Back to Journals » Open Access Emergency Medicine » Volume 13
Protective Boxes to Prevent Airborne Transmission of SARS-COV-2: Hospital-Based Experiences and a Narrative Literature Review
Authors AAl Ibrahim AM ![]() , Kentab O, Aljahany M
, Kentab O, Aljahany M ![]() , Aljohani K
, Aljohani K
Received 6 April 2021
Accepted for publication 19 July 2021
Published 28 July 2021 Volume 2021:13 Pages 355—362
DOI https://doi.org/10.2147/OAEM.S314559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Ahmad M AAl Ibrahim,1 Osama Kentab,2 Muna Aljahany,3 Khalid Aljohani1
1Emergency Medicine Department, King Abdullah Bin Abdulaziz University Hospital, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2Emergency Medicine, College of Medicine, Emergency Department, King Abdullah Bin Abdulaziz University Hospital, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 3Department of Clinical Science, College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Osama Kentab
Emergency Medicine, College of Medicine, Emergency Department, King Abdullah Bin Abdulaziz University Hospital, Princess Nourah Bint Abdulrahman University, P.O. box: 84428, Riyadh, Saudi Arabia
Email [email protected]
Objective: Occupational safety in healthcare settings is an integral part of treating COVID-19. A growing body of evidence suggests that the inhalation of both respiratory droplets (> 5 μm) and tiny aerosols (< 5 μm) is a possible route of virus transmission. Recently, innovative barrier enclosures (aerosol boxes) have been designed to cover patients’ heads while allowing the implementation of airway management procedures through fitted holes. The initial design has undergone a series of modifications to improve staff safety, operators’ ergonomics, and the efficacy of airway procedures.
Methods: We reviewed the literature concerning different box modifications and provided an insight into our experience of using the box. Aerosol boxes have garnered the attention of clinicians who are frequently exposed to aerosols while performing aerosol-generating medical procedures, particularly endotracheal intubation. Current evidence comes from simulation-based studies rather than real-life clinical investigations.
Results: The reports indicated that the box has significantly reduced the diffusion of aerosols into the room; however, the operators have experienced difficulties in the maneuverability of airway devices.
Conclusion: Aerosol boxes should be used for patients necessitating simple elective intubations after healthcare providers are adequately trained. Customized designs can be further made based on clinicians’ experiences.
Keywords: aerosols, healthcare, occupational safety, severe acute respiratory syndrome
Introduction
The novel coronavirus disease (COVID-19) has significantly burdened the public health sector across different regions globally. Since the emergence of the causative virus in the late 2019 in Wuhan, China, more than 8 million confirmed infected patients and approximately 800, 000 deaths have been reported as of August 22, 2020 worldwide.1 Clinicians, epidemiologists and virologists are racing to get deep insights into disease pathogenesis, aspects of virus transmission, and the best ways to manage critical patients. However, several aspects have remained elusive, yet an eminent fact is that the disease is both deadly and highly transmissible.
In particular, near-field transmission has been a primary concern, and it was a cornerstone of disease prevention. In essence, methods of transmission including hand-to-face as well as coughing or sneezing from infected patients have been emphasized.2 Such aspects have prompted the widely recognized guidance for hand washing, social distancing, surface disinfection, and respiratory protection. In healthcare facilities, interim guidance from the World Health Organization (WHO)3 underscored the need to implement strict protective measures while managing patients with respiratory symptoms, such as the use of a medical masks and a particular respirator (ie, European Union standard FFP2, Health-certified N95, or equivalent) while performing aerosol-generating medical procedures (AGMPs).
However, healthcare workers (HCWs) face severe risks: positive viral infections were confirmed in more than 3000 HCWs in China, and 20% of the responding HCWs in Italy.4,5 Aerosols are distributed in the frequently touched areas in intensive care units (ICUs) and general wards, such as trash cans, computer mouses, and doorknobs.6 The risk of grasping a nosocomial infection is even higher during AGMPs, such as non-invasive ventilation, tracheotomy, and intubation/extubation.6 As such, protecting clinicians during these procedures has been increasingly acknowledged in medical practice. In the current article, we reviewed our experience with a modified version of a plastic cube that can be used to cover a patient’s head, allowing clinicians to perform airway procedures. We have also compared the used protective barrier with other similar innovations published in the literature.
