Back to Journals » Patient Preference and Adherence » Volume 15
Proxy-Reported Quality of Life and Access to Nusinersen Among Patients with Spinal Muscular Atrophy in Saudi Arabia
Authors AlRuthia Y ![]() , Almuaythir GS, H Alrasheed H, Alsharif WR, Temsah MH
, Almuaythir GS, H Alrasheed H, Alsharif WR, Temsah MH ![]() , Alsohime F, Sales I
, Alsohime F, Sales I ![]() , Alwhaibi M
, Alwhaibi M ![]() , Bashiri FA
, Bashiri FA ![]()
Received 8 February 2021
Accepted for publication 19 March 2021
Published 13 April 2021 Volume 2021:15 Pages 729—739
DOI https://doi.org/10.2147/PPA.S305849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yazed AlRuthia,1,2 Ghadah S Almuaythir,1 Hala H Alrasheed,1 Wejdan R Alsharif,1 Mohamad-Hani Temsah,3,4 Fahad Alsohime,3,4 Ibrahim Sales,1 Monira Alwhaibi,1 Fahad A Bashiri3,5
1Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 2Pharmacoeconomics Research Unit, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 3College of Medicine, King Saud University, Riyadh, Saudi Arabia; 4Pediatric Intensive Care Unit, Pediatric Department, King Saud University Medical City, Riyadh, Saudi Arabia; 5Division of Neurology, Department of Pediatrics, King Saud University Medical City, Riyadh, Saudi Arabia
Correspondence: Yazed AlRuthia
Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia
Tel +996 114677483
Fax +966 114677480
Email [email protected]
Background: The recent approval of innovative therapies for spinal muscular atrophy (SMA), such as nusinersen, has brought hope to patients and their families.
Objective: The aims of this study were to compare the characteristics and HRQoL of SMA patients treated with nusinersen and those treated with the standard of care.
Methods: This was a cross-sectional, interviewer-administered telephone questionnaire, which used a purposive sampling of SMA patients through a social support network. EuroQol five-dimensions-3-level (EQ-5D-3L) and the visual analog scale (VAS) have been used to assess the HRQoL. Different descriptive and inferential tests have been performed to compare the characteristics, EQ-5D responses, and mean scores of EQ-VAS between patients on nusinersen and the standard of care.
Results: Eleven out of 36 SMA patients (30.55%) have been treated with nusinersen. Patients with type I SMA represented 54% of those treated with nusinersen (P=0.012). Only 12.5% of SMA patients living in the Mecca region are treated with nusinersen in comparison to 50% of patients living in the Riyadh region (P=0.029). No difference was noticed in the proxy-responses for the five domains of the EQ-5D or the mean VAS scores for patients on nusinersen and the standard of care despite controlling for the SMA type and the ability to breathe independently (β= 1.39, 95% CI= – 5.15-7.93, P=0.667). However, the mean VAS score for patients who are unable to breathe independently was significantly lower than their counterparts who are able to breathe independently even after controlling for the SMA type and nusinersen treatment (β= – 31.61, 95% CI= – 51.59 - – 11.63, P=0.003).
Conclusion: The results of this study highlight the uncertainty about the impact of nusinersen on SMA patients’ HRQoL. Therefore, the impact of nusinersen on HRQoL should be examined using more robust study designs.
Keywords: spinal muscular atrophy, health-related quality of life, nusinersen, health services accessibility, Saudi Arabia
Introduction
Spinal muscular atrophy (SMA) is the second most common autosomal-recessive genetic disorder after cystic fibrosis, and refers to a range of disorders characterized by the degeneration of the anterior horn cells (α-motor neurons).1 The symptoms of SMA range from progressive muscle weakness to respiratory failure in the late stages.2 It is believed to be the second most common cause of death among children after cystic fibrosis.2,3 SMA is commonly categorized into four types based on the onset and course of the disease. Type I is the most common and progressive type of SMA and is usually diagnosed within the first six months of a child’s life, leading to frequent respiratory infections and death by the age of two years for those untreated. The second type is less progressive than type I and is usually diagnosed between the 6th and 18th months of the child’s age. On the other hand, the time of type III diagnosis, which is considered a milder form of SMA in comparison to types I and II, is variable from 18 months to early adulthood. The last and rarest type of SMA is type IV. This type of SMA is mostly diagnosed in the second or third decade of life, and patients usually have a normal life expectancy.3 Data show that inadequate production of survival motor neuron (SMN) protein, which is produced mainly by SMN1 gene and to a lesser degree by SMN2 gene on chromosome 5q, is responsible for most of the motor symptoms of SMA.4–6 Although the prevalence and incidence of this rare disease are largely unknown in many countries, especially in low and middle-income countries, they are estimated to be 1–2 per 100,000 persons and 1 in 10,000 live births, respectively.7
The management of SMA has been largely supportive, such as physical and respiratory therapies, aimed at relieving patients’ symptoms and improving the residual functions.8 However, the approval of nusinersen in December 2016 by the United States Food and Drug Administration (USFDA) has brought new hope in the treatment of SMA.9 Nusinersen is an antisense oligonucleotide that corrects the splicing of SMN2 exon 7, resulting in higher production of fully functional SMN protein, which theoretically leads to improvement in the motor symptoms of SMA.10 This drug is administered intrathecally four times over 64 days in the loading phase, followed by maintenance doses every four months, and has shown promising results in achieving motor milestone endpoints, such as sitting independently as assessed by the Hammersmith Infant Neurological Examination (HINE) after 12 months of follow-up, in several Phase II and Phase III trials.11–13 Moreover, multiple observational studies that assessed the impact of nusinersen on the motor function of SMA patients with type I who have been treated under the expanded access program in different countries have revealed encouraging results.14–16 Although most patients with SMA who have been treated with nusinersen have reported improvements in their motor function, these improvements were not significant among all age groups. In