Back to Journals » International Medical Case Reports Journal » Volume 19
Propylthiouracil Induced Neutropenia in Thyroid Storm: A Case Requiring Urgent Total Thyroidectomy
Authors Aljishi AK, Altarooti SH, Albrahim AH, Alfaraj AW, Alqurain AA, Abohelaika S ![]()
Received 23 November 2025
Accepted for publication 7 March 2026
Published 16 March 2026 Volume 2026:19 583884
DOI https://doi.org/10.2147/IMCRJ.S583884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Abdulmohsen K Aljishi,1 Sukaina H Altarooti,2 Ali H Albrahim,3 Ali Wahab Alfaraj,4 Aymen Ali Alqurain,5 Salah Abohelaika3,6
1Adult Intensive Care Department, Qatif Central Hospital, Qatif, 32654, Saudi Arabia; 2Medical Department/Endocrinology Division, Qatif Central Hospital, Qatif, 32654, Saudi Arabia; 3Pharmacy Department, Qatif Central Hospital, Qatif, 32654, Saudi Arabia; 4Academic Training Affairs and Research Department, Qatif Central Hospital, Qatif, 32654, Saudi Arabia; 5Department of Clinical Practice, Faculty of Pharmacy, Northern Border University, Rafha, 91911, Saudi Arabia; 6Research Department, Qatif Central Hospital, Qatif, 32654, Saudi Arabia
Correspondence: Salah Abohelaika, Research Department, Qatif Central Hospital, Qatif, 32654, Saudi Arabia, Email [email protected]
Abstract: Thyroid storm is a rare but life-threatening complication of hyperthyroidism that requires urgent management. While propylthiouracil (PTU) is a key treatment, it carries multiple risks, including potentially fatal risk of agranulocytosis. We report a 40-year-old female with Graves’ disease who presented with thyroid storm and compressive goiter. High-dose PTU (1 g loading dose followed by 200 mg every 4 hours) was initiated; however, severe neutropenia (ANC: 0.22× 10ˆ 3/μL) developed within 48 hours, necessitating immediate drug discontinuation. Bridging therapy with hydrocortisone, cholestyramine, Lugol’s solution, was implemented once available, and low-dose carbimazole was cautiously reintroduced under close monitoring without recurrence of neutropenia. Once a euthyroid state was achieved, definitive management with a total thyroidectomy was performed without complications. This case highlights three key learning points: (1) agranulocytosis can occur very early during high-dose PTU therapy; (2) careful bridging strategies are essential to prevent rebound thyroid storm after antithyroid drug withdrawal; and (3) timely transition to definitive surgical management can be lifesaving when antithyroid drug intolerance occurs.
Keywords: thyroid storm, graves’ disease, propylthiouracil, neutropenia, total thyroidectomy
Introduction
Thyroid storm represents the most severe clinical manifestation of thyrotoxicosis, characterized by systemic decompensation and associated with considerable morbidity and mortality.1 Prompt recognition and aggressive management are essential to prevent multiorgan failure and death.2 Antithyroid drugs such as propylthiouracil (PTU) are cornerstone therapies but carry serious hematologic risks, including agranulocytosis.3 PTU-induced neutropenia poses a major clinical dilemma, as discontinuation can precipitate uncontrolled thyrotoxicosis. This report describes a rare case of PTU-induced neutropenia during a thyroid storm requiring an urgent total thyroidectomy as a definitive treatment.
While antithyroid drug–induced agranulocytosis is a recognized complication, most reports describe its occurrence several weeks after therapy initiation. Early onset severe neutropenia during thyroid storm management presents a particularly complex clinical scenario, as abrupt drug discontinuation risks precipitating uncontrolled thyrotoxicosis. The optimal bridging strategy and timing of definitive intervention in this setting remain insufficiently detailed in existing literature. This case illustrates these challenges and provides practical insights into safe transition to surgical management.
Case Presentation
A 40-year-old female with a 10-year history of Graves’ disease on a stable dose of carbimazole (45 mg daily), reported adherence to therapy but had not been attending regular endocrinology follow-up appointments. She presented to the emergency department with fever, sore throat, dry cough, palpitations, epigastric pain, vomiting and heat intolerance. In addition, she reported compressive symptoms, including hoarseness, shortness of breath, dysphagia, and progressive goiter enlargement. On physical examination, she was febrile (39.2°C) with a heart rate of 150 beats per minute, blood pressure of 142/65 mmHg, respiratory rate of 35 breaths per minute, and oxygen saturation of 97% in room air. Physical examination revealed a hyperemic congested throat without exudates, a markedly enlarged goiter with audible bruits, and bilateral exophthalmos.