Methods
First, since multiple epidemiological aspects of the COVID-19 virus are still unknown, we performed a literature review of current evidence that investigated hypotheses concerning aerosol transmission, particularly in hospitals. Second, considering the main objectives, the present narrative review included original research articles that investigated the application of protective boxes in-hospital settings to control the airborne transmission of COVID-19 virus particles. Original descriptive studies employing experimental models, simulated human participants, or patients were eligible. These articles were written in English language and published in peer-reviewed journals. Systematic reviews, case reports, and other narrative reviews were excluded.
Two authors (Ahmad M. Al Ibrahim and Osama Y. Kentab) independently reviewed the eligible articles in PubMed, Embase, and Google Scholar up to July 30, 2020. The following combinations of keywords and Boolean operators were used: (“protective” OR “aerosol” OR “airborne”) AND (“box*”) AND (“COVID-19” OR “coronavirus”) AND (“hospital” OR “emergency” OR “anesthesia”).
The obtained records were screened meticulously for eligible articles by two blinded authors (Ahmad M. Al Ibrahim and Osama Y. Kentab), and any disagreement regarding study selection was resolved by discussion with another author (Khalid Aljuhani). The full-article versions of eligible studies were downloaded and checked for consistency with our study objectives. Data were extracted from the included studies in a Spreadsheet (Microsoft Excel 2016, USA), including the last name of the first author, box dimensions, material, design, the number of ports, and the presence of specific modification. The extracted data were used to synthesize the narrative section discussing the described boxes in the literature. Finally, we demonstrated our experience with a modified design of the protective box, which would pave the way for other modifications and additional studies to assess the efficacy and safety of such a protective barrier, especially in critically ill patients.
Results and Discussion
An Overview of In-Hospital Aerosol Transmission and AGMPs in COVID-19
For infectious diseases, there is a broad agreement regarding human-to-human virus transmission.7 Physical contact is an essential element of direct (such as by a handshake) and indirect (via a fomite) contact. Contrastingly, airborne transmission requires no physical contact between individuals. Virus transmission is possible via the direct inhalation of respiratory droplets (greater than 5 µm in diameter) produced during sneezing or coughing or inhalation of tiny aerosols (<5 µm) containing the solid components remained after evaporation of respiratory droplets. Viral particles within aerosols can travel or remain suspended in air for about three hours.8 This was corroborated in large-scale epidemiological evidence in public places. Recently, in an analysis of COVID-19 infectious trends in three major epicenters, including Italy, Wuhan, and New York City, face covering was a major determinant of reducing the number of infections; while other measures, such as social distancing and hand sanitization, were not sufficient in all epicenters.9 This is because airborne transmission has been linearly associated with the frequencies of confirmed cases, suggesting a potent role of face covering to block the inhalation of virus-bearing aerosols. Nonetheless, the predominance of either routes of airborne transmission (droplet sprays or aerosol particles) in COVID-19 has remained enigmatic.
To address airborne transmission in-hospital settings, investigators have performed air sampling in different wards. In Singapore, air samples from isolation rooms tested positive for the virus in particles of diameters of 1–4 µm and >4 µm, and there was extensive contamination of air at the outlet of fans.10,11 The existence of virus-laden droplets on air exhaust outlets may suggest their displacement by airflows. In Wuhan, China, Guo et al6 found high rates of viral ribonucleic acid positivity in the indoor air near the patients (44.4%) and near the air outlets (35.7%) in ICUs; these rates were significantly higher than those detected in general wards (0% and 15.4% in both areas, respectively). In addition, about one-third and 12.5% of air samples from ICUs and general wards respectively, tested positive for the virus. The exposure to aerosols was possible for a distance of four meters; although, the transmission distance could not be determined accurately owing to the variation in viable virus quantification and the infectious dose.6 Additionally, a recent study conducted in two Wuhan hospitals used for COVID-19 treatment12 relied on droplet digital polymerase chain reaction-based detection assays to quantify virus copy counts in ICUs, coronary care units, and general wards. The authors reported high virus concentrations in patients’ mobile toilet rooms, suggesting that such contaminations might have come from either aerosolized virus particles from patients’ feces or patients’ breath in these areas. However, low or non-detectable virus concentrations were found at other patient areas with a negative pressure and high rates of air exchange, indicating the effectiveness of these preventive measures.12
