Back to Journals » International Journal of Women's Health » Volume 17
Protocol-Specific Outcomes of GnRH Agonist Use in Luteal Phase Support During Frozen Embryo Transfer Cycles
Authors Salame A ![]() , Dahdouh EM, Zhaffal M, Al Jafari R, Muraleekrishnan A, Bajpai A, Kainoth S, Koodathingal BP, Samuel D, Depret-Bixio L, Fakih M
, Dahdouh EM, Zhaffal M, Al Jafari R, Muraleekrishnan A, Bajpai A, Kainoth S, Koodathingal BP, Samuel D, Depret-Bixio L, Fakih M
Received 21 March 2025
Accepted for publication 27 September 2025
Published 3 October 2025 Volume 2025:17 Pages 3445—3453
DOI https://doi.org/10.2147/IJWH.S529614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Anastasia Salame,1 Elias M Dahdouh,2 Mokhamad Zhaffal,3 Rania Al Jafari,1 Arya Muraleekrishnan,1 Aparna Bajpai,1 Shabin Kainoth,1 Bhavya Puliyali Koodathingal,1 David Samuel,1 Leyla Depret-Bixio,1 Michael Fakih1
1Reproductive Endocrinology and Infertility, Fakih Fertility Centre, Al Ain, United Arab Emirates; 2Department of Obstetrics and Gynecology, Université de Montréal, Montreal, QC, Canada; 3Obstetrics and Gynecology Department, Oasis Hospital, Al Ain, United Arab Emirates
Correspondence: Anastasia Salame, Reproductive Endocrinology and Infertility, Fakih Fertility Centre, Al Markhaniyyah Abu Dhabi, Al Ain, United Arab Emirates, Tel +971543996368, Email [email protected]
Purpose: Recent data comparing natural cycles and artificial cycles in frozen embryo transfer (FET) showed an equivalent LBR when optimized luteal phase support (LPS) was used. Of the suggested methods is the use of GnRH agonists as part of LPS. We aim to study whether the addition of GnRH agonists as LPS in FET cycles increases the live birth rate (LBR) and decreases the miscarriage rate (MR).
Methods: A retrospective analysis was performed for 140 FET cycles, which were divided into two groups. The study group in which a GnRH agonist was used (AG) at the time of embryo transfer included 66 cycles, whereas the control group (NAG) included 74 cycles in which the use of GnRH agonist was not described.
Results: The implantation rate was greater in the AG (69/112 (61.6%) vs 60/124 (48.4%), p= 0.0413). The LBR was greater in the AG than in the CG but did not reach statistical significance (40/66 (60.6%) vs 35/74 (47.3%), p= 0.114). The MR was similar between the 2 groups (6/66 (10%) vs 5/74 (6.7%), p= 0.61). The subanalysis per FET protocol revealed that there was no difference in the LBR between the AG-medicated and NAG-medicated cycles (15/34 (44.62%) vs (36/65 (55.38%), p=0.1984) or between the AG-ovulation induction and NAG-ovulation induction FET cycles (21/32 (65.63%) vs 6/9 (66.67%), p=0.1985).
Conclusion: The use of a GnRH agonist as an add-on for LPS in FET cycles numerically increased the LBR without reaching statistical significance despite significantly improving the implantation rate. MR were not affected. This potential beneficial effect was comparable between the artificial and ovulation-induction FET cycles.
Keywords: GnRH agonist, frozen embryo transfer, live birth rate, luteal support, progesterone, miscarriage rate
Introduction
Infertility is described as the inability to conceive despite having regular unprotected intercourse. It is estimated to affect at least 15% of the world’s population. Of the proposed interventions to help the couple conceive is assisted reproductive technologies (ART).1 It has been estimated that in 2018, ART resulted in the birth of 670,000 infants.2 Initially, fresh embryo transfers were the gold standard however with the advent of cryopreservation, the use of frozen embryo transfers (FETs) has been increasing.2 There is a continuous search, however, to find the optimal protocol that would increase the live birth rate (LBR) and decrease the miscarriage rate (MR), especially in the setting of medicated FET. Multiple reports have shown the superiority of natural FET cycles over medicated artificial cycles, especially in terms of pregnancy loss.3,4 However, a recent retrospective study comparing natural cycles and artificial cycles in FET showed an equivalent LBR when optimized luteal phase support (LPS) was used with intramuscular progesterone alone or in combination with vaginal progesterone.5 Hence, finding the optimal LPS in FET cycles is crucial for maximizing reproductive outcomes. One of the suggested methods is the use of GnRH agonists as part of LPS. Initially, the use of the GnRH agonist was investigated in fresh embryo transfer cycles with reassuring results. Multiple meta-analyses have shown that the administration of such medications during the peri-implantation period increases the LBR.6,7 Later, the use of GnRH agonists was advocated for intrauterine insemination (IUI) cycles and even FET cycles. A study by Leppänen et al revealed that the benefit of the GnRH agonist when it is administered at the time of implantation in IUI cycles depends on the nature of the ovulation induction protocol used.8 To date, the effect of GnRH agonist administration has been studied in medicated cycles, also known as hormone replacement therapy (HRT) FET cycles. There are contradictory data concerning the benefit of GnRH agonist administration in FET cycles. While multiple studies have documented the benefit of LBR, other studies have shown no clear benefit despite reporting a lower miscarriage rate in the group receiving the GnRH agonist as part of luteal support.9–11 There is no consensus on the ideal time of GnRH agonist administration or the optimal dose of LPS; hence, there is a possible explanation for the variability in the results documented by different studies. The majority of the data available convey the use of one dose of GnRH agonist at the time of embryo transfer.7,10 The exact mechanism of action of GnRH agonists is not fully understood. It is speculated that this medication might be involved in corpus luteum rescue through endogenous LH secretion or through direct action on the receptors available in the endometrium or on the embryo.11,12 In theory, GnRH agonist administration during the peri-implantation period leads to increased endogenous LH levels 3–4 days prior to downregulation. This LH surge increases corpus luteum (CL) support and increases progesterone output, hence resulting in better luteal phase support. Increased levels of circulating steroids aid in the implantation process and hence the secretion of detectable serum hCG, which in turn will support the corpus CL.13 This is important in the setting of fresh embryo transfers since supraphysiologic estrogen levels during stimulation lead to luteal phase dysfunction and poor CL function. The effects of GnRH agonist administration, however, are most likely not limited to only the pituitary gland, as evidenced by the improved pregnancy rates, even in fresh GnRH agonist cycles.6 It remains questionable whether the same applies during ovulation induction (OI) or natural FET cycles since the estrogen levels are almost always within the physiologic ranges. To date, no studies have compared the addition of a GnRH agonist to LPS in different FET protocols.