Laboratory evaluation demonstrated a suppressed thyroid-stimulating hormone (TSH) level of 0.02 mIU/L (normal range: 0.55–4.78 mIU/L), elevated free triiodothyronine (FT3) of >30.8 pmol/L (normal range: 3.5–6.5 pmol/L), and elevated free thyroxine (FT4) of 45.8 pmol/L (normal range: 11.5–22.7 pmol/L). Electrocardiography (ECG) confirmed sinus tachycardia.
Supportive radiologic evaluation included thyroid doppler ultrasonography, which demonstrated marked diffuse enlargement of the thyroid gland with prominent hypervascularity, with the right lobe measuring 4.6×4.1×7.0 cm, and the left lobe measuring 4.8×4.0×7.1 cm (Figure 1). Non-Contrast enhanced computed tomography (CT) of the neck revealed diffuse thyroid gland enlargement causing a significant mass effect on the trachea and cervical esophagus, resulting in mild airway compression and displacement, without evidence of retrosternal extension or local tissue invasion (Figure 2). These radiologic findings correlated closely with the patient’s compressive symptoms.
 |
Figure 1 Ultrasound of the neck (a=right lobe length, b=right lobe width, c=right lobe vascularity, d=left lobe length, e=left lobe width, f=left lobe vascularity). The blue dotted lines indicating the exact measurements of the nodule (a, b, d and e), and the green line demarked region is a colored Doppler box which indicates the vascularity of the nodule (c and f). |
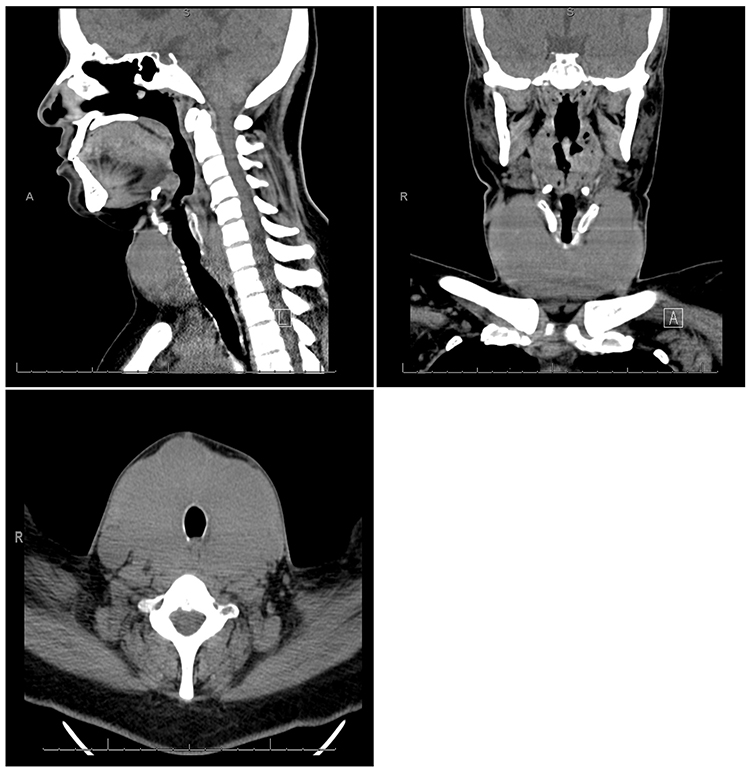 |
Figure 2 Computed tomography (CT) of the neck. |
A concurrent upper respiratory tract infection was considered the most likely precipitating factor, in the context of irregular endocrinology follow-up and uncertain biochemical control. Other common triggers, including recent trauma, surgery, or medication non-compliance, were not identified. The diagnosis of thyroid storm was supported by a Burch–Wartofsky Point Scale (BWPS) score exceeding 45 points and fulfillment of the Japanese Thyroid Association (JTA) criteria for definite thyroid storm (TS1), based on hyperpyrexia, marked tachycardia, gastrointestinal manifestations, and biochemical thyrotoxicosis.
Subsequently, she was admitted to the intensive care unit (ICU) and started the following treatment protocol. She was given hydrocortisone 300 mg intravenously, followed by 100 mg every 8 hours. Propylthiouracil (PTU) was initiated as a 1gm orally loading dose, then 200 mg every 4 hours, and propranolol at 60 mg orally every 6 hours for sympathetic over activity.
