Back to Journals » Clinical Optometry » Volume 17
Prospective Evaluation of a Novel Multifocal Toric Daily Disposable Contact Lens in Presbyopic Adults with Astigmatism
Authors Franklin R, Cannon-Hill JL, Sherrill R ![]() , Olivares GE
, Olivares GE
Received 23 April 2025
Accepted for publication 28 October 2025
Published 7 November 2025 Volume 2025:17 Pages 353—363
DOI https://doi.org/10.2147/OPTO.S536323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Ross Franklin, Jessica Lin Cannon-Hill, Ryan Sherrill, Giovanna E Olivares
Johnson & Johnson Vision Care, Inc., Jacksonville, FL, USA
Correspondence: Ross Franklin, Johnson & Johnson Vision Care, Inc., 7500 Centurion Pkwy, Ste 100, W2A, Jacksonville, FL, 32256, USA, Tel +19044431768, Fax +19044431783, Email [email protected]
Purpose: To evaluate the clinical performance of a novel multifocal toric contact lens design combining a pupil-optimized multifocal design with a blink stabilized toric design featuring a single cylinder power and a choice of 3 add powers in a group of presbyopic patients with low to moderate astigmatism.
Patients and Methods: A total of 171 subjects (105 myopic and 66 hyperopic) with refractive astigmatism of − 1.00 diopter (D) to − 1.75D with axes 90± 15 or 180± 15 degrees were fit with the study lenses in a two-week, multi-site prospective open-label clinical trial. The test lens was a multifocal toric soft contact lens with sphere powers of − 1.00D to − 4.00D and +1.00D to +4.50D, and a single cylinder power of − 1.00D with axes 90± 10 and 180± 10 degrees. Outcome measures included logMAR Visual Acuity, subjective assessments of vision, comfort and handling, and fit metrics including orientation, rotational stability and fit success.
Results: Over 96% of subjects were fit in the optimized lens power with 2 pairs of lenses or less. After 2-weeks of lens wear, the mean binocular high luminance high contrast (HLHC) logMAR visual acuities were − 0.085, − 0.023, and 0.083, for distance (4m), intermediate (64cm), and near (40cm), respectively. Subjective vision, comfort and handling scores established statistically higher scores for both hyperopes and myopes compared to the pre-defined margin. The percentage of eyes with absolute lens orientation error ≤ 10° was over 94% and rotational stability ≤ 5° was over 98%.
Conclusion: The multifocal toric contact lens design provided clear and consistent vision for a variety of critical distance, intermediate and near tasks across varying lighting conditions and had a high rate of lens fit success.
Keywords: presbyopia, astigmatism, clinical trial, soft contact lenses, senofilcon
Introduction
Despite improvements in multifocal design and availability of lens options in recent years, multifocal contact lenses (CLs) are still under-utilized around the world. According to the annual international contact lens prescribing survey of practitioners for 2024, only an estimated 19% of fits were reported as multifocals worldwide, with around 25% in developed markets such as Canada and the United Kingdom (32%, 22%, respectively).1 This survey also included countries in Asia (Japan, the Phillipines and Taiwan), Mexico and South America (Argentina, Colombia) where multifocal prescribing is markedly less prevalent. The racial makeup of the developed markets could be expected to include people of color, though this level of detail was not reported in this survey. The low rate of multifocal prescribing is despite estimates that around 40% of contact lens wearers in those markets are over 40.2 The reasons for this are many, but among them is the lack of suitable options for patients with astigmatism, which may impact as many as 47% of patients in at least one eye.3 Lack of correction for astigmatism was specifically cited in 2 studies examining factors for dissatisfaction with and/or dropping out of contact lens wear. In one report dealing specifically with presbyopic subjects wearing multifocal contact lenses, logistic regression analysis showed that absence of astigmatism was one of only four factors that influenced prediction of successful contact lens wear.4 The other study did not include multifocal contact lenses but covered a wide range of ages (16 to 60 years) and found that in the group of previously failed wearers with astigmatism, over half had not been wearing astigmatic correction at the time of discontinuation of wear. When refit with toric contact lenses, 94% were able to successfully resume wear.5
An even more emphatic case for being diligent about providing astigmatic correction in presbyopic vision correction options is with intraocular lenses (IOLs). Looking at quality of life issues and post-operative astigmatism in post-surgical cataract cases, patients were 34 times more likely to always use distance glasses per diopter (D) of astigmatic refractive error in the better eye (p=0.003), while spherical refractive error did not have a significant impact (p=0.15). Interestingly, the odds for near spectacle use were not dependent on astigmatic error (p=0.12).6 A more recent study found that while even low amounts of residual astigmatic error (0.25 to 0.50D) increased the odds of not achieving 20/20 vision (p<0.001), those amounts had negligible impact on patient satisfaction. However, with amounts of residual astigmatism as low as 0.75D to 1.00 D, the odds of not being satisfied with vision increased by a factor of 2.0 in monofocal and 1.5 in multifocal IOL patients.7
While clinical and subjective performance can be degraded with uncorrected astigmatism for both CLs and IOLs, an important difference to consider is accommodation. Contact lens patients have the ability to accommodate through many of their contact lens-wearing years, while pseudophakic patients must rely solely on the optics of the IOL and quality of the surgery and accuracy of IOL placement for visual clarity. The presence of even small levels of residual accommodative amplitude in contact lens wearers helps explain some of the difficulty researchers have encountered in using simulation of astigmatic blur to predict outcomes related to residual astigmatic refractive error with both CLs and IOLs. Various studies have shown that simulated astigmatism reduced visual acuity more than astigmatism induced in a real optical system.8,9 However, a model allowing small levels of accommodation in the simulations eliminated these discrepancies, indicating that phakic presbyopic subjects are able to produce a low level of accommodation that may counterbalance a part of the deleterious effect of the astigmatism on image quality.10 The lack of this ability to accommodate could explain the more dramatic losses experienced by pseudophakic patients with residual astigmatic refractive errors and the consequent need for more accurate correction of astigmatism during IOL implantation. Additionally, the theory that an uncorrected astigmatic refractive error in presbyopic contact lens patients may engage any remaining accommodation to compensate for residual astigmatism is worth pondering. This idea may support the theory that presbyopic patients already struggling with diminishing accommodative amplitude and facility may be even more hindered by uncorrected astigmatism than their younger counterparts, as the two competing needs fight for those last remaining diopters.
