Back to Journals » Research and Reports in Urology » Volume 17
Prostate Cancer Among Patients Presenting with Obstructive Lower Urinary Tract Symptoms at a Tertiary Hospital in South Western Uganda
Authors Kyegombe W ![]() , Ronald O, Nimusima A, Nsubuga Y
, Ronald O, Nimusima A, Nsubuga Y ![]() , Nakitto B
, Nakitto B ![]() , Nannungi C
, Nannungi C ![]() , Epodoi J, Opito R
, Epodoi J, Opito R ![]() , Ekuk E, Mwesigwa MM
, Ekuk E, Mwesigwa MM
Received 4 June 2025
Accepted for publication 6 September 2025
Published 30 September 2025 Volume 2025:17 Pages 367—381
DOI https://doi.org/10.2147/RRU.S515662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Willy Kyegombe,1,2 Okidi Ronald,3 Anitah Nimusima,4 Yakobo Nsubuga,3,4 Brenda Nakitto,3 Christine Nannungi,3 Joseph Epodoi,5 Ronald Opito,2 Eddymond Ekuk,1 Marvin Mutakooha Mwesigwa1
1Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2Faculty of Medicine, Soroti University, Soroti, Uganda; 3Faculty of Medicine, Gulu University, Gulu, Uganda; 4Mulago National Regional Referral Hospital, Kampala, Uganda; 5Soroti Regional Referral Hospital, Soroti, Uganda
Correspondence: Willy Kyegombe, Faculty of Medicine, Soroti University, P.O. BOX 211, Moroto Road, Soroti, Uganda, Tel +779755664, Email [email protected]
Background: Prostate cancer is currently the second commonest male cancer both globally and in Uganda. Men are often tested after presenting with obstructive lower urinary tract symptoms (LUTS). We evaluated total prostate-specific antigen patterns (tPSA), digital rectal examination (DRE) findings, histological findings and prostate cancer rates among patients presenting to Mbarara regional referral hospital with obstructive LUTS.
Methods: This was a cross-sectional study of 140 patients aged ≥ 50 with obstructive LUTS. Data on demographics and severity of LUTS was collected, plus the results of tPSA testing and DRE. Later, digitally guided transrectal tru-cut prostate biopsy was performed, if necessary. Analysis was done using SPSS (Statistical Package for Social Scientists), version 14. Confidence interval (CI) was set at 95% and P at 0.005.
Results: The majority of patients had severe LUTS (n=103, 73.57%), with a median tPSA of 14.4 ng/mL. Ninety-nine patients experienced digitally guided transrectal tru-cut prostate biopsy (70.71%; Fisher’s exact test = 0.001). DRE abnormalities were found in 57.14% (n=80) of participants and these carried a higher risk for prostate cancer diagnosis (risk ratio = 5.895; Fisher’s exact test = 0.04; CI 95%: 1.59– 21.822). The tru-cut biopsy positivity rate was high, at 46% (45/99; 95% CI: 30.1– 46.3); all had prostate adenocarcinoma and the majority (77.78%, n=35) had a total Gleason score of 8 and above. Of those who had a malignancy, more than a quarter were between 60– 80 years of age (37.8%, n = 17). There was no statistically significant relationship between LUTs and prostate cancer diagnosis (Fisher’s exact test 2-sided = 0.84).
Conclusion: Although severity of LUTS was not predictive of cancer, there was a high rate of advanced prostate cancer among study participants. DRE remains a valuable tool for identifying potential prostate cancer cases, especially in settings where PSA testing may be limited. Further research is needed to explore effective screening strategies and improve outcomes for men with prostate cancer in Uganda.
Keywords: prostate cancer, prostate-specific antigen, lower urinary tract obstruction, digital rectal examination
Introduction
Globally, prostate cancer is the second most common cancer in men, with 1.5 million new cases each year and incidence rates of 35.5 and 12.6 per 100,000 in high- and low-income countries, respectively.1 Over 75% of cases are being observed in men over the age of 65,2,3 which could be attributed to early detection and better survival rates.4 Lower rates have been reported by low-income countries and it is speculated that poor health-seeking behavior, lack of proper screening programs, and a relatively low number of elderly people could explain this variation.5 However African statistics are currently also indicating an upward trend in prostate cancer prevalence and incidence, with the main drivers of this being; aging population growth together with the associated increase in risk factors.6,7 Limited resources, urgent public health challenges, including communicable diseases such as acquired immunodeficiency syndrome (AIDS)/human immunodeficiency virus (HIV) infection, malaria, and tuberculosis, which continue to plague most African countries, are also main drivers of this situation as they absorb most of the merger resources.8
By 2006 in Uganda prostate cancer had become the most common type of male cancer, with an age-standardized incidence rate of 65 per 100,00 and annual increase in incidence of 5.2%; these are still among the highest recorded rates on the African continent.9,10 Data extracted from the Kyadondo cancer registry between 1991 and 2015 reveals a similar trend for prostate cancer.7,11 The true burden might be even higher since most12 of this data comes from a centralized registry that reports data from mainly the central region. Over 75% of cases are observed in men over the age of 70 years,11,13 and their cancer is always advanced and incurable at first presentation.12
Early prostatic cancer is usually asymptomatic. However, as it progresses patients can develop local symptoms like LUTS, hematuria, and finally metastatic disease can involve a variety of symptom ranging from back pain, pathological fractures, and respiratory symptoms to severe anemia.12 Among all these symptoms LUTS are generally becoming more prevalent among patients with confirmed prostate cancer.12,14–16 This supports the findings of one study that locally advanced cancer can cause LUTS that are similar to those for benign prostatic hypertrophy.17 In addition to LUTS, locally advanced prostate cancer can present with unique DRE findings, like fixation of rectal skin, bleeding per rectum, and increased nodularity.18,19
Despite the current global consensus on the lack of relationship between LUTS and prostate cancer,20 a large number of males are currently presenting with lower urinary tract symptoms21 and are more likely to have their first test for prostate cancer at this time.22 These symptoms serve as the main and only prerequisite for prostate cancer testing, especially among high risk elderly patients. Such testing involves being subjected to total serum prostate-specific antigen level estimation, digital rectal examination and tru-cut prostate biopsy to establish histological confirmation, as guided by the National Institute for Health and Care Excellence (NICE), Canadian Urology Association.23 The current scarcity of information on prostate cancer in this population of patients in our setting might be leading to overutilization of LUTS as an entry point to testing and disregarding of other recommended but even more sensitive methods like yearly tPSA and routine DRE.
This makes it imperative to ascertain the regional clinical and biochemical profile of prostate cancer in this population of patients. This information is not only crucial in successfully developing strategic plans to combat the current late presentation with advanced prostate cancer but also in guiding the equitable distribution of cancer care resources. Therefore, this study set out to describe the commonest DRE findings, PSA patterns, prostate cancer rates, and histological characteristics in a small population of men presenting with LUTS to a regional referral hospital in south western Uganda.
Materials and Methods
Study Design and Setting
This was a cross-sectional descriptive study of men aged 50 years and above who presented to Mbarara Regional Referral Hospital with LUTS. The hospital is a government-owned facility that started in 1930 as a nursing school for the south western region of Uganda. Being within the vicinity of the Mbarara University of Science and Technology, it also serves as a teaching hospital providing clinical training for medical students, nurses, pharmacists, and laboratory technologists. Through this program, the hospital also provides specialized care and serves as a major referral hospital for a population of over 4 million people in its catchment area of western Uganda. The Urology Division is one of the avenues through which the hospital provides specialized services to the community. It has a full-time urologist, 4 nurses and 1 medical officer. This team runs an outpatient clinic every Friday and also has an inpatient wing with a bed capacity of 10 patients.