a recently published study that assessed the impact of nusinersen among seven adult SMA patients with types II and III in Germany who have been followed up for at least 10 months and used valid assessment scales, such as, the Hammersmith Functional Motor Scale Expanded (HFMSE) and the Revised Upper Limb Module (RULM), there was a reported improvement in the patients’ motor function; however, these changes did not reach statistical significance.17 Additionally, the high list price of this drug makes it not cost effective at various traditional cost effectiveness thresholds.18,19 Using the cost effectiveness threshold of €195,600 per Quality Adjusted Life Year (QALY), which is considered a reasonable threshold for rare diseases in Sweden, nusinersen was not found to be cost effective from the perspective of the health technology assessment body in Sweden, also known as the Dental and Pharmaceutical Benefits Agency. The study used a Markov health-state transition model utilizing data from ENDEAR and CHERISH phase III trials to examine the cost effectiveness of nusinersen for infantile-onset and later-onset SMA. The incremental cost effectiveness ratios were found to be €551,300 and €311,800 per QALY for the infantile-onset and later-onset SMA, respectively.18 In another economic evaluation study that explored the cost effectiveness of nusinersen in comparison to the best supportive care from the United States healthcare sector perspective, nusinersen was not found to be cost effective as well at a cost effectiveness threshold of $500,000 per QALY.19 Despite the high cost and outcome uncertainty, many healthcare systems have provided coverage for SMA patients who are eligible for nusinersen through different managed entry agreements.20–23
Another one-time injection highly expensive SMN1 gene replacement therapy was approved by the USFDA in May 2019.10 Onasemnogene abeparvovec has shown promising results,24 and received conditional approval by the European Commission for the management of SMA type I patients with bi-allelic mutation in SMN1 gene.10 In Saudi Arabia, rare diseases represent a huge financial challenge to the public healthcare sector, and SMA is one of the commonly encountered rare diseases.25 Only nusinersen has been approved so far in the management of SMA by the Saudi Food and Drug Authority (SFDA), and the drug is only administered in few tertiary care centers. Recently, a managed entry agreement that was established between the Saudi Ministry of Health (MOH) and nusinersen manufacturer, but the agreement did not come into effect yet and is expected to be launched soon.25 Nevertheless, no study has been published so far about the efficacy or cost effectiveness of this drug among the Saudi SMA patient population. Moreover, its impact on patient health-related quality of life (HRQoL) in real-world practice is largely unknown.26 Therefore, the aim of this study was to explore the impact of nusinersen on patient HRQoL and compare the characteristics of SMA patients who had received nusinersen in comparison to those who did not in Saudi Arabia.
Methods
Study Design and Data Collection
This was a proxy-reported questionnaire-based cross-sectional study whereby parents or caregivers of patients with a confirmed SMA diagnosis were interviewed over the phone by three healthcare professionals who were trained using the role-play method. The patients were identified through a social network of SMA patients that was established in 2016 by the parents of some SMA patients in Saudi Arabia. Parents and caregivers of SMA patients were approached by members of the network who informed them about the objectives of the study prior to the start of data collection that took place between May 16th and August 28th 2020. Only those with confirmed SMA diagnosis who consented to participate after explaining the purpose of the study and the right of the participants to withdraw at any time were contacted. Those who did not consent to participate were excluded. The date of SMA diagnosis, type of SMA, age, age at diagnosis, gender, and whether nusinersen was administered were retrieved from the patients’ medical records. Type of hospital where the patient was first diagnosed (eg, public or private), nationality (Saudi or non-Saudi), presence of comorbidities, place of residence, family monthly income, whether the patient is able to breathe and/or walk, whether the patient has any relatives with SMA, whether the parents or caregivers were told that the patient needs nusinersen by the treating neurologist, and whether any application was made by the parents/caregivers or on their behalf by the treating neurologist to receive nusinersen from the MOH or other public healthcare entities, such as the ministry of defense and aviation health affairs, were collected from the parents or caregivers over the phone in an interview that lasted approximately 15 minutes.
Patients’ Health-Related Quality of Life
In order to compare the health-related quality of life (HRQoL) for patients who were treated with nusinersen and their counterparts on the standard of care only (eg, respiratory support, nutritional support, airway clearance), the Arabic version of the EuroQol five-dimensions-3-level (EQ-5D-3L) questionnaire was used.27,28 This generic scale has been used in assessing the HRQoL of SMA patients before,26 therefore, it was used in this study to assess the HRQoL of SMA patients. It assesses five domains of HRQoL (mobility, self-care, usual activities, pain and discomfort, and depression and anxiety) with three possible responses (no problems, some problems, and confined to bed/unable/extreme problems).28 Moreover, the 20 centimeters EQ visual analog scale (VAS) with 0 to 100 end points where 0 corresponds to the worst health state and 100 corresponds to the best health state was used as well.27,28 Patients’ responses to EQ-5D-3L items were collected during the phone interviews, and the EQ-VAS was sent to the participants as a WhatsApp® message so they could view the scale and rate the health state of their SMA patients.
Ethical Considerations
All personal identifiers were removed from the collected data to protect patient privacy and confidentiality, and the study adhered to the ethical principles of the Helsinki’s declaration.29 The study was approved by the institutional review board in the College of Medicine at King Saud University, Riyadh, Saudi Arabia (Project No. E-19-4512).