One key question that needed to be addressed with the presbyopic contact lens patient was how accurate the astigmatic correction needs to be to provide definable performance benefits versus a simple spherical correction. This study evaluated the ability of a novel multifocal toric contact lens in a daily disposable lens with a single astigmatic lens power (−1.00D) and six axes (90° and 180° ± 10°) to provide adequate correction for a range of presbyopic patients with refractive astigmatism from −1.00D to −1.75D. The novelty of the daily disposable modality is of particular interest in this patient population. It affords a convenient way to wear lenses that has been associated with lower adverse event rates by offering a clean lens every day, eliminating the lens case and solution, both of which have been identified as risk factors for complications.11
Materials and Methods
This study was a two-week, 3 visit, open-label, single-arm study across 15 clinical sites in the United States. This study was performed in accordance with ISO 14155 standards for Good Clinical Practice (GCP) and the ethical principles of the Declaration of Helsinki, and United States (US) Code of Federal Regulations (CFR). The study was approved by Sterling IRB (Atlanta GA) and registered on ClinicalTrials.gov (#NCT06377488). All subjects signed a written informed consent prior to study participation.
Subjects
Subjects were habitual wearers of soft contact lenses between the ages of 40 and 70 with hyperopia or myopia and astigmatism correctable within the range of the study lens parameters. They were using some form of correction for presbyopia (reading glasses over contact lenses, multifocal or monovision contact lenses) or had responded positively to at least one symptom on a questionnaire regarding presbyopia. Subjects were screened and examined for eligibility at the baseline visit to assure they met all inclusion and exclusion criteria. Eligible subjects had to sign the informed consent and be willing and able to adhere to the study requirements. Additional eligibility criteria included entering distance visual acuity of 20/20−3 or better best corrected distance visual acuity, a distance spherical refraction component of −1.25D to −3.75D or +1.25D to +4.25D, refractive cylinder from −1.00D to −1.75D in each eye with axes within the range of 90° ± 15° or 180° ± 15°, and a near addition (add) power from +0.75D to +2.50D. Participants were excluded from participation if they did not meet all inclusion criteria, had any disease or condition that could interfere with contact lens wear or participation in the study, were using any ocular medication other than rewetting drops or systemic medications that could interfere with contact lens wear or cause blurred vision, have any hypersensitivity or allergic reaction of sodium fluorescein, or were an employee or immediate family member of an employee of a clinical site.
Study Lenses
Lenses were investigational daily disposable multifocal toric contact lenses manufactured in senofilcon A, a 38% water silicone hydrogel with an ultraviolet (UV) blocker and high energy visible (HEV) filter. Available powers were −1.00D to −4.00D or +1.00D to +4.50D in 0.25D steps with −1.00D cylinder power at axes 90° ± 10° and 180° ± 10° in low, mid or high add powers. Lenses were marked with fiducial lines at 6 and 12 o’clock to facilitate assessment of orientation and stability. The stabilization feature for this lens employed two highly refined areas of elevation in the horizontal mid-periphery that create equal and opposite torsional forces on the lens as the upper and lower eyelids contact these zones of differential thickness. This design has been shown to have advantages in stability with unusual head positions and gaze directions.12–14 The design of the multifocal portion of the lens is varied based on known differences in pupil size with age and refractive error such that the optical zone of each lens is unique to each combination of distance and add powers. All eligible subjects were dispensed the study lenses in a bilateral fashion.
Study Procedures
There were 3 scheduled visits. Figure 1 details the visits and procedures performed at each visit. Subjects reported to the site wearing their habitual contact lenses to accurately assess baseline patient-reported-outcomes (PROs) using CLUE and MRD questionnaires. Screening and baseline assessments were carried out, and the eligible subjects were fitted with the study lenses in a bilateral fashion according to the fitting guide. The lenses were allowed to settle for a minimum of 15 minutes and assessments were carried out. A maximum of two modifications of one or both lenses were allowed, if necessary. Further assessments were carried out, and the lenses were dispensed for 7±1 days.