Owing to the paucity of data on how to improve the LPS in FET, we conducted this study to evaluate the effect of GnRH agonist (Gonapeptyl-Triptorelin) administration in different FET protocols, namely, medicated FET and OI, which are known as modified natural FET protocols using aromatase inhibitors (letrozole). The choice of the GnRH agonist was based on the availability of the drug as well as the fact that many of the published studies discussed the effect of triptorelin as part of LPS. Our primary outcomes were the LBR, pregnancy rate, and miscarriage rate in FET cycles with and without the addition of the GnRH agonist. Our secondary aim was to study the effect of the addition of a GnRH agonist at the time of embryo transfer in OI cycles.
Data and Methods
A retrospective cohort analysis was performed in a private practice in the United Arab Emirates during the period between December 1, 2018, and December 31, 2020. The charts reviewed resulted in 140 FETs of euploid embryos, 66 of which were found to describe the use of a GnRH agonist at the time of ET referred to as the agonist group (AG). The remaining cycles did not describe the use of a GnRH agonist at the time of ET referred to as to non- agonist group (NAG), accounting for 74 cycles. The use of a GnRH agonist as an add-on was implemented as of January 2020 in an attempt to improve the reproductive outcomes of FET cycles. To note that during the mentioned duration, there was no change in the medical staff or the laboratory personnel.
Demographic data were compared for both groups. Cycle characteristics, number of embryos transferred, endometrial thickness, and implantation rates were compared. The primary outcome of our study was the live birth rate, whereas the secondary outcomes included pregnancy rates and miscarriage rates. A subanalysis was performed per the FET protocol.
The study was approved by the research ethical committee (REC) of the fertility center where the study was performed which is Fakih Fertility Clinic. The study was conducted in accordance with the Declaration of Helsinki.
Description of Treatment Cycles and Genetic Testing
The patients underwent PGT-A for advanced reproductive age (ARA), severe male factor, consanguinity, recurrent pregnancy loss (RPL), recurrent implantation failure (RIF), sex selection, and personal choice.14 The controlled ovarian stimulation protocol used was the antagonist protocol. The type and dose of gonadotropins used were selected on the basis of the baseline hormonal profile, antral follicular count, and ovarian response to stimulation. The type and dose of ovulation trigger depended on the number of follicles on the trigger day and the estrogen level. The embryo biopsy procedure was performed on the basis of the facility’s internally validated standard of procedure (SOP). The detailed process of embryo biopsy and genetic testing has already been described in previous publications.15,16 The grading of the embryos on the day of the biopsy was based on the grading system adopted by Capalbo et al.17
The FET cycle protocols used were either OI cycles or medicated cycles using hormone replacement therapy (HRT), also known as artificial cycles or programmed cycles. Medicated cycles were used with anovulatory patients and patients who live far away and are unable to present frequently to the clinic.
In the medicated cycles, after the patient presented on her second day of the period, baseline blood tests were performed, and estradiol valerate (Progyluton®, only white pills) 6 mg daily was started. The patient was followed on cycle days 10 and 14. The dose of Progyluton was adjusted on the basis of the thickness of the endometrium. When the endometrial thickness reached at least 7 mm, 8% vaginal progesterone gel (Crinone®) was started twice daily. The embryo transfer was performed on the 6th day of progesterone supplementation. In OI cycles, patients were started on letrozole (Letara®) 2.5 mg twice daily for 5 days. The patient was then seen on cycle day 10. If a leading follicle was observed, the patient was seen on alternating days until the follicle reached at least 17 mm, the endometrial lining was 7 mm, and the estrogen level was 150 pg/mL. Ovulation was then triggered with 250 mcg recombinant hCG (Ovitrelle®) in the evening. Embryo transfer was performed on trigger +7 days. When triptorelin (Gonapeptyl®) was used, 0.1 mg was given subcutaneously on the embryo transfer day. Quantitative hCG was performed 7 days after embryo transfer. A transvaginal ultrasound was used to document an intrauterine gestational sac, and the fetal heart was evaluated 2 weeks after a positive pregnancy test.