Other preprint articles (non-peer-reviewed) have also shown similar outcomes, demonstrating a proportion of positive samples in the air of isolation areas, particularly in ICUs.13,14 Indeed, the aforementioned observations support potential risks implied owing to aerosol exposure in healthcare settings as emphasized in the contaminated samples swabbed from infrequently touched areas, such as air exhaust vents. HCWs can contract the infection during specific procedures.15 These could entail high-risks of infection, such as non-invasive ventilation, tracheal intubation, tracheostomy, and manual ventilation before intubation. High-risk AGMPs are frequently associated with producing aerosols of high viral load, consequently posing a significant risk for HCWs. In contrast, the AGMPs with lower risks of occupational infection include endotracheal aspiration, sputum collection, cardiopulmonary resuscitation, and nebulizer treatment.15,16 Such a discrepancy in the risk of infection may be ascribed to several factors. Intuitively, the necessity to be in close proximity to patients’ airways for long periods (the duration of exposure) is a major contributor to virus infection. Moreover, HCWs, who would manipulate tissues with high viral loads, such as oropharynx and nasopharynx, are also at an increased risk. Both the duration of exposure and proximity to virus-laden aerosols have been previously cited as major drivers of increased odds of nosocomial infections in the SARS outbreak of 2003, particularly during endotracheal intubation.16 The use of energy devices, such as drills, cautery, laser, etc., may also produce high loads of aerosols. Accordingly, the use of recognized respiratory personal protective equipment (PPE) by HCWs is imperative. N95 masks/respirators are a widely used means of protection. However, since they represent the lowest level of reliable respiratory protection,17 they may be inappropriate for high-risk AGMPs. It is, therefore, imperative to heighten the level of respiratory protection, such as the use of respirators of masks with 99- to 100-level filters.18 The use of PPE or full-body protection may, in some instances, hinder performing respiratory procedures efficiently, especially for brief or high-volume procedures. Innovative protective tools may have potent roles; but they should be used based on robust evidence to preserve patient and operator safety, conserve hospital resources, and offer a cost-effectiveness solution.
An Overview of Protective Boxes in the Literature
The recently published guidelines for the management of airway in patients with COVID-1919 have emphasized explicit measures for emergency tracheal intubation, such as limiting the number of staff present at the procedure, performing intubation in a negative pressure room with more than 12 air changes/hour, and wearing PPEs at all times. These relatively inconvenient conditions have inspired the clinicians in some areas to develop specific protective barrier enclosures, through which they can perform endotracheal intubation. On March 21, 2020, Dr. Hsien Yung Lai, a Taiwanese anesthesiologist, first described a simple, transparent plastic box with two openings on one side (the posterior side) to fit over patients.20,21 The box was made of acrylic or polycarbonate sheets, which could be recurrently disinfected with 70% alcohol after each intubation. Subsequently, clinicians in the United States have tested a similar plastic cube with two openings on one side, named an aerosol box, using a cough simulated model (Table 1).22 The investigators have used a mannequin with a small latex balloon filled with fluorescent dye and placed it in the hypopharynx. The balloon is then inflated with compressed oxygen to simulate a forceful cough, and the experiment was repeated with and without using the aerosol box. Without using the box, video records showed that the dye was found on the gown, face mask, gloves, eye shield, neck, ears, and hair of the laryngoscopist in addition to the floor and a monitor at a 2-m distance. By repeating the experiment using the box, the authors found that only the gloves and gowned forearms of the clinician and the inner sides of the box were contaminated. Nevertheless, the experiment may not reflect several aspects of the true clinical circumstances, such as real particle size distribution, cough force and directions, and the infectious doses.