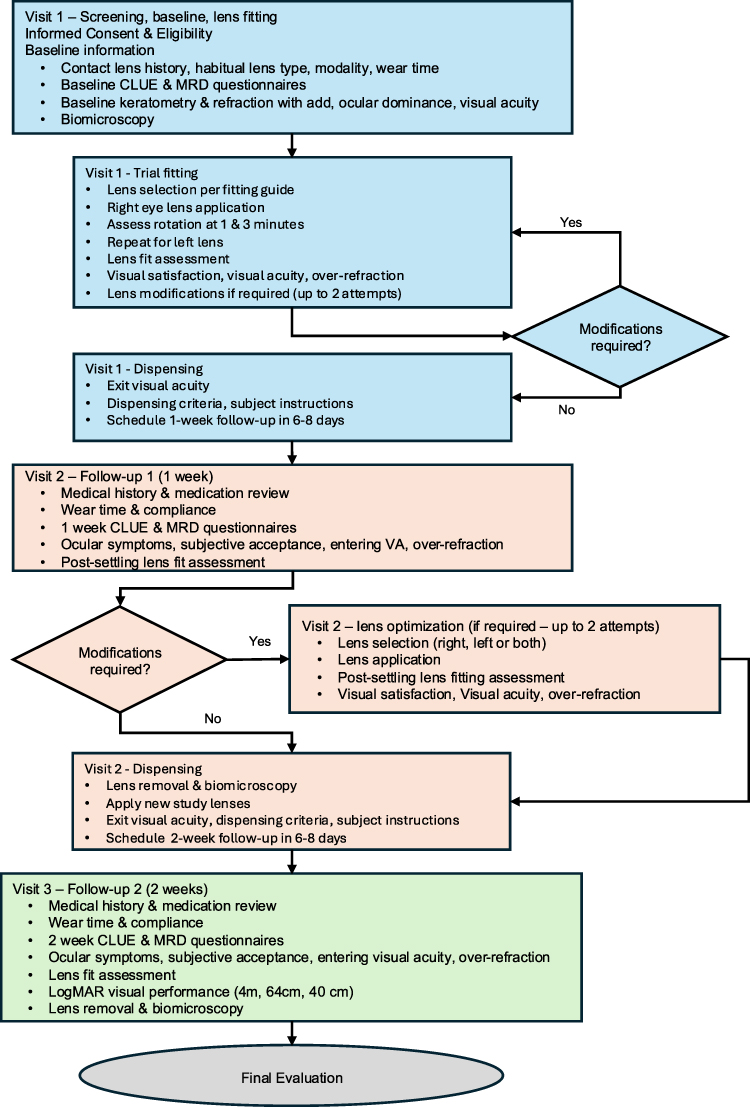 |
Figure 1 Study flow with procedures performed at each visit. Abbreviations: CLUE, Contact Lens User Experience, MRD, market research department. |
For visit 2, subjects reported to the site wearing their study lenses. Follow-up evaluations were carried out. If necessary, a maximum of two modifications of one or both lenses were allowed. Further assessments were carried out, and the lenses were dispensed for 7±1 days. Subjects reported to the site for visit 3 wearing their study lenses. Follow-up evaluations were carried out. Monocular and binocular VA was evaluated for 3 different distances, 2 contrast levels (high 100% and low 10%) and 2 luminance conditions. At distance (4 meters) VA was assessed using ETDRS Charts. At near (40 cm) and intermediate (64 cm) distances, assessments were made using reduced Guillon-Poling logMAR charts. Additional visual acuity was measured using high and low contrast charts in bright illuminance conditions. Visual acuity was also measured using high contrast charts in dim illuminance conditions (created by using goggles). The lenses were removed, stored, and then discarded after biomicroscopy, and the final evaluation was completed.
Efficacy
Binocular high luminance high contrast (HLHC) logMAR VA at Distance (4m), intermediate (64cm), and near (40cm) was assessed after 2-weeks of lens wear. Subjective vision, comfort and handling scores were assessed using the CLUE questionnaire after 2-weeks of lens wear. CLUE is a validated PRO questionnaire to assess patient-experience attributes of soft, disposable contact lenses (comfort, vision, and handling) in a contact-lens wearing population in the US, ages 18–65.15 Derived CLUE scores follow a normal distribution with a population average score of 60 (SD 20), where higher scores indicate a more favorable/positive response with a range of 0–120.15,16
Rotational stability and absolute lens orientation error were assessed for each eye at least 15 minutes after lens insertion at the initial fitting visit (Visit 1). Rotational stability is the amount of observed rotational movement of the scribe markings on the lens in degrees that occurs while blinking in primary gaze. Absolute lens orientation error was quantified by the absolute value of mis-location of the lens scribe markings in degrees relative to a vertical reference line. Lens fit success was quantified by the number of lenses needed to fit (optimize) the subject’s vision. Lens optimization occurred at visit 1 and visit 2.
Safety
Standard safety assessments in the form of slit-lamp biomicroscopy and lens fit acceptability were included in all study visits, but these routine results were all found to be satisfactory and have not been included here for the sake of brevity.
Statistical Analyses
The sample size of the trial required at least 140 subjects to complete the entire study (through visit 3). This sample size provides a statistical power of at least 99% to detect statistical superiority for each efficacy endpoint. For VA and CLUE endpoints, sample size calculations were performed using one-sample t-test for superiority by a margin.17 For all remaining endpoints, sample size estimates were performed using a Bayesian beta-binomial model for correlated binary data.
All statistical analyses were conducted on the intention-to-treat population (ITT), which included all subjects with data collected at a given time for an endpoint. Binocular HLHC logMAR visual acuity at distance (4m), intermediate (64cm), near (40cm), and subjective, vision, comfort, and handling scores were all analyzed separately, using a linear mixed model. Subjective vision, comfort, and handling models were adjusted using baseline scores as a covariate. For all models, sphere strata (hyperope and myope) was included as a fixed effect and gender was included as a fixed covariate. The Satterthwaite Method was used for the calculation of the denominator degrees of freedom. Mean estimates for each endpoint were carried out using 2-sided 95% confidence intervals (CI) constructed for the least squares mean (LSM). Estimated means for subjective vision comfort and handling were provided for each sphere stratum (hyperope and myope).
Absolute rotation error was calculated using the absolute value of toric lens rotation (degrees) and was dichotomized as Y = 1 if absolute toric lens rotation (degrees) ≤ 10°) and Y = 0, otherwise. Lens Fit Success was quantified by the number of lenses needed to fit (optimize) the subject’s vision and dichotomized as Y=1 if a subject’s vision is optimized in 4 lenses or less, and Y=0, otherwise. Absolute rotation error and lens fit success were analyzed separately using a Bayesian beta-binomial model for correlated binary data. The Metropolis sampler algorithm was used to carry out parameter estimation. Convergence of the simulated chains was assessed using correlation and sample trace plots. Results were reported as estimated percentages and corresponding 95% credible intervals (CrI).
Rotational Stability was dichotomized as Y=1 is lens stability with blinks ≤5° and Y=0 otherwise. Rotational stability was analyzed using a Bayesian beta-binomial hierarchical model accounting for zero-event problem.18,19 Results were reported as estimated percentages and corresponding 95% CrI.
Hypothesis testing for statistical superiority was conducted separately for each endpoint. All hypothesis tests compared the mean (or percentage of eyes [or subjects]) to a pre-defined threshold (superiority margin). Hypothesis testing for subjective vision, comfort, and handling was performed separately for sphere strata.