Statistical Analysis
Continuous variables are expressed as the means ± standard deviations (SDs), and categorical variables are expressed as numbers and frequencies (percentages). Statistical differences between groups were estimated via the chi-square test or Fisher test according to the number of observations for categorical variables.
The genmode procedure was used to test the difference for continuous variables. GEE (generalized estimating equation) was applied to calculate the estimates by accounting for the fact that each patient could have more than one embryo.
Factors associated with the use of Gonapeptyl (yes vs no), which was significant at the 0.05% threshold in the univariate analysis, were included in the multivariate analysis to determine whether the use of Gonapeptyl was a predictive factor for implantation, clinical pregnancy, miscarriage, chemical pregnancy, and live birth rates. A logistic regression model was used to identify the predictive factors. Odds ratios and 95% confidence intervals (ORs [95% CIs]) were calculated for each analysis; forest plot figures were generated for easy interpretation. Bonferroni correction was used to avoid a type I error. All analyses were performed via SAS Studio (SAS® Studio). There were no missing values for any of the collected variables that were analyzed. A two-sided P value of 0.05 was considered statistically significant.
Results
Demographical Data
The mean male age was greater in the NAG (36.1 vs 32.9, p= 0.024); however, the mean female age was the same between the 2 groups (30.7 vs 31.7, p=0.338). The duration of infertility was longer in the AG than in the NAG (3.7 vs 2, p= 0.003). The demographic data of the 2 groups are presented in Table 1.
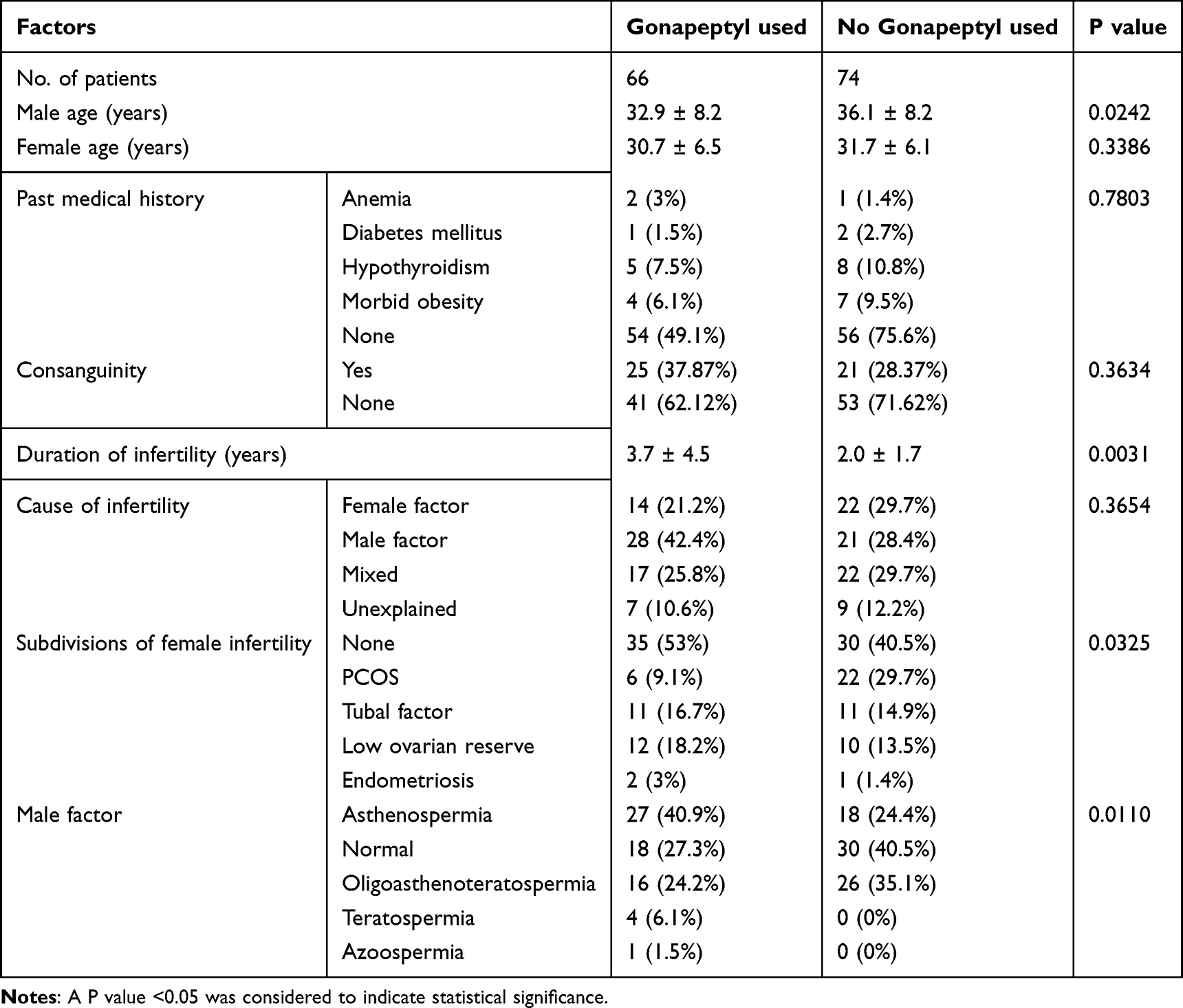 |
Table 1 Demographic Data of Both Groups |
FET Cycle Characteristics
Among the AGs, 32 (51.5%) were medicated in FET cycles, whereas 65 (87.8%) were medicated in NAG cycles. OI FET cycles were present mainly in the AG (32 (78%) vs 9(21.9%), p<0.0001). The FET cycle characteristics are presented in Table 2. Excellent embryos were transferred in 62 (61.38%) of the patients in the AG group compared with 50 (43.1%) in the NAG group (p= 0.0267). Embryos with trophectoderm (TE) grade A were transferred more commonly in the AG than in the NAG (69 (68.31%) vs 57 (49.14%), p= 0.0043).
