femoral fracture, (F) Non-femoral fracture and (G) All-cause mortality. |
The incidence rate (IR) of composite psychiatric disorders was 45.9 per 1,000 person-years (PY) for oxycodone and 51.0 per 1,000 PY for codeine, with an adjusted HR (aHR) of 1.11 (95% CI 1.04–1.19) (Table 2). The IR of anxiety was 18.7 per 1,000 PY for oxycodone and 20.3 per 1,000 PY for codeine (aHR 1.14, 95% CI 1.03–1.26). The IR of sleep disorder was also significantly higher among patients treated with codeine (aHR 1.15, 95% CI 1.02–1.30). With respect to fracture outcomes, codeine use was associated with a higher risk of non-femoral fractures (aHR 1.10, 95% CI 1.04–1.16), whereas a lower risk of femoral fracture was observed (aHR 0.65, 95% CI 0.58–0.72). However, the overall fracture risk did not differ significantly between the two groups in the fully adjusted model. No statistically significant differences were observed between oxycodone and codeine users in the risks of death and MACE, including stroke, cardiovascular death/arrest, and hospitalization for heart failure.
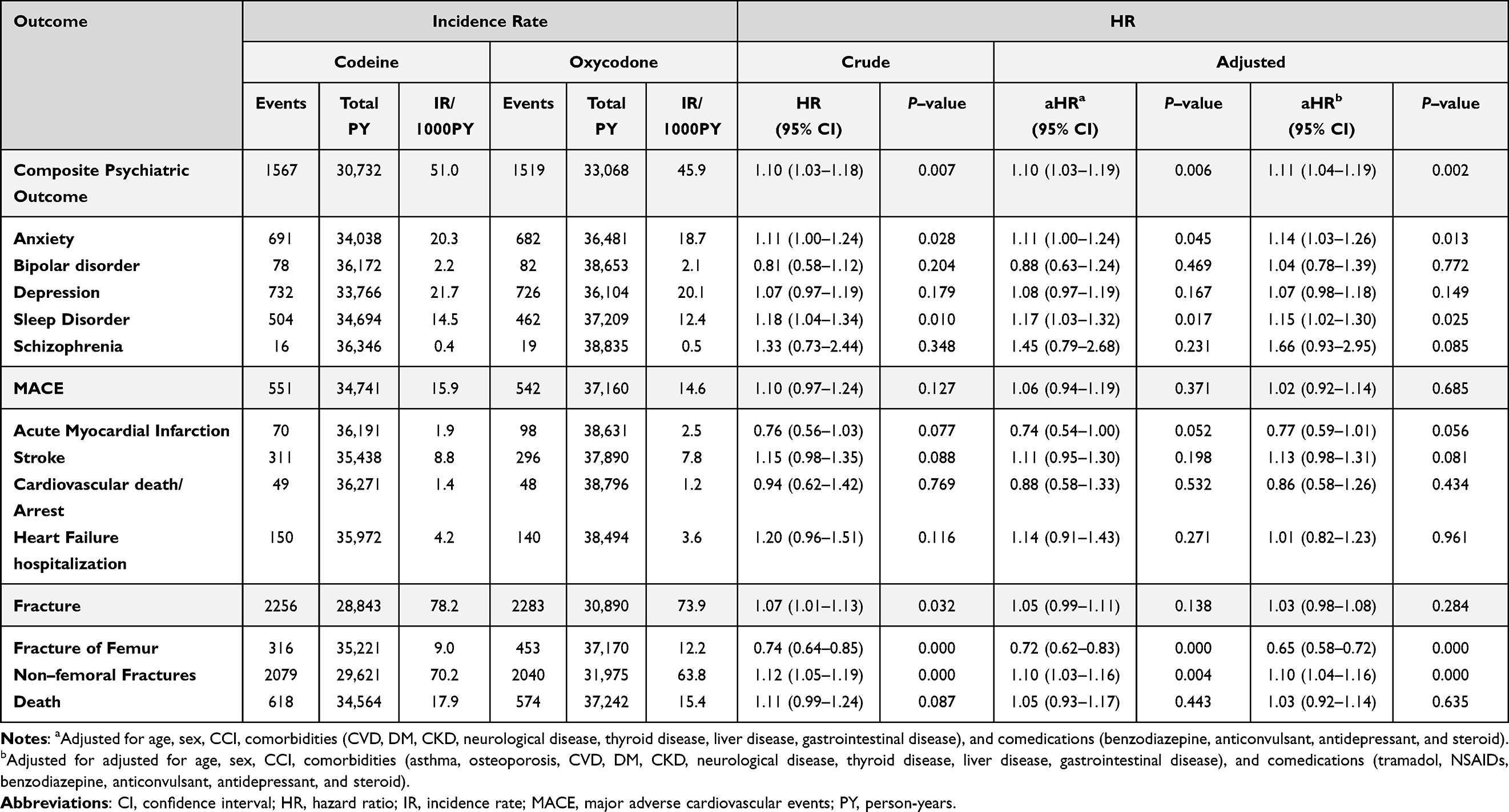 |
Table 2 Risk of Outcomes and All-Cause Mortality in Codeine vs Oxycodone Users |
Subgroup Analysis
Subgroup-based stratified analyses of composite psychiatric outcomes by patient characteristics, including age, sex, CCI, insurance type, comorbidities and concomitant medications, are summarized in Table 3. Among patients aged 40–64 years, codeine use was associated with a significantly higher risk of composite psychiatric outcomes (HR 1.22, 95% CI 1.07–1.38) and anxiety disorders (HR 1.25, 95% CI 1.04–1.51). Factors associated with a significantly higher risk of sleep disorders with codeine included older age ≥ 65 years (HR 1.17, 95% CI 1.00–1.37), female sex (HR 1.18, 95% CI 1.00–1.38), CCI scores ≥ 3 (HR 1.23, 95% CI 1.03–1.45), DM (1.32, 95% CI 1.09–1.61), and concomitant antidepressant use (HR 1.28, 95% CI 1.01–1.62). The risks of composite psychiatric disorders, including anxiety disorders and sleep disorders, were more pronounced with codeine in patients without CKD, neurological disorders, or osteoporosis, as well as in those not receiving concomitant benzodiazepines, antipsychotics, hypnotics, corticosteroids, and antiepileptics. The risk of composite psychiatric disorder was greater with codeine regardless of NSAIDs use, but the risk of anxiety and depression was higher in those not using NSAIDs (HR 1.38, 95% CI 1.05–1.81 for anxiety and HR 1.34, 95% CI 1.04–1.71 for depression). The risk of anxiety was greater in the codeine group regardless of tramadol use, whereas composite psychiatric outcome was significantly elevated with codeine among patients receiving tramadol (HR 1.13, 95% CI 1.04–1.22).