Statistically significant superiority was established for binocular HLHC logMAR VA at distance (4m), intermediate (64cm), and near (40cm) if the upper limit of the 95% CI was less than the pre-defined threshold. While for CLUE scores (vision, comfort and handling), rotational stability, absolute lens orientation error, and lens fit success, statistically significant superiority was established if the lower limit of the 95% CI (or 95% CrI) was above the pre-defined threshold (Table 1).
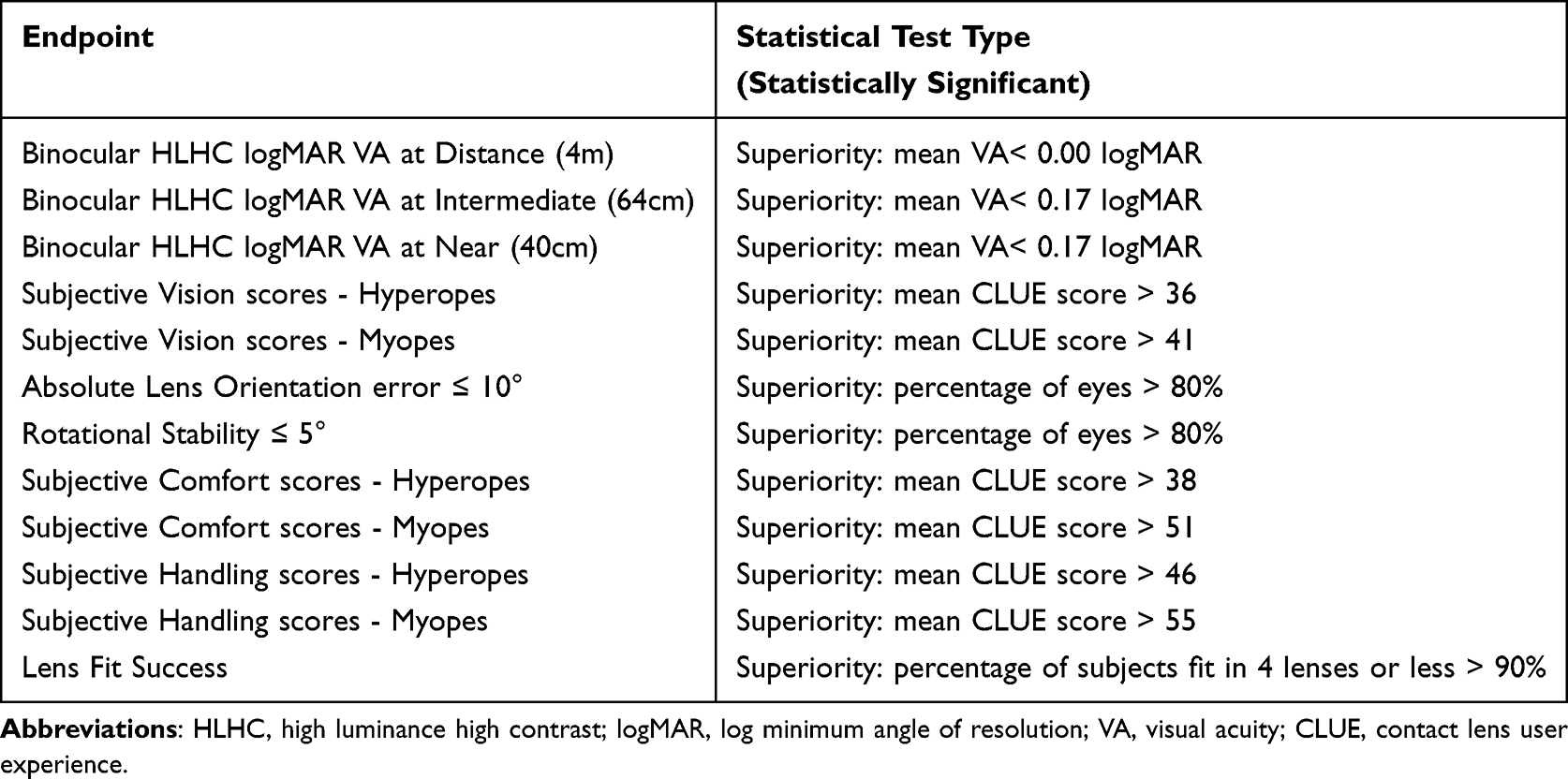 |
Table 1 Statistical Hypotheses Tests by Efficacy Endpoint |
All endpoints were required to demonstrate statistically significant superiority. All analyses were performed in SAS Version 9.4 (SAS Institute, Cary, NC).20
Results
The study was conducted between April and June 2024 at 15 clinical sites. Details regarding subject accountability are shown in Table 2. A total of 176 subjects were enrolled. Five subjects failed to meet all eligibility criteria (screen failures), and 171 subjects were fitted with the study lenses. A total of 8 subjects discontinued, and 163 subjects completed the study.
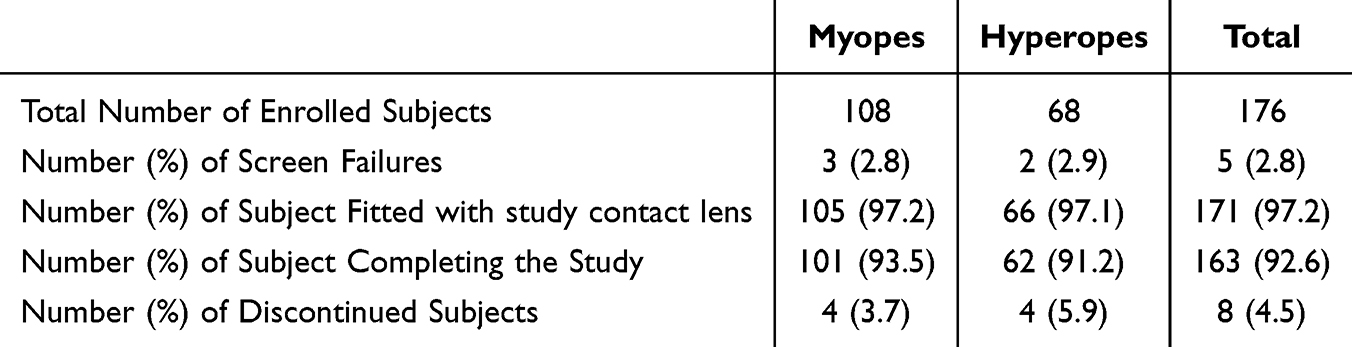 |
Table 2 Subject Accountability |
Of those discontinued, 2 subjects were discontinued due to unsatisfactory visual response (not correctable as the optimized lens power was not available); 2 subjects were discontinued due to unsatisfactory lens fitting in at least one eye (rotation greater than 30°); 1 subject was discontinued due to non-compliance to protocol; and 3 subjects were discontinued due to other reasons (1 subject was unable to attend visit 3 within the visit window and 2 were dispensed the incorrect power). Subject characteristics for those fit with the study lenses are shown in Table 3. No significant differences were noted between the 2 groups (p < 0.05).