Inclusion and Exclusion Criteria
We included all males aged 50 years of age and above who presented to Mbarara Regional Referral Hospital with obstructive lower urinary tract symptoms. Those with a diagnosis of prostate cancer and already receiving treatment were excluded.
Operational Definitions
- Obstructive lower urinary tract symptoms: A study participant has obstructive lower urinary symptoms if he reports any one of the following clinical complaints lasting a period of one or more months. The symptoms, according to the American Urological Association, include straining, incomplete emptying of the bladder, urgency, straining, urinary frequency, or nocturia.
- Abnormal digital rectal examination findings: Detection of any of the following on the prostate gland: enlargement, nodules, induration, asymmetry, loss of the median groove, or tethering of rectal mucosa to the prostate gland. Prostate size was estimated using finger breadth and enlargement was set at more than 1.5 finger breadth and/or inability to get examining finger above the gland.
- Normal tPSA: The normal value was set at ≤ 4 ng/mL.
- Histological patterns: The different types of prostate cancer (ductal adenocarcinoma, sarcomatoid, basal cell, squamous cell, adenosquamous [ASC], and urothelial carcinoma) and Gleason scores.
Sampling Procedure
The consecutive sampling method was used. For a period of one year, participants were selected by convenience as they arrived at either the outpatient urological general and private clinic or emergency department. Each patient was assigned a participant-specific number to avoid reselection.
Sample Size Calculation
This was determined using the Kish and Leslie formula (1965): n = Z2 P(1−P)/D2. P = an estimated prevalence of 0.107, adjusted from a Caribbean screening study on the prevalence of prostate cancer (Bunker et al, 2004) (N = 147 participants).
Data Collection Tools and Procedure
Demographic and symptom data was collected using a structured questionnaire, administered by either a trained research assistant or the principal investigator. IPSS was self-administered with minimal help from the research assistant, tPSA level testing was done for each of the participants by a qualified laboratory technician from the Mbarara Regional Referral Hospital certified clinical labs (SANAS: ISO 15189).
This was then followed by a digital rectal examination conducted the principal investigator or a urologist to assess the prostate for abnormalities. Those with abnormalities of serum PSA levels or DRE findings underwent a digitally guided tru-cut prostate biopsy (Figure 1).
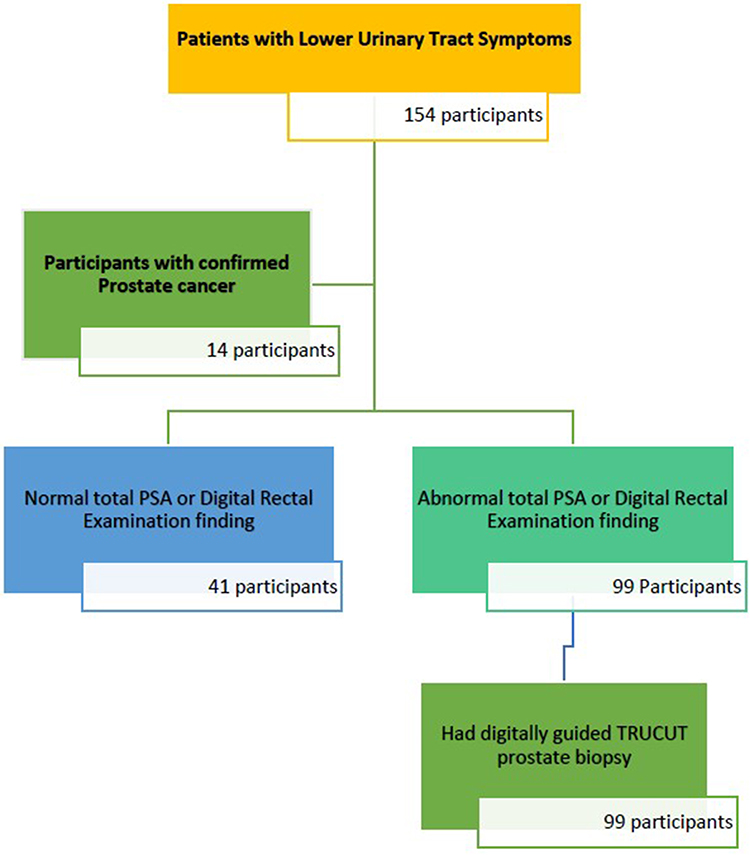 |
Figure 1 Selection schema for participants presenting with LUTS. |
For patients who agreed to undergo this procedure, the following steps occurred:24
- Oral ciprofloxacin 500mg as a single dose was provided for prophylaxis.
- Anesthesia was provided by either a saddle block, topical local anesthetic (Lignocaine cream) or periprostatic infiltration.
- At approximately 10 minutes from application of the local anesthetic agent, the patient was placed in the lithotomy position and a digitally guided sterile tru-cut needle was introduced into the rectal canal. From this multiple core biopsies were picked from quadrants of the prostate and any other nodular areas.
- A total of 6 to 12 cores were collected from different prostatic zones. These were then preserved in 10% formalin and transported to the pathology department of Mbarara University for histological analysis.
The results of the histological analysis were received and recorded against corresponding questionnaires.
Data Management and Analysis Plan
Data analysis was performed using SPSS, version 14, with descriptive statistics presented as means, medians, or interquartile ranges for continuous variables and counts for categorical variables. Proportions of categorical data were compared using Fisher’s exact test, with a significance level set at p = 0.05. Spearman correlation was employed to assess relationships among non-normally distributed continuous variables, with outcomes illustrated in scatter plots.
Ethical Consideration
Approval was obtained from the Research Ethical Committee of MUST and the Institutional Review Board (approval number: MUST-2021-149). Written consent was secured from all patients before enrollment, and they retained the right to withdraw from the study at any time. This article complies with the Declaration of Helsinki.
Results
Overall, 140 participants were enrolled in this study, the majority of whom were aged between 61 to 70 years (32.86%, (46/140; mean = 69.8±11.1). They came from mainly the districts of Mbarara (30%) and Insingiro (25%). Their major occupation was peasant farming (n=111, 79.28%). The majority (73.57%, 103/140) presented with severe LUTS, as shown in Table 1.