Although inflammatory markers and microbiological studies did not support a confirmed bacterial infection—given the normal leukocyte count, low procalcitonin level, negative blood and urine cultures, and unremarkable chest radiography—empiric antibiotics were administered because of the presence of fever and upper respiratory symptoms, recognizing infection as a well-known precipitant of thyroid storm. No definitive bacterial source was subsequently identified.
Following initiation of therapy, the patient demonstrated marked clinical improvement, with well-controlled palpitations and fever. However, on day 2, she developed severe leukopenia, mainly neutropenia, with white blood cell (WBC) count reaching 1.82x10ˆ3/uL (normal range: 4–10x10ˆ3/uL) and an absolute neutrophil count (ANC) of 0.22×10ˆ3/uL (normal range: 1.5–6x10ˆ3/uL) (Figure 3) necessitating the immediate cessation of PTU as a possible cause. Reverse isolation was implemented. Bridging therapy was planned to be introduced to stabilize the patient’s condition and prevent a rebound of thyroid storm.
 |
Figure 3 Absolute neutrophil count trends during hospital stay, showing a sharp decline following PTU loading dose followed by gradual recovery after discontinuation. |
The intended regimen included the addition of super-saturated potassium iodine (SSKI) solution orally every six hours, and cholestyramine given every eight hours. However, both medications were temporarily unavailable due to pharmacy stock limitations, which posed additional therapeutic challenges in the acute management of this case.
The patient’s ANC gradually improved following PTU discontinuation, with full neutrophil recovery observed on day 5 (Figure 3). A diagnostic evaluation was performed to investigate the severe neutropenia. Sepsis was excluded based on a negligible procalcitonin, mildly elevated CRP, and negative blood and urine cultures (Table 1). The patient had a normal baseline leukocyte count and no history of cytopenias or exposure to other myelosuppressive drugs. While thyrotoxicosis can cause mild leukopenia, the precipitous drop to an absolute neutrophil count (ANC) following high-dose PTU exposure—with prompt recovery upon discontinuation—confirmed PTU-induced agranulocytosis.