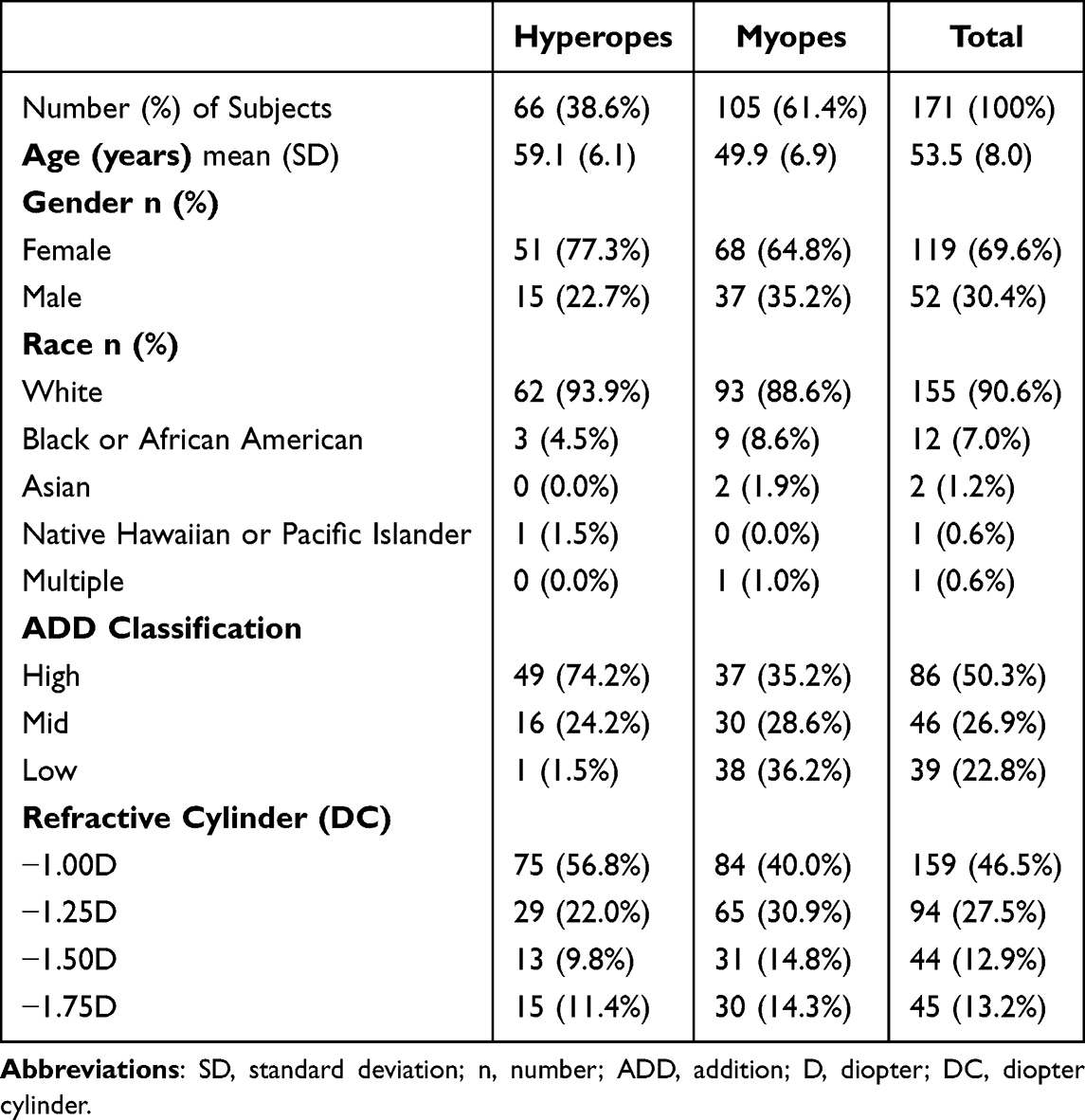 |
Table 3 Subject Demographics and Characteristics – All Subjects Fit with Study Lens |
Efficacy
Binocular High Luminance, High Contrast Visual Acuity
After 2-weeks of lens wear, the adjusted mean estimate (LSM) and 2-sided 95% CI for binocular HLHC VA were −0.085 (−0.115, −0.056), −0.023 (−0.050, 0.005), and 0.083 (0.051, 0.116) logMAR at distance (4m), intermediate (64cm) and near (40cm), respectively. As displayed in Figure 2, the mean VA at each distance was statistically significantly lower (superior, all p-values <0.0001) compared to the pre-defined threshold (superiority margin) of 0.00 logMAR (20/20 Snellen VA) and 0.17 logMAR (20/30 Snellen VA), for distance and intermediate/near, respectively.