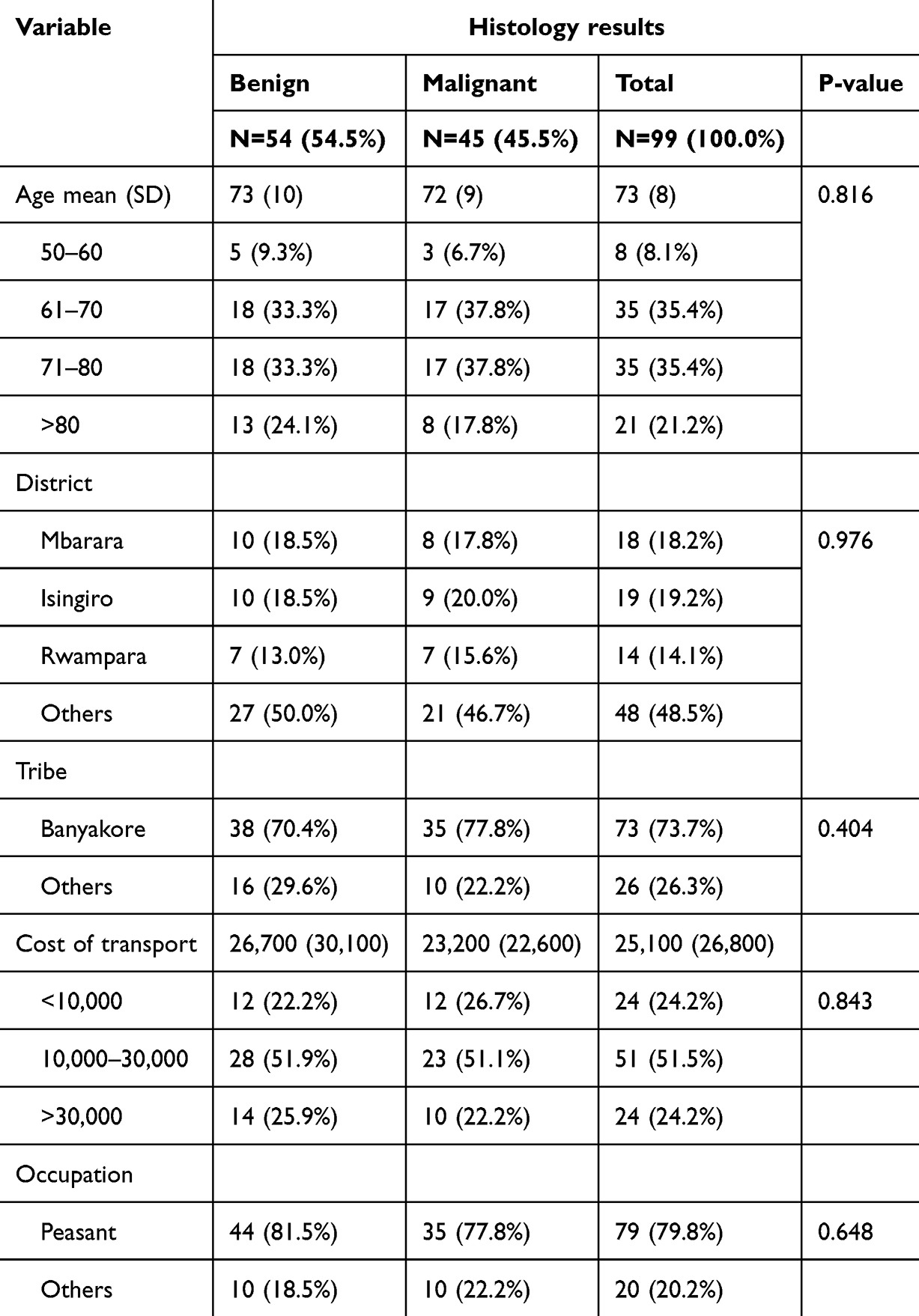 |
Table 1 Sociodemographic Characteristics of Patients Presenting with Obstructive Lower Urinary Tract Symptoms at Mbarara Regional Referral Hospital |
Only 99 were investigated for prostate cancer. Of these, 2% (n = 2) had a low IPSS, 15.2% (n = 15) a medium IPSS, and 82.8% (n = 82) a high IPSS. Of those who had a malignancy (45.5%, n = 45), the majority (77.8%, n = 35) had an unfavorable Gleason grade (IUSP grade 3) (Table 2). More than a quarter were between 60–80 years of age (37.8%, n = 17) compared to those aged between 50–60 years (6.7%, n = 3). The majority were peasant farmers (77%, n = 35) with no chronic medical illnesses (66.7%, n = 30) (Table 2).
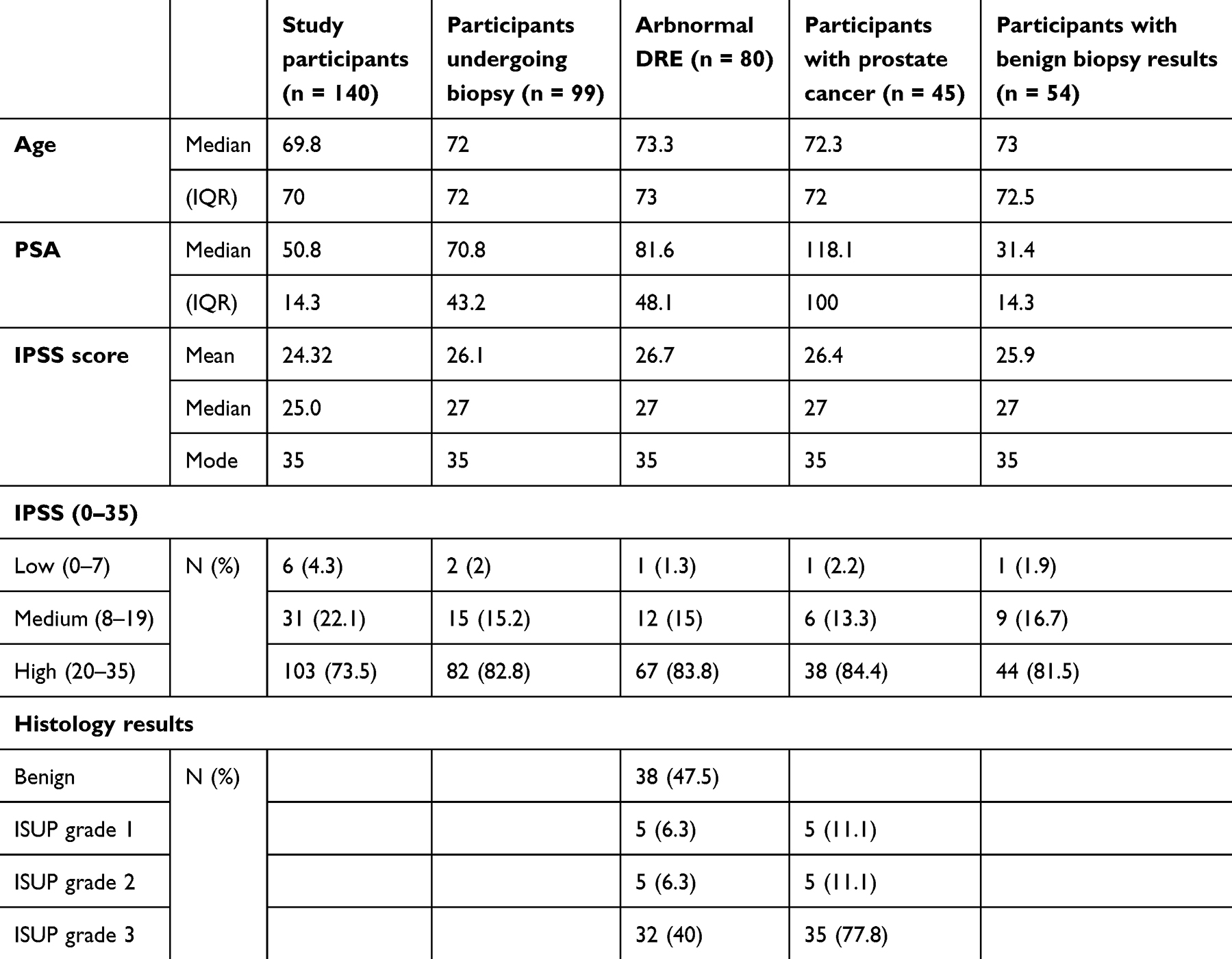 |
Table 2 Clinical Characteristics of Participants |
Total Serum Prostate-Specific Antigen and Digital Rectal Examination Patterns
Median PSA was 14.3 ng/mL; the lowest PSA value recorded was 0.29ng/mL and the highest was 592 ng/mL. The majority of participants (99/140, 71%) had tPSA values above 4 ng/mL (Table 3) and there was a fairly strong positive (r = 0.4114) correlation between age and PSA (p<0.001) (Figure 2).