 |
Table 2 FET Cycle Characteristics of AG# Vs NAG% |
The Embryo Characteristics and Reproductive Outcomes
The embryo characteristics of both groups are presented in Table 3. The implantation rate was greater in the AG (69/112 (61.6%) vs 60/124 (48.4%), p= 0.0413). The PR and LBR were numerically greater in the AG but did not reach statistical significance (51/66 (77.2%) vs.49/74 (66.2%), p= 0.147 and (40/66 (60.6) % vs 35/74 (47.3%), p= 0.114). Interestingly, the miscarriage rate was similar between the 2 groups (6/66 (10%) vs 5/74 (6.7%), p= 0.61). The reproductive outcomes of both groups are presented in Table 4. Given that (41/140)29.2% of the FET cycles were OIs and that most of them were in the AG group, we decided to perform further subanalysis to determine whether the effect of the GnRH agonist depended on the FET protocol used. The PR rate was comparable between the AG-OI FET and AG-medicated FET cycles (23/32 (71.88%) vs 28/34 (82.35%), p= 0.31). The PRs in the AG-OI FET and NAG-OI FET cycles were also similar (23/32 (71.88%) vs 7/9 (77.7%), p= 0.3021). The MR was similar between the AG-medicated and AG-OI FET cycles (5/34 (14.7%) vs 1/32 (3.13%), p= 0.19). There was no difference in the LBR between the AG-medicated and NAG-medicated cycles (19/34 (55.38%) vs 29/65 (44.62%), p=0.1984) or between the AG-OI and NAG-OI FET cycles (21/32 (65.63%) vs 6/9 (66.67%), p=0.19536). The PR, MR, and LBR with respect to the FET protocol used and the presence or absence of the agonist add-on are presented in Figure 1. A regression analysis was performed to detect the actual predictors of pregnancy in our study. The only significant predictor was the grade of the embryo transferred, especially when the good versus the average embryo was compared, with an OR of 0.096 (95% CI (0.016–0.57), p= 0.009). The FET protocol, whether medicated or OI, was not found to be a significant predictor, with an OR of 2.23 (95% CI (0.58–8.5), p= 0.239). The results of the regression analysis are presented in Table 5.
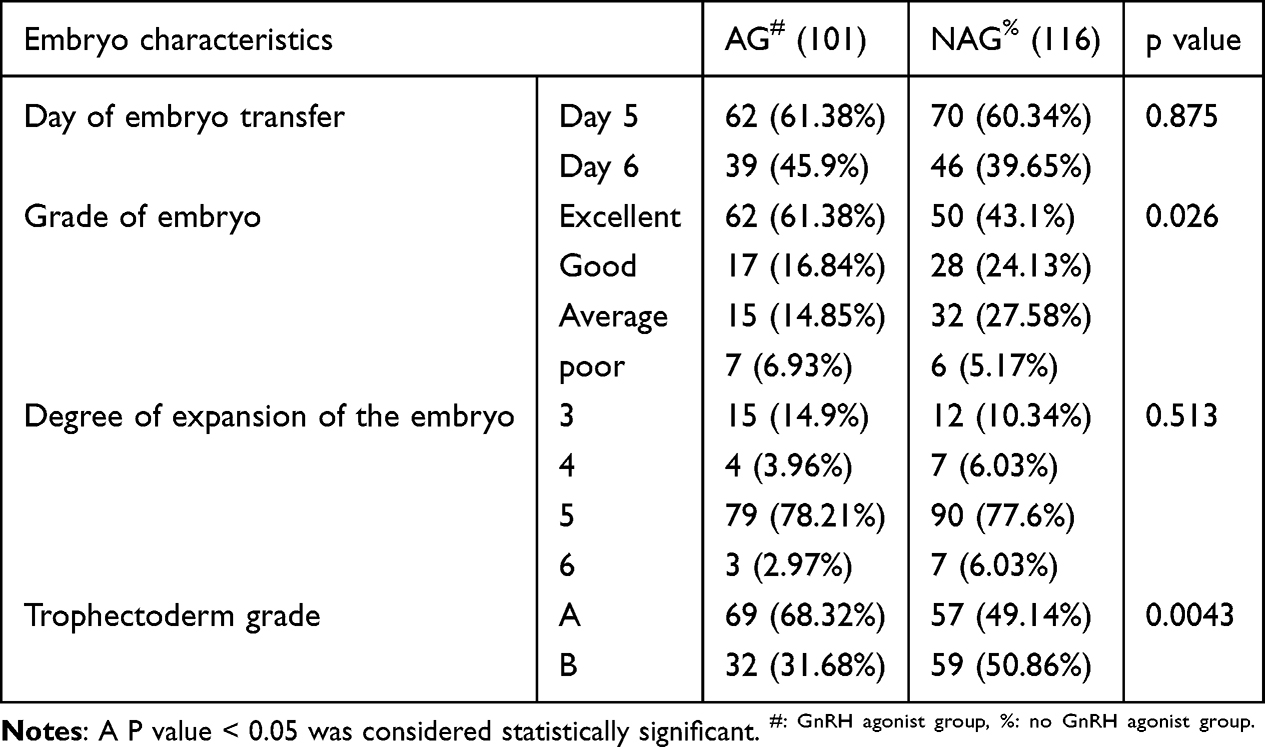 |
Table 3 Characteristics of Embryos Transferred in the AG Vs the NAG |
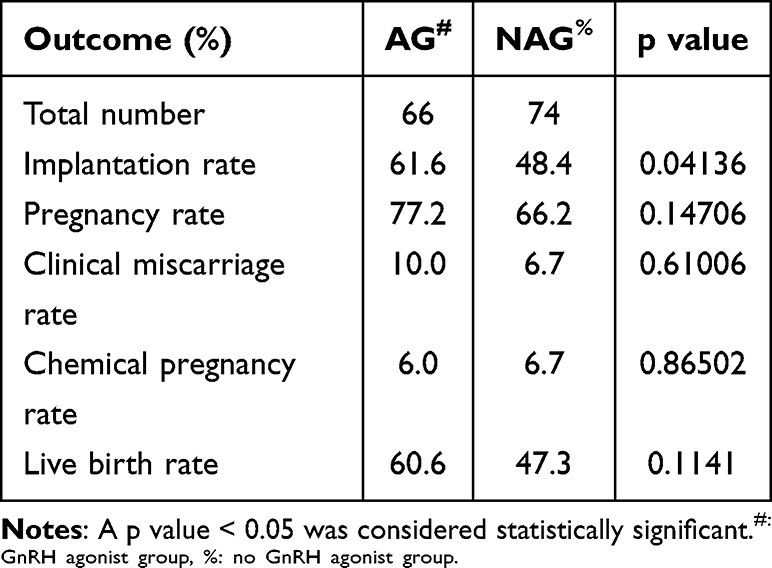 |
Table 4 Reproductive Outcomes of Both Groups |
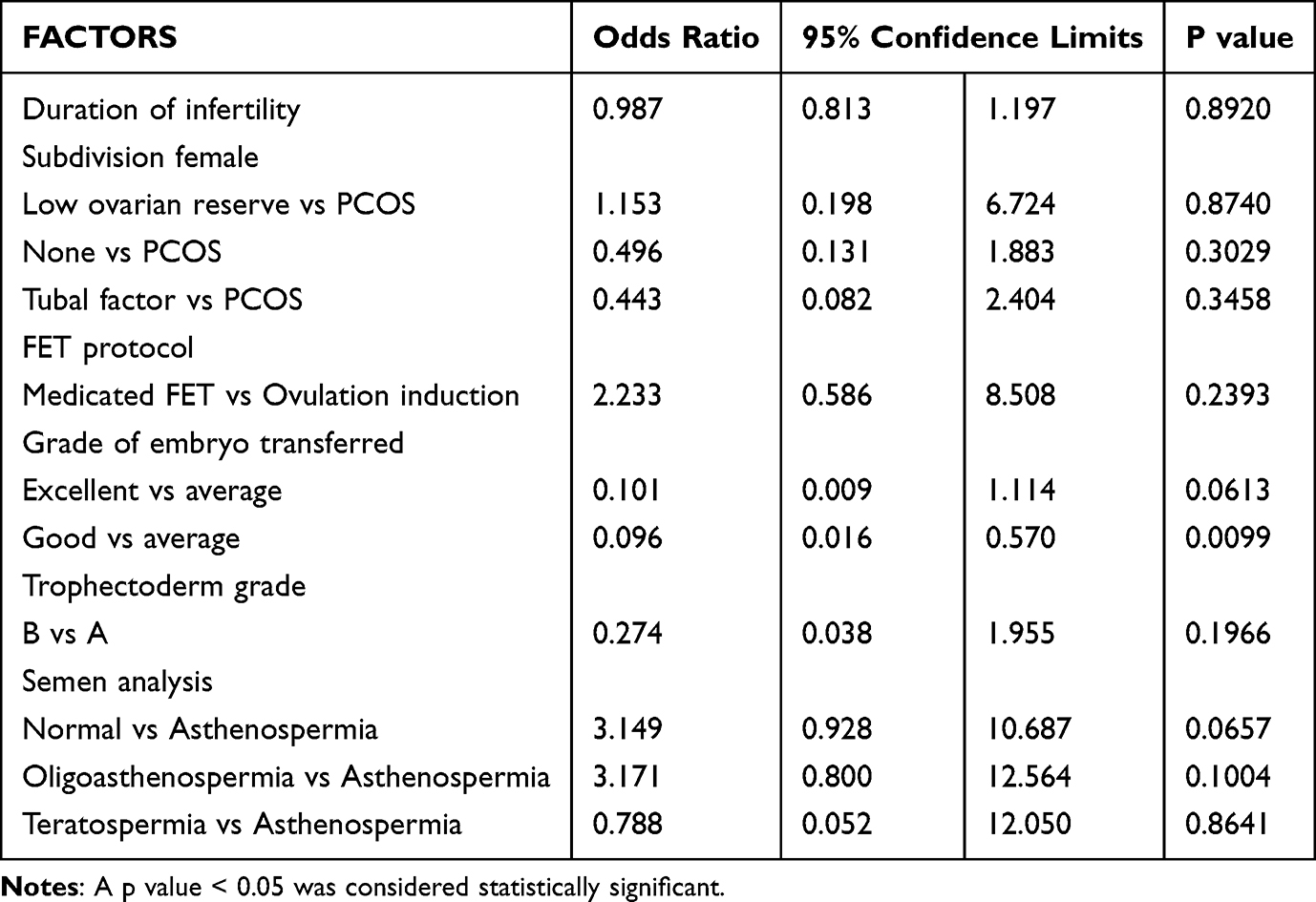 |
Table 5 Multivariate Regression Analysis: Predictors of Pregnancy |
 |
Figure 1 Reproductive outcomes per FET cycle based on different FET protocols and the use of a GnRH agonist as an add-on. |
Discussion
