Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Pseudofolliculitis barbae; current treatment options
Authors Ogunbiyi A
Received 10 July 2018
Accepted for publication 4 February 2019
Published 16 April 2019 Volume 2019:12 Pages 241—247
DOI https://doi.org/10.2147/CCID.S149250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Adebola Ogunbiyi
Department of Medicine, University College Hospital, Ibadan, Oyo State, Nigeria
Abstract: Pseudofolliculitis barbae (PFB) is a chronic inflammatory disorder of follicular and peri-follicular skin characterized by papules, pustules, and post-inflammatory hyperpigmentation. It occurs more frequently in men of African and Asian descent. The etiology of PFB is multifactorial. Shaving or plucking the hair precipitates the onset of an inflammatory reaction that results from the penetration of the adjacent skin by the growing sharp tips. The curved shape of the hair follicle allows for the downward curvature and penetration of the growing hair tips into the skin. The onset of the foreign body reaction leads to itching and the development of papules, pustules, and post-inflammatory hyperpigmentation, especially in the beard area although other shaved areas of the body may be affected. Keloids have also been known to develop after the onset of PFB, giving rise to extensive unsightly scars. Diagnosis is clinical. Cessation of shaving or removal of the involved hair follicles usually terminates the development of PFB. Individuals with the single nucleotide substitution in the hair follicle companion layer specific keratin gene (K6hf) have a six fold increased chance of developing PFB.
Keywords: pseudofolliculitis barbae, pathogenesis, treatment
Introduction
Pseudofolliculitis barbae (PFB) also known as shaving bumps, sycosis barbae, and traumatic folliculitis of the beard, is an inflammatory disorder of follicular and peri-follicular skin resulting from ingrown hairs due to hair removal.1–4 It is characterized by the development of itchy papules, pustules, and post-inflammatory hyperpigmentation. It is commonly seen in the beard area but it has been reported in other areas with terminal hairs after hair removal. It occurs more frequently in those with tight curly hair, especially in men of African and, to a lesser extent, those of Asian descent.5,6 PFB is multifactorial in origin, but the shaving of terminal hair usually triggers it.
History
The occurrence of a rash after shaving had been described by Fox in 19087 but the term pseudo-folliculitis barbae was coined by Strauss and Kligman in 1956.8 An increase in the number of African Americans into the US armed forces in the sixties and seventies saw a rise in its prevalence to 45% in the population of black men in the forces5 because of the “clean-shaven policy” in the Military. However, there appears to be a reduced prevalence of PFB in Nigeria, possibly as a result of the change in shaving habits and availability of better treatment options.
Epidemiology
The current incidence of PFB is unknown. It has been suggested that ~5 million blacks have severe PFB in the USA. It has however been reported less frequently in Asians, Hispanics and, fewer still, in Caucasians. In the military where a clean-shaven policy exists, earlier reports gave a prevalence of 45%–83% among black recruits and soldiers in the US army with fewer occurrences in the white soldiers.5,9,10
The age of onset is post-pubertal at which time the secondary sexual hairs (facial, axillary, pubic, chest) commence significant growth. The hairs are thick and curly requiring a shave especially with the desire of a hairless body. Although facial PFB is uncommon in women, its prevalence is increased in those with hirsutism due to PCOS.11 There has also been an increase in PFB in peri-menopausal or menopausal women.
Pathogenesis
The pathogenesis of PFB is multifactorial. Implicated factors include the shape of the hair follicle, the structure of the hair, genetic factors, and hair grooming methods. Its onset is precipitated by hair removal in genetically predisposed individuals. These factors are discussed in the following sections.