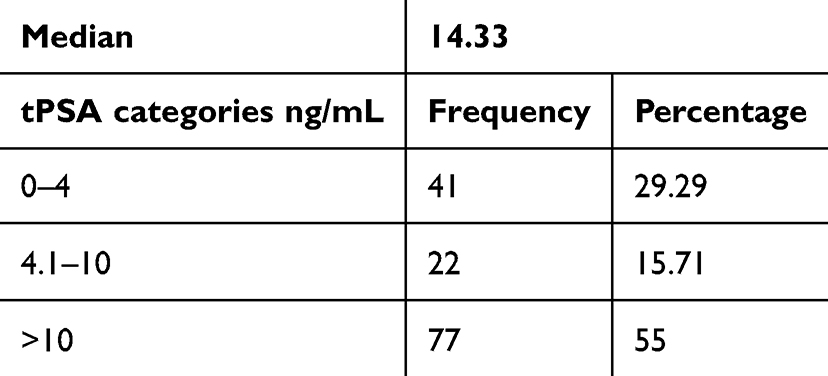 |
Table 3 Percentage of Patients per tPSA Category |
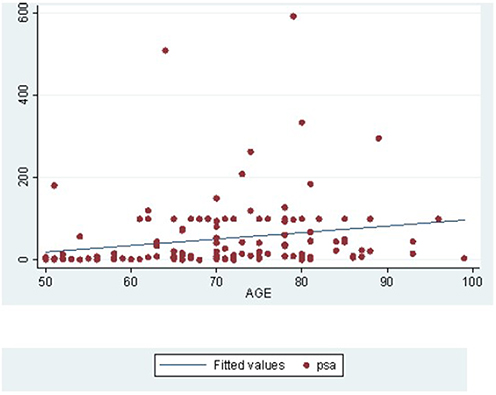 |
Figure 2 Distribution total serum PSA levels with age. |
Abnormalities on DRE were found in 57.14% (80/140) of participants who presented with LUTS. All but one of these had a serum PSA of more than 4 ng/mL (Fisher’s exact test = 0.001).
The majority of participants with a an malignancy had an enlarged prostate (88%, n = 40), a nodular prostate (88%, n = 37) with a loss of the median groove (81%, n = 37), and abnormal digital rectal exam results (93%, n = 42) (Table 4).
 |
Table 4 Digital Rectal Examination Findings Among Patients Who Underwent Prostate Biopsy |
Histological Findings
All patients with histologically confirmed malignancy had prostate adenocarcinoma, as shown in Figure 3. Histological patterns among student participants who underwent tru-cut prostate biopsy revealed that the mean Gleason risk score was 8 (±1.148). When the individual Gleason scores were classified into three categories, the majority of the adenocarcinoma had a Gleason score of 8 and above.(77.78%, n = 35), as shown in Figure 4.
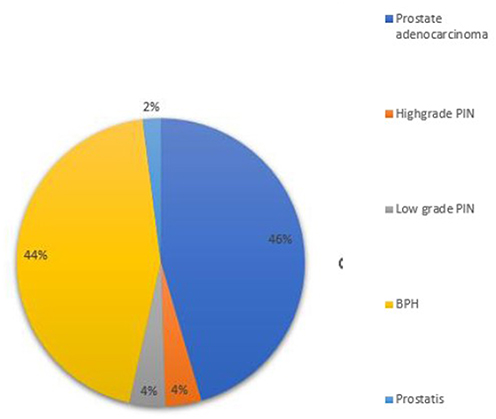 |
Figure 3 Histological patterns among study participants who underwent tru-cut prostate biopsy. |
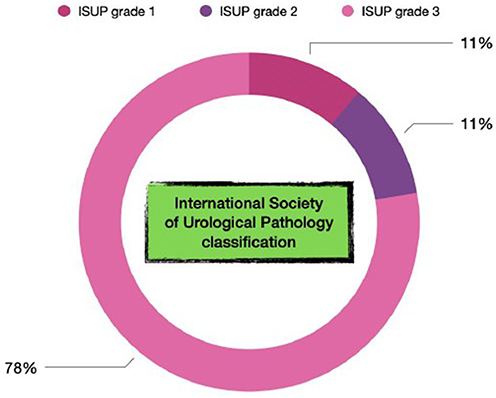 |
Figure 4 International Society of Urological Pathology prostate cancer results among participants. |
The distribution of IPSS among men who underwent prostate biopsy and how this corresponds with the risk of cancer are shown in Figures 5 and 6. The proportion of positive histology results increased significantly among those with severe LUTS. However, this increase was not statistically significant (Fisher’s exact test 2-sided: p = 0.84). Figure 6 further illustrates that the risk of prostate cancer narrowly varied for all three categories of IPSS.
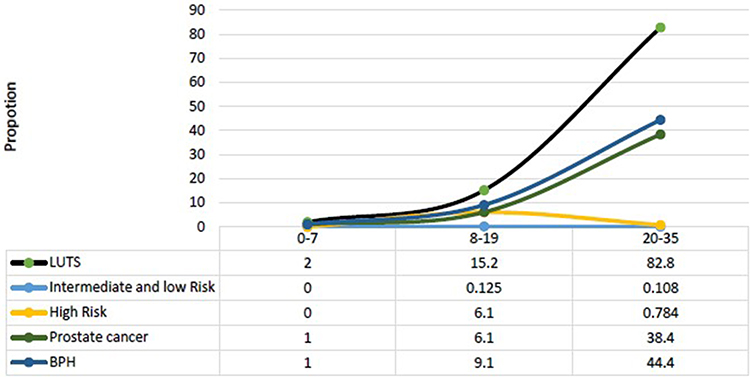 |
Figure 5 Histological outcomes subdivided by distribution of IPSS. |
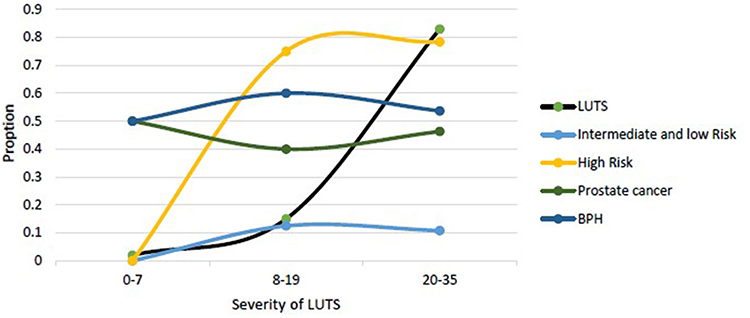 |
Figure 6 Risk of prostate cancer subdivided by distribution of IPSS. |
Individuals with abnormalities on digital rectal examination were more likely to have a biopsy positive for prostate cancer (OR 5.895; CI 95%: 1.59–21.822; Fisher’s exact test: P = 0.04). The OR decreased to 5.68 after adjusting for total serum PSA in a binary logistic regression analysis (Table 5). Age and histological outcome did not demonstrate any statistically significant relationship and therefore were adjusted for as a confounder in the above relationship.
