Back to Journals » Clinical Ophthalmology » Volume 13
Prospective evaluation of a novel silicone corneal shield after PRK: 6-month efficacy, safety, and predictability outcomes
Received 8 August 2018
Accepted for publication 24 November 2018
Published 7 January 2019 Volume 2019:13 Pages 115—121
DOI https://doi.org/10.2147/OPTH.S183120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Christopher S Sáles,1 Edward E Manche2
1Weill Cornell Medical College, Department of Ophthalmology, New York, NY, USA; 2Byers Eye Institute, Department of Ophthalmology, Stanford University School of Medicine, Palo Alto, CA, USA
Purpose: The aim of this study was to report the 1-week and 6-month refractive outcomes of eyes treated with a novel silicone corneal shield designed to improve visual recovery after photorefractive keratectomy (PRK).
Patients and methods: This prospective, observational clinical trial recruited 45 myopic eyes with or without astigmatism at a university eye clinic to undergo wavefront-guided PRK followed by application of an investigational silicone corneal shield that was removed on postoperative day 4. The primary outcome measures were efficacy, predictability, and safety at the 6-month visit. The secondary end points included short-term uncorrected distance visual acuity (UDVA) and pain.
Results: No adverse outcomes occurred using the device. At 6 months, 79.5% of eyes achieved UDVA >20/20, 94.9% achieved ≥20/25, and 97.4% achieved ≥20/40. Also, 2.6% lost one line of corrected distance visual acuity and none lost two lines; 71.8% and 97.4% measured within ±0.25 and ±0.50 D of emmetropia, respectively. During the first week, preoperative UDVA improved from 1.34 logarithm of the minimum angle of resolution (logMAR; <20/400 Snellen) to 0.14 logMAR (>20/30) on postoperative day 1 (P<0.0001) and remained stable on days 2–3 (all P>0.05). After removal of the shield on day 4, UDVA declined by two lines before rebounding to 0.16 logMAR (>20/30) on day 7 (both P<0.001). Subjective metrics of pain all peaked between days 2 and 3 before declining.
Conclusion: The investigational silicone corneal shield is safe and effective when used after PRK and may aid early visual recovery and patient comfort, but comparative studies are needed to validate these preliminary findings.
Precis: One-week and 6-month refractive outcomes of a novel silicone corneal shield used after PRK show that the device is not only safe and effective but may also speed visual recovery.
Keywords: PRK, contact lens, safety, wound healing
Introduction
Wavefront-guided photorefractive keratectomy (PRK) delivers efficacy, safety, and predictability that is equivalent to wavefront-guided LASIK.1 PRK offers the advantage of eliminating potential flap complications, but its major drawbacks are the morbidity associated with epithelial removal and the delay in visual recovery. Until now, there have been no significant advancements in how refractive surgeons manage the delay in visual recovery in the immediate postoperative period following PRK, when the epithelium is closing. The standard of care continues to be a silicone hydrogel soft bandage contact lens. This prospective, observational study reports the efficacy, safety, and predictability of an investigational silicone corneal shield designed to improve uncorrected distance visual acuity (UDVA) in the early postoperative period after PRK.
Patients and methods
The study was conducted at the Stanford Eye Laser Center after obtaining institutional review board approval from Stanford University. The investigational silicone device was registered with ClinicalTrials.gov (NCT01592643). All participants provided their written informed consent after full disclosure of the nature of the research. The study adhered to the tenets of the Declaration of Helsinki and the Health Insurance Portability and Accountability Act.