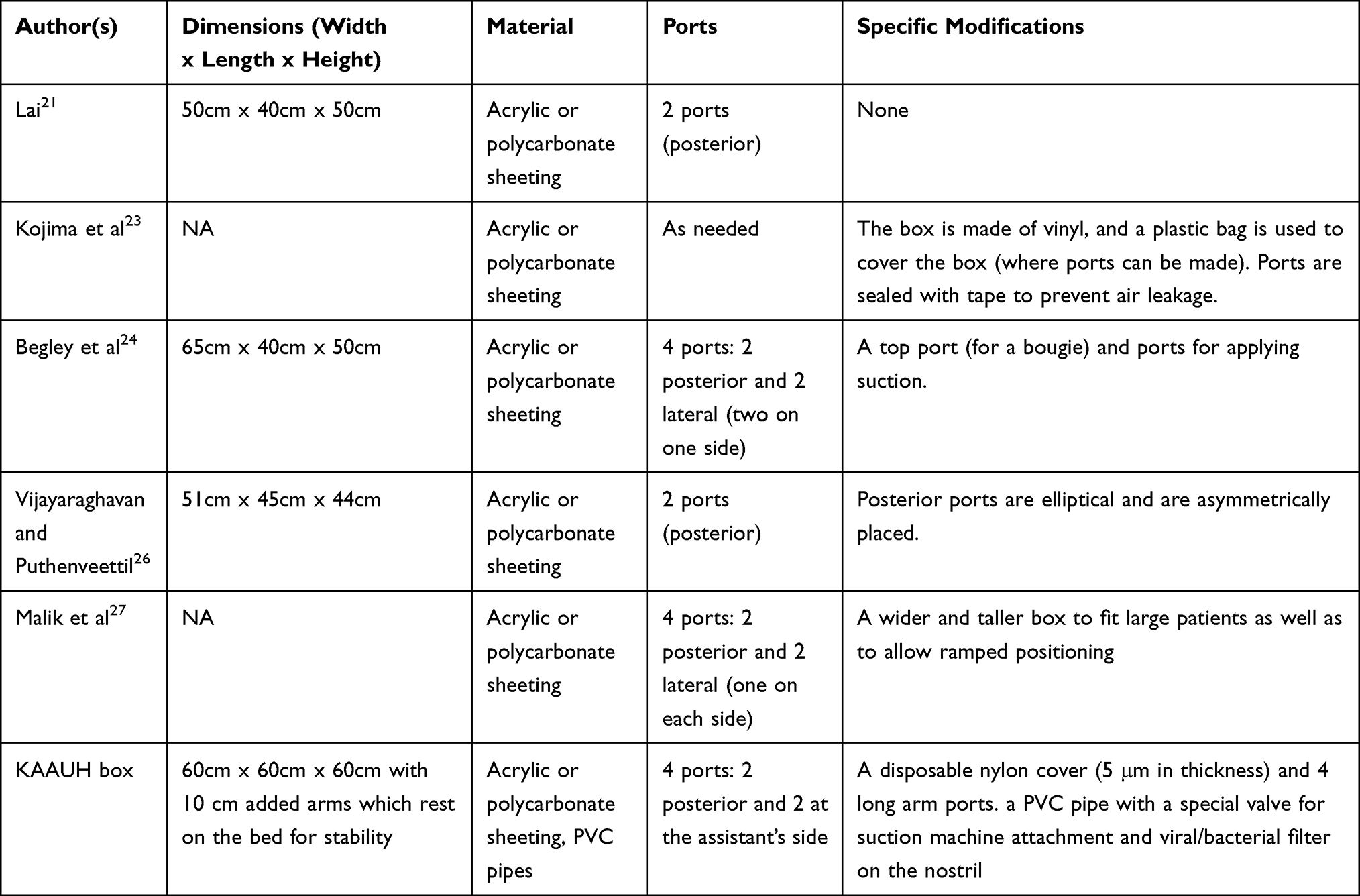 |
Table 1 The Traditional Aerosol Box and the Subsequent Modifications Reported in the Literature |
In Japan, Kojima et al23 demonstrated a modified version of the aerosol box (Kojima/Sugimura-type aerosol box). The modified box is covered with a vinyl, and a plastic bag is used to cover the box on all sides. Notches are made in the bag to access the patient. The new modification has allowed the clinicians to perform complicated tasks, such as fiber intubation and nasal intubation procedures, thanks to the high mobility of the arms. Additionally, creating as many notches as needed would have created a more convenient approach to the patient. Nevertheless, making unnecessary or inadequate cuts in the plastic bag may facilitate leakage and aerosol exposure. Thus, the notches should be appropriately sealed with tape. Furthermore, the authors could not reliably verify the extent that aerosol exposure and contamination could be prevented. They did not provide any analytical data regarding the intubation times, safety outcomes, and operators’ ergonomics.