Statistical Analyses
The sociodemographic and medical characteristics were compared between patients on nusinersen and those on the standard of care using Chi-square and Fisher’s exact tests as appropriate. EQ-5D-3-L domains’ responses were compared between patients on nusinersen and those on the standard of care using one-way ANOVA with Bonferroni correction. Student’s t-test and one-way ANOVA with Bonferroni correction were used to compare mean EQ-VAS scores across nusinersen use, age groups, gender, SMA types, ability to walk with assistance, ability to breathe independently (eg, without a ventilator), and presence of comorbidities. Multiple linear regression analysis was conducted to examine the impact of nusinersen on EQ-VAS score controlling for factors that have shown a significant association with the EQ-VAS score. The data were presented as means, standard deviations, frequencies, percentages, and box plots. Furthermore, beta coefficients with 95% confidence limits were used to present the results of multiple linear regression. The minimum sample size was estimated to be 35 patients for multiple linear regression with up to three predictors, α = 0.05, β = 0.2, power of 0.8, and a large effect size of Cohen’s F2 = 0.24. All the statistical analyses were conducted using SAS software, version 9.4 (SAS Institute Inc, Cary, NC, USA).
Results
Study Participants
A list of 63 patients who were diagnosed with SMA was received from the SMA social support network in Saudi Arabia; however, only 45 patients met the inclusion criteria, and 36 of them consented and participated in the study as shown in Figure 1. Eleven patients (30.55%) were treated with nusinersen for at least 12 months, and 72.72% (8/11) of them had been treated with nusinersen since 2018. On the other hand, 25 patients (69.44%) were treated with the standard of care. Most of the treated patients with nusinersen have type I SMA (54.54%). However, patients with type I SMA only represented 