Inclusion criteria included stable refraction with a change of <0.50 D of sphere or cylinder in the last year and <11 D of myopia with <3.50 D of refractive astigmatism, best-corrected distance visual acuity ≥20/20, and age ≥18 years. Patients were excluded for use of rigid gas-permeable contact lenses, of if they had severe ocular surface disease, corneal dystrophy, irregular astigmatism, a difference of ≥0.75 D in sphere or ≥0.50 D in cylinder between the baseline manifest and cycloplegic refractions, history of herpetic eye disease, or corneal warpage (ie, contact lens-induced topographical abnormalities). Patients were also excluded for previous ocular surgery, glaucoma or preoperative intraocular pressure of ≥21 mmHg, and macular disease. Certain systemic diseases or conditions (ie, connective tissue disease, diabetes, pregnancy or lactation, immunocompromised state, and severe atopy) as well as sensitivity to the study’s medications and participation in a clinical trial for another ophthalmic drug or device were also grounds for exclusion.
Subjects underwent a comprehensive preoperative evaluation, including history, slit-lamp biomicroscopy, Goldmann applanation tonometry, dilated fundus examination, and manifest and cycloplegic refractions using Early Treatment Diabetic Retinopathy Study charts. Subjects also underwent testing with infrared pupilometry (Neuroptics, Irvine, CA, USA), computerized corneal topography, and wavefront aberrometry using the VISX WaveScan (Abbott Medical Optics, Santa Ana, CA, USA) with a physiologic pupil under controlled scotopic conditions in the same manner described in previous studies on wavefront-guided PRK.1–3
All surgeries were performed at the Stanford University Eye Laser Center by a single surgeon (EEM) in the same manner described in previous studies on wavefront-guided PRK.1–3 An epithelial scrubber (Amoils; Innovative Excimer Solutions, Inc., Toronto, ON, Canada) was used to remove the epithelium over an 8.0 mm zone centered on the pupil. The VISX CustomVue Star S4 IR excimer laser system (Abbott Medical Optics) was used to perform the treatments, which were targeted for full correction using the default 6 mm optical treatment zone and 8 mm blend zone. Adjunctive mitomycin C 0.02% was applied for 20 seconds in all cases.
The investigational silicone corneal shield was placed at the conclusion of the case and removed on postoperative day 4. Postoperatively, patients received topical moxifloxacin hydrochloride 0.5% (Alcon, Fort Worth, TX, USA) four times daily for 1 week and topical fluorometholone 0.1% (Allergan, Irvine, CA, USA) four times daily for 2 weeks followed by two times daily for 2 weeks before stopping. Subjects were evaluated at postoperative days 1, 2, 3, 4, and 7 as well as months 1, 3, and 6. Evaluations on day 4 were performed after removal of the silicone corneal shield.
The primary end points were efficacy, predictability, and safety. The secondary outcome measures included UDVA at days 1, 2, 3, 4 and 7, higher-order aberrations at the 6-month visit (ie, coma, trefoil, spherical aberration, and root mean square error), and pain. Pain was reported by the patient on an ordinal scale of 0–10 using a subjective questionnaire that was administered on days 1–7 and 30 for the variables of pain, discomfort, light sensitivity indoors, light sensitivity outdoors, foreign body sensation, burning, tearing, heavy eyelid, and dryness.
Statistical analyses were performed with a commercially available software package (SPSS for Mac, Version 20.0; IBM Corporation, Armonk, NY, USA). Comparisons of mean values were performed with the Wilcoxon signed rank test. Normal distribution of the preoperative and postoperative data was assessed by the Shapiro–Wilk test. All P-values were two-sided and considered statistically significant when <0.05.
Results
Forty-five eyes in 30 subjects were enrolled in the study (42% female, mean age 38.6 years; Table 1). Six eyes in four subjects were lost to follow-up at 6 months. Preoperative corrected distance visual acuity (CDVA) was better in the group lost to follow-up than the 39 eyes analyzed at 6 months by about half of an Early Treatment Diabetic Retinopathy Study line (−0.13 to −0.07 logarithm of the minimum angle of resolution [logMAR], P=0.04). Otherwise, there were no statistically significant differences in preoperative clinical parameters between the groups (ie, UDVA, manifest refraction, and higher-order aberrations; all P>0.05).