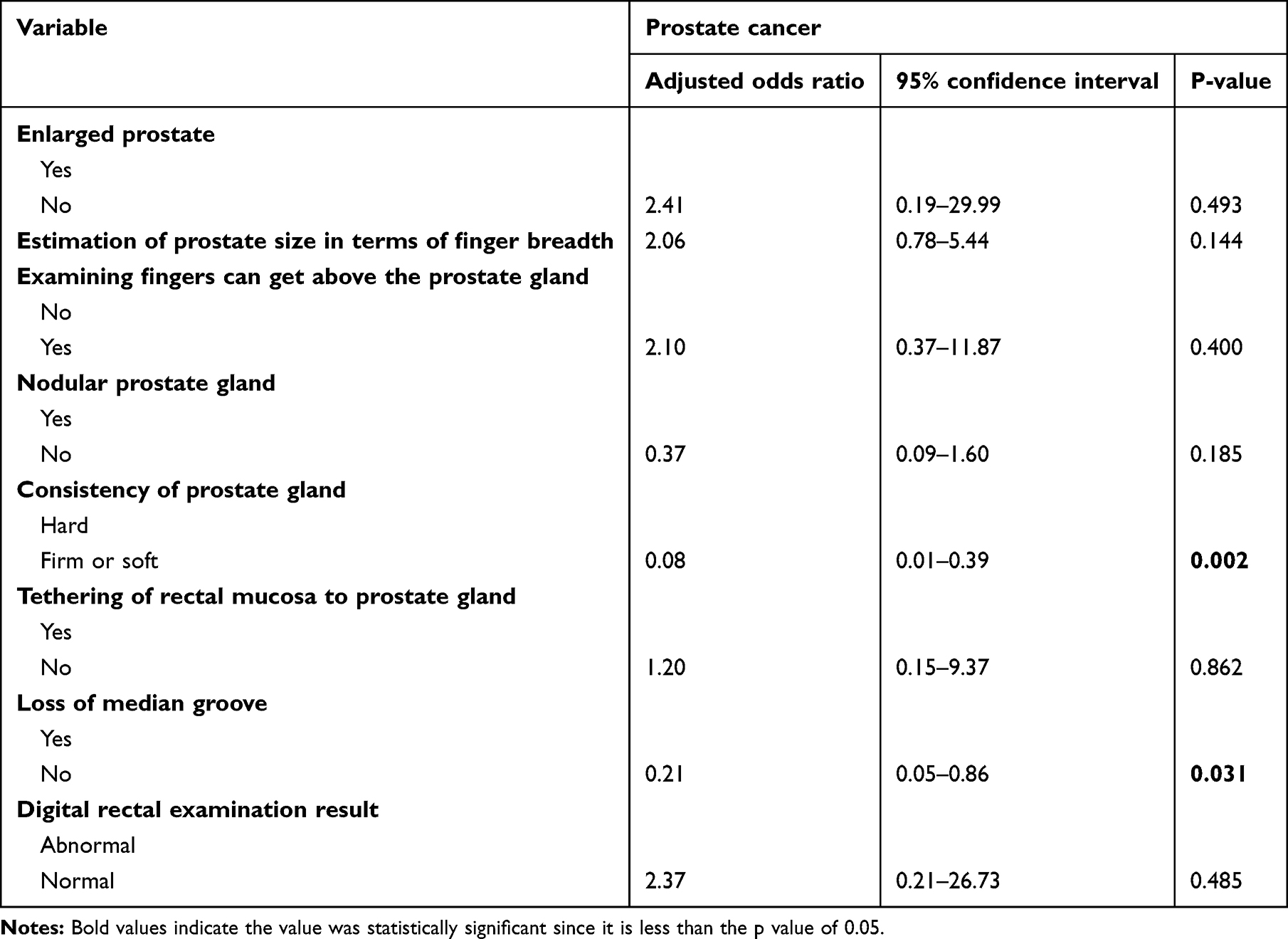 |
Table 5 Logistic Regression Analysis of Factors Associated with Prostate Cancer Among Patients Presenting with Obstructive Lower Urinary Tract Symptoms at Mbarara Regional Referral Hospital |
The factors associated with prostate cancer include consistency of the prostate, that is, having a firm or soft prostate meant being less likely to have prostate cancer than having a hard prostate (OR: 0.08; 95% CI: 0.01–0.39, P = 0.002) and loss of the median groove (OR: 0.21; 95% CI: 0.05–0.86; P = 0.031).
Discussion
Several pieces of recent scientific evidence continue to reveal conflicting results on the association between prostate cancer and LUTS. This, coupled with lack of a global consensus on screening and testing for prostate cancer among men, has resulted in the largely reported late presentation with advanced disease that is only amenable to palliative care and thus results in high mortality. Our study setting faces the same challenges whereby clinicians have no option but to initiate testing only when patients present with unrelated lower urinary symptoms. In this study we present data from hospital-based patients with LUTS as the main presenting complaint who are subjected to testing for prostate cancer diagnosis.
The majority of our participants presented with severe LUTS, which is in contrast to studies conducted in high-income countries20,25–27 and community-based studies revealing higher rates for mild LUTS. One community-based study of LUTS among Ugandan males aged 55 years and above estimated that 40.5% of males suffer from moderate LUTS while only 1% have severe LUTS.21 Hospital-based studies and some low-income country studies had similar results with the majority of patients presenting with severe LUTS.14,28,29 This might be explained by the ascertainment bias that is inherent to hospital-based study designs; however, in settings similar to ours, where the majority of participants are peasant farmers, poor health-seeking behavior and limited access to health care29,30 could be plausible explanations for this observed trend, whereby patients present with symptomatic advanced disease.12,31,32
In our study, severity of LUTS was not a determinant of eligibility for undergoing a tru-cut prostate biopsy, as guided by the NICE guidelines. However, patients with severe LUTS were more likely to qualify for a tru-cut prostate biopsy (Fisher’s exact test = 0.001) and this is in agreement with the 2018 NICE recommendation to test symptomatic patients with raised PSA levels.33
The majority of our participants were aged between 61 to 70 years (32.86%, 46/140), with mean ages of 69.8 and 72 for the entire study population and those who qualified for tru-cut prostate biopsy, respectively. This age group encompasses the currently globally accepted mean age of 68 for diagnosis of prostate cancer34 and is similar to that reported by other studies: 69.8 in Nigeria,31 62–72 in a systematic review of localized prostate cancer as reported by different African studies,32 and 69.5 by the Uganda Cancer Institute.12 This age also coincides with the commonest age at presentation with LUTS.21,30 Unlike other studies that have found a positive correlation between age and incidence of prostate cancer,35 we did not find any statistically significant relationship between age and the presence of prostate cancer. Unlike most studies,36 for our study population, age did not show any statistically significant positive relationship with a prostate cancer diagnosis; however, similar to other studies, serum total PSA showed a fairly strong positive (r = 0.4114, P<0.001) correlation with age. We did not come across any other study that assessed the relationship between age and risk of prostate cancer diagnosis in clusters of patients with LUT. However, the observed increase in PSA with age has also been confirmed by other studies and is largely attributed to the age-related increase in prostate size with age and associated increase in the amount of glandular tissues secreting PSA.37,38
The median PSA was 14.3 ng/mL, and the majority of participants (71% 99/140) had TPSA values above 4 ng/mL. We did not find any local or continental studies that had specifically profiled PSA among patients with LUTS. However, retrospective sub-Saharan studies conducted with already confirmed prostate cancer cases to determine the commonest presenting complaints, and also ascertain PSA patterns, revealed higher mean PSA values (91.3 ng/mL12 in Kampala, Uganda, and 92.6– 96 ng/mL in Nigeria).14,16,29 The lowest values of PSA and rates of abnormal PSA values were reported from community-based studies: 2.6 ng/mL in Brazil, 1.46 ng/mL amongst healthy males at a community Nigerian hospital,39 and 9.4 ng/mL in Olmsted County, Minnesota.40 All of these community studies had concurrently lower prostate biopsy rates, and comparison of their outcomes supports our finding that patients presenting to our hospital with LUTS are more likely (Fisher’s exact test = 0.001) to meet the NICE 2018 criteria for testing than those in the community, who are mostly asymptomatic.
With these low biopsy eligibility rates from community studies coupled with low detection rates of indolent prostatic cancers, it is not a surprise that screening has been found to minimally reduce disease-specific mortality but not overall mortality.41
Abnormalities on DRE were very common among our study participants (57.14%), with the commonest abnormality being prostatic enlargement (54.29%). This concurs with a cross-sectional study in Ireland that assessed the clinical relevance of digital rectal examination in general medical and urology clinics: abnormalities in digital rectal examination were found in over 67% of participants.42 Chiang et al found that approximately a third of men 50 years and older will have some DRE findings that are due to prostate pathology,43 and a Nepalese hospital-based study assessing the relationship between LUTS and BPH found that 47.1% of DREs were abnormal. 44 A West African study on the prevalence of LUTS also found a higher rate: 62.3%.45 In contrast, community-based studies on largely asymptomatic males found lower rates of DRE abnormalities: a multicenter trial of 6630 men found abnormal DRE rates at 15%46 and 29% in Trinidad and Tobago.36 The discrepancy highlighted by these contrasting studies supports the NICE guidelines to assess for additional signs among symptomatic patients who are at risk of developing prostate cancer.33 However, they also support the fact that there is still late presentation with symptoms of locally advanced disease. The relevancy of a well-performed digital rectal examination has, however, already been supported by results from autopsy studies revealing that 70% of cases of prostate cancer show local extension, which is likely to be detected during DRE.47,48
Among the patients who underwent a digitally guided transrectal tru-cut biopsy, the positivity rate for prostate cancer was 46% (45/99). This was higher than that reported by most studies that did not consider the presence of LUTS as a major determinant in the denominator.