To further assess the usability of aerosol boxes, investigators from an Australian health institute recently published the results of an in-situ simulation crossover study,24 where 12 consultant anesthetists were invited to perform three intubations: one without an aerosol box, one using Hsien Yung’s box (the earliest generation),20 and one using a modified version using specifications provided by an American manufacturer.25 The use of aerosol boxes was associated with significantly prolonged intubation times and reduced first-pass success rates as compared to the traditional intubation procedures. Indeed, the experienced airway specialists have faced remarkable procedural difficulties, possibly owing to reduced arm movement, impaired device manipulation, or increased cognitive overload. Importantly, the reported delays in intubation might be associated with critical desaturation and unfavorable consequences. The authors also reported one and seven breaches of PPE using the early- and latest-generation boxes, respectively. This may increase the risk of infection for the working clinicians. Notably, the small sample size, inability to explore the risk of virus exposure to clinicians, and the lack of relevant insights into the difficulties to less-experienced clinicians may all limit the interpretation of the reported outcomes.
With the purpose of improving operator ergonomics while using the aerosol boxes, Vijayaraghavan and Puthenveettil26 implemented specific modifications in the design of the box. Posterior ports were made elliptical (rather than circular), and they were asymmetrically placed (the left port is higher than the right). These modifications had been adopted based on multiple intubation attempts by a number of consultants on mannequin. Nonetheless, the authors reported that the clinicians still have encountered slight procedural difficulties, which could be improved by practice. In another modification, Malik et al27 developed a wider and taller box than the early generation box to allow a convenient positioning of large patients besides providing additional space to manipulate airway equipment, such as a gum elastic bougie. A supportive lip was also added at the base to stabilize the box and side handles were added to enable easy removal of the box if needed. Side ports (one at each side) were designed to enable an assistant to access the patient, a video laryngoscope lead, or suction tubing. The investigators added a sloping angled surface at the main clinician’s side to improve ergonomics by reducing the refractive error. No clinical investigations were performed; hence, no conclusive patient-related outcomes could be reported. However, the authors recommended the use of protective boxes in non-emergency airway management procedures, such as nasogastric tube insertion, tracheal tube exchange, tracheostomy suctioning, and postoperative tracheal extubation (in non-critical patients). Additionally, the box may be used to transfer ventilated and non-ventilated patients inside the hospital.27
Clinically, aerosol boxes may also provide additional benefits during surgical interventions of patients with COVID-19. The box was conveniently used by operating room staff to perform intubations in a series of six patients with COVID-19 who underwent surgeries for gastrointestinal complications.28 To our knowledge, no clinical studies have assessed the impact of these boxes on the safety of HCWs/patients as well as the efficacy of performing endotracheal intubation and other airway procedures. An open-label, prospective randomized controlled trial is being held involving 100 patients selected for elective surgery (ClinicalTrials.gov Identifier: NCT04366141). The patients will be randomized to an intervention group (intubated with the aerosol box) and a control group (no box). Differences in the time to endotracheal intubation, first-pass access rates, and the time of airway manipulation will be analyzed.
Our Hospital-Based Experience Using a Modified Aerosol Box
The aerosol box was modified at the Emergency Department, King Abdullah Bin Abdulaziz University hospital, Princess Noura Bint Abdulrahman University in Riyadh, Saudi Arabia (Figure 1). The box is a modified version of the early generation box of Hsien Yung Lai. It is a cube-shaped box (60 cm3) with one side open for the patient to be fitted on the emergency bed. We added 10-cm long arms to fit on the emergency stretcher and to allow clinicians of different statutes to operate conveniently. The frames of the box are made of acrylic, and a transparent plastic disposable sheet, five microns in thickness, is used to cover the box from all sides, through which operators’ notches can be made (Figure 1). This would also improve operators’ maneuverability, especially upon the manipulation of a gum elastic bougie or other airway management devices. The cover allows creating a negative pressure chamber inside the box with the application of suction, attached to it is small bacterial/viral filter, which is in agreement with the consensus guidelines for airway management in patients with COVID-19.3 Holes could be customized for the main operator and the assistants. Moreover, additional ports were designated for the insertion of a bougie and applying the suction. The large space with two additional helper openings could offer more area for maneuvers and the use of other airway aids, such as bag mask ventilation. Furthermore, these openings have allowed convenient assessment of the airway more frequently.