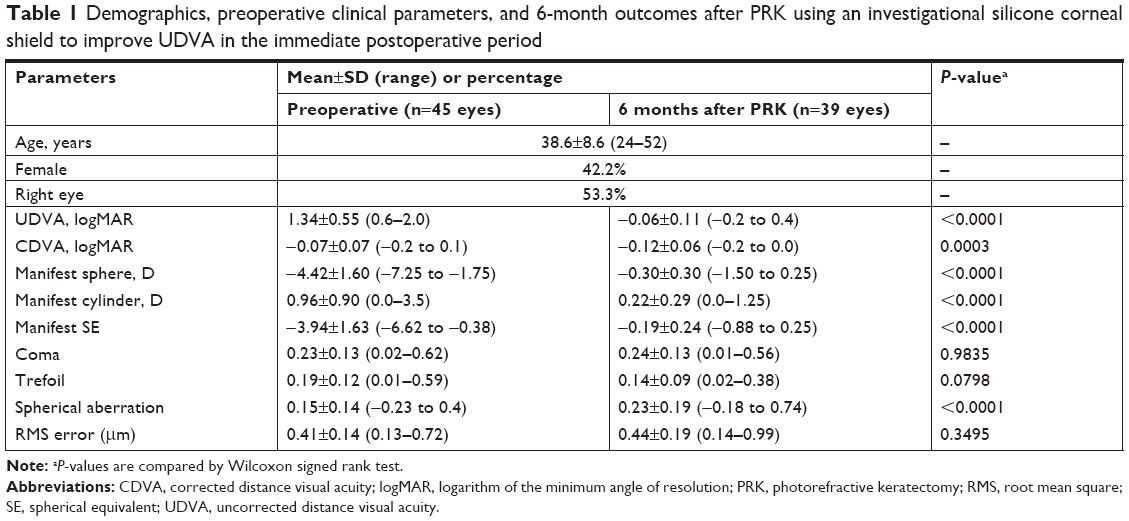 | Table 1 Demographics, preoperative clinical parameters, and 6-month outcomes after PRK using an investigational silicone corneal shield to improve UDVA in the immediate postoperative period |
Mean UDVA improved from 1.34±0.55 logMAR (range: 0.6–2.0) to −0.06±0.11 logMAR (range: −0.2 to 0.4) 6 months after PRK (P<0.0001). CDVA improved from −0.07±0.07 logMAR (range: −0.2 to 0.1) to −0.12±0.06 logMAR (range: −0.2 to 0.0) with P=0.0003. Manifest sphere improved from −4.42±1.60 D (range: −7.25 to −1.75) to −0.30±0.30 D (range: −1.50 to 0.25) with P<0.0001, and cylinder improved from 0.96±0.90 D (range: 0–3.50) to 0.22±0.29 D (range: 0–1.25) with P<0.0001. There were no statistically significant differences between preoperative and postoperative month 6 measurements of coma and root mean square (all P>0.05), but the mean spherical aberration increased by 0.08 (P<0.0001), and the mean trefoil decreased by 0.05, which trended toward but did not reach statistical significance (P=0.08), as shown in Table 1.
At 6 months, 31 eyes (79.5%) achieved UDVA of 20/20 or better, 94.9% achieved 20/25 or better, and 97.4% achieved 20/40 or better (Table 2; Figure 1A). One eye (2.6%) lost one line of CDVA, but none lost two lines at 6 months (Table 2; Figure 1B). Twenty-eight eyes (71.8%) measured within ±0.25 D of emmetropia and 97.4% measured within ±0.50 D of emmetropia at 6 months (Table 2; Figure 1C and D). Ninety percent and 97% of eyes achieved ≤0.50 and ≤1.00 D of astigmatism, respectively, at 6 months (Figure 1E). Spherical equivalent remained stable between postoperative months 3 and 6 (Figure 1F).