Community-based studies in which LUTS were not part of the participant selection procedure revealed lower rates of prostate cancer. A Brazilian meta-analysis of 12 studies comparing the prevalence of prostate cancer among African and Caucasian men revealed an overall prevalence of prostate cancer in 9.6% of black men and 5.6% of white men.49 A Caribbean screening study of men aged 40–79 years who did not have LUTS also found a lower prevalence at 10.7%.50
A studyconducted in a hospital setting or on patients with LUTS revealed a comparably higher prostate cancer detection rate at Jos University, Nigeria (19.4%)51, and a Stockholm3 study found a rate of 39.2%. Despite the high rate found by the Stockholm3 study, it did not reveal any statistically significant relationship between presence or severity of prostate cancer and severity of LUTS. This is in accordance with other studies that have not found any significant relation between LUTS and prostate cancer diagnosis.25,52,53 Ørsted et al,54 on the other hand, presented a very large observational study of more than 3 million men in Denmark and revealed that men with LUTS had an increased risk of prostate cancer (HR 2.2; 95% CI: 2.13–2.31) over a follow-up period of 27 years. A Norwegian study of about 30,000 men also found an increased risk of detecting prostate cancer in men with severe LUTS (HR 4.6; 95% CI: 2.23–9.54).55 Okidi et al, at Lacor Hospital in northern Uganda, concluded that LUTS were associated with an increased risk of prostate cancer.56 The few studies which identified a clinically significant relation were found to have only assessed the presence or absence of LUTS rather than their severity or to have used retrospective data that most likely suffered from ascertainment bias.54
It is recognized that cancer most often develops in the peripheral zone, which is at some distance from the urethra and indicates a reduced likelihood of obstruction of urinary flow57 unless it is locally advanced or associated with age-related benign enlargement. The results of our study do not support a positive association between LUTS and prostate cancer and therefore also make anatomical sense.
In our studyr having abnormalities on DRE carried a significantly increased risk of having prostate cancer (Risk ratio = 5.895; 95% CI: 1.59–21.822; Fisher’s exact test = 0.04). Prostatic abnormalities have been shown to have high sensitivity, specificity and positive predictive values by very many studies. Nnamdi Azikiwe University in Nigeria found an overall diagnostic accuracy of 72.6%. A systematic review conducted by a team at Hull University in the UK revealed that abnormal DRE meant a 42.3% chance of prostate malignancy.58 In Rwanda, the risk was found to be even higher (92%) compared to 41.7% among those who had normal DRE findings.59 These studies were largely conducted on patients who had never presented with LUTS. These findings, together with those from our study, support the fact that abnormal DRE findings are likely to make good predictors and therefore screening tools for prostate cancer compared to LUTs,60 especially in communities where PSA measuring is not readily accessible. The anatomical origin of prostate cancer suggests that malignant lesions57 are likely to be palpated early in the disease process, long before they progress to involve the transitional zone and therefore cause LUTS that clinicians largely rely on to test for prostate cancer.61 However studies to ascertain the specific signs that are more likely to be related to prostate cancer diagnosis and the staging of cancer at diagnosis will be relevant in assessing whether screening with DRE is expected to have any impact on disease-specific and overall mortality which serum PSA has partially demonstrated.
The only histological subtype of prostate cancer found among our study population was adenocarcinoma. Other rare histological patterns that account for 5–10% of the carcinomas that originate from the prostate, like small cell, ductal adenocarcinoma, sarcomatoid, basal cell, squamous cell, adenosquamous (ASC), and urothelial carcinoma,62,63 were not found among any of our participants.
Most African and Ugandan studies found almost 100% adenocarcinoma in their histological specimens.12,14 A retrospective re-examination of prostate specimens collected between 1994 and 2004 at the University of Calabar Teaching Hospital, Nigeria also revealed that 99% of cases had adenocarcinoma); only one had a mesenchymal tumor (rhabdomyosarcoma; 1%).64 This could mean that the prevalence of other rare histological subtypes of prostate cancer is much more unlikely among men of black descent; however, further evaluation with different study designs and higher sample sizes is still needed to verify this.
The mean Gleason score was high at 8. When individual scores were clustered into three risk categories, the majority of patients who had prostate cancer (35/45, 77.78%) had Gleason scores above 8, which means that most had a high risk of poorly differentiated cancer that was most likely incurable or presented too late and was now advanced. This was a higher score than that detected by Oluwole et al in a 10-year retrospective review of 151 cases at Ahmadu Bello University Teaching Hospital in Zaria, Nigeria; here, 51.6% of cancers were poorly differentiated and 58.4% were moderately differentiated or presented a moderate risk.65
Yahaya’s study conducted at Mulago Mulago National Refferal Hospital in Uganda in 2019 also revealed that a significant proportion of his patients (44.6%) had a Gleason score of ≥ 8.14 However, this was still lower than that found in our study.
A South African study published in 2014 revealed that black South Africans presented with significantly more aggressive disease as defined by a Gleason score of > 7. It also found poorly differentiated tumor grades within rural versus urban localities.66 Okuku conducted a retrospective review at Makerere University in Uganda and found that 66.7% of of specimens had a high-risk disease, with a Gleason score of 9 or 10.12
The higher rates of prostate cancer we observed could not be explained by the fact that our patients presented with symptoms of locally advanced disease, as we did not find any statistically significant relationship between severity of LUTS and Gleason risk grade. However, our results, in addition to those of other studies conducted with black participants, suggest and are in agreement with findings that African men, in contrast to white men, are likely to present with aggressive poorly differentiated prostate cancer.35 African men, as a result of high testosterone levels and genetic predisposition, are more likely to develop highly aggressive rapidly progressing prostate cancer.35
Limitations
The limitations of this study are as follows: (1) we used digitally guided transrectal prostate biopsy, which is less sensitive than transrectal ultrasound guided biopsy; (2) we were unable to assess other tests, such as PSA kinetics, that have already been found to have higher sensitivity than conventional total serum PSA; (3) ascertainment bias was likely as the study was conducted in a hospital setting with symptomatic patients; and (4) the small sample size reduced the power of our study.
Conclusions
There was a high rate of severe LUTS among patients presenting at the OPD with these symptoms. These are likely to qualify for a tru-cut prostate biopsy and should be assessed for suitability to undergo this procedure.
Patients with LUTS have higher median PSA values, higher rates of DRE abnormalities and prostate cancer. However, there was no statistically significant relationship between severity of LUTS and either a diagnosis of prostate cancer or a high Gleason score.
The increased risk of prostate cancer among patients with DRE abnormalities makes DRE an appropriate and low cost substitute for screening in areas where PSA testing is not accessible.
High risk adenocarcinoma was the commonest type of malignancy among patients attending OPD with LUTS.
Further studies into the staging of disease at presentation and treatment will be useful in guiding the equitable distribution of resources for treatment of this condition.
Data Sharing Statement
All relevant data are provided within this article and its supporting information files. Data are available upon reasonable request from the first author.
Acknowledgment
Special appreciation to Dr Kirya Musa and Dr Otim Paul of Soroti University Department of Surgery for their insightful inputs during writing of this article.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interest.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000. The global picture. Eur J Cancer. 2001;37:4–66.