Our analysis revealed that the addition of a GnRH agonist in the form of 0.1 mg Gonapeptyl at the time of embryo transfer to genetically euploid embryos did not significantly improve the reproductive outcomes of the FET cycles despite a significant increase in the implantation rate in the AG (61.6% vs 48.4%, p= 0.041). Similarly, the effect is nonsignificant whether a medicated FET cycle or an OI FET cycle is used. The PR rate was similar between the medicated and OI FET cycles, irrespective of whether a GnRH agonist was used (p= 0.319). The values are presented in Figure 1. The MR was also not affected despite a nonsignificantly higher rate of miscarriages in the AG-medicated cycles (p= 0.348). The LBR was also similar between the different treatment groups (p= 0.209). The theory of GnRH agonist addition to FET cycles and specifically to OI was based on the possible effect not only on the CL through the endogenous LH surge but also on the receptivity of the endometrium per se and possibly the embryo. The presence of agonist receptors has been documented in the endometrium for some time. The activation of those receptors through GnRH agonist binding leads to the activation of signaling cascades (urokinase-type plasminogen activator and matrix metalloproteinase systems) that affect trophoblast invasion and the implantation process.18 Studies have suggested increased expression of endometrial GnRH agonist receptors in the luteal phase of the menstrual cycle. The presence of the receptors on the placental cytotrophoblasts and syncytiotrophoblasts was documented; thus, a possible role in the regulation of hCG secretion and maintaining progesterone excretion could be suggested.19 However, there is no clear explanation for the actual mechanism of action of GnRH agonists when used as LPS, especially given the lack of extensive data and RCTs. Our results support the latest publication by Alsbjerg et al. The authors of a randomized control trial reported that the addition of an agonist such as LPS in medicated artificial FET did not improve the reproductive outcomes of the cycles. However, they reported a nonsignificant reduction in the MR in the GnRH agonist group.9 The difference between our study and the study of Alsberg et al is that we used a single dose at the time of embryo transfer in the setting of different euploid FET protocols, whereas the authors used 2 doses in the setting of nontested HRT FET cycles. Another RCT used the same GnRH agonist as we did in the setting of artificial cycles and reported nonsignificant improvements in the PR and LBR as well as a nonsignificant reduction in the MR.20 Interestingly, an RCT by Ye et al revealed that advanced-aged patients (35–37 years old) had a significantly greater implantation rate with the addition of an agonist 3 days after embryo transfer than with no agonist addition (45.3% vs 27.8%, p= 0.03).21 The only meta-analysis published on the use of GnRH agonists as part of LPS did show a significant improvement in implantation