The hair follicle in Africans is curved with its concavity toward the epidermis. The curved shape of the hair follicle is responsible for the curly, spiral or helical nature of the African hair.12–14 After a close shave, emerging sharp-tipped hairs from the follicle grow downwards or parallel to the skin and penetrate the skin a few millimeters away from the follicle, known as extra-follicular penetration (Figure 1A, B). The penetration of the epidermis by the hair shaft causes invagination of the epidermis simulating a follicle hence the name “pseudofollicle”. Extra-follicular penetration occurs frequently where the hair normally grows at an oblique angle to the skin as seen in the anterior neck area.15 The penetration of the hair into the epidermis or dermis gives rise to a foreign body reaction. The reaction is characterized by the formation of papules or pustules, which may be perifollicular or follicular (Figure 2).
 | Figure 1 Penetration of sharptipped hairs into the skin (A) and multiple extrafollicular penetration with papules (B). |
 | Figure 2 Extra-follicular and transfollicular penetration. |
In cases where there is pulling on the hair before cutting, either by stretching the skin or shaving against the grain, the cut sharp tip of the hair retracts into the follicle. Due to the curved nature of the hair, while attempting to grow the sharp tip will penetrate the follicular wall below the skin and produce a foreign body reaction. This is known as transfollicular penetration (Figure 3). This transfollicular penetration can be verified by histology. The thickness of the hair shaft and its curly nature encourage penetration, and this may explain why PFB is uncommon in the upper lip (mustache area) where the hair is less coiled and has a smaller diameter compared with other facial hair. A previous report showed that the curly nature of hair and the presence of whorls increase the risk of developing PFB by 50%.16 If left to grow to a length of ~10 mm, the entrapped hair is pulled out of the inflammatory papule.17 This leads to spontaneous regression of the lesion (Figure 4).
 | Figure 3 Transfollicular penetration. |
 | Figure 4 Trapped hair separating from the papule. |
Hair grooming methods
Shaving of facial hair with various shaving instruments has been linked to PFB. Double-edged razor blades have been associated with transfollicular penetration of growing hairs. When using multiple blade razors, the first blade pulls the hair while the second cuts the hair. The pulled hair retracts into the follicle giving a smooth shave but encourages transfollicular penetration of the growing hair.14,15,18 A recent report however has suggested that improper shaving techniques with razors rather than multiple blades is what predisposes to transfollicular penetration.19,20 Stretching the skin before shaving, shaving against the grain or use of blunt blades may also increase the chance of transfollicular penetration. Dry shaving (no prior moisturization of the hair) with razors usually produces sharp beveled tips encouraging extra-follicular penetration (Figure 5). The use of pre-shave care with warm water or other pre-shave care regimes, improves hydration of the hair shaft causing it to swell, thus ending up with blunt edges after shaving.
 | Figure 5 Multiple sharp, beveled hair tips after a dry shave. |
Infrequent shaving allows the hair to grow to a length that leads to penetration.20 Plucking of hairs by various means may be insufficient leaving behind some hair fragment under the skin leading to an inflammatory reaction.21 Thus, frequent shaving is encouraged when using razors.
Genetics
Winter et al discovered a single-nucleotide substitution in the hair follicle companion layer specific keratin (K6hf).22 Carriers of the A12T polymorphism of the gene coding for keratin, have a six fold increased chance of developing PFB.21 It is believed that the mutation in K6hf leads to a weakened cytoskeleton increasing the chances of ingrowing hair. The same authors reported that 76% of regularly shaving men who carry the A12T polymorphism develop PFB making this a significant risk factor for the condition.
Finally, PFB has been associated with the use of cyclosporine and corticosteroids in renal transplant patients23,24 and it has also been associated with pressure from the violin under the mandible “Fiddlers neck”.25
Clinical features
PFB presents with pruritus or pain in the shaved areas a day or two after shaving, followed by the development of papules and pustules. Facial hair is the most common site for shaving, thus explaining why PFB is seen commonly on the face. The most common site in men is the anterior neck region, followed by the cheeks, and the chin. The anterior neck region is commonly affected because of the oblique nature and increased density of hair follicles in the area (Figure 6A, B). In women, the chin is the most common area involved, most probably because hirsute women tend to have more hair on the chin when compared to the anterior neck and cheeks.