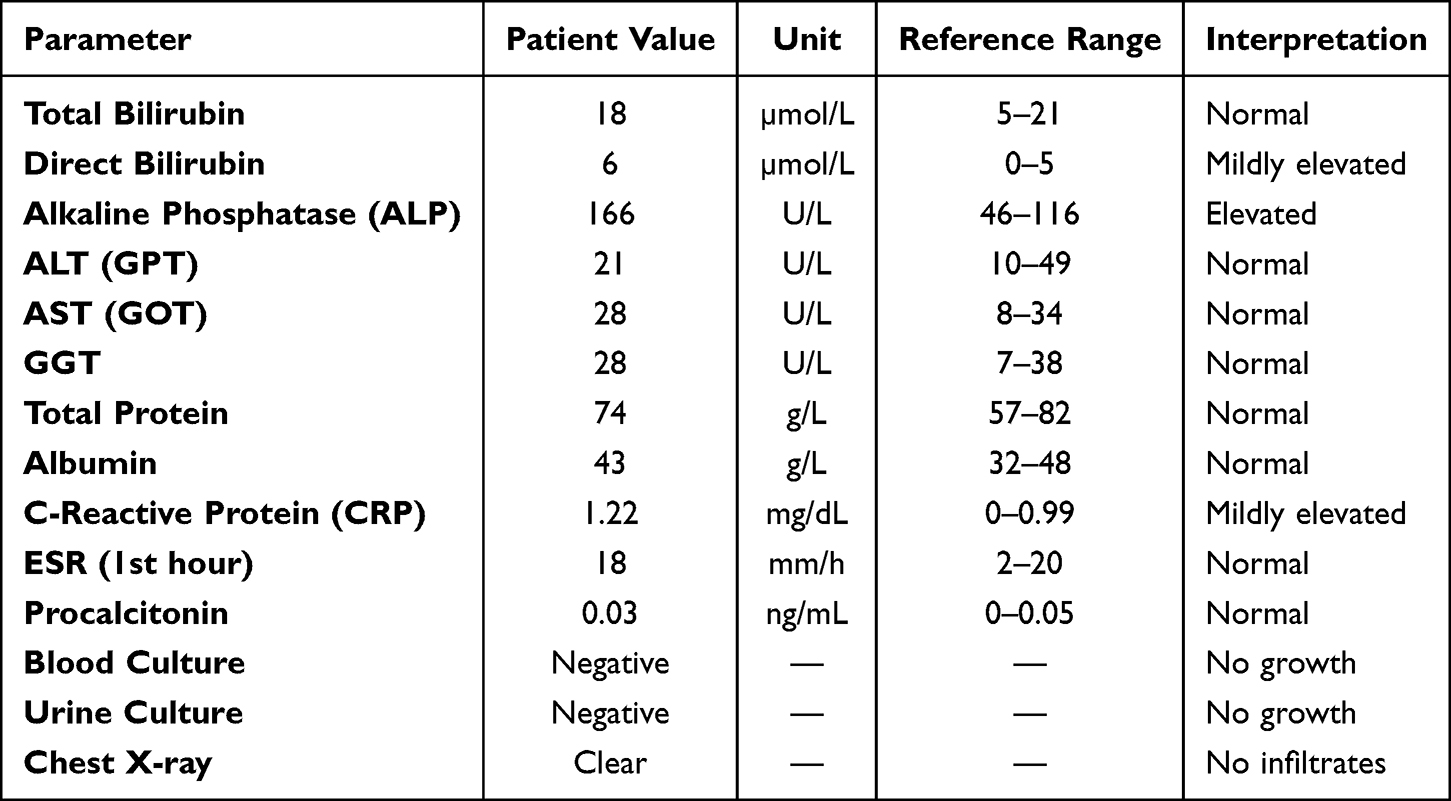 |
Table 1 Physical and Laboratory Work-Up |
Despite initial improvement, the patient developed biochemical evidence of rebound hyperthyroidism (Figure 4). Given this, a decision was made to re-start carbimazole at a dose of 10 mg orally twice daily, with the patient’s full consent and close neutrophil monitoring. Cholestyramine and Lugol’s solution were subsequently introduced to the regimen, leading to a gradual decline in FT4 levels and successful achievement of a euthyroid state on the 11th day of admission (Figure 4). Importantly, no recurrence of neutropenia was observed despite continued carbimazole therapy (Figure 3). Therapeutic plasma exchange (TPE) was considered as a potential rescue and bridging therapy, however, given the patient’s clear clinical and biochemical improvement with optimized medical management, escalation to plasma exchange was deemed unnecessary and therefore was not performed.
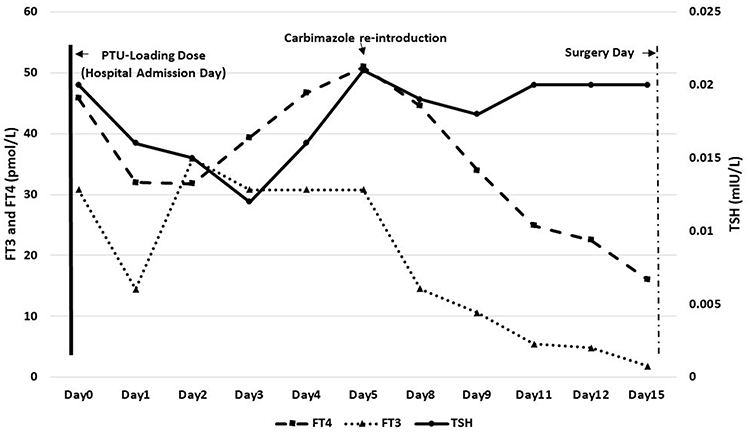 |
Figure 4 Trend of TSH, FT3, and FT4 with PTU-free medical therapy until definitive thyroidectomy. It illustrates the downward trend in FT3 and FT4 during PTU-free bridging therapy, achieving euthyroidism before definitive thyroidectomy. |
In light of severe neutropenia precluding further antithyroid therapy, as well as the presence of compressive symptoms and Graves’ orbitopathy, radioactive iodine therapy was considered inappropriate. Consequently, total thyroidectomy was selected as the definitive treatment. Perioperative optimization included continuation of beta-blockade and corticosteroid therapy, along with iodine administration to reduce the risk of intraoperative thyroid storm. Close multidisciplinary coordination among the endocrinology, anesthesia, and surgical teams ensured meticulous perioperative planning and hemodynamic stability.
By day 15, the patient underwent total thyroidectomy without intraoperative or postoperative complications.