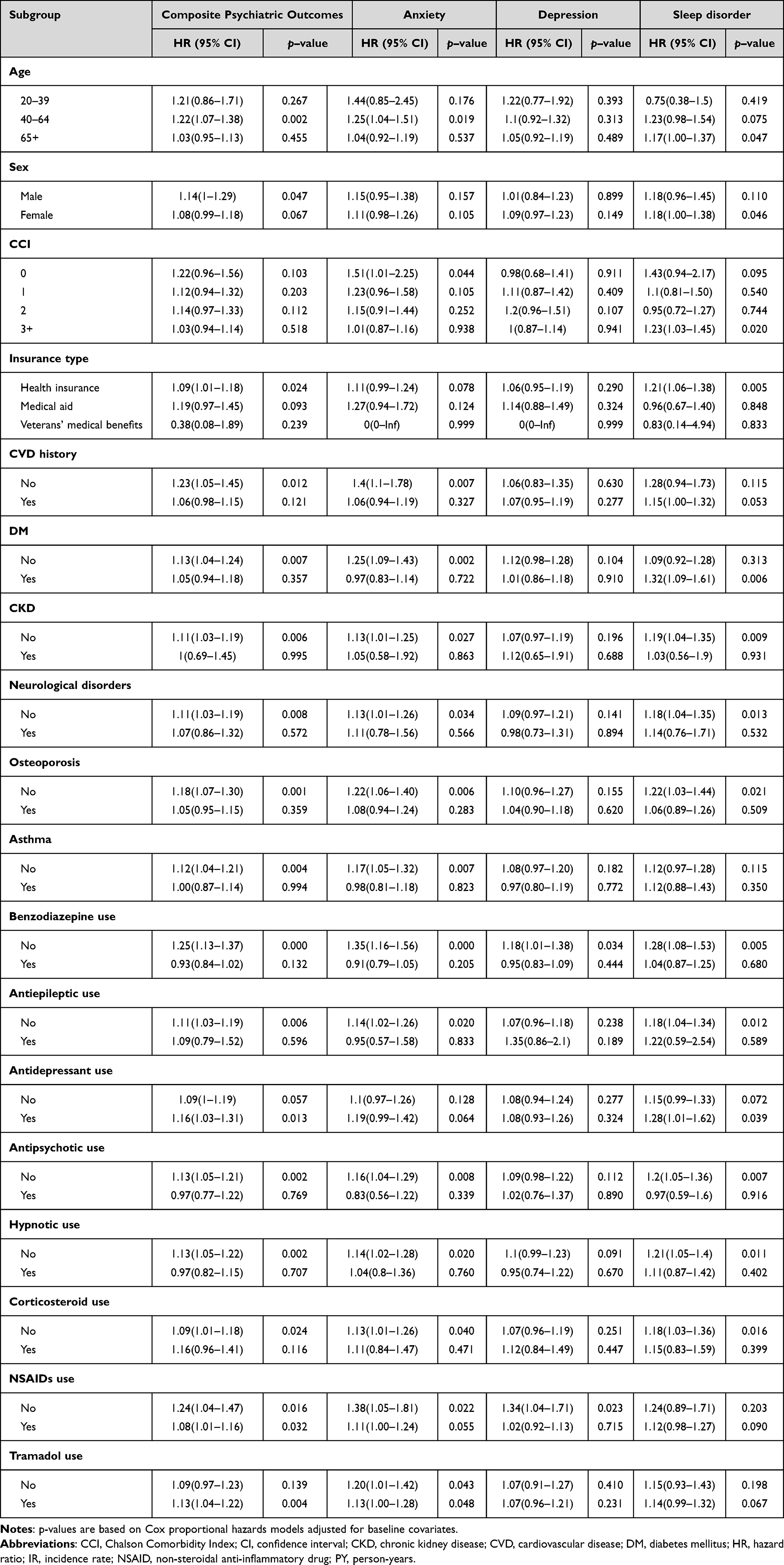 |
Table 3 Subgroup Analysis on the Risk of Psychiatric Outcomes |
Concomitant use of benzodiazepines and antipsychotics was associated with higher risk of stroke and MACE among patients received codeine (Table 4). In addition, codeine use was associated with an increased risk of MACE in patients with underlying CKD or neurological disorders.