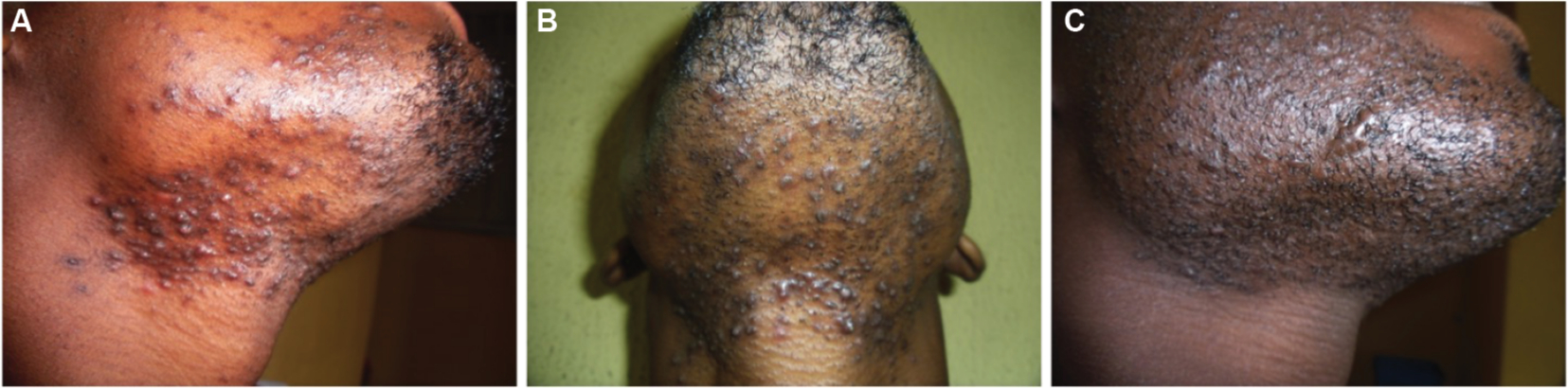 | Figure 6 Papules and pustules on the anterior neck, chin, and cheeks (A); PFB affecting mainly the anterior neck region (B); keloids resulting from lesions from PFB (C). Abbreviation: PFB, pseudofolliculitis barbae. |
New lesions may be erythematous while older lesions are usually darker. Most papules range from 2 to 5 mm in diameter although larger lesions may be seen, especially when there is secondary infection. The pustules are usually secondary lesions due to infection with Staphylococcus epidermidis.
Post-inflammatory hyperpigmentation is a common complication in darker skin, which may lead to the development of keloids especially in the beard area in predisposed individuals17 (Figure 6C).
PFB is also seen on the limbs, the pubic region, and axilla in women who shave those areas commonly. Women with PFB have a higher prevalence of hyperandrogenism with 41% of them reporting a family history of hirsutism or hypertrichosis.26
Dermoscopic findings include extra-follicular penetration, peri-follicular and follicular papules and pustules. Peri-follicular hyperkeratosis is usually present in older lesions. Linear hair growth in the skin may also be seen.
We have found dermoscopy useful in diagnosis and management of patients with PFB. Dermoscopic pictures showing ingrown hairs and sharp-tipped hairs convince the patient of the etiology of PBF and the contribution of shaving methods to the development of PFB. Figure 7 shows blunt-tipped hairs as a result of using depilatories instead of shaving. A prior history of hair removal on the affected site predates the rash. Important information required from the patient includes method of hair removal and shaving techniques. The severity of PFB can be assessed using a PFB tool which is useful in monitoring treatment.27
 | Figure 7 Use of depilatories produced two crooked blunt tips unlikely to cause penetration in a patient with existing papules. |
Differential diagnosis of PFB on the face includes other causes of papules and pustules on the face. Traumatic folliculitis (razor burns) usually develops after a close shave but usually clears within 24–48 hours and acne usually presents with comedones and papules on the non-hairy areas of the face. Primary folliculitis, impetigo, and tinea barbae could all present as facial papules and pustules. Typical annular, raised, scaly lesions with central clearing and peripheral activity usually suggest tinea barbae, which commonly occurs unilaterally and presents with erythematous and skin-colored papules. Micropapular sarcoidosis is also a differential diagnosis in dark skin.28 The lesions of sarcoidosis are usually monomorphic, asymptomatic, and remain unchanged for long periods of time. The absence of ingrown hairs on dermoscopy helps to exclude the conditions listed.