25% (9/36) of the total number of patients in comparison to patients with types II and III who represented 52.78% and 22.22% of the total number of recruited patients, respectively, (P=0.012). About 55% of the patients were females, 55.55% were under 10 years of age, 58.33% were diagnosed when they were under two years of age, 72% were diagnosed with SMA in public hospitals, and 97% were Saudis with no significant differences between patients treated with nusinersen and those treated with the standard of care. Approximately 73% of the patients (8/11) treated with nusinersen are living in the Riyadh region, which represents 50% of the SMA participants living in the Riyadh region; whereas only one out of eight patients (12.5%) living in the Mecca region were treated with nusinersen (P=0.02). The patients’ family incomes, ability to walk with assistance, ability to breathe independently, and other patients’ characteristics are shown in Table 1.
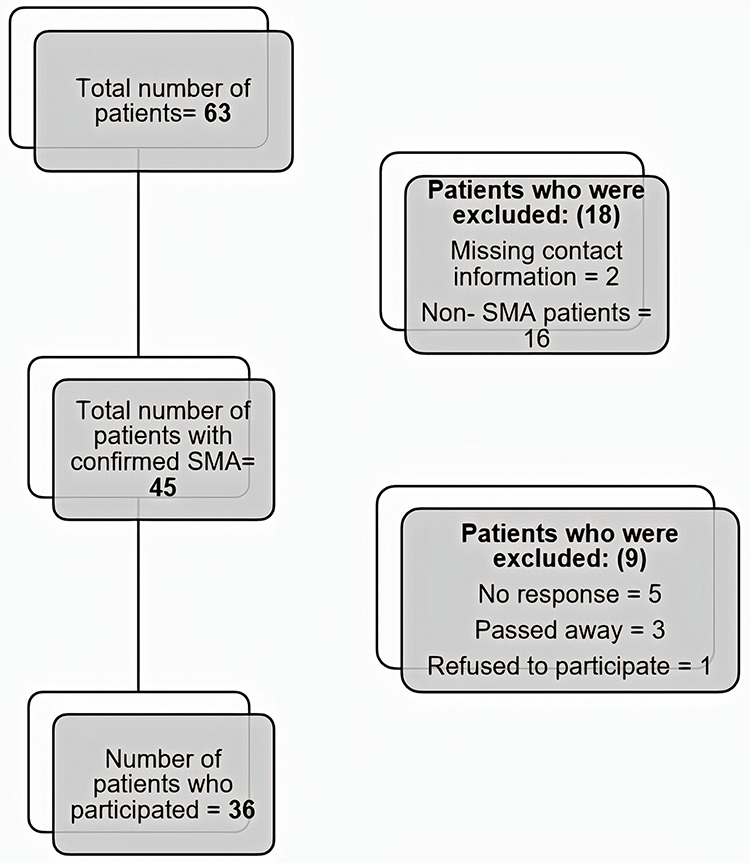 |
Figure 1 Patient recruitment scheme. |
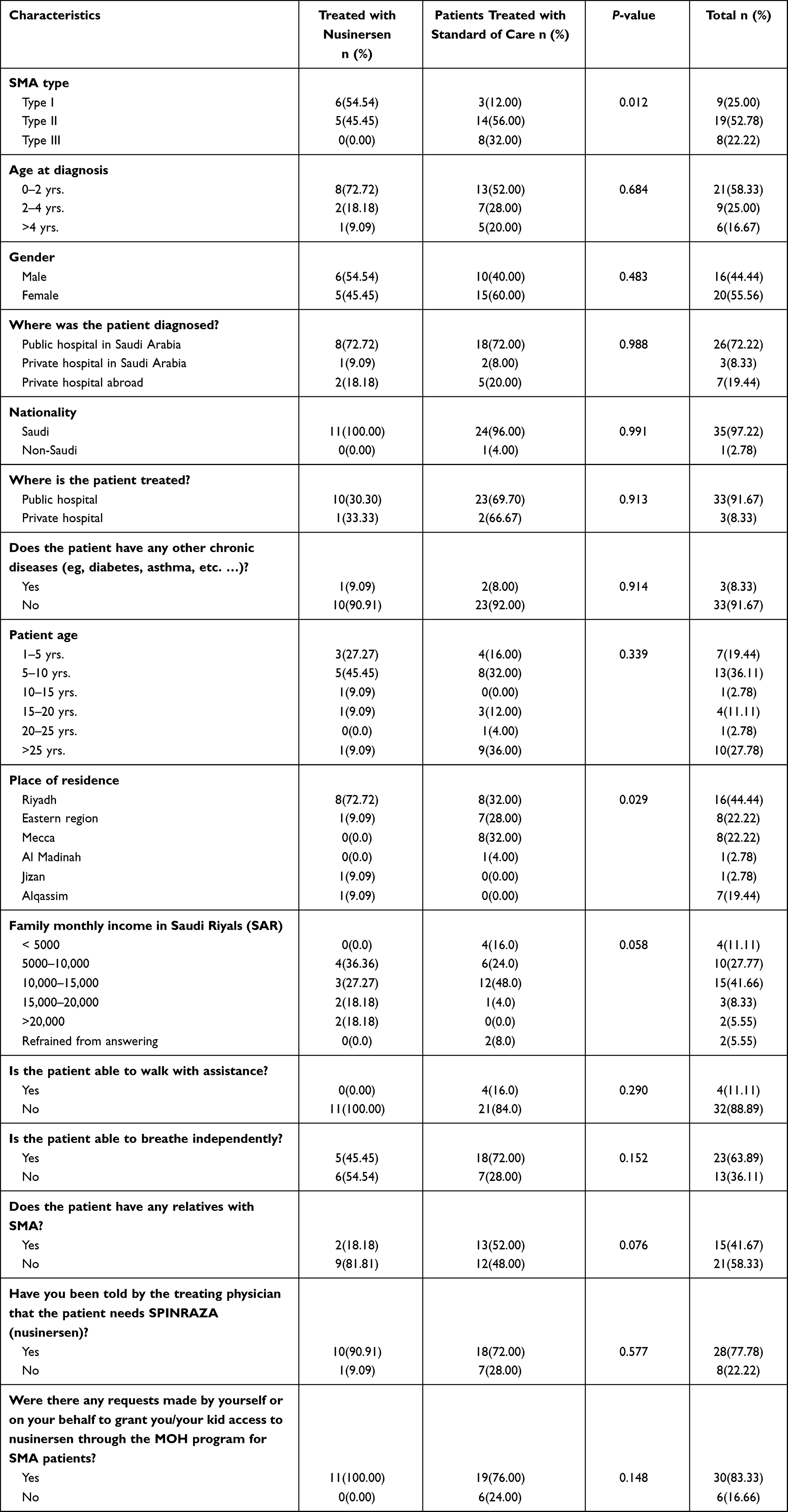 |
Table 1 Spinal Muscular Atrophy Patients’ Baseline Characteristics (N=36) |
EuroQol 5-Dimensions 3-Level (EQ-5D-3L)
The proxy-responses for the EQ-5D-3L five domains (mobility, self-care, usual activities, pain and discomfort, and depression and anxiety) for patients on nusinersen and those on the standard of care were not significantly different as shown in Table 2. More than two-thirds of participants reported extreme problems for the mobility and self-care domains. Furthermore, over two-thirds of participants reported some or extreme problems in both usual activities and pain and discomfort domains, while 80.5% of the patients reported no or some problems in the depression and anxiety domains.
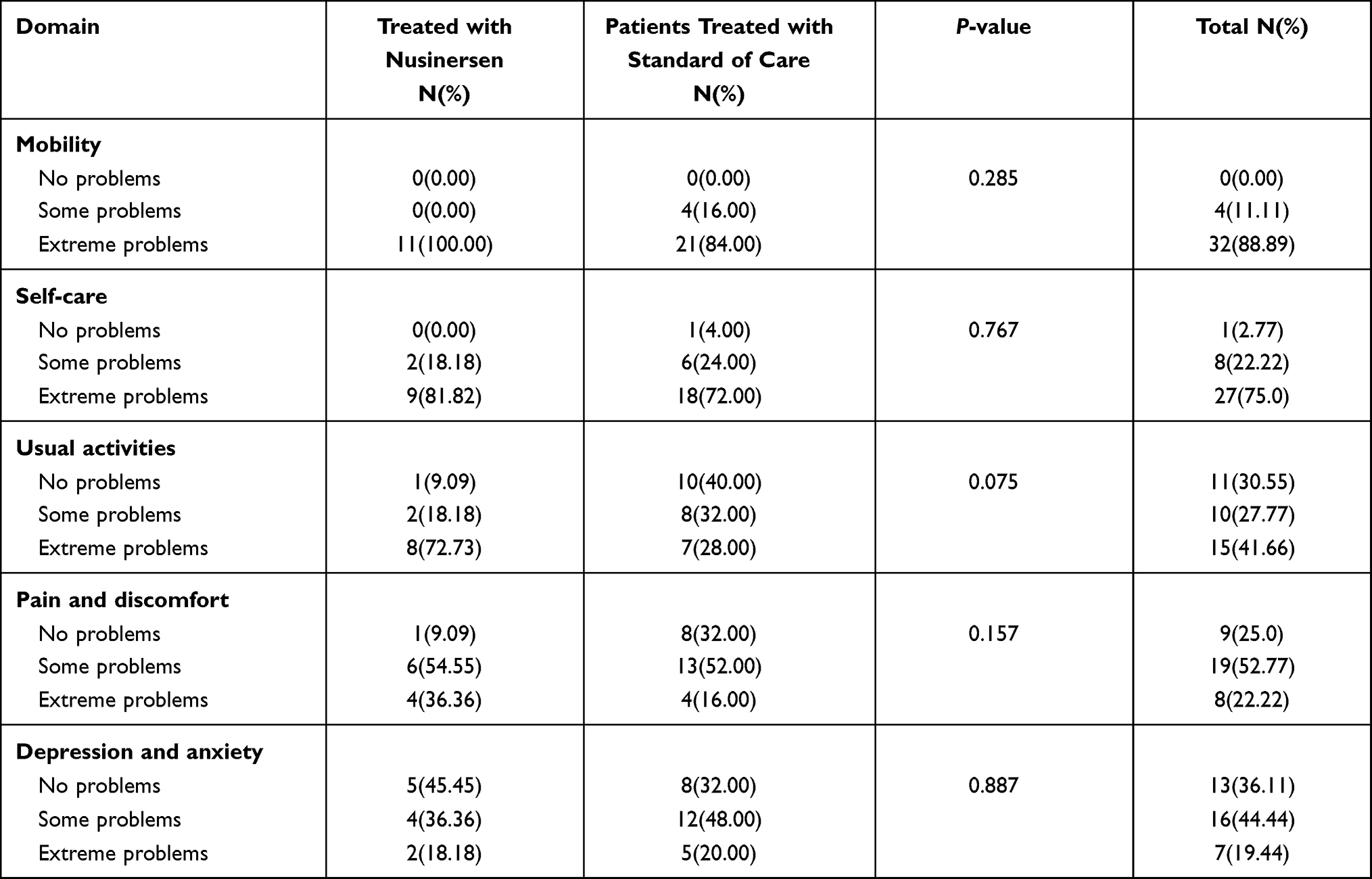 |
Table 2 Proxy Responses for Patients’ Health-Related Quality of Life (HRQoL) Using the EQ-5D-3L |