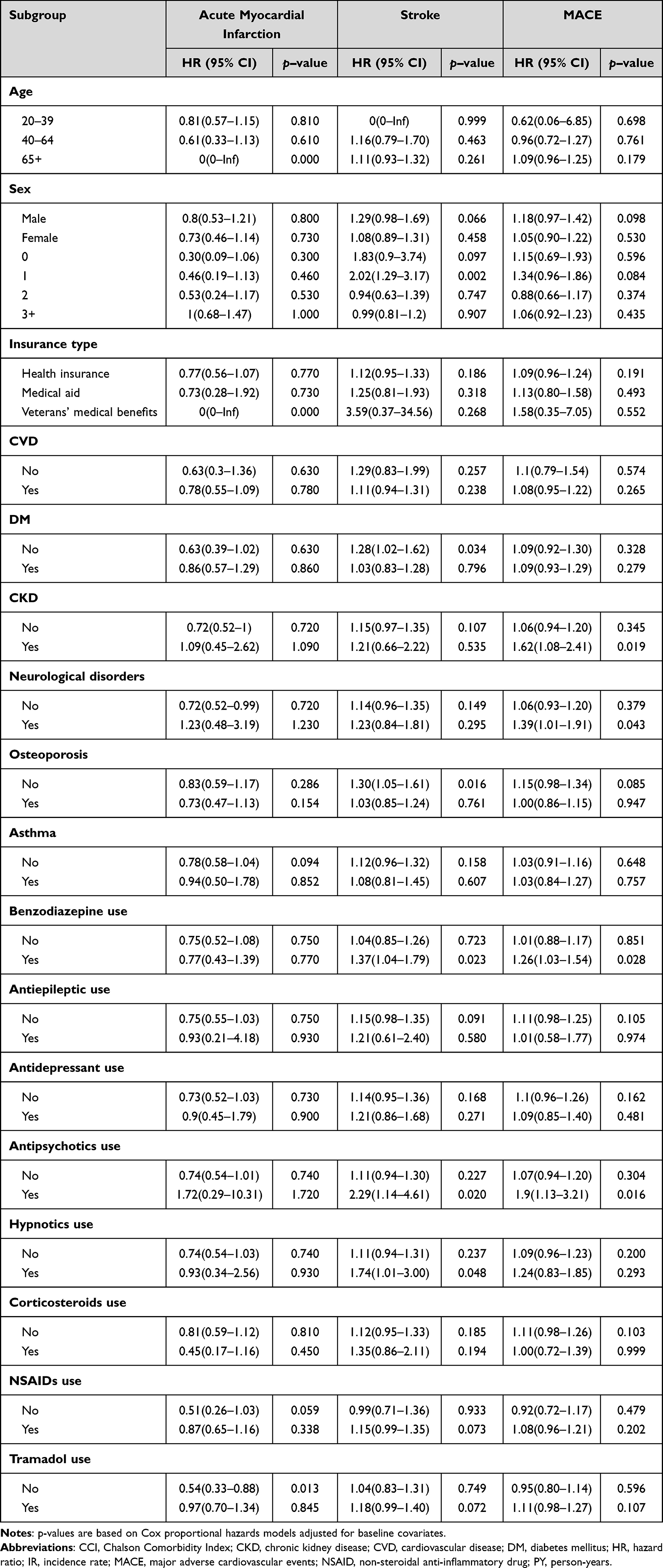 |
Table 4 Subgroup Analysis on the Risk of MACE |
The risk of overall fracture was significantly elevated with codeine in patients without DM (HR 1.09, 95% CI 1.01–1.17), CKD (HR 1.08, 95% CI 1.02–1.14), asthma (HR 1.06, 95% CI 1.00–1.12), or neurological disorder (HR 1.08 95% CI 1.02–1.15), as well as in those without concomitant use of antiepileptics (HR 1.07, 95% CI 1.01–1.13), hypnotics (HR 1.09, 95% CI 1.03–1.16), or corticosteroids (HR 1.07, 95% CI 1.01–1.14) (Table 5). Notably, heterogeneous patterns in the risk of overall fracture were observed across subgroups stratified by NSAIDs and tramadol use, with elevated risks in the codeine group among patients receiving NSAIDS or tramadol, and lower risks among those not receiving these medications. On the other hand, the risk of femoral fracture was consistently lower with codeine, irrespective of age, sex, comorbidities (including DM, osteoporosis, asthma, neurological disorders, osteoporosis and asthma), or concomitant medication use (benzodiazepines, antiepileptics, antidepressants, hypnotics, NSAIDs and tramadol). However, the risks of non-femoral fracture and death were substantially elevated in the codeine group receiving concomitant NSAIDs (HR 1.19, 95% CI 1.12–1.26 for non-femoral fracture and HR 1.19, 95% CI 1.06–1.33 for all-cause mortality) or tramadol (HR 1.25, 95% CI 1.17–1.33 for non-femoral fracture, and HR 1.27, 95% CI 1.12–1.43 for all-cause mortality).
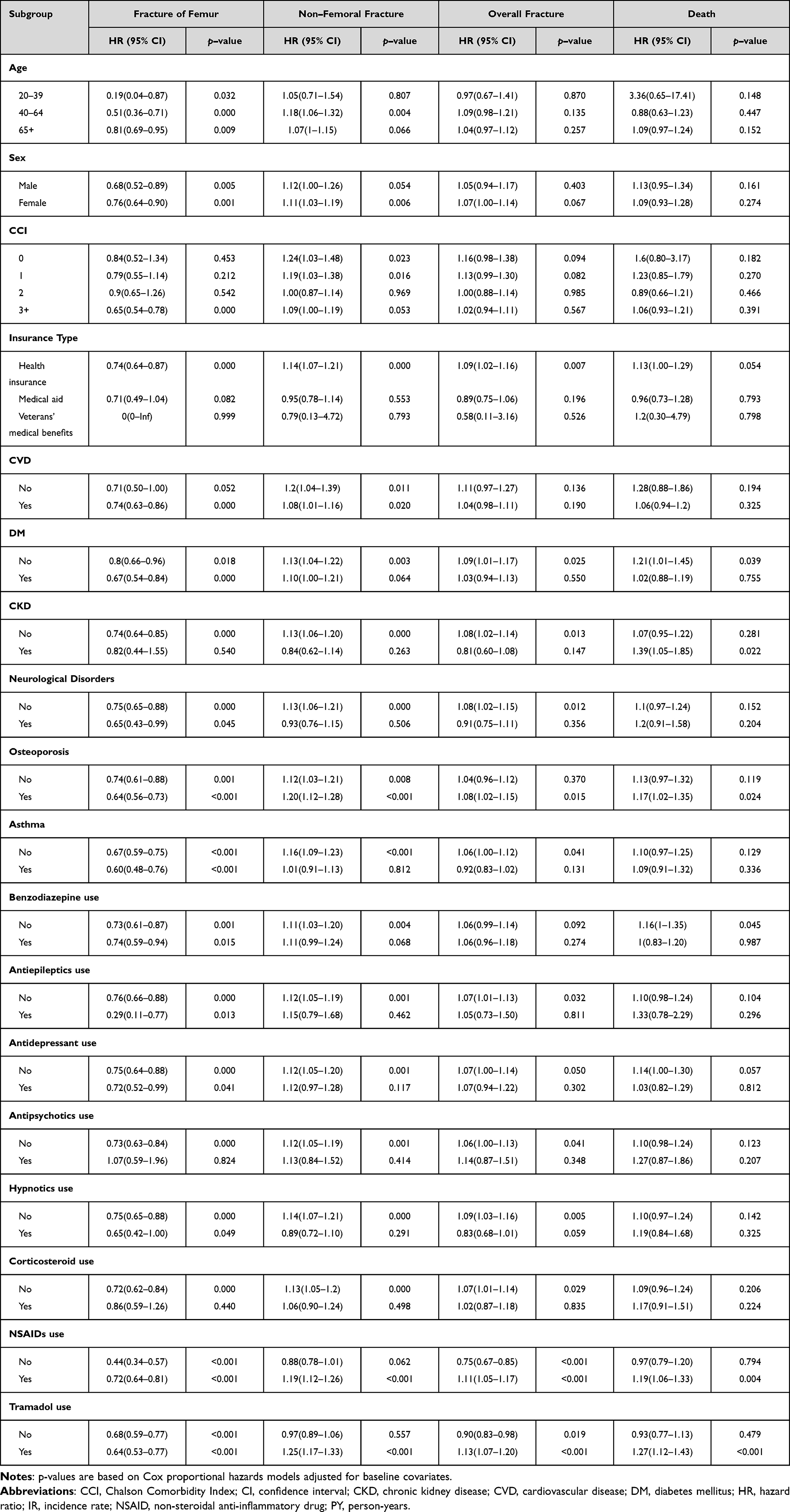 |
Table 5 Subgroup Analysis on the Risks of Fracture and Death |
Sensitivity Analysis
Sensitivity analyses using IPTW generally supported the robustness of the primary findings (Table 6). Codeine use remained associated with higher risk of composite psychiatric outcomes (HR 1.06, 95% CI 1.00–1.12), sleep disorders (HR 1.12, 95% CI 1.01–1.24), and non-femoral fractures (HR 1.05, 95% CI 1.00–1.10). In contrast, codeine use was associated with a lower risk of femoral fracture (HR 0.61, 95% CI 0.55–0.66) and AMI (HR 0.78, 95% CI 0.63–0.97). Drug-duration interaction analyses showed no significant effect modification for most psychiatric and cardiovascular outcomes (Table 7). A significant interaction was observed for acute myocardial