rates and PR (OR 1.6, 95% CI (1.22,2.09) and OR 1.87, 95% CI (1.4–2.4).22 Ye et al reported that there might be an age-related effect on implantation.21 Chang et al recently reported that the GnRH agonist LPS improved the LBR in both regular and RIF patients.23 The data concerning the effects of the GnRH agonist LPS on CL-containing FET cycles are even scarcer. After extensive research, only 2 articles discussing the use of GnRH agonists as LPSs in natural FET cycles were found. The first study by Haas et al reported increased implantation and ongoing pregnancy rates in a group receiving agonists. However, the results should be interpreted with caution given that the patients in the intervention group also received hCG injections in addition to the GnRH agonist, the control and intervention groups belonged to 2 different periods of 2 years apart, and the embryos were transferred at the cleavage stage, which limits the generalizability of the data published.24 The other study was a pilot RCT on the effect of the addition of a GnRH agonist to the LPS of natural FET cycles published by Seikkula et al. The authors reported no significant findings in the LBR or MR when the GnRH agonist group was compared with the no-intervention group (30.8% vs 24.2%, p= 0.481, and 12% vs 11.8%, p= 0.88, respectively).25
To the best of our knowledge, our study is the first, albeit retrospective, to analyze the use of GnRH agonist add-on for LPS in OI FET cycles. On the basis of our results, the addition of Gonapeptyl in the preimplantation period as part of LPS in FET with CL did not improve reproductive outcomes compared with the addition of OI without the GnRH agonist and to the medicated FET cycles. The latter could be explained by the extensive LPS that we provide to patients undergoing medicated FET cycles since, on the basis of internal data from our center, the MR in medicated FET cycles is similar to that in OI FET cycles (10% vs 2.4%, p= 0.115). A possible explanation for the lack of significant benefit for the use of GnRH agonists in OI cycles is the presence of 1–2 CLs only. This reflects that estrogen levels during the follicular phase are within the physiologic range; thus, the deleterious effect on supraphysiologic estrogen levels observed during ovarian stimulation and fresh embryo transfers should not be expected in FET cycles with only a few CLs. Ideally, the progesterone secreted by the CL postovulation causes endometrial secretory changes and defines the implantation window. This endogenous progesterone provides support for the endometrium, as well as early pregnancy until the placenta takes over. Importantly, in our study, patients receiving GnRH agonists such as LPS had a higher implantation rate (Table 4).