Histopathology
Both the extra-follicular and intra-follicular penetration of the hair shaft into the epidermis or dermis evokes an inflammatory reaction. Histology of an affected lesion shows polymorphonuclear cellular aggregation around the penetrating shaft leading to a micro-abscess in the epidermis. Dermal penetration leads to a more severe inflammatory reaction. Foreign body granulomatous inflammation may result from this penetration and fibrosis can be stimulated from the foreign body reaction.
Management
PFB is a chronic disorder that ultimately affects a patient’s self-esteem and quality of life. The therapeutic objectives for PFB include managing ongoing inflammation and its complications, and preventing the development of new lesions. This will ultimately improve the esthetic appearance of the lesions.
In patients with acute inflammation, shaving should be stopped. Shaving an irregular skin surface due to the presence of the papules leads to more irritation. When ingrown hairs are few, the trapped hairs may be removed with the use of a sterile needle.28 Cessation of shaving may lead to a temporary increase in symptoms for the first few days, however this gradually improves over time. If shaving can be stopped then symptoms will abate and complications such as post-inflammatory hyperpigmentation or keloids can be dealt with (Figure 8).
 | Figure 8 Treatment algorithm for PFB. Reprinted from Coley MK, Kelly Alexis AF. Pseudofolliculitis barbae and acne keloidalis nuchae. In Alexis AF, Barbosa VH, editors. Skin of Color: a practical guide to dermatologic diagnosis and treatment, 1st edition. New York: Springer; 2013:127 with permission from Springer Nature.40 Abbreviation: PFB, pseudofolliculitis barbae. |
In patients with moderate to severe inflammation, the use of topical medications such as corticosteroids, antibiotics, and benzyl peroxide has been found useful as monotherapy or in combination.29,30 Topical clindamycin and benzyl peroxide have been found useful in reducing inflammation by reducing contamination of the normal skin flora which may contribute to inflammation. They also prevent the development of secondary infection. In cases of moderate to severe inflammation or when the lesions are predominantly pustules, oral antibiotics, low dose tetracycline derivatives, macrolides, or penicillins may be used. Topical steroid combinations and intralesional corticosteroids can also be used for short periods to reduce inflammation. Atrophy and hypopigmentation may occur in black skin when used for prolonged periods of time.
Keratolytics have been found useful in the management of PFB. They help in reducing the peri-follicular hyperkeratosis associated with the condition. Topical keratolytics including retinoids, salicylic acid, and alpha hydroxy acids can be used. Daily application of glycolic acid has been found useful in treatment of PFB.31,32 Chemical peels, especially glycolic and salicylic acid peels, have also been found useful. Glycolic acid peels reduce the curvature of the hair by reducing the sulfhydryl bonds in the hair shaft, thus reducing the chance of penetration into the skin.33
Post-inflammatory hyperpigmentation is a frequent complication of PFB in blacks. Chemical peels, azelaic acid, hydroquinone, and its derivatives have been found useful in reducing post-inflammatory hyperpigmentation. Patients should avoid the use of photosensitizers in their shave care regime and sunscreens should be applied as needed.17,28
The use of intralesional steroids, dermabrasion, semi-ablative lasers, and surgery have been found useful in the management of scars, including keloids.