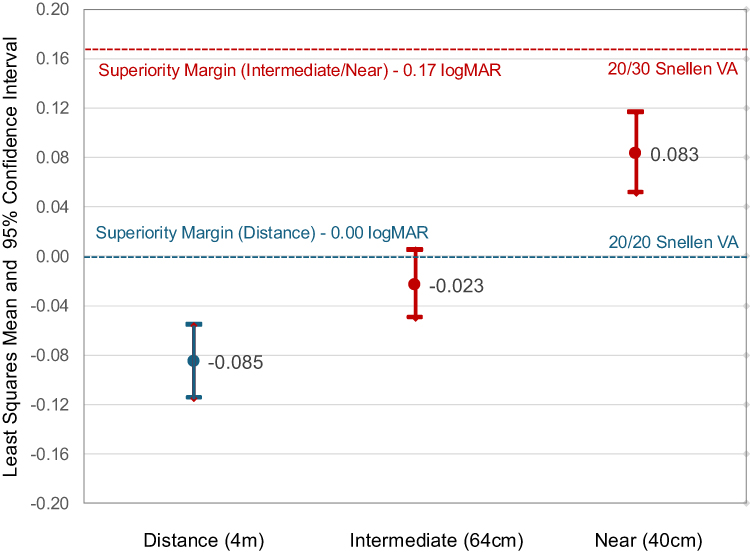 |
Figure 2 Binocular HLHC VA at distance (4m), intermediate (64cm) and near (40cm); n=163 subjects with data at Visit 3. Dotted lines represent superiority margin for binocular HLHC logMAR VA for distance (blue) and intermediate/near (red). |
Subjective Vision, Comfort, and Handling Scores
After 2-weeks of lens wear, the adjusted mean estimate (least squares mean, LSM) and 2-sided 95% CI for CLUE vision scores were 57.8 (51.7, 64.0) and 62.1 (56.7, 67.5), for hyperopes and myopes, respectively. As displayed in Figure 3, the mean CLUE vision for each sphere strata was statistically significantly higher (superior; both p-values <0.0001) compared to the pre-defined threshold of 36 and 41 CLUE points, for hyperopes and myopes, respectively, values that were established based on extensive historical data across multiple lens types and brands. The adjusted mean estimate and 2-sided 95% CI for CLUE comfort scores were 64.7 (58.6, 70.8) and 64.2 (59.0, 69.5) for hyperopes and myopes, respectively. CLUE handling scores were 67.9 (62.2, 73.5) for hyperopic subjects and 67.0 (62.2, 71.8) for myopic subjects. Figure 4 displays the adjusted mean estimate and 2-sided 95% CI for comfort and handling scores for each stratum. These mean CLUE scores are above 60 which indicates that the lens provides good comfort and handling, and the lower confidence intervals were all above the pre-defined superiority margins (all p-values <0.0001).
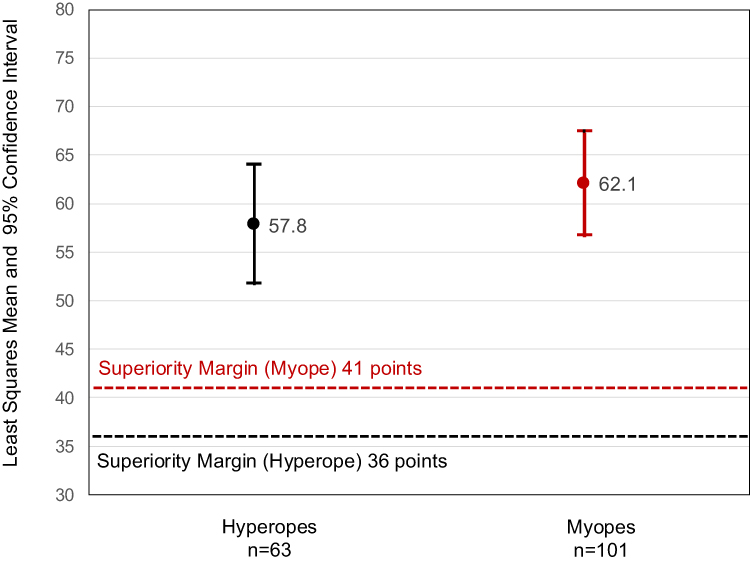 |
Figure 3 CLUE vision scores with data collected after 2-weeks of lens wear (visit 3). Dotted lines represent superiority margin for CLUE vision scores for hyperopes (black) and myopes (red). |
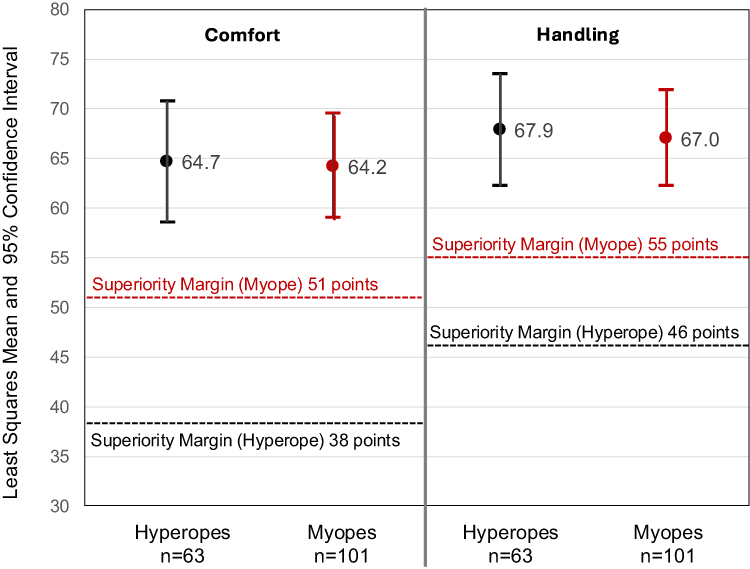 |
Figure 4 CLUE comfort and handling scores for hyperopes (black) and myopes (red) after 2-weeks of lens wear (visit 3). |
Lens Fit Success, Rotational Stability, and Absolute Lens Orientation Error
The estimated percentage of subjects (out of 171 subjects fitted with the study lens) who were fit with the optimized lens pair in 4 lenses or less was 96.6% (95% CrI: 93.3%, 98.8%). The estimated percentage of eyes with rotational stability ≤5° or less was 98.8% (95% CrI: 97.4%, 99.7%) and the estimated percentage of eyes with absolute lens orientation error ≤10° or less was 94.3% (95% CrI: 90.8%, 96.8%).