3. Zhou CK, Check DP, Lortet-Tieulent J, et al. Prostate cancer incidence in 43 populations worldwide: an analysis of time trends overall and by age group. Int J Cancer. 2016;138(6):1388–1400. doi:10.1002/ijc.29894
4. Mahdavifar N, Mohammadian M, Ghoncheh M, Salehiniya H. Pancreatic cancer in the world: an epidemiological review. World Cancer Res J. 2018;5(10).
5. Adeloye D, David RA, Aderemi AV, et al. An estimate of the incidence of prostate cancer in Africa: a systematic review and meta-analysis. PLoS One. 2016;11(4):e0153496. doi:10.1371/journal.pone.0153496
6. Seraphin TP, Joko-Fru WY, Kamaté B, et al. Rising prostate cancer incidence in Sub-Saharan Africa: a trend analysis of data from the African cancer registry network. Cancer Epidemiol Biomarkers Prev. 2021;30(1):158–165. doi:10.1158/1055-9965.EPI-20-1005
7. Chu LW, Ritchey J, Devesa SS, Quraishi SM, Zhang H, Hsing AW. Prostate cancer incidence rates in Africa. Prostate Cancer. 2011;2011(1):947870. doi:10.1155/2011/947870
8. Parkin EDM, Ferlay J, Jemal A, et al. IARC Scientific Publications – no. 167.
9. Parkin DM, Nambooze S, Wabwire‐Mangen F, Wabinga HR. Changing cancer incidence in Kampala, Uganda, 1991–2006. Int J Cancer. 2010;126(5):1187–1195. doi:10.1002/ijc.24838
10. Rebbeck TR, Haas G. Temporal trends and racial disparities in global prostate cancer prevalence. Can J Urol. 2014;21(5):7496–7506.
11. Bukirwa P, Wabinga H, Nambooze S, et al. Trends in the incidence of cancer in Kampala, Uganda, 1991 to 2015. Int J Cancer. 2021;148(9):2129–2138. doi:10.1002/ijc.33373
12. Okuku F, Orem J, Holoya G, De Boer C, Thompson CL, Cooney MM. Prostate cancer burden at the Uganda cancer institute. J Glob Oncol. 2016;2(4):181–185. doi:10.1200/JGO.2015.001040
13. Gondos A, Brenner H, Wabinga H, Parkin DM. Cancer survival in Kampala, Uganda. Br J Cancer. 2005;92(9):1808–1812. doi:10.1038/sj.bjc.6602540
14. Yahaya JJ. Clinical and histopathological profile of patients with prostate cancer in Kampala, Uganda. Med J Zambia. 2019;46(1):19–27. doi:10.55320/mjz.46.1.219
15. Ikuerowo SO, Omisanjo OA, Bioku MJ, Ajala MO, Mordi VPN, Esho JO. Prevalence and characteristics of prostate cancer among participants of a communitybased screening in Nigeria using serum prostate specific antigen and digital rectal examination. Pan Afr Med J. 2013;15(1). doi:10.11604/pamj.2013.15.129.2489
16. Nwofor AME, Oranusi CK. Cancer of the prostate: experience at Nnewi, Southeast, Nigeria. Niger J Clin Pract. 2004;7(2):65–68.
17. Hamilton W, Sharp D. Symptomatic diagnosis of prostate cancer in primary care: a structured review. Br J Gen Pract. 2004;54(505):617–621.
18. Chavan PR, Chavan SV, Chavan NR, Trivedi VD. Detection rate of prostate cancer using prostate specific antigen in patients presenting with lower urinary tract symptoms: a retrospective study. J Postgrad Med. 2009;55(1):17. doi:10.4103/0022-3859.43548
19. Jones D, Friend C, Dreher A, Allgar V, Macleod U. The diagnostic test accuracy of rectal examination for prostate cancer diagnosis in symptomatic patients: a systematic review. BMC Fam Pract. 2018;19(1):79. doi:10.1186/s12875-018-0765-y
20. Chandra Engel J, Palsdottir T, Aly M, et al. Lower urinary tract symptoms (LUTS) are not associated with an increased risk of prostate cancer in men 50–69 years with PSA ≥3 ng/mL. Scand J Urol. 2020;54(1):1–6. doi:10.1080/21681805.2019.1703806
21. Bajunirwe F, Stothers L, Berkowitz J, Macnab AJ. Prevalence estimates for lower urinary tract symptom severity among men in Uganda and sub-Saharan Africa based on regional prevalence data. Can Urol Assoc J. 2018;12(11):E447–52. doi:10.5489/cuaj.5105
22. Katongole P, Sande OJ, Yusuf M, et al. Clinical characteristics and primary management of patients diagnosed with prostate cancer between 2015 and 2019 at the Uganda Cancer Institute. PLoS One. 2020. doi:10.1371/journal.pone.0236458
23. Mason RJ, Marzouk K, Finelli A, et al. UPDATE – 2022 Canadian Urological Association recommendations on prostate cancer screening and early diagnosis. Can Urol Assoc J. 2022;16(4):E184–96. doi:10.5489/cuaj.7851
24. Mottet N, Bellmunt J, Bolla M, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71(4):618–629. doi:10.1016/j.eururo.2016.08.003
25. Al-Zubaidi M, Hawks C, Fernando S, et al. Relationship between lower urinary tract symptoms (LUTS) and prostate cancer: a persistent myth. J Clin Urol. 2023:20514158231170420.
26. Speakman M, Kirby R, Doyle S, Ioannou C. Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH) – focus on the UK. BJU Int. 2015;115(4):508–519. doi:10.1111/bju.12745
27. Huang J, Chan CK, Yee S, et al. Global burden and temporal trends of lower urinary tract symptoms: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2023;26(2):421–428. doi:10.1038/s41391-022-00610-w
28. Asare GA, Sule DS, Oblitey JN, et al. High degree of prostate related LUTS in a prospective cross-sectional community study in Ghana (Mamprobi). Heliyon. 2021;7(11):e08391. doi:10.1016/j.heliyon.2021.e08391
29. Okeke CJ, Obi AO, Ojewola RW, et al. Prostate cancer and challenges in management in a semi-urban centre: a 10-year experience. J West Afr Coll Surg. 2022;12(3):44–48. doi:10.4103/jwas.jwas_140_22
30. Stothers L, Macnab AJ, Bajunirwe F, Mutabazi S, Berkowitz J. Associations between the severity of obstructive lower urinary tract symptoms and care-seeking behavior in rural Africa: a cross-sectional survey from Uganda. PLoS One. 2017;12(3):e0173631. doi:10.1371/journal.pone.0173631
31. Ugwumba FO, Nnabugwu II. Prostate cancer characteristics: a descriptive analysis of clinical features at presentation in the last decade in a black African community. Ann Afr Med. 2022;21(2):153. doi:10.4103/aam.aam_101_20
32. Cassell A, Yunusa B, Jalloh M, et al. A review of localized prostate cancer: an African perspective. World J Oncol. 2019;10(4–5):162–168. doi:10.14740/wjon1221
33. Recommendations | Prostate cancer: diagnosis and management | guidance | NICE [Internet]. NICE; 2019 [cited July 14, 2024]. Available from: https://www.nice.org.uk/guidance/ng131/chapter/Recommendations#assessment-and-diagnosis.
34. Gupta S, Gupta A, Saini AK, Majumder K, Sinha K, Chahal A. Prostate cancer: how young is too young? Curr Urol. 2015;9(4):212–215. doi:10.1159/000447143
35. Rawla P. Epidemiology of Prostate Cancer. World J Oncol. 2019;10(2):63–89. doi:10.14740/wjon1191
36. Bunker CH, Patrick AL, Maharaj G, et al. Prostate cancer risk is three-fold higher among men, aged 50–64, of African descent compared with men of Asian-Indian descent in Trinidad and Tobago. Ethn Dis. 2002;12(4):30–33.