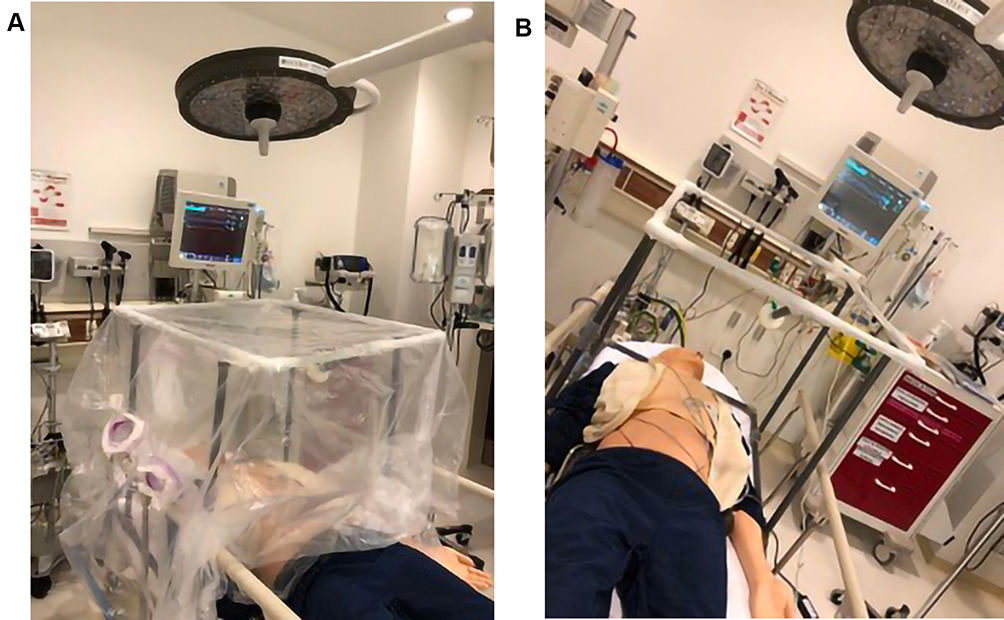 |
Figure 1 The utilized aerosol box at our institution with (A) and without (B) a transparent plastic disposable sheet. |
To further investigate the efficacy of the aerosol box, we conducted several tests to check for aerosol transmission outside the box. First, we placed a small-sized balloon containing fluorescent dye in the oropharynx of a manikin, which was then inflated with oxygen until it burst to simulate the cough of a COVID-19 patient. UV light was used to check whether there was any leakage of the dye from the box to the surroundings and/or the operator. We found that the fluorescent material stained the walls of the box as well as the suction nostril, indicating that the suction process within the box was effective in trapping the aerosol, leaving the outside of the box clean. Second, suction force is powerful as indicated by the visualization of the smoke of an e-cigarette smoked by a practitioner. Third, we used aromatic spray “air freshener” within the box, and no smell was detected by the staff outside the box. Finally, the box was tested on a critically ill patient who required an immediate bag mask ventilation. The use of the aerosol box was very effective in handling the patient, airway maneuvering, and providing assurance and confidence for the team as they can work with the feelings of safety and protection. In addition, the box fits well on ED stretchers and can be tucked around the bed in very stable way.
Overall, the mentioned modifications were intended for improving the flexibility of the box, operators’ ergonomics, and safety of the attending HCWs. Emergency physicians, anesthesiologists and the assisting medical staff would protect themselves from infection. This applies to patients with a suspected or confirmed COVID-19 infection. It may reduce air contamination and aerosol distribution in the operation room as confirmed in simulation studies. Ideally, aerosol boxes can be used for simple elective intubations. The box can be a versatile component of a broad protocol that can be specifically designated to airway management based on real-world practice and operators’ experiences in each institution. Expectedly, this can also conserve the PPE supply as HCWs are not forced to change their gowns, face shields, and caps between patients.
Limitations of the Aerosol Box
The use of currently modified aerosol boxes may have some limitations. Air leakage is possible through the holes made in the plastic sheet while making unnecessary cuts. The lack of supportive clinical evidence concerning severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) distribution while using the box may limit making a definite conclusion. It is unknown whether the use of flexible plastic covers would be associated with breaches in the PPE, especially for untrained personnel, which could threaten their safety. Owing to the lack of adequate training with using aerosol boxes in the context of emergencies and the need to perform rapid endotracheal intubation in patients with COVID-19 after failed non-invasive ventilation approaches, it is currently recommended to stick to well-trained procedures for airway management. Accordingly, the application of aerosol boxes should be avoided when critically ill patients require an instant intervention.