Discussion
This study answers several important questions about contact lens correction of astigmatism in a presbyopic patient. First, the study showed that good visual acuity performance can be expected at distance, intermediate and near for mild-to-moderate astigmats when employing a single cylindrical power of −1.00D. It is also worth noting that the 20/30 criteria for near and intermediate visual acuity selected in this study represent a high bar, particularly in the digital world of today. According to SPIE, the international society for optics and photonics, 20/30 Snellen near visual acuity corresponds to J2 in the Jaeger system or a 5-point font size in Times New Roman, while typical newsprint is between 10- and 14-point, J7 to J10, or 20/70 to 20/100 Snellen equivalent.21
Next, under-correction of cylinder appeared not to be an impediment to good visual acuity and subjective performance. In the subjects enrolled in this study, cylindrical under-correction would have ranged from 0.00 D in those with 1.00D of refractive cylinder, up to 0.75D for those with 1.75D refractive cylinder. While not statistically analyzed as an outcome variable, inspection of monocular HLHC VA performance across distances for each refractive cylinder revealed only small differences (up to 0.03 logMAR, or 1.5 letters) with no clear pattern of decreasing performance with increasing refractive cylinder levels (Figure 5). This is very similar to the situation that exists with many non-toric multifocal lenses as prescribed today, as manufacturer fitting guides for these lenses often have indications for fitting patients with up to 0.75D astigmatism, and in some cases even more. Using a similar approach to that used when fitting mildly astigmatic presbyopic patients with multifocal contact lenses, a multifocal toric lens with a single −1.00D cylinder power may be indicated for use in correcting up to 1.75D refractive cylinder, leaving up to 0.75 D cylinder uncorrected. There are a few factors that support this approach.
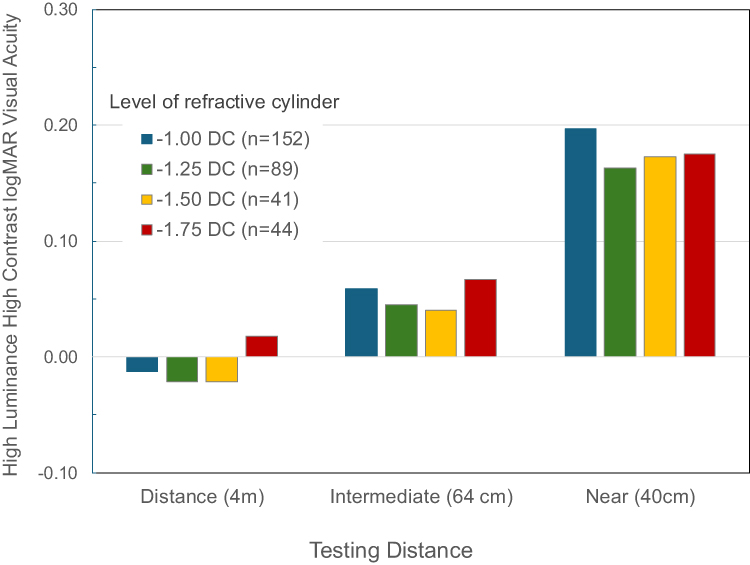 |
Figure 5 Variation in monocular high luminance, high contrast logMAR visual acuity by level of baseline refractive cylinder at distances tested. |
First, the distribution of astigmatic refractive errors in the population is highly skewed toward low amounts of cylinder. Multiple studies over the past 50 years have confirmed this beginning with Holden in 1975 who found that 84.2% of an Australian population of prospective contact lens patients had astigmatism under 1.75D.22 A 2011 analysis of over 11,000 spectacle prescriptions in the United Kingdom revealed only 7.6% of eyes with cylinders greater than 1.50D, with the over 40-year-old group reflecting a number similar to the larger group.3 Finally, a 2015 study in Australia found a prevalence of 44.8% (43.2–46.4%) for refractive astigmatism between 0.50 and 1.75 D and another 51.9% (95% CI 50.3–53.5%) for under 0.50 D leaving just 3.3% in the over 1.75 group.23 They also found that astigmatism increased in the older groups, but the largest shifts occurred in the 60 years and over groups.
Second, the burden on manufacturers to produce the multitude of lenses created by the combination of sphere powers, cylinder powers, axes and adds creates potential for material waste, back ordered product and delays in launching new products due to capacity and inventory constraints. For a lens offered in +6.00 to −9.00 in 0.25D steps, 10 axes and 3 add powers, it adds 1830 parameters or stock keeping units (SKUs). This also creates inventory management issues for a busy practice. With one cylinder power that performs well across the most commonly encountered levels of cylinders seen in practice, many of these issues are minimized.
And third, based on the hypothesis that the small reserves of accommodation can be tasked in the effort to compensate for uncorrected cylinder in a presbyopic patient, a quick and easy option for successful management of the 30 to 50% of patients who may present to a practice with low to moderate levels of astigmatism is attractive.
The ability to correct presbyopic patients with astigmatism with a daily disposable contact lens is also worth mentioning. Not only do daily disposable lenses afford patients the many benefits of a fresh lens every day, they also allow patients to control costs by managing the number of days per week they choose to wear the lenses.
Limitations of this study include a limited set of parameters tested, though both hyperopic and myopic subjects were included in the most common powers. The lack of a control group also represents a limitation. A spherical multifocal control would have illuminated more specific benefits to correcting astigmatism, though the levels of astigmatism of subjects in this study are generally regarded as excessive for fitting of spherical lenses. Currently, the only mass marketed multifocal toric lenses are monthly lenses which make comparisons to a daily disposable cumbersome due to differences in material, care systems, wearing and replacement schedules. This may be an avenue for further research to better understand the advantages and disadvantages of a single versus multi-cylinder option, as well as to contrast daily disposable versus a monthly reusable option. Lastly, a longer study duration may pick up more subtle subjective changes related to adaptation or a greater variety of environments and visual challenges encountered.
