Back to Journals » Clinical Ophthalmology » Volume 16
Propylene Glycol and Hydroxypropyl Guar Nanoemulsion - Safe and Effective Lubricant Eye Drops in the Management of Dry Eye Disease
Authors Srinivasan S, Williams R
Received 9 June 2022
Accepted for publication 15 September 2022
Published 10 October 2022 Volume 2022:16 Pages 3311—3326
DOI https://doi.org/10.2147/OPTH.S377960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sruthi Srinivasan, Ravaughn Williams
Alcon Research LLC, Johns Creek, GA, 30097, USA
Correspondence: Sruthi Srinivasan, Alcon Research LLC, 11460 Johns Creek Parkway, Johns Creek, GA, 30097, USA, Tel +1 678 415 5315, Email [email protected]
Abstract: Dry eye disease (DED) is a chronic condition of the ocular surface characterized by a loss of the tear film homeostasis and accompanied by symptoms such as eye discomfort and visual disturbances. DED is classified as aqueous deficient dry eye (ADDE), evaporative dry eye (EDE), and mixed dry eye etiologies. The mainstay treatment in the management of DED is artificial tear drops or lubricant eye drops that replenish the aqueous and/or lipid layer of the tear film. These are available as both lipid-based and non-lipid-based formulations, with/without preservatives. Lipid-based lubricant eye drops can stabilize the tear film lipid layer, reduce tear evaporation, and improve signs of EDE. In this review, we present the formulation components, mechanism of action, and summary of preclinical and clinical evidence on a lipid-based formulation – propylene glycol-hydroxypropyl guar (PG-HPG) nanoemulsion lubricant eye drops (SystaneTM Complete). These eye drops consist of the demulcent (lubricant), PG (0.6%). HPG forms a soft, thin, cross-linked in situ gel matrix with borate ions, when exposed to the tear film, which prolongs lubricant retention and provides ocular surface protection. Dimyristoyl phosphatidyl glycerol, an anionic phospholipid, helps in replenishing the lipid layer of the tear film. Moreover, the nanoemulsion formulation serves as a depot for delivery of dimyristoyl phosphatidyl glycerol to enhance ocular surface coverage. Preclinical and clinical evidence demonstrate that PG-HPG nanoemulsion lubricant eye drops are safe and effective in providing temporary relief of symptoms of DED, regardless of its subtypes. Specifically, it provides sustained reduction in dry eye symptoms, improves tear film stability/lipid layer grade, and improves ocular surface characteristics.
Keywords: artificial tears, aqueous deficient dry eye, dry eye syndrome, evaporative dry eye, lipid-based eye drops, mixed dry eye
Introduction
Dry Eye Disease
Dry eye disease (DED) is a chronic condition impacting ≥30 million people in the United States and ≥344 million people globally.1 It is a multifactorial disease of ocular surface characterized by a loss of tear film homeostasis, and accompanied by ocular symptoms such as eye discomfort and visual disturbances.2,3 The prevalence of DED with/without symptoms ranges from 5% to 50%; and based on signs alone, up to 75%.3,4 Moreover, the prevalence of DED is reportedly higher in women (9.5%) than men (6.8%); high prevalence (9.5% to 87.5%) is reported with use of digital screens (computers and smartphones).5,6
DED can be classified as aqueous deficient dry eye (ADDE), evaporative dry eye (EDE), and mixed DED.3,7 ADDE is due to tear underproduction by the lacrimal glands. EDE can occur due to causes related to either lid (meibomian gland dysfunction [MGD] or blink-related) or ocular surface (mucin deficiency and contact lens wear), resulting in abnormal lipid secretion, tear film instability, and excessive evaporation of tears.3 Although EDE is considered a leading cause of DED, ADDE can occur without obvious signs of EDE and vice versa. Therefore, as DED progresses, it increasingly adapts clinical characteristics of both ADDE and EDE, that is known as mixed DED.3,8 DED patients across the United States were approximately 3 times more likely to be subclassified as EDE (characterized by MGD) than ADDE; and approximately 36% of patients had mixed DED.7,9 Further, iatrogenic DED could be caused by topical or systemic drugs, contact lens wear, and ophthalmic surgical/non-surgical procedures. Goblet cells, which produce mucins and contribute to the stability of the tear film and immune defenses, are extremely sensitive to toxic/inflammatory stress and are reduced in density after exposure to iatrogenic factors.10,11 Owing to the multifactorial nature of DED, medications that can target multiple underlying pathologies simultaneously are desirable.12