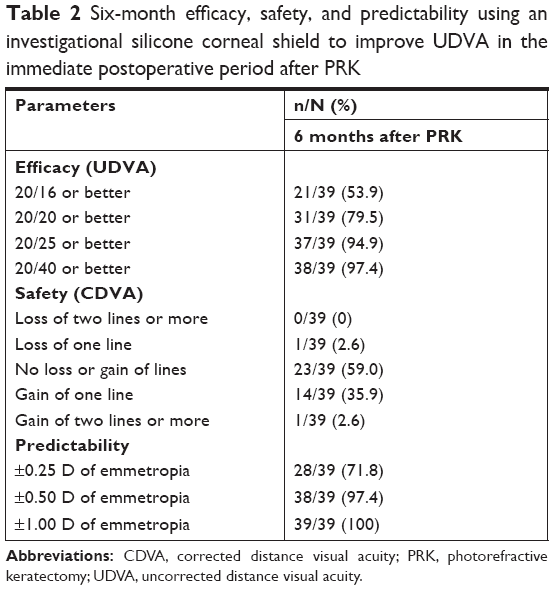 | Table 2 Six-month efficacy, safety, and predictability using an investigational silicone corneal shield to improve UDVA in the immediate postoperative period after PRK |
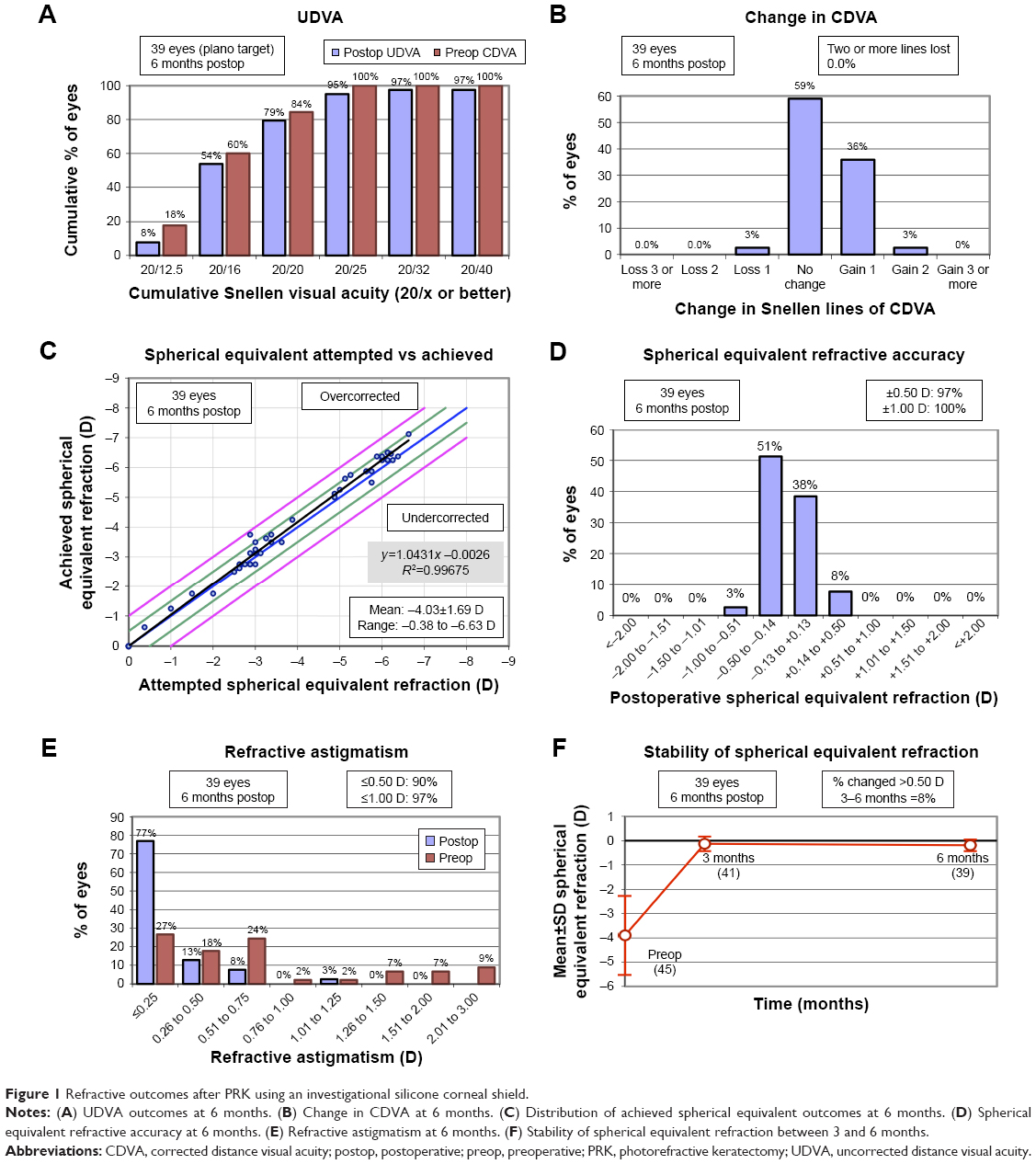 | Figure 1 Refractive outcomes after PRK using an investigational silicone corneal shield. |
In the immediate postoperative period, mean preoperative UDVA improved from 1.34 logMAR (worse than 20/400 Snellen) to 0.14 logMAR (better than 20/30) on postoperative day 1 (P<0.0001). UDVA remained stable on days 2 and 3, while the corneal shield remained in place (0.09 logMAR or about 20/25 and 0.16 logMAR or about 20/29, respectively; all P>0.05). After the corneal shield was removed on day 4, mean UDVA worsened by about two Snellen lines (P<0.001) before rebounding to 0.16 logMAR on day 7 (P<0.001). After 3 days without the shield, UDVA on day 7 was equivalent to UDVA prior to shield removal on day 3 (P=0.75; Figure 2). Except for day 4 (after shield removal), more than half of all eyes had UDVA of 20/25 or better during the first postoperative week. On day 4, 13% and 33% of eyes had UDVA of 20/25 and 20/40 or better, respectively (Figure 3).
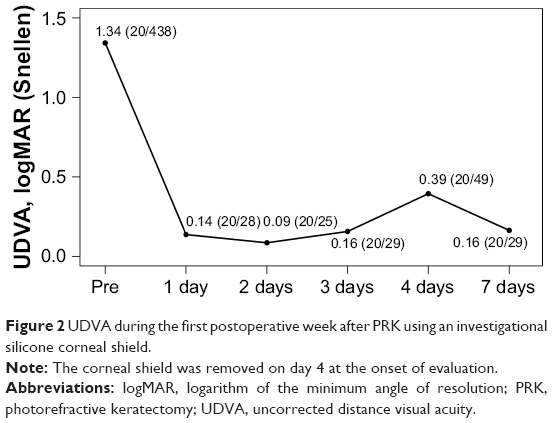 | Figure 2 UDVA during the first postoperative week after PRK using an investigational silicone corneal shield. |
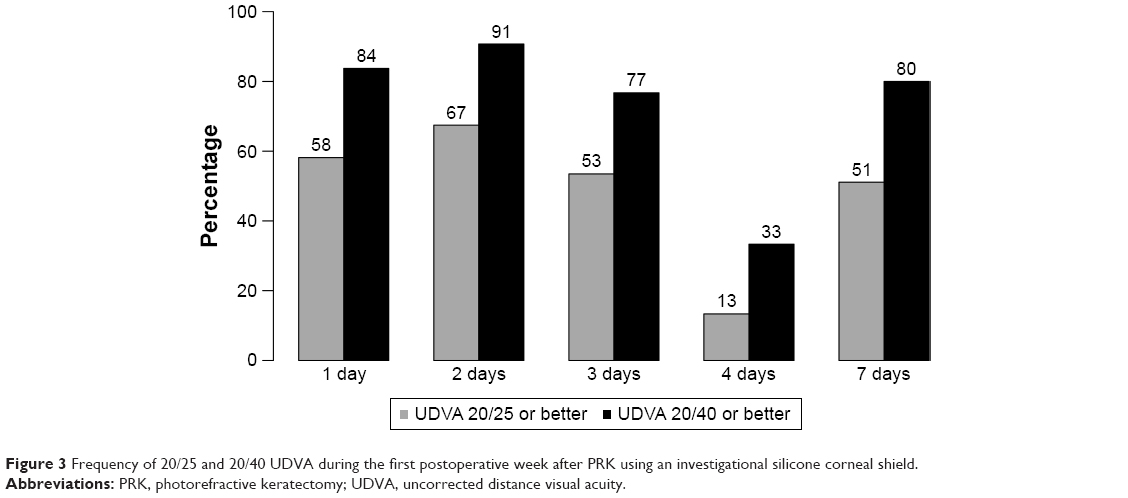 | Figure 3 Frequency of 20/25 and 20/40 UDVA during the first postoperative week after PRK using an investigational silicone corneal shield. |
Subjective assessments of pain, discomfort, light sensitivity indoors, light sensitivity outdoors, foreign body sensation, burning, tearing, heavy eyelid, and