infarction (interaction HR 1.93, 95% CI 1.02–3.67), indicating that the comparative association between codeine and oxycodone varied by duration of use. Significant interactions were also identified for overall fracture (interaction HR 0.85, 95% CI 0.76–0.94) and non-femoral fracture (interaction HR 0.89, 95% CI 0.80–0.99), whereas no interaction was observed for femoral fracture or all-cause mortality.
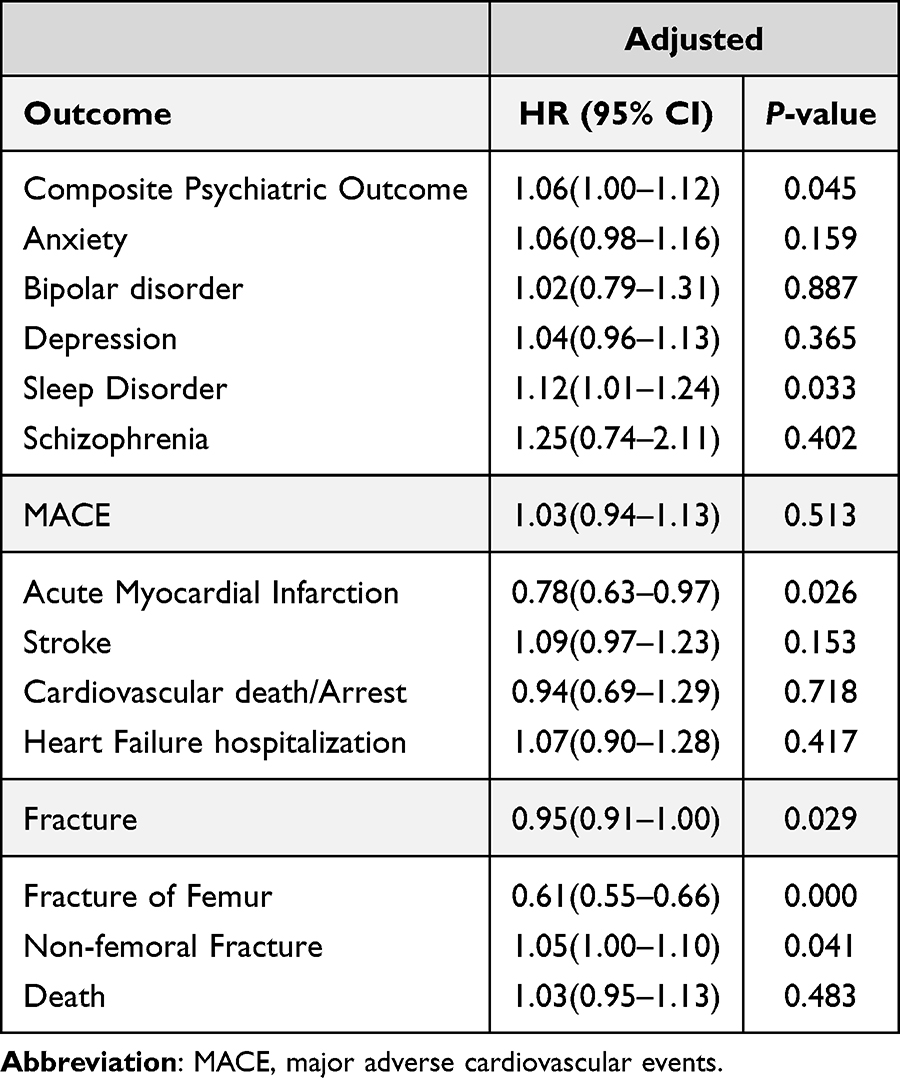 |
Table 6 IPTW-Weighted Analysis of Outcomes in Codeine vs Oxycodone Users |
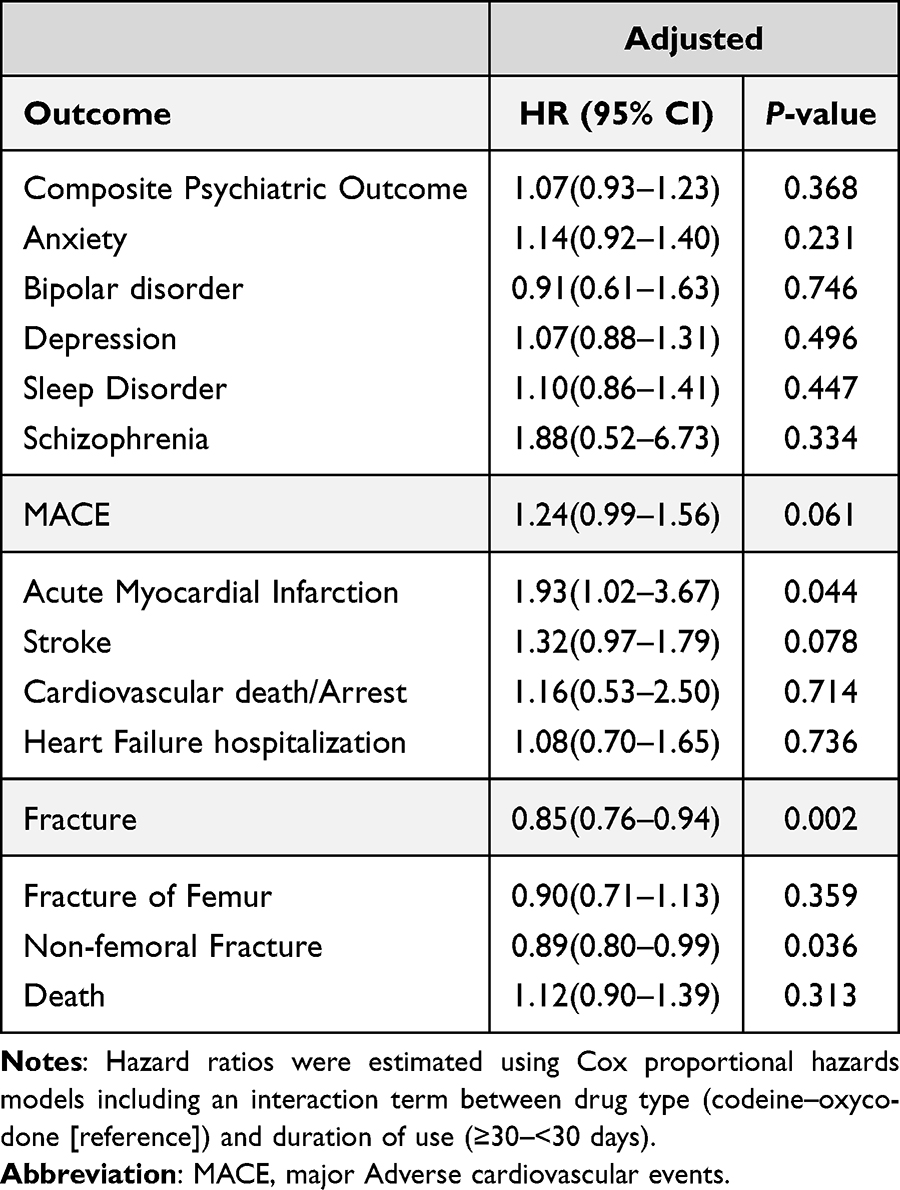 |
Table 7 Drug-Duration Interaction Analysis of Outcomes in Codeine vs Oxycodone Users |
Discussion
This nationwide cohort of patients with hip OA revealed clinically meaningful differences in the safety profiles of oxycodone and codeine. Codeine use was consistently associated with a higher risk of psychiatric disorders, particularly anxiety and sleep disorders. Overall risks of MACE and all-cause mortality were comparable between codeine and oxycodone. However, fracture outcomes demonstrated heterogeneous patterns between the two opioids. Specifically, codeine was associated with a substantially lower risk of femoral fracture, yet a higher risk of non-femoral fractures across most subgroups.
These findings have important clinical implications for opioid prescribing practice in patients with hip OA. Although codeine is generally considered a weak opioid and is often recommended before initiating strong opioids such as oxycodone, our results highlight that its safety profile is not uniformly more favorable across all outcomes. While the precise mechanisms underlying these findings remain unclear, several potential explanations can be proposed. Unlike oxycodone, codeine is a prodrug that requires CYP2D6-mediated metabolism to be converted to morphine, and genetic variability in CYP2D6 activity can result in unpredictable analgesic efficacy and heterogeneous opioid exposure in the central nervous system (CNS).20 Notably, East Asians frequently carry CYP2D6*10 allele, which is associated with reduced enzymatic activity and slower metabolism of codeine to morphine, leading to lower morphine concentrations and suboptimal analgesic responses in many patients.20,21 Such interindividual