Definitive treatment of PFB involves removal of the hair follicle. Various modalities for hair removal are currently in use and these include; wax epilation as well as mechanical removal with tweezers. Both methods however may predispose to transfollicular penetration. Electrolysis is another method in use but it is painful and expensive and usually has to be repeated as required. It has also been noted that the needle for the procedure may miss the hair bulb in some curved hair follicles, thus predisposing to transfollicular penetratration.17 Surgical depilation of involved hair follicles has also been tried. However, this may predispose to keloid formation in predisposed individuals.
Various laser systems have been found useful for hair removal. In dark skin, the long-pulsed neodymium:yttrium aluminum garnet (Nd:YAG) 1,064 mm, diode 800–810 nm, pulsed alexandrite 755 nm, and pulsed non-coherent light source are particularly effective.34–36 Hair follicles are targeted for removal with melanin acting as the chromophore. The hair bulb contains a lot of melanin and thus suffers the greatest damage. Usually 3–7 sessions are necessary for optimal results. The diameter of the hair shafts may also be reduced if not completely destroyed, which also reduces the chance of PFB occurring. Side effects from lasers include pain, erythema, and scab and scar formation.
Prevention
Hair removal is the main trigger for the development of PFB and cessation of shaving usually stops its occurrence over a period of ~12 weeks. However, for those who prefer to have a clean shave or have jobs requiring employees to maintain a clean shave, shaving methods with fewer chances of developing PFB should be used with emphasis on proper shaving techniques (Figure 8). Ongoing inflammation can then be managed as discussed previously.
The use of electric hair clippers for shaving has been associated with a reduction in the occurrence of PFB and is currently being used for shaving both facial and scalp hair in men of African descent. The clipper has a guard that can be adjusted in width thus preventing a close shave. It is recommended that a minimum of 1 mm of hair should be left behind. This reduces the chance of trans- and extra-follicular penetration of the growing hair shaft.37,38 The use of pre- and post-shave care may further reduce the occurrence of PFB in those who shave with clippers.
Shaving with razors, especially with multiple blades is commonly associated with PFB and is usually discouraged. However, shaving with razors does give the cleanest shave. It has been emphasized that proper attention to the shaving process and increasing the frequency of shaving can reduce the occurrence of PFB in individuals who wish to shave with razors. Pulling or stretching the skin while shaving should be discouraged as it may encourage transfollicular penetration of the growing hair shaft. Dry shaving with razors should be discouraged as it produces sharp, beveled hair tips aiding penetration into the skin. Shaving against the grain also increases the chance of PFB. Pre-shave regime, especially with warm water causes the hair shaft to swell thus reducing the chance of producing a beveled, sharp tip after a shave. Blunt razors also increase the chances of developing PFB because the blunt razor may not cut the hair at once, causing the hair to stretch before cutting. This may lead to a recoil of the cut hair shaft into the follicle, thereby encouraging transfollicular penetration. The use of aftershave care has also been found useful.12
The use of depilatories rarely causes PFB. They act by lysing the disulfide bonds in the hair shaft, thereby softening the hair, leading to a blunt or feathered tip unlikely to lead to extra- or transfollicular penetration (Figure 7).12 Unfortunately, most depilatories contain barium sulfide and sodium thioglycollate, which have unpleasant odors and may lead to skin irritation. They could be applied for hair removal every 2–3 days but they must be washed off properly.
Topical eflornithine hydrochloride has been used for the treatment of unwanted facial hair in women. It retards the rate of hair growth by inhibiting an enzyme necessary for hair cell division. It has to be used in conjunction with another hair removal technique, usually for the first 8 weeks.39 It can be used in combination with laser therapy.