The mean EQ-VAS scores for patients on nusinersen and those treated with the standard of care are not significantly different as shown in Table 3. Moreover, no significant difference in the mean EQ-VAS scores across age groups, gender, ability to walk with assistance, and presence of comorbidities was found. The mean EQ-VAS score was the lowest for patients with SMA type I, followed by patients with type III, while patients with type II had the highest score (P=0.001). Patients who are able to breathe independently have higher mean EQ-VAS score in comparison to their counterparts who are unable to breathe independently (P<0.001). The EQ-VAS scores based on nusinersen use and across SMA types and ability to breathe independently are shown in Figures 2 and 3, respectively. Although patients on nusinersen had a higher likelihood than their counterparts on the standard of care only to have higher EQ-VAS scores, this was not statistically significant when controlling for both the type of SMA and ability to breathe independently (β=1.39, 95% CI= – 5.15–7.93, P=0.667). However, patients who were unable to breathe independently have a lower likelihood to have high EQ-VAS scores in comparison to their counterparts who were able to breathe independently controlling for nusinersen use and SMA type (β= –31.61, 95% CI= – 51.59- – 11.63, P=0.003; Table 4).
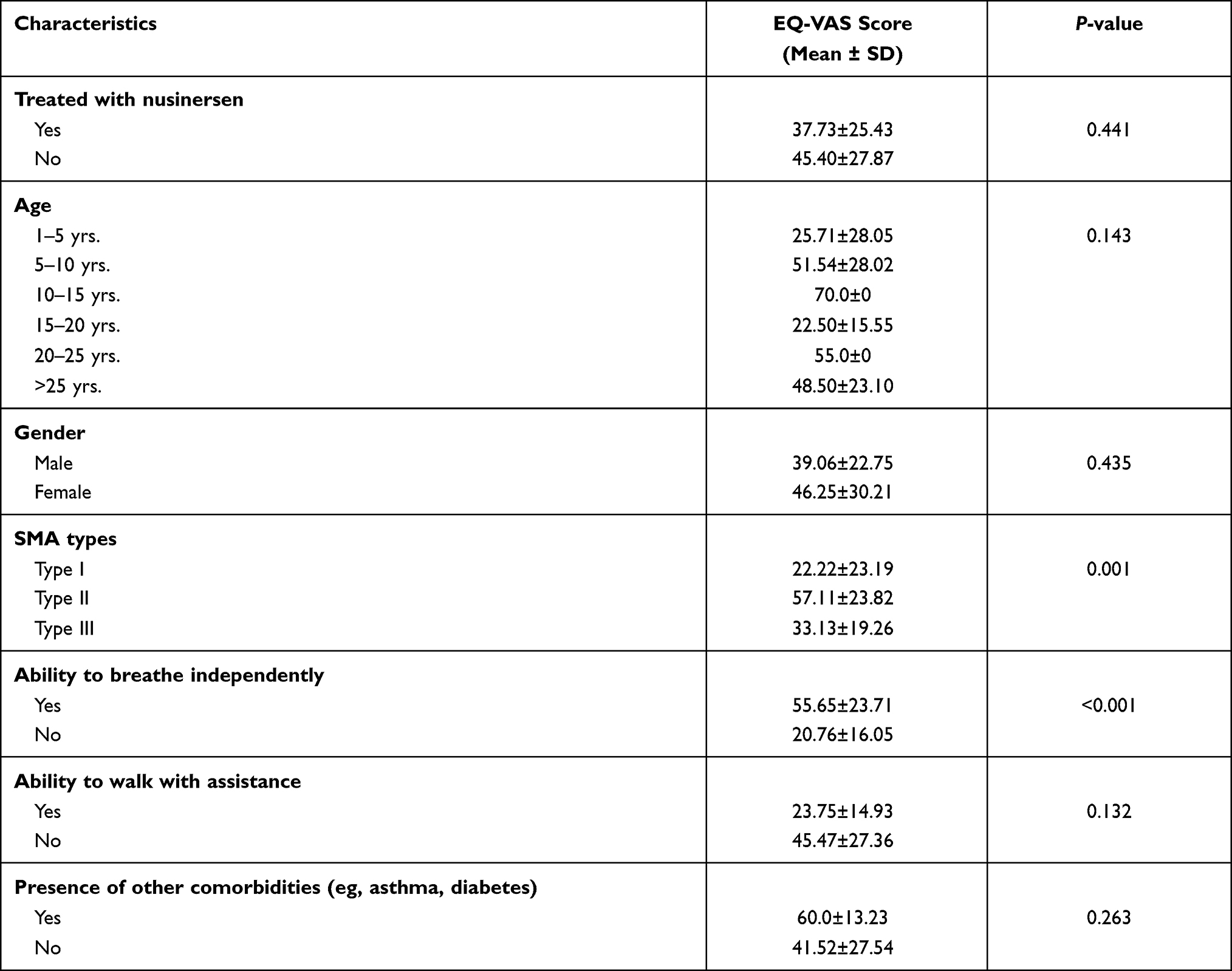 |
Table 3 The Mean EQ-VAS Score Across Nusinersen Use, Gender, Age Groups, SMA Types, Ability to Breathe Independently, Ability to Walk with Assistance, and Presence of Other Comorbidities |
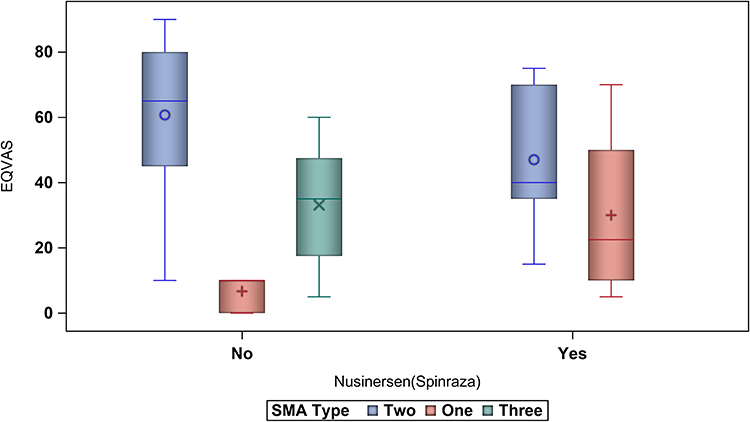 |
Figure 2 The boxplot of the VAS scores for patients on nusinersen versus standard of care across SMA types. |
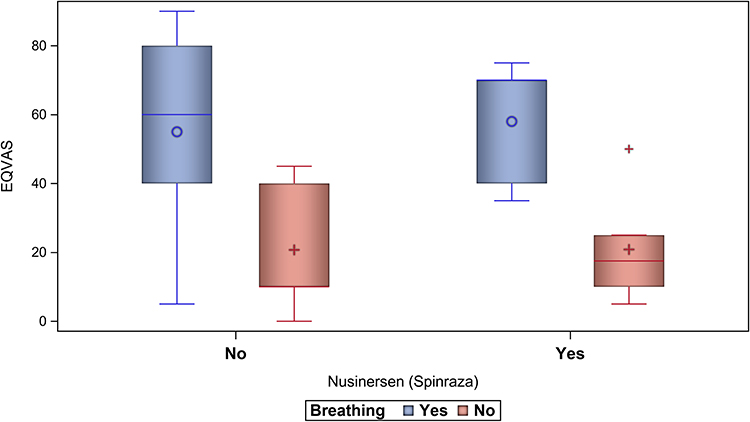 |
Figure 3 The boxplot of the VAS scores for patients on nusinersen versus standard of care across the patient ability to breathe independently (eg, use of ventilator). |
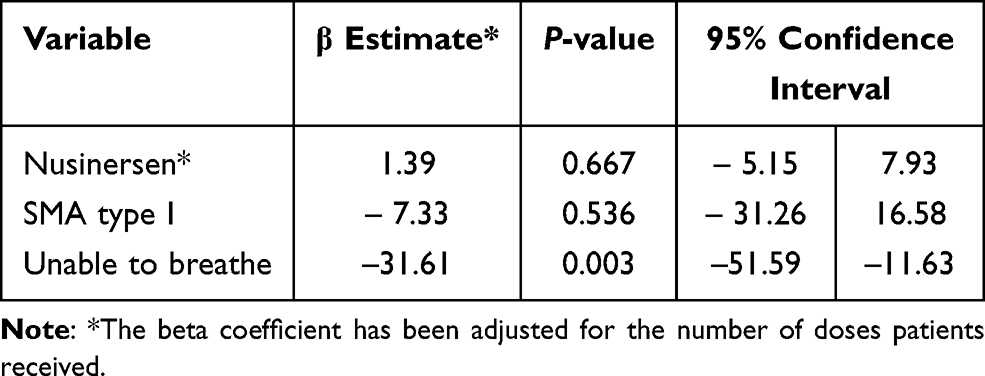 |