An Updated Overview from the Literature
Given that COVID-19 research articles are being published at an exceptionally fast pace, new scoping reviews and simulation models have been available while reviewing the current article. Simpson et al29 assessed the exposure of laryngoscopists to airborne particles of nebulized saline (sized 0.3–5.0 microns) generated in an in-situ simulation model; the authors used five containment devices, including a vertical drape, a horizontal drape, sealed boxes with and without suction, and an aerosol box. Notably, airborne particle exposure at 300 s increased significantly with the use of a sealed intubation box compared with no device use, and the exposure increased consistently when a patient coughed compared with other devices and/or no device use.29 In a more recent scoping review of 52 articles (primarily small case series, expert opinions, pre-print articles, and simulation studies),30 the authors have revealed significant concerns regarding limitations on conducting airway interventions, PPE compromise, and patient injuries. Furthermore, evidence was lacking regarding a consensus regarding cleaning standards to reduce the risk of infection to healthcare providers and regarding the risk of exposure to secondary aerosolization upon barrier removal.30 Accordingly, although the food and drug administration (FDA) had previously issued an umbrella Emergency Use Authorization (EUA) for emergency use of the protective aerosol boxes by healthcare providers,31 the organization revoked the authorization of barrier enclosures with or without negative pressure on August 21,2020.32
Conclusions
Aerosol boxes have garnered a considerable amount to attention to protect HCWs while they perform airway procedures, particularly endotracheal intubation. These protective enclosures have undergone a series of modifications to improve the efficacy of performing airway interventions, patients’ and HCWs’ safety, and operators’ ergonomics. To date, evidence relied exclusively on simulated models rather than real-life clinical aspects. Although video recordings have shown promising protective outcomes that limited the diffusion of aerosols into the operating room, recent studies have revealed no added benefits of barrier enclosures to prevent the exposure of healthcare providers to pathogenic airborne particles. The FDA has revoked the EUA of aerosol boxes because there is no reliable evidence concluding that the potential benefits of such barriers could outweigh the potential risks. Besides, some technical difficulties (reduction in maneuverability) have been encountered while using the boxes as compared to box-free procedures.
Until a learning curve can be identified, aerosol boxes can only be used after adequate training as an adjunct to PPE (not an alternative). Their use during emergency endotracheal intubation still needs further clinical exploration to be fully adopted.
Abbreviations
AGMPs, aerosol-generating medical procedures; COVID-19, the novel 2019 coronavirus disease; HCWs, healthcare workers; ICUs, intensive care units; PPE, personal protective equipment; SARS-COV-2, severe acute respiratory syndrome coronavirus 2; WHO, World Health Organization.
Funding
This research was funded by the Deanship of Scientific Research at Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia, through the Fast-track Research Funding Program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Coronavirus disease (COVID-2019) situation reports. Geneva: WHO; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports.
2. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. doi:10.1016/j.jaut.2020.102433
3. World Health Organization. Advice on the use of masks in the community, during home care, and in health care settings in the context of COVID-19: interim guidance, 19 March 2020. Geneva: World Health Organization; 2020. Available from: https://apps.who.int/iris/bitstream/handle/10665/331493/WHO-2019-nCoV-IPC_Masks-2020.2-eng.pdf.
4. Yimeng Z, Kun L Medical worker infections under control; 2020. Available from: https://www.chinadaily.com.cn/a/202003/06/WS5e6246c8a31012821727d0bc.html.
5. Remuzzi A, Remuzzi G. COVID-19 and Italy: what next? Lancet (London, England). 2020;395:1225–1228. doi:10.1016/S0140-6736(20)30627-9
6. Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020:26. doi:10.3201/eid2607.200885.