Conclusion
These results demonstrate the efficacy of this combination of multifocal and toric contact lens designs, and they show that a single cylinder of a power designed to best bridge the most commonly encountered levels of refractive cylinder in the contact lens practice can provide successful multifocal fits when following the manufacturer’s fitting guide.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, RF. The data are not publicly available due to the proprietary nature of the designs discussed.
Acknowledgments
Editorial assistance was provided by Dr. Cristina Schnider. Dr. Meredith Bishop provided helpful review and suggestions on content.
Funding
The study was funded by Johnson and Johnson Vision Care, Inc., manufacturer of the device used in this clinical investigation.
Disclosure
The authors are employees of Johnson & Johnson Vision Care, Inc.
References
1. Morgan PB, Woods CA, Tranoudis IG, et al. International contact lens prescribing in 2024. Contact Lens Spectrum. 2025;40(January/February 2025):22–24,26,28–30.
2. Schnider C, Ruston D. Presbyopia: the short journey to soft contact lens success. Contact Lens Spectrum. 2021;36(Online Exclusive):E1–E6.
3. Young G, Sulley A, Hunt C. Prevalence of astigmatism in relation to soft contact lens fitting. Eye & Contact Lens. 2011;37(1):20–25. doi:10.1097/ICL.0b013e3182048fb9
4. Zeri F, Di Censi M, Livi S, Ercoli A, Naroo SA. Factors that influence the success of contact lens fitting in presbyopes: a multicentric survey. Eye & Contact Lens. 2019;45(6):382. doi:10.1097/ICL.0000000000000606
5. Sulley A, Young G, Lorenz KO, Hunt C. Clinical evaluation of fitting toric soft contact lenses to current non-users. Ophthalmic and Physiological Optics. 2013;33(2):94–103. doi:10.1111/opo.12028
6. Wilkins MR, Allan B, Rubin G. Moorfields IOL study group. Spectacle use after routine cataract surgery. British Journal of Ophthalmology. 2009;93(10):1307–1312. doi:10.1136/bjo.2008.151829
7. Schallhorn SC, Hettinger KA, Pelouskova M, et al. Effect of residual astigmatism on uncorrected visual acuity and patient satisfaction in pseudophakic patients. J Cataract Refract Surg. 2021;47(8):991–998. doi:10.1097/j.jcrs.0000000000000560
8. Ohlendorf A, Tabernero J, Schaeffel F. Visual acuity with simulated and real astigmatic defocus. Optom Vis Sci. 2011;88(5):562–569. doi:10.1097/OPX.0b013e31821281bc
9. Remón L, Benlloch J, Pons A, Monsoriu JA, Furlan WD. Visual acuity with computer simulated and lens-induced astigmatism. OPTICA APPLICATA. 2014. doi:10.5277/OA140403
10. Vincent M, Marin G, Legras R. Subjective evaluation of defocus and astigmatism combinations using image simulation in presbyopes. Optometry and Vision Science. 2021;98(1):73. doi:10.1097/OPX.0000000000001627
11. Stapleton F, Edwards K, Keay L, et al. Risk factors for moderate and severe microbial keratitis in daily wear contact lens users. Ophthalmology. 2012;119:1516–1521. doi:10.1016/j.ophtha.2012.01.052
12. Zikos GA, Kang SS, Ciuffreda KJ, et al. Rotational stability of toric soft contact lenses during natural viewing conditions. Optometry and Vision Science. 2007;84(11):1039–1045. doi:10.1097/OPX.0b013e318159aa3e
13. Chamberlain P, Morgan PB, Moody KJ, Maldonado-Codina C. Fluctuation in visual acuity during soft toric contact lens wear. Optom Vis Sci. 2011;88(4):E534–538. doi:10.1097/OPX.0b013e31820ea1ea
14. McIlraith R, Young G, Hunt C. Toric lens orientation and visual acuity in non-standard conditions. Contact Lens and Anterior Eye. 2010;33(1):23–26. doi:10.1016/j.clae.2009.08.003
15. Wirth RJ, Edwards MC, Henderson M, Henderson T, Olivares G, Houts CR. Development of the contact lens user experience: CLUE scales. Optom Vis Sci. 2016;93(8):801–808. doi:10.1097/OPX.0000000000000913
16. Edelen MO, Reeve BB. Applying item response theory (IRT) modeling to questionnaire development, evaluation, and refinement. Qual Life Res. 2007;16(1):5–18. doi:10.1007/s11136-007-9198-0
17. PASS. Power analysis and sample size software. Kaysville, Utah, USA: NCSS, LLC; 2021. Available from: https://www.ncss.com/software/pass/pass-documentation.
18. Jovanovic BD, Levy PS. A look at the rule of three. The American Statistician. 1997;51(2):137–139. doi:10.2307/2685405
19. Chen Z, McGee M. A Bayesian approach to zero-numerator problems using hierarchical models. Journal of Data Science. 2008;6(2):261–268. doi:10.6339/JDS.2008.06(2).401
20. SAS help center: SAS/STAT user’s guide. Available from: https://documentation.sas.com/doc/en/pgmsascdc/9.4_3.5/statug/titlepage.htm.
21. Visual Acuity. Available from: https://spie.org/publications/spie-publication-resources/optipedia-free-optics-information/fg04_p19-20_visual_acuity.
22. Holden BA. The principles and practice of correcting astigmatism with soft contact lenses*. The Australian Journal of Optometry. 1975;58(8):279–299. doi:10.1111/j.1444-0938.1975.tb01830.x
23. Sanfilippo PG, Yazar S, Kearns L, Sherwin JC, Hewitt AW, Mackey DA. Distribution of astigmatism as a function of age in an Australian population. Acta Ophthalmologica (1755375X). 2015;93(5):e377–e385. doi:10.1111/aos.12644
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Wear Experiences with Two Soft Contact Lenses for Astigmatism of Different Modalities
Fogt JS, Satiani N, Bickle KM, Wesley G, Patton K
Clinical Optometry 2024, 16:93-100
Published Date: 26 March 2024