variability in analgesic response may exacerbate pain and pain-related distress and increase vulnerability to psychiatric outcomes, including anxiety and sleep disorders.22 However, considering the observational nature of this study and absence of individual-level CYP2D6 genotyping data, these pharmacogenetic and mechanistic considerations should be interpreted as biologically plausible associations rather than causal explanations. Hence, future studies incorporating genetic profiling and pharmacokinetic assessments are warranted to further elucidate the mechanism underlying the observed psychiatric risks associated with codeine use.
Additionally, codeine can induce non-IgE-mediated mast cell degranulation, leading to the release of mediators such as histamine that may produce pseudoallergic symptoms.23 Moreover, elevated histamine levels can promote wakefulness and neuroinflammation, and may consequently contribute to psychiatric disorders, including sleep disorders.24,25 Furthermore, opioid-induced modulation of multiple neurotransmitter systems, including dopaminergic and serotonergic pathways, may disrupt the regulation of mood, reward, and anxiety.26 Nonetheless, it is critical to acknowledge that the increased psychiatric risks with codeine use were more pronounced among patients without preexisting CVD, CKD, osteoporosis, or neurological disorders, as well as in those without concomitant use of CNS-active medications such as benzodiazepines, antiepileptic, antipsychotics, corticosteroids, and hypnotics. This consistently elevated risk of psychiatric disorders with codeine, particularly anxiety and sleep disorders, emphasizes the importance of cautious psychiatric screening and monitoring when initiating opioid therapy, especially in patients vulnerable to anxiety or sleep disturbances. Further studies are warranted to clarify the underlying biological mechanisms including potential gene-drug interactions that may contribute to long-term psychiatric outcomes. Furthermore, a potential link between metabolic disorders and psychiatric outcomes should be considered, as the risk of composite psychiatric disorders and anxiety disorders was higher among patients without history of cardiovascular disease, DM CKD or neurological disorders.