dryness all peaked on postoperative days 2 or 3 before declining. The metrics that exhibited the greatest and least change over the first week were light sensitivity outdoors and dryness, respectively (Figure 4).
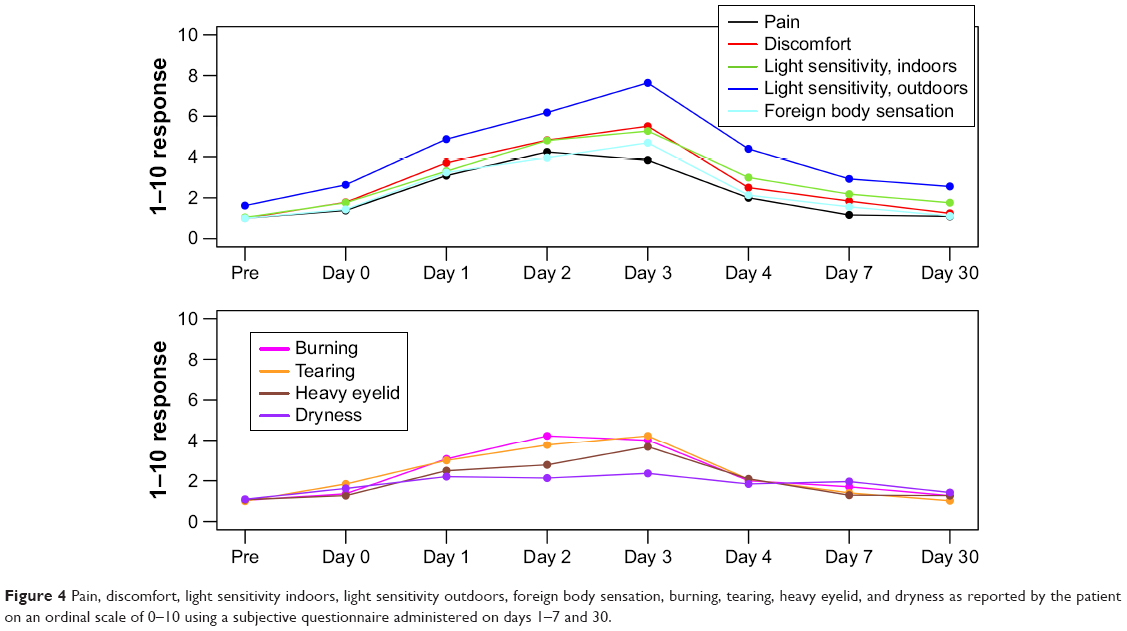 | Figure 4 Pain, discomfort, light sensitivity indoors, light sensitivity outdoors, foreign body sensation, burning, tearing, heavy eyelid, and dryness as reported by the patient on an ordinal scale of 0–10 using a subjective questionnaire administered on days 1–7 and 30. |
No adverse outcomes occurred using the investigational silicone corneal shield. No eyes had delayed epithelial healing or developed stromal haze in the immediate or late postoperative period, and no eyes experienced infectious or inflammatory keratitis, anterior chamber inflammation, or elevation in intraocular pressure.