Table 4 Multiple Linear Regression for the Association Between the Administration of Nusinersen and the EQ-VAS Score |
Discussion
The highly expensive and innovative therapies that have been approved over the last three years have revolutionized the treatment of SMA.10 Although these new drugs, such as nusinersin and onasemnogene abeparvovec-xioi, and risdiplam, have been fully or conditionally approved by the USFDA and the European Medicines Agency, they have not been approved by other regulatory bodies in many countries especially in the low and middle-income countries.30 This creates variable access to innovative treatments for patients affected by this debilitating health condition. Despite the fact that nusinersin was approved by the SFDA in Saudi Arabia, many SMA patients have only been treated with the standard of care.25 Such a finding sheds light on the eligibility criteria that were used in granting access to therapy in different healthcare centers. For example, patients with SMA type I, which is the most severe form of the disease, had more access to nusinersen than patients with other types of SMA. However, some patients with type II SMA had access to nusinersen and not all patients with type I SMA had access to nusinersin. Furthermore, no difference was noticed among patients who were treated with nusinersen in comparison to those who were not in terms of their age, gender, nationality, type of hospital where the patient is being treated (public vs private), presence of comorbidities (eg, diabetes, asthma, etc ….), and ability to breathe or walk. Interestingly, only one SMA patient (12.5%) in the Mecca region was treated with nusinersen in comparison to 50% (8/16) of patients in the Riyadh region. Although this is a cross-sectional study with limited generalizability, these findings shed light on the inconsistent criteria that were set by different tertiary healthcare institutions in Saudi Arabia to assess the eligibility of SMA patients for nusinersen.