The risk of MACE and mortality were comparable between codeine and oxycodone users. Chronic opioid use has been associated with increased risk of myocardial infarction, stroke, arrhythmias, and sudden cardiac death, potentially mediated through mechanisms involving opioid-induced respiratory depression, hypoxemia, endothelial dysfunction and enhanced platelet activation.11,12,27 However, our study results did not demonstrate significant differences in the MACE risk between codeine and oxycodone, suggesting that the two opioids may confer broadly similar cardiovascular risk profiles in patients with hip OA under routine clinical use. With respect to AMI, codeine use was associated with a lower risk of AMI in the IPTW sensitivity analysis, whereas the primary adjusted Cox model did not show a consistent protective association. In addition, drug-duration interaction analysis revealed a significant interaction for AMI, indicating that the comparative association between codeine and oxycodone varied according to duration of use rather than reflecting a uniform main effect. Therefore, these findings suggest that the observed AMI associations are likely influenced by residual confounding, treatment duration, or underlying cardiovascular risk profiles, rather than a direct drug-specific effect, and should therefore be interpreted with caution Nonetheless, subgroup analyses revealed that codeine was associated with an elevated risk of MACE in patients with underlying CKD or neurological disorders, and when used concomitantly with CNS-active drugs such as benzodiazepines and antipsychotics. These findings highlight the importance of considering comorbidity profiles and potential drug-drug interactions when initiating opioid therapy. Moreover, cautious interpretation is required, as more than 75% of included patients had some form of preexisting cardiovascular events, including hypertension, dyslipidemia, heart failure, and myocardial infarction. Therefore, further controlled studies are warranted to investigate comparative cardiovascular safety in populations with fewer baseline comorbidities to determine the independent effect of opioid exposure from underlying cardiovascular risk.
This study revealed a divergent pattern in risk of fracture between codeine and oxycodone users. Codeine use was consistently associated with a lower risk of femoral fractures and a higher risk of non-femoral fractures across multiple analyses, including subgroup and sensitivity analyses. Opioids have been associated with reduced BMD through suppression of sex hormones and direct effects on bone remodeling.15 In addition, opioid-related sedation, impaired balance, dizziness, and orthostatic hypotension further increase the likelihood of fall-related fractures.14 Importantly, duration-stratified and drug-duration interaction analyses indicated that the comparative fracture risk between codeine and oxycodone differed according to duration of opioid exposure, rather than demonstrating a uniform effect across exposure periods. Although the precise mechanisms underlying this divergent pattern remain unknown, previous studies have reported that patients with hip OA were more likely to experience trochanteric fractures than femoral neck fractures, and that increasing OA severity has been associated with a greater prevalence of extracapsular rather than intracapsular fractures. In contrast, individuals without hip OA more frequently experience femoral neck fractures, which represent a more severe clinical form.28 Importantly, however, due to the limitations inherent to administrative claims data, the present study could not distinguish intracapsular from extracapsular fracture subtypes or capture fall mechanism. Therefore, these observations should be interpreted with caution. These findings raise the possibility that hip OA-related factors, such as disease severity, altered joint biomechanics, reduced mobility, or differential fall patterns, may partially contribute to the observed lower risk of femoral fractures among codeine users, rather than indicating a direct protective effect of the drug itself. Conversely, the elevated risk of non-femoral fractures with codeine may reflect residual vulnerability related to opioid-induced falls, altered fall dynamics, or differences in skeletal fragility at non-hip sites. Therefore, further studies incorporating more granular fracture site classifications, fall-related clinical data, and refined assessment of exposure duration are warranted to clarify the underlying pathological and pharmacological mechanisms and to inform strategies for mitigating skeletal complications in patients with hip OA.
The interpretation of our findings should be considered in the context of contemporary opioid prescribing principles. Although the 2018 World Health Organization (WHO) analgesic ladder was originally developed for cancer pain and focuses primarily on pain control, more recent guidance emphasizes balancing analgesic efficacy, safety, and regular reassessment.29,30 While codeine has traditionally been classified as a “weak” opioid, this binary classification may be misleading, as inadequate analgesic efficacy can paradoxically increase harm by prolonging pain exposure and prompting treatment escalation or overlapping analgesic regimens.29,30 Inadequate pain control with codeine may therefore exacerbate pain-related distress and psychiatric vulnerability, particularly anxiety and sleep disorders.31 In contrast, appropriately selected and dosed higher-potency opioids, such as oxycodone, when combined with non-opioid analgesics, may provide more stable analgesia with lower escalation pressure.29,30 From this perspective, our subgroup analyses showed that psychiatric and fracture risks associated with codeine were more pronounced among patients receiving concomitant NSAIDs or tramadol, suggesting that stepwise or combination analgesic strategies may reflect refractory pain states rather than improved safety. Accordingly, a rigid “weak-first” opioid strategy may not be optimal for all patients with hip osteoarthritis. Instead, individualized opioid selection that integrates analgesic potency, concomitant non-opioid therapy, psychiatric vulnerability, and comorbidity burden may help minimize unnecessary dose escalation and overlapping opioid exposure, thereby potentially contributing to overdose risk mitigation. However, given the observational nature of this study, these interpretations should be made cautiously and should not be construed as causal inferences. Future prospective studies are warranted to evaluate whether efficacy-driven opioid selection and structured reassessment strategies can reduce adverse outcomes, including overdose and long-term psychiatric complications.