7. Tellier R, Li Y, Cowling BJ, Tang JW. Recognition of aerosol transmission of infectious agents: a commentary. BMC Infect Dis. 2019;19:101. doi:10.1186/s12879-019-3707-y
8. van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020;382:1564–1567. doi:10.1056/NEJMc2004973
9. Zhang R, Li Y, Zhang AL, Wang Y, Molina MJ. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc Natl Acad Sci U S A. 2020;117:14857. doi:10.1073/pnas.2009637117
10. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;323:1610–1612. doi:10.1001/jama.2020.3227
11. Chia PY, Coleman KK, Tan YK, et al. Detection of air and surface contamination by SARS-CoV-2 in hospital rooms of infected patients. Nat Commun. 2020;11:2800. doi:10.1038/s41467-020-16670-2
12. Liu Y, Ning Z, Chen Y, et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature. 2020. doi:10.1038/s41586-020-2271-3
13. Jiang Y, Wang H, Chen Y, et al. Clinical data on hospital environmental hygiene monitoring and medical staffs protection during the coronavirus disease 2019 outbreak. medRxiv. 2020. doi:10.1101/2020.02.25.20028043
14. Ding Z, Qian H, Xu B, et al. Toilets dominate environmental detection of SARS-CoV-2 virus in a hospital. medRxiv. 2020. doi:10.1101/2020.04.03.20052175
15. Zhang M, Zheng H, Wang J. Strategy of using personal protective equipment during aerosol generating medical procedures with COVID-19. J Clin Anesth. 2020;66:109911. doi:10.1016/j.jclinane.2020.109911
16. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7:e35797. doi:10.1371/journal.pone.0035797
17. Centers for Disease Control and Prevention. Interim domestic guidance on the use of respirators to prevent transmission of SARS: CDC; 2003. Available from: https://www.cdc.gov/sars/clinical/respirators.html.
18. Howard BE. High-risk aerosol-generating procedures in COVID-19: respiratory protective equipment considerations. Otolaryngo Head Neck Surg. 2020;163:98doi:10.1177/0194599820927335
19. Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: guidelines from the difficult airway society, the association of anaesthetists the intensive care society, the faculty of intensive care medicine and the royal college of anaesthetists. Anaesthesia. 2020;75:785–799. doi:10.1111/anae.15054
20. Everington K Taiwanese doctor invents device to protect US doctors against coronavirus Taiwan; 2020. Available from: https://www.taiwannews.com.tw/en/news/3902435.
21. Lai H. Aerosol box - design Taiwan; 2020. Available from: https://sites.google.com/view/aerosolbox/design?authuser=0.
22. Canelli R, Connor CW, Gonzalez M, Nozari A, Ortega R. Barrier enclosure during endotracheal intubation. N Engl J Med. 2020;382:1957–1958. doi:10.1056/NEJMc2007589
23. Kojima Y, Aoyama K, Yamagata K, Sugimura M. A modified barrier enclosure to prevent viral aerosol transmission during endotracheal intubation and extubation of patients with coronavirus disease. J Clin Anesth. 2020;65:109876. doi:10.1016/j.jclinane.2020.109876
24. Begley JL, Lavery KE, Nickson CP, Brewster DJ. The aerosol box for intubation in coronavirus disease 2019 patients: an in-situ simulation crossover study. Anaesthesia. 2020. doi:10.1111/anae.15115
25. Intubation box - aerosol box a protective shield against covid-19 USA; 2020. Available from: https://intubationbox.com/.
26. Vijayaraghavan S, Puthenveettil NJ. Aerosol box for protection during airway manipulation in covid-19 patients. Indian J Anaesth. 2020;64:148.
27. Malik JS, Jenner C, Ward PA. Maximising application of the aerosol box in protecting healthcare workers during the COVID-19 pandemic. Anaesthesia. 2020;75:974–975. doi:10.1111/anae.15109
28. Bianco F, Incollingo P, Grossi U, Gallo G. Preventing transmission among operating room staff during COVID-19 pandemic: the role of the Aerosol Box and other personal protective equipment. Updates Surg. 2020;1–4. doi:10.1007/s13304-020-00818-2
29. Simpson JP, Wong DN, Verco L, Carter R, Dzidowski M, Chan PY. Measurement of airborne particle exposure during simulated tracheal intubation using various proposed aerosol containment devices during the COVID‐19 pandemic. Anaesthesia. 2020;75:1587–1595.
30. Sorbello M, Rosenblatt W, Hofmeyr R, Greif R, Urdaneta F. Aerosol boxes and barrier enclosures for airway management in COVID-19 patients: a scoping review and narrative synthesis. Br J Anaesth. 2020;125:880–894. doi:10.1016/j.bja.2020.08.038
31. U.S Food and Drug Administration. Protective barrier enclosures - letter of authorization: FDA; 2020. Available from: https://www.sawbones.com/media/assets/product/documents/Protective-Barrier-Enclosures-EUA.pdf.
32. U.S Food and Drug Administration. Protective barrier enclosures without negative pressure used during the COVID-19 pandemic may increase risk to patients and health care providers - letter to health care providers: FDA; 2020. Available from: https://www.fda.gov/media/141415/download.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.