The proxy-responses for the five domains of the EQ-5D-3L, which assessed the HRQoL, were not significantly different between those treated with nusinersen and their counterparts treated with the standard of care. Similarly, patients treated with nusinersen did not have a significantly different mean EQ-VAS score in comparison to their counterparts who are treated with the standard of care only. The absence of any impact on EQ-VAS score remained even after controlling for type of SMA and the ability of patients to breathe independently. On the other hand, patients with SMA type I had the lowest mean EQ-VAS score in comparison to their counterparts with types II and III. This is consistent with a previously published study that confirmed a negative relationship between the most severe forms of SMA and patients’ quality of life.26,31 Furthermore, patients who are unable to breathe independently had a significantly lower mean EQ-VAS score in comparison to their counterparts who are able to breathe independently; this difference remained significant even after controlling for the type of SMA and the use of nusinersen. These findings, although they come from an observational cross-sectional study that used a generic scale to assess HRQoL, represent the first attempt at a national level to assess the impact of nusinersen as well as the different clinical characteristics on SMA patients’ HRQoL. In addition, little is known about the impact of different SMA disease phenotypes or the few available SMA treatments on patients’ HRQoL despite the fact that several studies have assessed the HRQoL of SMA patients using different scales.26 Thus, these findings highlight the importance of HRQoL in the assessment of any current or future innovative therapy for SMA or other rare diseases due to the high level of uncertainty about the value of these highly expensive drugs. There may be a statistically significant improvement of motor function; however, this slight increase may not be meaningful to the patients and their caregivers.31,32
Although this is the first study to the best of our knowledge to explore the factors that influence access to nusinersen among SMA patients in Saudi Arabia, multiple limitations must be acknowledged. This was a cross-sectional study that used a non-probability purposive sampling. Therefore, any causal relationship between the use of nusinersen and any of the EQ-5D domains or EQ-VAS score cannot be assessed. Furthermore, some sociodemographic and clinical characteristics as well as the HRQoL have been collected through an interviewer-administered questionnaire that involved proxy respondents, which increases the risk of acquiescence and information bias.33,34 Additionally, the motor function was not assessed or collected using a validated scale, such as the HFMSE and/or RULM.26–32 Moreover, the HRQoL was assessed using the EQ-5D, which is a non-disease specific scale that was used before in assessing HRQoL among SMA patients.26
Conclusions
The findings of this study highlight the uncertainty about the value of nusinersen in improving the HRQoL of SMA patients. SMA patients on nusinersen do not seem to have better HRQoL in comparison to their counterparts on the standard of care only. Therefore, the impact of nusinersen on HRQoL needs to be examined further using robust study designs and disease-specific scales to verify the impact of this innovative therapy on patients’ HRQoL. Moreover, disease phenotypes and geographic location seem to influence the utilization rate of this innovative therapy. Hopefully, the new risk sharing agreement which will take effect soon under the Saudi Ministry of Health will address these issues since a scientific committee is involved in assessing the eligibility of patients to nusinersen and monitoring the outcomes of the treatment upon which the reimbursement will be based.
Abbreviations
SMA, spinal muscular atrophy; SMN, survival motor neuron; USFDA, United States Food and Drug Administration; HINE, Hammersmith Infant Neurological Examination; HFMSE, Hammersmith Functional Motor Scale Expanded; RULM, Revised Upper Limb Module; QALY, Quality Adjusted Life Year; SFDA, Saudi Food and Drug Authority; HRQoL, health-related quality of life; EQ-5D-3L, EuroQol five-dimensions-3-level; VAS, visual analog scale; MOH, Ministry of Health.
Data Sharing Statement
Study data are available from the authors upon request from the corresponding author (Yazed AlRuthia).
Acknowledgment
The authors acknowledge financial support from the Deanship of Scientific Research at King Saud University, research group number [RG-1441-366].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kolb SJ, Kissel JT. Spinal muscular atrophy: a timely review. Arch Neurol. 2011;68(8):979. doi:10.1001/archneurol.2011.74
2. Tisdale S, Pellizzoni L. Disease mechanisms and therapeutic approaches in spinal muscular atrophy. J Neurosci. 2015;35(23):8691. doi:10.1523/JNEUROSCI.0417-15.2015
3. Oskoui MDB, DeVivo DC. Chapter 1. In: Sumner CJ, Paushkin S, Ko CP, editors. Spinal Muscular Atrophy: Disease Mechanisms and Therapy. London: Academic Press; Elsevier; 2017:3-17.
4. Lefebvre S, Bürglen L, Reboullet S, et al. Identification and characterization of a spinal muscular atrophy-determining gene. Cell. 1995;80(1):155–165. doi:10.1016/0092-8674(95)90460-3
5. Matthew DM, John WH, Audrey CP, et al. Molecular analysis of spinal muscular atrophy and modification of the phenotype by SMN2. Genet Med. 2002;4(1):20. doi:10.1097/00125817-200201000-00004
6. Lunn MR, Wang CH. Spinal muscular atrophy. Lancet. 2008;371(9630):2120–2133. doi:10.1016/S0140-6736(08)60921-6
7. Verhaart IE, Robertson A, Wilson IJ, et al. Prevalence, incidence and carrier frequency of 5q–linked spinal muscular atrophy–a literature review. Orphanet J Rare Dis. 2017;12(1):1–5. doi:10.1186/s13023-017-0671-8
8. Oskoui M, Darras BT, De Vivo DC. Spinal muscular atrophy: 125 years later and on the verge of a cure. In: Sumner CJ, Paushkin S, Ko C-P, editors. Spinal Muscular Atrophy: Disease Mechanisms and Therapy. San Diego, CA: Academic Press; 2017:3–19.