The strengths of our study include the analysis of a completely new concept, which is the use of agonists as part of the LPS in OI cycles. Our analyses also compared the still widely used artificial FET cycles with the OI cycles. Despite not showing statistical significance, the results of our study did show an improved PR and LBR in medicated FET cycles receiving GnRH agonists such as LPS. Given the numerical differences, one could reason that there is a promising future for GnRH agonist add-on; however, further larger RCT trials with larger sample sizes are urgently needed to clarify this matter further.
The main limitations of our study are its retrospective nature and the small sample size of the OI FET cycles (41 cycles). However, given the novelty of this concept, this sample size seems acceptable and can lay the groundwork for future well-designed double-blinded RCTs involving the use of GnRH agonist add-ons in modified natural cycles or OI FET cycles to eliminate bias, which would be a step toward properly studying this controversial topic. The other limitation is that the AG resulted in better-quality embryos being transferred. Given that the quality of the embryos (specifically good vs average) was a significant predictive factor of pregnancy, performing an RCT would be the only resort to highlight any potential beneficial effect of GnRH agonist supplementation as part of luteal phase support in FET cycles.
Conclusion
The use of a GnRH agonist as an add-on for LPS in FET cycles numerically increased the LBR without reaching statistical significance despite significantly improving the implantation rate. This potential beneficial effect was comparable between the artificial and ovulation-induction FET cycles. Further studies are needed to elucidate the effects of these medications on FET cycles.
Human Rights Statements and Informed Consent
The study was retrospective in nature; hence, no informed consent was needed. Nevertheless, no identifying personal data were used in this study, with the patients’ anonymity being maintained at all times.
Approval by the Ethics Committee
The study was approved by the research ethical committee of the fertility center where the study was conducted.
Data Sharing Statement
The datasets used and/or analyzed during the current study will be made available by the corresponding author upon request.
Acknowledgments
We are grateful to Sonia Khoutra, Marvi May Panelo, and Grace Angel Baysa for their assistance in the data collection process.
Author Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Anastasia A. Salame, Elias M. Dahdouh, Mokhamad Zhaffal Rania Aljafari, David A. Samuel, Bhavya P. Koodathingal, Aparna Bajpai, Shabin Kainoth, and Michael Fakih. The first draft of the paper was composed by Anastasia Salame, and all other authors provided their valuable comments on the paper. The final paper was read and approved by all the authors.
Funding
The authors received no Financial support for the research authorship or publication of this article.
Disclosure
Elias Dahdouh is a member of the international advisory committee of the MEFS. The other authors declare that they have no conflicts of interest related to this article.
References
1. Awonuga AO, Camp OG, Biernat MM, Abu-Soud HM. Overview of infertility. Syst Biol Reprod Med Taylor and Francis Ltd. 2025;71(1):116–142. doi:10.1080/19396368.2025.2469582
2. Adamson GD, Zegers-Hochschild F, Dyer S. Global fertility care with assisted reproductive technology. Fertil Steril. 2023;120(3P1):473–482. doi:10.1016/j.fertnstert.2023.01.013
3. Wang ET, Kathiresan ASQ, Bresee C, Greene N, Alexander C, Pisarska MD. Abnormal implantation after fresh and frozen in vitro fertilization cycles. Fertil Steril. 2017;107(5):1153–1158. doi:10.1016/j.fertnstert.2017.03.012
4. Levi Setti PE, Cirillo F, De Cesare R, et al. Seven years of vitrified blastocyst transfers: comparison of 3 preparation protocols at a single ART center. Front Endocrinol. 2020;11:346. doi:10.3389/fendo.2020.00346
5. Wolfe EL, Vaughan D, Craig W, et al. Modified natural and optimized programmed frozen embryo transfers have equivalent live birth rates: an analysis of 6,682 cycles. Fertil Steril. 2023;120(1):80–88. doi:10.1016/j.fertnstert.2023.02.020
6. Kyrou D, Kolibianakis EM, Fatemi HM, Tarlatzi TB, Devroey P, Tarlatzis BC. Increased live birth rates with gnrh agonist addition for luteal support in ICSI/IVF cycles: a systematic review and meta-analysis. Hum Reprod Update. 2011;17(6):734–740. doi:10.1093/humupd/dmr029
7. Liu Y, Wu Y, Pan Z, Jiang F, Lu Y, Meng Y. Single-dose versus multiple-dose gnrh agonist for luteal-phase support in women undergoing IVF/ICSI cycles: a network meta-analysis of randomized controlled trials. Front Endocrinol. 2022;13:802688. doi:10.3389/fendo.2022.802688
8. Leppänen R, Tinkanen H, Huhtala H, Ahinko K. Single-administered GnRH agonist as luteal phase support in insemination cycles: a randomized controlled trial. Gynecological Endocrinol. 2022;38(5):438–442. doi:10.1080/09513590.2022.2054984