Strength and Limitation
To the best of our knowledge, this study represents one of the largest nationwide population-based study to longitudinally and directly compare the risks of psychiatric disorders, MACE, and fractures between codeine and oxycodone in patients with hip OA. The large sample size, extended follow-up period, and rigorous methodological approaches, including PSM and IPTW, strengthen the validity of our findings. Additionally, stratified subgroup analyses allowed us to differentiate risks according to patient-, disease-, and treatment-specific characteristics, providing clinically valuable insights for opioid prescribing. Nonetheless, several limitations should be acknowledged. First, as this was an observational study, residual confounding cannot be completely excluded despite extensive covariate adjustment and matching strategies. Important unmeasured confounding variables, including pain severity and intensity, functional limitation, and osteoarthritis stage, were not available, all of which may influence both opioid selection and the outcome measured. Second, outcomes definitions relied on diagnostic codes, and information on lifestyle factors such as smoking, alcohol use, and physical activity, as well as laboratory data, was not available in claims data. In addition, opioid dose-related information, including morphine milligram equivalents (MME), treatment adherence, and time-varying patterns of opioid exposure, could not be assessed. Moreover, over-the-counter use of NSAIDs was also unavailable and therefore could not be accounted for in the analysis. Third, only psychiatric disorders were screened prior to the index date, as excluding patients with histories related to secondary outcomes would have substantially reduced the sample size. Fourth, patients aged ≥85 years were excluded from the analysis to reduce potential bias related to extreme age, including pronounced heterogeneity in health status, frailty, multimorbidity, polypharmacy, and competing risks such as non-opioid-related mortality, which could complicate the interpretation of comparative safety outcomes. While this approach improved internal validity, it may limit the generalizability of our findings to the very old population, and caution is warranted when extrapolating these results to patients aged ≥85 years. Finally, residual imbalance in certain comorbidities, including osteoporosis and asthma, as well as concomitant tramadol use, persisted between groups even after propensity score matching, which may have influenced outcomes given tramadol’s CNS activity and analgesic properties. However, osteoporosis, asthma, and concomitant tramadol use were all adjusted for in the multivariable Cox regression models, and their potential effect modification was further examined through stratified subgroup analyses. Importantly, IPTW sensitivity analyses yielded results consistent with the primary findings, suggesting that the influence of these residual imbalances on the overall conclusions was likely limited; nevertheless, cautious interpretation remains warranted. Further studies are warranted to extend and refine the findings of this study, incorporating pain severity, functional status, frailty indices, and laboratory measurements, to better account for disease severity and patient vulnerability. Moreover, investigations focusing on very old populations (aged ≥85 years) are particularly important to address safety concerns in this high-risk group. Further studies are warranted to refine these findings by incorporating more clinical data, including pain severity, functional status, frailty indices, osteoarthritis staging, and laboratory measurements, to better address disease severity and patient vulnerability. Future research should also integrate opioid dose metrics, treatment duration and adherence, pharmacogenetic modifiers (eg, CYP2D6 polymorphisms), and pathological factors related to fall dynamics and fracture site distribution. In addition, investigations focusing on very old populations (aged ≥85 years) and on interactions between opioids and concomitant CNS-active medications are essential to improve individualized opioid prescribing strategies and safety.
Conclusion
This study revealed clinically meaningful differences in the safety profiles of codeine and oxycodone. Codeine use was consistently associated with a higher risk of psychiatric disorders, particularly anxiety and sleep disorders, while the risks of MACE and death were comparable between the two opioids. Fracture outcomes demonstrated divergent patterns, with codeine use associated with a lower risk of femoral fractures but a higher risk of non-femoral fractures. Importantly, these findings challenge the conventional assumption that codeine, as a “weak” opioid, represents a uniformly safer initial analgesic option. Conversely, oxycodone demonstrated a comparatively lower observed risk of psychiatric outcomes, particularly among patients with psychiatric vulnerability. This study emphasizes the importance of individualized opioid prescribing strategies that account for mental health risk, comorbidity profiles, and fracture risk, rather than relying solely on opioid potency classification. In this context, pharmacogenetic factors, including variability in CYP2D6 activity, may represent an important consideration for future individualized opioid selection strategies. In addition, further controlled studies integrating detailed measures of pain severity, functional status, frailty, opioid dose and duration, as well as pharmacogenetic and drug-drug interaction data, are needed to understand disease-related factors from drug-specific effects and to optimize long-term opioid safety in diverse patient populations.
Data Sharing Statement
The data used in this study were obtained with permission from the Korean Health Insurance Review and Assessment Service (HIRA). Due to HIRA regulations, the data cannot be publicly shared or directly provided by the authors. However, the data are available from HIRA upon reasonable request and with appropriate institutional review board approval.
Author Contributions
Jeongmin Lee and Yujin Kim are co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from Kyung Hee University in 2024 (KHU–20241064). Y.J. Choi received funds from Kyung Hee University.
Disclosure
The authors declare no competing interest.