Discussion
Thyroid storm is a life-threatening endocrine emergency characterized by extreme systemic decompensation due to excessive thyroid hormone activity. Although it is rare, occurring in 0.57–0.76 cases per 100,000 hospitalized patients annually, its 8–25% mortality rate underscores the urgency of early recognition and intervention.1,4 The hallmark features include hyperthermia, tachycardia, altered mental status, and gastrointestinal symptoms, often leading to cardiovascular collapse, hepatic dysfunction, or multi-organ failure if untreated.5,6 The pathophysiological mechanisms involve increased adrenergic activity and heightened sensitivity to catecholamines, which can precipitate cardiovascular collapse and multi-organ failure.2 The management of thyroid storm focuses on rapidly reducing thyroid hormone levels and mitigating the effects of excess hormones on the body.7
PTU, a thionamide derivative, plays a dual role in thyroid storm management by inhibiting thyroid peroxidase activity (reducing thyroid hormone synthesis) and peripheral T4-to-T3 conversion. This unique mechanism makes PTU a preferred agent during acute episodes of thyroid storm.2 However, its use is complicated by the risk of rare but severe adverse effects, notably agranulocytosis.3,8 Proposed mechanisms for agranulocytosis induced by PTU include producing reactive PTU metabolites that lead to direct bone marrow toxicity or antibody-mediated destruction of granulocytes.9
The incidence of agranulocytosis is estimated to be 0.3–0.6%,8,10 women are 10 times more likely to be affected compared to men,11 and it is notable to be dose-dependent, with various studies indicating that higher doses correlate with an increased risk of this adverse effect. One study showed that the risk increased dramatically by increasing the dose, with an incidence of 0.81% at 300 mg per day of PTU compared to 0.33% at 150 mg per day.5 PTU-induced agranulocytosis, defined as an absolute neutrophil count (ANC) <0.5×10ˆ3/uL, typically manifests within the first 90 days of treatment.4,12 However, using PTU in terms of thyroid storm can lead to the rapid development of agranulocytosis, as seen in the current patient and in some case reports where patients developed this condition shortly after starting PTU therapy.5 This can be attributed to both the pathophysiological mechanisms of PTU-induced neutropenia and the high dosage administered during thyroid storm management. The development of agranulocytosis in a patient undergoing treatment for a thyroid storm poses significant clinical challenges. The risk of infection increases substantially, complicating the management of thyroid storm, which is already a critical condition. Patients may present with fever and signs of infection, which can be misattributed to thyroid storm, leading to delays in appropriate management. Furthermore, the presence of agranulocytosis necessitates the discontinuation of PTU, which can hinder the control of hyperthyroidism and exacerbate the thyroid storm.10
Importantly, there is a significant risk of cross-reactivity between carbimazole and propylthiouracil (PTU), with approximately 15%–20% of patients who develop agranulocytosis from one antithyroid drug potentially experiencing the same adverse reaction if switched to the other.13 Interestingly, our patient had no prior episode of agranulocytosis despite long-term treatment with a high dose of carbimazole (45 mg daily). However, she developed agranulocytosis shortly after switching to PTU. This unexpected response provided an opportunity to cautiously reintroduce carbimazole at a lower dose, under very close monitoring, while awaiting the availability of bridging therapy. On the fifth day, the full neutrophil recovery was achieved in our patient, which aligns with literature reporting that the average recovery time of agranulocytosis is within 13 days.11
Bridging therapies are essential to stabilize thyroid hormone levels while addressing the underlying agranulocytosis. Key interventions include cholestyramine and potassium iodide (SSKI) to reduce circulating free T4 and T3 levels.4,5,14 Corticosteroids play a crucial role by inhibiting peripheral T4-to-T3 conversion and reducing the inflammatory response.3,8 Lastly, beta-blockers, such as propranolol, are routinely employed to alleviate adrenergic symptoms and inhibit peripheral T4-to-T3 conversion, delivering dual benefits in the management of thyroid storm.1,4 In cases of severe thyroid storm and when conventional treatments fail or are contraindicated, current guidelines from the American Society for Apheresis recommend considering therapeutic plasma exchange as salvage therapy.15 Total thyroidectomy serves as a definitive curative option, and early surgical intervention is particularly advantageous in cases complicated by PTU-induced agranulocytosis, which aligns with existing guidelines that advocate for surgery as the definitive treatment in refractory thyroid storm or cases of antithyroid drug intolerance.8,14