9. Alsbjerg B, Kesmodel US, Elbaek HO, et al. GnRH agonist supplementation in hormone replacement therapy–frozen embryo transfer cycles: a randomized controlled trial. Reprod Biomed Online. 2022;44(2):261–270. doi:10.1016/j.rbmo.2021.10.019
10. Zareii A, Davoodi S, Alborzi M, Moghadam ME, Askary E. Co-administration of GnRH agonists with vaginal progesterone compared to vaginal progesterone in luteal phase support of the frozen-thawed embryo transfer cycle: an RCT. Int J Reprod Biomed. 2021;19(10):863–872. doi:10.18502/ijrm.v19i10.9817
11. Tesarik J, Hazout A, Mendoza C. Enhancement of embryo developmental potential by a single administration of GnRH agonist at the time of implantation. Hum Reprod. 2004;19(5):1176–1180. doi:10.1093/humrep/deh235
12. Pirard C, Donnez J, Loumaye E. GnRH agonist as luteal phase support in assisted reproduction technique cycles: results of a pilot study. Hum Reprod. 2006;21(7):1894–1900. doi:10.1093/humrep/del072
13. de Ziegler D, Pirtea P, Andersen CY, Ayoubi JM. Role of gonadotropin-releasing hormone agonists, human chorionic gonadotropin (hCG), progesterone, and estrogen in luteal phase support after hCG triggering, and when in pregnancy hormonal support can be stopped. Fertil Steril Elsevier Inc. 2018;109(5):749–755. doi:10.1016/j.fertnstert.2018.03.006
14. Salame AA, Dahdouh EM, Aljafari R, et al. Predictive factors of aneuploidy in infertile patients undergoing IVF: a retrospective analysis in a private IVF practice. Middle East Fertil Soc J. 2024;29(1):1–10. doi:10.1186/s43043-024-00172-y
15. Salame A, Dahdouh EM, Zhaffal M, et al. Embryos with “no result” after PGT-A: a retrospective analysis of causative factors. Obstet Gynecol Int. 2025;2025(1). doi:10.1155/ogi/4043963
16. Salame AA, Dahdouh EM, Aljafari R, et al. Predictive factors of aneuploidy in infertile patients undergoing IVF: a retrospective analysis in a private IVF practice. East Fertility Soc J. 2024;29(1):12. doi:10.1186/s43043-024-00172-y
17. Capalbo A, Rienzi L, Cimadomo D, et al. Correlation between standard blastocyst morphology, euploidy and implantation: an observational study in two centers involving 956 screened blastocysts. Hum Reprod. 2014;29(6):1173–1181. doi:10.1093/humrep/deu033
18. Limonta P, Marelli M, Mai S. GnRH receptors in cancer: from cell biology to novel targeted therapeutic strategies. academic.oup.com. 2012. Available from: https://academic.oup.com/edrv/article-abstract/33/5/784/2354875.
19. Maggi R, Cariboni AM, Marelli MM, et al. GnRH and GnRH receptors in the pathophysiology of the human female reproductive system. Hum Reprod Update. 2016;22(3):358–381. doi:10.1093/humupd/dmv059
20. Seikkula J, Ahinko K, Polo-Kantola P, et al. Mid-luteal phase gonadotropin-releasing hormone agonist support in frozen-thawed embryo transfers during artificial cycles: a prospective interventional pilot study. J Gynecol Obstet Hum Reprod. 2018;47(8):391–395. doi:10.1016/j.jogoh.2018.04.009
21. Ye H, Luo X, Pei L, et al. The addition of single dose GnRH agonist to luteal phase support in artificial cycle frozen embryo transfer: a randomized clinical trial. Gynecological Endocrinol. 2019;35(7):618–622. doi:10.1080/09513590.2018.1563888
22. Li S, Li Y. Administration of a GnRH agonist during the luteal phase frozen–thawed embryo transfer cycles: a meta-analysis. Gynecological Endocrinol. 2018;34(11):920–924. doi:10.1080/09513590.2018.1480714
23. Chang WS, Lin PH, Li CJ, et al. Additional single dose GnRH agonist during luteal phase support may improve live birth rate in GnRHa-HRT frozen-thawed embryo transfer cycle: a retrospective cohort study. BMC Pregnancy Childbirth. 2023;23(1):174. doi:10.1186/s12884-023-05491-y
24. Haas J, Lantsberg D, Feldman N, et al. Modifying the luteal phase support in natural cycle frozen-thawed embryo transfer improves cycle outcome. Gynecological Endocrinol. 2015;31(11):891–893. doi:10.3109/09513590.2015.1075502
25. Seikkula J, Anttila L, Polo-Kantola P, et al. Effect of mid-luteal phase GnRH agonist on frozen-thawed embryo transfers during natural menstrual cycles: a randomised clinical pilot study. Gynecological Endocrinol. 2016;32(12):961–964. doi:10.1080/09513590.2016.1196176
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Endometrial Thickness Change in Response to Progesterone is Associated with Ongoing Pregnancy Rate in Women with Treated Intrauterine Adhesion - A Prospective Cohort Study
Hou Z, Xu B, Zhao J, Zhang Q, Yang T, Tian F, Wang B, Li Y
International Journal of Women's Health 2025, 17:1363-1374
Published Date: 13 May 2025
Association of GnRH Agonist Pretreatment with Reproductive Outcomes in Women ≥35 years with Diminished Ovarian Reserve Undergoing Frozen Embryo Transfer: A Large Retrospective Cohort Study
Zhou Y, Liao Z, Guo Y
International Journal of Women's Health 2025, 17:5361-5373
Published Date: 10 December 2025