9. Singh NN, Howell MD, Androphy EJ, Singh RN. How the discovery of Iss-N1 led to the first medical therapy for spinal muscular atrophy. Gene Ther. 2017;24(9):520–526. doi:10.1038/gt.2017.34
10. Messina S, Sframeli M. New treatments in spinal muscular atrophy: positive results and new challenges. J Clin Med. 2020;9(7):2222. doi:10.3390/jcm9072222
11. Finkel RS, Chiriboga CA, Vajsar J, et al. Treatment of infantile-onset spinal muscular atrophy with nusinersen: a Phase 2, open-label, dose-escalation study. Lancet Lond Engl. 2016;388:3017–3026. doi:10.1016/S0140-6736(16)31408-8
12. Finkel RS, Mercuri E, Darras BT, et al. Nusinersen versus sham control in infantile-onset spinal muscular atrophy. N Engl J Med. 2017;377:1723–1732. doi:10.1056/NEJMoa1702752
13. Mercuri E, Darras BT, Chiriboga CA, et al. Nusinersen versus sham control in later-onset spinal muscular atrophy. N Engl J Med. 2018;378:625–635. doi:10.1056/NEJMoa1710504
14. Pechmann A, Langer T, Schorling D, et al. Evaluation of children with SMA type 1 under treatment with nusinersen within the expanded access program in Germany. J Neuromuscul Dis. 2018;5:135–143. doi:10.3233/JND-180315
15. Aragon-Gawinska K, Seferian AM, Daron A, et al. Nusinersen in patients older than 7 months with spinal muscular atrophy type 1: a cohort study. Neurology. 2018;91:1312–1318. doi:10.1212/WNL.0000000000006281
16. Pane M, Coratti G, Sansone VA, et al. Nusinersen in type 1 spinal muscular atrophy: twelve-month real-world data. Ann Neurol. 2019;86:443–451. doi:10.1002/ana.25533
17. Jochmann E, Steinbach R, Jochmann T, et al. Experiences from treating seven adult 5q spinal muscular atrophy patients with nusinersen. Ther Adv Neurol Disord. 2020;13:1756286420907803. doi:10.1177/1756286420907803
18. Zuluaga-Sanchez S, Teynor M, Knight C, et al. Cost effectiveness of nusinersen in the treatment of patients with infantile-onset and later-onset spinal muscular atrophy in Sweden. Pharmacoeconomics. 2019;37(6):845–865. doi:10.1007/s40273-019-00769-6
19. Thokala P, Stevenson M, Kumar VM, Ren S, Ellis AG, Chapman RH. Cost effectiveness of nusinersen for patients with infantile-onset spinal muscular atrophy in US. Cost Eff Resour Alloc. 2020;18(1):1–2. doi:10.1186/s12962-020-00234-8
20. Robertson D BIOGEN’S SPINRAZA®(nusinersen) receives recommendation from nice for the treatment of infants, children and adults with 5q spinal muscular atrophy. 2019.
21. Ali I, Gilchrist FJ, Carroll WD, et al. Healthcare utilisation in children with SMA type 1 treated with nusinersen: a single centre retrospective review. BMJ Paediatr Open. 2019;3(1):e000572. doi:10.1136/bmjpo-2019-000572
22. Kamusheva MS, Dimitrova MJ. Clinical and economic assessment of nusinersen: the bulgarian perspective. Expert Opin Orphan Drugs. 2020;8(10):403–415. doi:10.1080/21678707.2020.1835641
23. Ecker T, Leismann J. PBI31 managed entry agreements for ATMPs despite access already granted? The case of Germany. Value Health. 2020;23:S19. doi:10.1016/j.jval.2020.04.095
24. Day JW, Chiriboga CA, Crawford TO, et al. Onasemnogene abeparvovec-xioi gene-replacement therapy for spinal muscular atrophy type 1 (SMA1): phase 3 US study (STR1VE) update (1828). 2020.
25. Alsaqa’aby MF, Ibrahim N. An overview about rare diseases in Saudi Arabia and reimbursement of orphan drugs. Glob J Med Therap. 2019;1(2):8–13.
26. Landfeldt E, Edström J, Sejersen T, Tulinius M, Lochmüller H, Kirschner J. Quality of life of patients with spinal muscular atrophy: a systematic review. Eur J Paediatr Neurol. 2019;23(3):347–356. doi:10.1016/j.ejpn.2019.03.004
27. Whynes DK. Correspondence between EQ-5D health state classifications and EQ VAS scores. Health Qual Life Outcomes. 2008;6:94. doi:10.1186/1477-7525-6-94
28. Aburuz S, Bulatova N, Twalbeh M, et al. The validity and reliability of the Arabic version of the EQ-5D: a study from Jordan. Ann Saudi Med. 2009;29(4):304–308. doi:10.4103/0256-4947.55313
29. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
30. Lucas F. Improving market access to rare disease therapies: a worldwide perspective with recommendations to the industry. Med Access Point Care. 2018;2:2399202618810121. doi:10.1177/2399202618810121
31. Belter L, Cruz R, Jarecki J. Quality of life data for individuals affected by spinal muscular atrophy: a baseline dataset from the Cure SMA community update survey. Orphanet J Rare Dis. 2020;15(1):1. doi:10.1186/s13023-020-01498-2
32. Audic F, de la Banda MG, Bernoux D, et al. Effects of nusinersen after one year of treatment in 123 children with SMA type 1 or 2: a French real-life observational study. Orphanet J Rare Dis. 2020;15(1):1. doi:10.1186/s13023-020-01414-8
33. Jones TL, Baxter MA, Khanduja V. A quick guide to survey research. Ann R Coll Surg Engl. 2013;95(1):5–7. doi:10.1308/003588413X13511609956372
34. Bowling A. Mode of questionnaire administration can have serious effects on data quality. J Public Health (Bangkok). 2005;27(3):281–291. doi:10.1093/pubmed/fdi031
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.