Conclusion
This case illustrates a high-risk therapeutic paradox in thyroid storm management: the abrupt onset of severe PTU-induced agranulocytosis during high-dose therapy can necessitate immediate drug withdrawal at a time when hormonal control is most critical. The key learning point is that structured bridging therapy, cautious reassessment of cross-reactivity risk, and early multidisciplinary planning for definitive treatment can achieve safe stabilization without precipitating rebound thyroid storm. Clinicians managing thyroid storm should anticipate this complex high-risk scenario and initiate predefined alternative therapeutic strategies when standard therapy becomes contraindicated.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved for publication by the Institutional Review Board of Qatif Central Hospital, Eastern Province, Saudi Arabia (QCH SREC055/2025, approved on 14 September 2025). Written informed consent was obtained from the patient for publication of this case report, including the publication of clinical details and accompanying images.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vicente N, Cardoso L, Barros L, Carrilho F. Antithyroid drug-induced agranulocytosis: state of the art on diagnosis and management. Drugs RD. 2017;17(1):91–7. doi:10.1007/s40268-017-0172-1
2. Snyder S, Joseph M. The perfect storm: a case of ischemic stroke in the setting of thyroid storm. Cureus. 2020;12(5):e7992. doi:10.7759/cureus.7992
3. Yu W, Wu N, Li L, Wang J, OuYang H, Shen H. Side effects of PTU and MMI in the treatment of hyperthyroidism: a systematic review and meta-analysis. Endocr Pract. 2020;26(2):207–217. doi:10.4158/EP-2019-0221
4. Andrès E, Lorenzo-Villalba N, Mourot-Cottet R, et al. Severe Neutropenia and agranulocytosis related to antithyroid drugs: a study of 30 cases managed in a single reference center. Medicines. 2020;7(3):15. doi:10.3390/medicines7030015
5. Yoshimura Noh J, Inoue K, Suzuki N, et al. Dose-dependent incidence of agranulocytosis in patients treated with methimazole and propylthiouracil. Endocr J. 2024;71(7):695–703. doi:10.1507/endocrj.EJ24-0135
6. García Gómez C, Navarro E, Alcázar V, et al. Therapeutic management and long-term outcome of hyperthyroidism in patients with antithyroid-induced agranulocytosis: a retrospective, multicenter study. J Clin Med. 2023;12(20):6556. doi:10.3390/jcm12206556
7. Miller A, Silver KD. Thyroid storm with multiorgan failure treated with plasmapheresis. Case Rep Endocrinol. 2019;2019(1):2475843. doi:10.1155/2019/2475843
8. Shaikh UN, Ghoto MA, Dayo A, Arain MI, Parveen R. Propylthiouracil: a thyro-suppressive as well as haemato-suppressive to induce agranulocytosis in hyperthyroid patients. RADS J Pharm Pharm Sci. 2020;8(4):1–6. doi:10.37962/jpps.v8i4.429
9. Huang C, Li K, Wu J, Wang P, Juang J. Antithyroid drug-induced agranulocytosis: report of 13 cases. Chang Gung Med J. 2007;30(3):242–248.
10. Candoni A, De Marchi F, Vescini F, et al. Graves’ disease thyrotoxicosis and propylthiouracil related agranulocytosis successfully treated with therapeutic plasma exchange and g-csf followed by total thyroidectomy. Mediterr J Hematol Infect Dis. 2017;9(1):e2017058. doi:10.4084/mjhid.2017.058
11. Yang J, Zhu Y-J, Zhong -J-J, et al. Characteristics of antithyroid drug–induced agranulocytosis in patients with hyperthyroidism: a retrospective analysis of 114 cases in a single institution in China involving 9690 patients referred for radioiodine treatment over 15 years. Thyroid. 2016;26(5):627–633. doi:10.1089/thy.2015.0439
12. Debbyousha M, Zufry H. Diagnosis and management of antithyroid drug induced agranulocytosis. Procee Malikussaleh Int Conf Health Disaster Med. 2022;1(1):48–56. doi:10.29103/micohedmed.v1i1.27
13. Han JY, Lee JM, Jung SY, et al. Comparison of agranulocytosis and anti-neutrophil cytoplasmic antibody-associated vasculitis caused by two antithyroid drugs: a pharmacovigilance study using the WHO international database. Fundam Clin Pharmacol. 2024;38(4):780–788. doi:10.1111/fcp.12991
14. Rabelo PN, Rabelo PN, Paula AFD, et al. Propylthiouracil-induced agranulocytosis as a rare complication of antithyroid drugs in a patient with Graves’ disease. Rev Assoc Med Bras. 2019;65(6):755–760. doi:10.1590/1806-9282.65.6.755
15. Hoque A. Therapeutic plasma exchange in the management of impending thyroid storm: experience from Bangladesh. J Med Sci Clin Res. 2019;7(5):793–798. doi:10.18535/jmscr/v7i5.127
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.