Conclusion
PFB is a chronic disease occurring in genetically predisposed individuals. It is precipitated by hair removal and characterized by itchy, painful papules, and pustules. It is seen in individuals with curly, thick hair, especially those of African and, to a lesser extent, Asian descent. Although it is commonly seen in the beard area, it can occur in other areas with terminal hairs that are frequently shaved. Paying close attention to hair grooming methods may reduce its occurrence. Topical steroids, retinoic acid, keratolytics, and antibiotics are useful adjuncts in management. Definitive therapy involves the removal of the hair follicle using lasers.
Disclosure
The author received honorarium from Proctor and Gamble while carrying out the study. The author reports no other conflicts of interest in this work.
References
Kenney JA. Management of dermatoses peculiar to Negroes. Arch Dermatol. 1965;91(2):126–128. | ||
Steck WD. Pseudofolliculitis of the Beard. Digest. 1971;22:1–4. | ||
Brauner GJ, Flandermeyer KL. Pseudofolliculitis barbae. Medical consequences of interracial friction in the US army. Cutis. 1979;23(1):61–66. | ||
Quarles FN, Coley MK, Alexis AF, Dermatological disorders in men of African descent. In: Dadzie OE, Petit A, Alexis AF, editors. Ethnic Dermatology Principles and Practice. 1st ed. Chichester, West Sussex: Wiley-Blackwell; 2013:241–256. | ||
Alexander AM, Delph WI. Pseudofolliculitis barbae in the military. a medical, administrative and social problem. J Natl Med Assoc. 1974;66(6):459–795. | ||
Coley MK, Alexis AF. Dermatologic conditions in men of African ancestry. Expert Rev Dermatol. 2009;4(6):595–609. | ||
Fox H. Observations on skin diseases in the Negro. J Cutan Dis. 1980;26:67–79. | ||
Strauss JS, Kligman AM. Pseudofolliculitis of the beard. Arch Dermatol. 1956;74(5):533–542. | ||
Alexander AM, Delph WI, Am A, Alexander WI. Pseudofolliculitis barbae in the military. A medical, administrative and social problem. J Natl Med Assoc. 1974;66(6):459–464. | ||
Sattgast JE. Pseudofolliculitis – a dilemma for the army. Med Bull US Army Eur. 1982;39:3–11. | ||
Gilchrist VJ, Hecht BR. A practical approach to hirsutism. Am Fam Physician. 1995;52(6):1837–1846. | ||
Steggerda M, Seibert HC. Size and shape of head hair from six racial groups. J Hered. 1941;32(9):315–318. | ||
Halder RM, Grimes PE, McLaurin CI, Kress MA, Kenney JA. Incidence of common dermatoses in a predominantly black dermatologic practice. Cutis. 1983;32(4):388–390Jr. | ||
Vogt A, McElwee KJ, Blume-Peytavi U. Biology of the hair follicle. In: Blume-Peytavi U, Tosti A, Tr€ueb RM, editors. Hair Growth and Disorders. Springer, Berlin: Heidelberg; 2008:1–22. | ||
Halder RM. Pseudofolliculitis barbae and related disorders. Dermatol Clin. 1988;6(3):407–412. | ||
Ross EV, Evans LA, Yeager JK, La E. Pseudofolliculitis barbae associated with an unusual hair whorl. Cutis. 1993;51(2):107–108. | ||
Perry PK, Cook-Bolden FE, Rahman Z, Jones E, Taylor SC. Defining pseudofolliculitis barbae in 2001: a review of the literature and current trends. J Am Acad Dermatol. 2002;46(2 Suppl Understanding):S113–S119. | ||
Brown LA. Pathogenesis and treatment of pseudofolliculitis barbae. Cutis. 1983;32(4):373–375. | ||