Discussion
Visual recovery in the immediate postoperative period has been a topic of great interest to refractive surgeons since the introduction of PRK, which was supplanted by LASIK as the most pervasive refractive surgical procedure due at least in part to its slower visual recovery as well as its discomfort.
A number of techniques have been developed in an attempt to speed visual recovery after surface ablation, including but not limited to laser-assisted subepithelial keratectomy,4 epithelial laser in situ keratomileusis (epi-LASIK),5,6 and lamellar epithelial debridement.7 But the results have been mixed at best.8 Limited published data have shown that use of an epikeratome could be beneficial, with epi-LASIK offering marginal gains in efficacy over the first year9 and lamellar epithelial debridement providing better day 1 UDVA over PRK.7 However, neither of these methods has rivaled the popularity of PRK, and in addition, laser-assisted subepithelial keratectomy has never been shown to deliver better visual acuity than PRK, either.8
To the best of our knowledge, no one in the peer-reviewed literature has evaluated the use of a novel corneal shield to improve UDVA in the early postoperative period. The NexisVision (Menlo Park, CA, USA) corneal shield is a bi-modulus silicone elastomer material designed to provide rapid visual recovery to eyes treated with PRK (Figure 5). Its proprietary material is highly permeable to oxygen, especially overlying the limbal area, but impermeable to water, which aids in accelerating the resolution of corneal edema. The lens has a thin, soft periphery and a thicker, slightly stiffer central optic designed to improve vision during the early postoperative period. The corneal shield is sized according to each eye’s preoperative keratometric data.
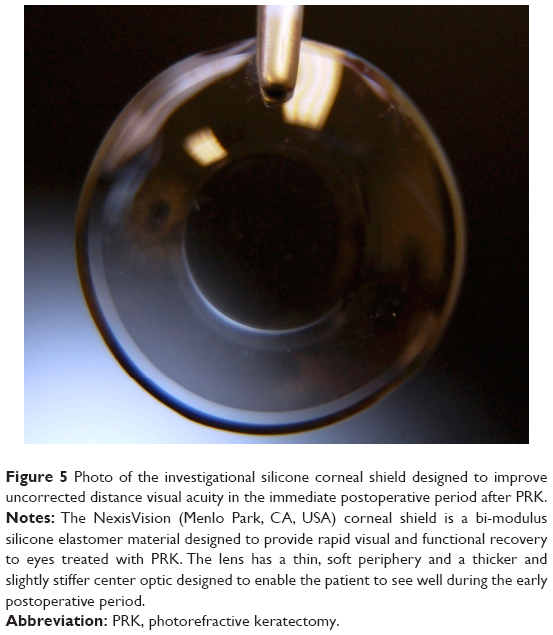 | Figure 5 Photo of the investigational silicone corneal shield designed to improve uncorrected distance visual acuity in the immediate postoperative period after PRK. |
In addition to showing that the silicone corneal shield delivers safe, effective, and predictable 6-month refractive outcomes, this study also exhibits promising 1-week UDVA results. To the best of our knowledge, there is only one study in the peer-reviewed literature that reports early postoperative UDVA after PRK with a standard-of-care contact lens. Kim et al reported UDVA on days 1, 3, and 7 in a retrospective comparison of epi-LASIK vs PRK in 2010. Fifty-four myopic eyes that underwent PRK in their study received a Focus 1–2 Week bandage contact lens (CIBA Vision, Duluth, GA, USA) until the epithelium closed. Mean closure time was 3.76 days.10
Comparisons, albeit limited, made between UDVA from the current study and data published by Kim et al suggest that the investigational silicone corneal shield might offer a slight advantage over a bandage contact lens early in the postoperative period. On day 1, Kim et al reported UDVA of 0.31 logMAR, or about 1.5 Snellen lines worse than our reported UDVA of 0.14 logMAR. On day 3, Kim et al reported UDVA of 0.19 logMAR, or about 0.5 lines worse than our reported UDVA of 0.16 logMAR. However, on day 7, Kim et al reported UDVA of 0.11 logMAR, or about 0.5 lines better than the 0.16 logMAR that we reported on day 7 (3 days after removal of the corneal shield).