References
1. Fan Z, Yan L, Liu H, et al. The prevalence of Hip osteoarthritis: a systematic review and meta-analysis. Arthritis Res Ther. 2023;25(1):51. doi:10.1186/s13075-023-03033-7
2. Lopes DG, Costa D, Cruz EB, et al. Association of physical activity with physical function and quality of life in people with Hip and knee osteoarthritis: longitudinal analysis of a population-based cohort. Arthritis Res Ther. 2023;25(1):14. doi:10.1186/s13075-023-02996-x
3. Gibbs AJ, Gray B, Wallis JA, et al. Recommendations for the management of Hip and knee osteoarthritis: a systematic review of clinical practice guidelines. Osteoarthritis Cartilage. 2023;31(10):1280–20. doi:10.1016/j.joca.2023.05.015
4. van den Driest JJ, Schiphof D, de Wilde M, Bindels PJE, van der Lei J, Bierma-Zeinstra SMA. Opioid prescriptions in patients with osteoarthritis: a population-based cohort study. Rheumatology. 2020;59(9):2462–2470. doi:10.1093/rheumatology/kez646
5. Li W, He H, Yang Z, Wu Z, Xie D. Comparative risk-benefit profiles of weak opioids in the treatment of osteoarthritis: a network meta-analysis of randomized controlled trials. Postgrad Med. 2022;134(8):784–794. doi:10.1080/00325481.2022.2080360
6. Martins SS, Fenton MC, Keyes KM, Blanco C, Zhu H, Storr CL. Mood and anxiety disorders and their association with non-medical prescription opioid use and prescription opioid-use disorder: longitudinal evidence from the National Epidemiologic Study on Alcohol and Related Conditions. Psychol Med. 2012;42(6):1261–1272. doi:10.1017/s0033291711002145
7. Scherrer JF, Svrakic DM, Freedland KE, et al. Prescription opioid analgesics increase the risk of depression. J Gen Intern Med. 2014;29(3):491–499. doi:10.1007/s11606-013-2648-1
8. Choi YJ, Kim M-H, Chung EK, et al. Prevalence and seriousness of analgesic-induced adverse events in Korea: a 10-year nationwide surveillance. J Patient Saf. 2020;16(4):e215–e224. doi:10.1097/PTS.0000000000000742
9. Scherrer JF, Salas J, Copeland LA, et al. Prescription opioid duration, dose, and increased risk of depression in 3 large patient populations. Ann Fam Med. 2016;14(1):54. doi:10.1370/afm.1885
10. Cheatle MD, Compton PA, Dhingra L, Wasser TE, O’Brien CP. Development of the revised opioid risk tool to predict opioid use disorder in patients with chronic nonmalignant pain. J Pain. 2019;20(7):842–851. doi:10.1016/j.jpain.2019.01.011
11. Schofield J, Conti AA, Khan F, Baldacchino AM. Association between chronic opioid exposure and cardiovascular disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2025;zwaf500. doi:10.1093/eurjpc/zwaf500
12. Oh TK, Cho HW, Song IA. Association of opioid prescription with major adverse cardiovascular events: nationwide cohort study. J Clin Med. 2025;14(4):1205. doi:10.3390/jcm14041205
13. Saunders KW, Dunn KM, Merrill JO, et al. Relationship of opioid use and dosage levels to fractures in older chronic pain patients. J Gen Intern Med. 2010;25(4):310–315. doi:10.1007/s11606-009-1218-z
14. Peach EJ, Pearce FA, Gibson J, Cooper AJ, Chen LC, Knaggs RD. Opioids and the risk of fracture: a self-controlled case series study in the clinical practice research datalink. Am J Epidemiol. 2021;190(7):1324–1331. doi:10.1093/aje/kwab042
15. Ramli FF, Syed Hashim SA, Mohd Effendy N. Factors associated with low bone density in opioid substitution therapy patients: a systematic review. Int J Med Sci. 2021;18(2):575–581. doi:10.7150/ijms.52201
16. Virnes RE, Tiihonen M, Karttunen N, van Poelgeest EP, van der Velde N, Hartikainen S. Opioids and falls risk in older adults: a narrative review. Drugs Aging. 2022;39(3):199–207. doi:10.1007/s40266-022-00929-y
17. Abrego-Guandique DM, Nucera S, Ilari S, et al. The association between long-term opioid use and dementia risk: a systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Pyschiatry. 2025;144:111595. doi:10.1016/j.pnpbp.2025.111595
18. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
19. Kim HK, Song SO, Noh J, Jeong IK, Lee BW. Data configuration and publication trends for the Korean national health insurance and health insurance review & assessment database. Diabetes Metab J. 2020;44(5):671–678. doi:10.4093/dmj.2020.0207
20. Wu X, Yuan L, Zuo J, Lv J, Guo T. The impact of CYP2D6 polymorphisms on the pharmacokinetics of codeine and its metabolites in Mongolian Chinese subjects. Eur J Clin Pharmacol. 2014;70(1):57–63. doi:10.1007/s00228-013-1573-x
21. Jung EH, Lee C-M, Byeon J-Y, et al. Relationship between plasma exposure of zolpidem and CYP2D6 genotype in healthy Korean subjects. Arch Pharm Res. 2020;43(9):976–981. doi:10.1007/s12272-020-01250-1
22. Tang NK. Insomnia co-occurring with chronic pain: clinical features, interaction, assessments and possible interventions. Rev Pain. 2008;2(1):2–7. doi:10.1177/204946370800200102
23. Sheen CH, Schleimer RP, Kulka M. Codeine induces human mast cell chemokine and cytokine production: involvement of G-protein activation. Allergy. 2007;62(5):532–538. doi:10.1111/j.1398-9995.2007.01345.x
24. Thakkar MM. Histamine in the regulation of wakefulness. Sleep Med Rev. 2011;15(1):65–74. doi:10.1016/j.smrv.2010.06.004
25. Zhou Z, An Q, Zhang W, Li Y, Zhang Q, Yan H. Histamine and receptors in neuroinflammation: their roles on neurodegenerative diseases. Behav Brain Res. 2024;465:114964. doi:10.1016/j.bbr.2024.114964
26. Rickli A, Liakoni E, Hoener MC, Liechti ME. Opioid-induced inhibition of the human 5-HT and noradrenaline transporters in vitro: link to clinical reports of serotonin syndrome. Br J Pharmacol. 2018;175(3):532–543. doi:10.1111/bph.14105
27. Toska E, Mayrovitz HN. Opioid impacts on cardiovascular health. Cureus. 2023;15(9):e46224. doi:10.7759/cureus.46224
28. Maluta T, Toso G, Negri S, Samaila EM, Magnan B. Correlation between Hip osteoarthritis and proximal femoral fracture site: could it be protective for intracapsular neck fractures? A retrospective study on 320 cases. Osteoporos Int. 2019;30(8):1591–1596. doi:10.1007/s00198-019-05015-5
29. Thompson J. The WHO guidelines: the new and the old. Curr Opin Support Palliat Care. 2024;18(4):169–174. doi:10.1097/SPC.0000000000000722
30. Yang J, Bauer BA, Wahner-Roedler DL, Chon TY, Xiao L. The modified WHO analgesic ladder: is it appropriate for chronic non-cancer pain? J Pain Res. 2020;13:411–417. doi:10.2147/JPR.S244173
31. Seiger AN, Penzel T, Fietze I. Chronic pain management and sleep disorders. Cell Rep Med. 2024;5:101761. doi:10.1016/j.xcrm.2024.101761
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.