37. Balk SP, Ko YJ, Bubley GJ. Biology of prostate-specific antigen. J Clin Oncol. 2003;21(2):383–391. doi:10.1200/JCO.2003.02.083
38. Putra IBOW, Hamid ARAH, Mochtar CA, Umbas R. Relationship of age, prostate-specific antigen, and prostate volume in Indonesian men with benign prostatic hyperplasia. Prostate Int. 2016;4(2):43–48. doi:10.1016/j.prnil.2016.03.002
39. Aisuodionoe-Shadrach OI, Eniola SB, Nwegbu MM, Kolade-Yunusa HO, Okereke OO, Yunusa T. Determination of serum prostate specific antigen levels amongst apparently healthy Nigerian males in a university and university hospital community in the federal capital territory. Cancer Control. 2022;29:10732748221081366. doi:10.1177/10732748221081366
40. Jacobsen SJ, Bergstralh EJ, Guess HA, et al. Predictive properties of serum prostate-specific antigen testing in a community-based setting. Arch Intern Med. 1996;156(21):2462–2468. doi:10.1001/archinte.1996.00440200080010
41. Ilic D, Djulbegovic M, Jung JH, et al. Prostate cancer screening with prostate-specific antigen (PSA) test: a systematic review and meta-analysis. BMJ. 2018;362:k3519. doi:10.1136/bmj.k3519
42. Walsh AL, Considine SW, Thomas AZ, Lynch TH, Manecksha RP. Digital rectal examination in primary care is important for early detection of prostate cancer: a retrospective cohort analysis study. Br J Gen Pract. 2014;64(629):e783–7. doi:10.3399/bjgp14X682861
43. Chiang PPC, Glance D, Walker J, Walter FM, Emery JD. Implementing a QCancer risk tool into general practice consultations: an exploratory study using simulated consultations with Australian general practitioners. Br J Cancer. 2015;112(1):S77–83. doi:10.1038/bjc.2015.46
44. Raya A, Bhatta P, Sah S, Aryal V. Lower urinary tract symptoms, serum PSA, digital rectal examination and prostate volume in patients presenting to urology department: a cross-sectional study. J Inst Med Nepal. 2022;44(2):53–55. doi:10.59779/jiomnepal.1225
45. Chokkalingam AP, Yeboah ED, DeMarzo A, et al. Prevalence of BPH and lower urinary tract symptoms in West Africans. Prostate Cancer Prostatic Dis. 2012;15(2):170–176. doi:10.1038/pcan.2011.43
46. Catalona WJ, Richie JP, Ahmann FR, et al. Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J Urol. 2017;197. doi:10.1016/j.juro.2016.10.073
47. Walker HK, Hall WD, Hurst JW, editors.. Clinical Methods: The History, Physical, and Laboratory Examinations.
48. Jahn JL, Giovannucci EL, Stampfer MJ. The high prevalence of undiagnosed prostate cancer at autopsy: implications for epidemiology and treatment of prostate cancer in the Prostate-specific Antigen-era. Int J Cancer. 2015;137(12):2795–2802. doi:10.1002/ijc.29408
49. Romero FR, Romero AW, Almeida RM, Tambara Filho R. The prevalence of prostate cancer in Brazil is higher in Black men than in White men: systematic review and meta-analysis. Int Braz J urol. 2012;38:440–447. doi:10.1590/S1677-55382012000400002
50. Bunker CH, Patrick AL, Miljkovic-Gacic I, et al. Prostate cancer screening parameters in a high-risk African-Caribbean population. Urology. 2004;63(4):737–741. doi:10.1016/j.urology.2003.10.064
51. Mattiuzzi C, Lippi G. Current Cancer Epidemiology. J Epidemiol Glob Health. 2019;9(4):217. doi:10.2991/jegh.k.191008.001
52. Bhindi A, Bhindi B, Kulkarni GS, et al. Modern-day prostate cancer is not meaningfully associated with lower urinary tract symptoms: analysis of a propensity score-matched cohort. Can Urol Assoc J. 2017;11(1–2):41–46. doi:10.5489/cuaj.4031
53. Cicione A, Cormio L, Cantiello F, et al. Presence and severity of lower urinary tract symptoms are inversely correlated with the risk of prostate cancer on prostate biopsy. 2017 [cited July 22, 2024]. Available from: https://repositorium.sdum.uminho.pt/handle/1822/48480.
54. Ørsted DD, Bojesen SE, Nielsen SF, Nordestgaard BG. Association of clinical benign prostate hyperplasia with prostate cancer incidence and mortality revisited: a Nationwide Cohort Study of 3 009 258 men. Eur Urol. 2011;60(4):691–698. doi:10.1016/j.eururo.2011.06.016
55. Martin RM, Vatten L, Gunnell D, Romundstad P, Nilsen TIL. Lower urinary tract symptoms and risk of prostate cancer: the HUNT 2 Cohort, Norway. Int J Cancer. 2008;123(8):1924–1928. doi:10.1002/ijc.23713
56. Okidi R, Opira C, Sambo VDC, Achola C, Ogwang DM. Prostate hyperplasia in St Mary’s Hospital Lacor: utility of prostate specific antigen in screening for prostate malignancy. Afr Health Sci. 2020;20(3):1259–1263. doi:10.4314/ahs.v20i3.30
57. Ali A, Du Feu A, Oliveira P, Choudhury A, Bristow RG, Baena E. Prostate zones and cancer: lost in transition? Nat Rev Urol. 2022;19(2):101–115. doi:10.1038/s41585-021-00524-7
58. Mbaeri TU, Nwadi U, Abiahu JA, Orakwe JC, Okoli C. Correlation between prostate specific antigen, digital rectal examination and histology in patients with prostate cance. Niger J Med. 2018;27(3):212. doi:10.4103/1115-2613.278783
59. Nzeyimana I, Nyirimodoka A, Ngendahayo E, et al. Diagnosis of advanced prostate cancer at the community level in Rwanda. Int Urol Nephrol. 2021;53(10):1977–1985. doi:10.1007/s11255-021-02921-8
60. Mistry K, Cable G. Meta-analysis of prostate-specific antigen and digital rectal examination as screening tests for prostate carcinoma. J Am Board Fam Pract. 2003;16(2):95–101. doi:10.3122/jabfm.16.2.95
61. Welliver C, Feinstein L, Ward JB, et al. Poor clinical guideline adherence and inappropriate testing for incident lower urinary tract symptoms associated with benign prostatic hyperplasia. Prostate Cancer Prostatic Dis. 2022;25(2):269–273. doi:10.1038/s41391-021-00435-z
62. Dema S, Dema ALC, Tăban S, et al. Prostate carcinomas mimicking a digestive malignancy. Rom J Morphol Embryol. 2020;61(3):751–758. doi:10.47162/RJME.61.3.13
63. Aktaş S, Köseoğlu H, Yucetas U, Koca S. Histopathological variant types diagnosed in prostate surgery. Ann Urol Oncol. 2020;3:47–53. doi:10.32948/auo.2020.12.30
64. Ugare UG, Bassey IE, Jibrin PG, Ekanem IA. Analysis of Gleason grade and scores in 90 Nigerian Africans with prostate cancer during the period 1994 to 2004. Afr Health Sci. 2012;12(1):69–73.
65. Oluwole OP, Rafindadi AH, Shehu MS, Samaila MOA. A ten-year study of prostate cancer specimens at Ahmadu Bello University Teaching Hospital (A.B.U.T.H), Zaria, Nigeria. Afr J Urol. 2015;21(1):15–18. doi:10.1016/j.afju.2014.09.004
66. Tindall EA, Monare LR, Petersen DC, et al. Clinical presentation of prostate cancer in black South Africans. Prostate. 2014;74(8):880–891. doi:10.1002/pros.22806
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.