Daniel A, Gustafson CJ, Zupkosky PJ, et al. Shave frequency and regimen variation effects on the management of pseudofolliculitis barbae. J Drugs Dermatol. 2013;12(4):410–418. | ||
Gray J, McMichael AJ, Michael M. Pseudofolliculitis barbae: understanding the condition and the role of facial grooming. Int J Cosmet Sci. 2016;38(suppl 1):24–27AJ. | ||
Benedette DV. Pseudofolliculitis barbae can lead to medical and social problems. Cosmetic Dermatol. 1993;6(12):44–45. | ||
Winter H, Schissel D, Parry, et al. An unusual Ala12Thr polymorphism in the 1A alpha-helical segment of the companion layer-specific keratin K6hf: evidence for a risk factor in the etiology of the common hair disorder pseudofolliculitis barbae. J Invest. 2004;122(3):652–657. | ||
Lear J, Bourke JF, Burns DA. Hyperplastic pseudofolliculitis barbae associated with cyclosporin. Br J Dermatol. 1997;136(1):132–133. | ||
Lally A, Wojnarowska F. Hypertrophic pseudofolliculitis in white renal transplant recipients. Clin Exp Dermatol. 2007;32(3):268–271. | ||
Lachappelle JM, Tennstedt D, Cromphaut P. Pseudofolliculits of the beard and fiddlers neck (letter). Contact Dermatol. 1982;7:247. | ||
Garcia RL, White JW. Pseudofolliculitis barbae in a woman. Arch Dermatol. 1978;114(12):1856. | ||
Dunn JF. Pseudofolliculitis barbae. Am Fam Physician. 1988;38(3):169–174. | ||
Ribera M, Fernandez-Chico N, Casals M. [Pseudofolliculitis barbae]. Actas Dermosifiliogr. 2010;101(9):749–757. Spanish. | ||
Bridgeman-Shah S. The medical and surgical therapy of pseudofolliculitis barbae. Dermatol Ther. 2004;17(2):158–163. | ||
Cook-Bolden FE, Barba A, Halder R, Taylor S. Twice-daily applications of benzoyl peroxide 5% clindamycin 1%gel versus vehicle in the treatment of pseudofolliculitis barbae. Cutis. 2004;73(Suppl)18–24. | ||
Kligman AM. Mills OH Jr. Pseudofolliculitis of the beard and topically applied tretinoin. Arch Dermatol. 1973;107(4):551–552. | ||
Coley MK, Alexis AF. Managing common dermatoses in skin of color. Semin Cutan Med Surg. 2009;28(2):63–70. | ||
Perricone NV. Treatment of pseudofolliculitis barbae with topical glycolic acid: a report of two studies. Cutis. 1993;52(4):232–235. | ||
Thomas EJ. Lasers in treatment of pseudofolliculitis barbae. Dermatol Surg. 1999;25(5):422–423. | ||
Rogers CJ, Glaser DA. Treatment of pseudofolliculitis barbae using the Q-switched Nd:YAG laser with topical carbon suspension. Dermatol Surg. 2000;26(8):737–742. | ||
Battle EF, Hobbs LM. Laser-assisted hair removal for darker skin types. Dermatol Ther. 2004;17(2):177–183. | ||
Alexander AM. Evaluation of a foil-guarded shaver in the management of pseudofolliculitis barbae. Cutis. 1981;27(5):534–542. | ||
Al H, Garcia RL, Garcia RL, Henderson AL. The adjustable rotary electric razor in the control of pseudofolliculitis barbae. J Assoc Mil Dermatol. 1978;4:28. | ||
Xia Y, Cho S, Howard RS, Maggio KL. Topical eflornithine hydrochloride improves the effectiveness of standard laser hair removal for treating pseudofolliculitis barbae: a randomized, double-blinded, placebo-controlled trial. J Am Acad Dermatol. 2012;67(4):694–699. | ||
Coley MK, Kelly Alexis AF. Pseudofolliculitis barbae and acne keloidalis nuchae. In: Alexis AF, Barbosa VH, editors. Skin of Color: A Practical Guide to Dermatologic Diagnosis and Treatment. 1st edition. New York: Springer; 2013:127. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.