The strengths of this study include its prospective design and use of a standardized technique for performing wavefront-guided PRK by an experienced refractive surgeon. Due to the study’s observational structure, no direct statistical comparisons can be made between the investigational device and a standard-of-care bandage contact lens with respect to visual recovery and pain.
Conclusion
We present the first prospective study of an investigational silicone corneal shield designed to aid visual recovery in the early postoperative period after PRK. Our results suggest that the device delivers safe and effective refractive outcomes, but a comparative study is needed to ascertain how it compares to a standard-of-care bandage contact lens after PRK with respect to vision, epithelial closure, and pain.
Data sharing statement
The authors do not intend to share individual de-identified personal data, which will not be made accessible. Study documents will not be made available, either.
Acknowledgments
The abstract of this paper was presented at the American Academy of Ophthalmology 2014 as a poster with interim findings. This research was partially supported by NexisVision, Menlo Park, CA, USA.
Disclosure
EEM reports: equity in Calhoun Vision, Inc., Seros Medical, LLC, and Veralas, Inc.; serves as a consultant for Best Doctors, Gerson Lehrman, Abbott Medical Optics, and Avellino Laboratories; and conducts sponsored research for Abbott Medical Optics, Avellino Laboratories, and Presbia. The authors report no other conflicts of interest in this work.
References
Manche EE, Haw WW. Wavefront-guided laser in situ keratomileusis (Lasik) versus wavefront-guided photorefractive keratectomy (Prk): a prospective randomized eye-to-eye comparison (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2011;109:201–220. | ||
He L, Manche EE. Contralateral eye-to-eye comparison of wavefront-guided and wavefront-optimized photorefractive keratectomy: a randomized clinical trial. JAMA Ophthalmol. 2015;133(1):51–59. | ||
He L, Manche EE. Prospective randomized contralateral eye evaluation of subjective quality of vision after wavefront-guided or wavefront-optimized photorefractive keratectomy. J Refract Surg. 2014;30(1):6–12. | ||
Camellin M. Laser epithelial keratomileusis for myopia. J Refract Surg. 2003;19(6):666–670. | ||
Pallikaris IG, Naoumidi II, Kalyvianaki MI, Katsanevaki VJ. Epi-LASIK: comparative histological evaluation of mechanical and alcohol-assisted epithelial separation. J Cataract Refract Surg. 2003;29(8):1496–1501. | ||
Partal AE, Rojas MC, Manche EE. Analysis of the efficacy, predictability, and safety of LASEK for myopia and myopic astigmatism using the Technolas 217 excimer laser. J Cataract Refract Surg. 2004;30(10):2138–2144. | ||
Youm DJ, Tchah H, Choi CY. Comparison of early postoperative clinical outcomes of photorefractive keratectomy and lamellar epithelial debridement. J Cataract Refract Surg. 2009;35(4):703–709. | ||
Reilly CD, Panday V, Lazos V, Mittelstaedt BR. PRK vs LASEK vs Epi-LASIK: a comparison of corneal haze, postoperative pain and visual recovery in moderate to high myopia. Nepal J Ophthalmol. 2010;2(2):97–104. | ||
Sia RK, Coe CD, Edwards JD, Ryan DS, Bower KS. Visual outcomes after Epi-LASIK and PRK for low and moderate myopia. J Refract Surg. 2012;28(1):65–71. | ||
Kim JH, Lee J, Kim JY, Tchah H. Early postoperative pain and visual outcomes following epipolis-laser in situ keratomileusis and photorefractive keratectomy. Korean J Ophthalmol. 2010;24(3):143–147. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.