Treatment goal for DED is to restore ocular surface and tear film homeostasis. Current treatment options in the management of DED include artificial tears or ocular lubricants, nutraceuticals, anti-inflammatory agents, tear stimulants, autologous serum, antibiotics, and other therapies (eg, physical treatments such as warm compresses, complementary medicines such as herbal products, punctal occlusion, and surgical approaches).7,13,14
Artificial Tears
Artificial tears, which substitute or supplement the natural tear film, are the first line option in the management of DED.2,7 Artificial tears improve symptoms (burning, irritation, and/or discomfort), and provide temporary relief of dryness of the eye, but have not been shown to treat pathophysiology of DED.2,7,15 Ideal artificial tears should spread uniformly and evenly, minimize friction during blinks, have minimal visual disturbance upon instillation, be safe/convenient to use, and effectively improve the signs/symptoms of DED.12,16
Artificial tears are formulated with polymeric lubricants, demulcents, buffering agents (compatible with ocular pH of approximately 7.5), electrolytes, osmolality adjusting excipients, and surfactants, with/without preservatives.15 Most of artificial tears are formulated to supplement either lipid layer or aqueous layer of the tear film.16 However, some eye drops are formulated as emulsions, which contain aqueous lubricants (such as hydroxypropyl guar [HPG], polyethylene glycol [PEG], and propylene glycol [PG]) and lipid ingredients (such as phospholipid and mineral oil). Lipid-based artificial tears have been shown to stabilize the tear film lipid layer, reduce tear evaporation, and improve the signs of MGD and EDE.17–20
One of the major challenges with eye drops is low retention time.7,12 To increase the retention time, viscosity-enhancing agents such as hyaluronic acid (HA) and carboxymethyl cellulose (CMC) are incorporated in eye drops; these agents also exhibit muco-mimetic properties and reduce desiccation by forming a protective layer on the ocular surface.7,12,21 However, eye drops with high viscosity may cause transient visual disturbances (blurred vision) and also result in debris, leading to intolerance and non-compliance.7,12 Thus, to overcome low ocular retention, in situ gelling chemistry is used; this is achieved through HPG, a natural polysaccharide, that forms a viscoelastic gel at ocular pH through cross-linking.7,15,22 HPG forms the backbone in artificial tears of the SystaneTM family (Alcon Laboratories, Inc., Fort Worth, TX, USA), which are indicated for the temporary relief of dry eye symptoms (such as burning and irritation) and ocular surface protection in patients with DED.15 Artificial tears of the SystaneTM family include non-lipid-based (PEG/PG-HPG lubricant eye drop [SystaneTM Original], PEG/PG-HPG-sorbitol lubricant eye drop [SystaneTM Ultra] and PEG/PG-HPG/sodium hyaluronate (HA)-sorbitol lubricant eye drop [SystaneTM Hydration]) as well as lipid-based (PG-HPG microemulsion lubricant eye drop [SystaneTM Balance] and PG-HPG nanoemulsion lubricant eye drop [SystaneTM Complete]) formulations.23
In this review, we present the formulation components, mechanisms of action, and the summary of literature evidence of PG-HPG nanoemulsion lubricant eye drop (SystaneTM Complete, Alcon Laboratories, Inc., Fort Worth, TX, USA) that is indicated for temporary relief of symptoms of burning and irritation in DED.
PG-HPG Nanoemulsion Lubricant Eye Drops
Formulation Components
PG-HPG nanoemulsion lubricant eye drops contain the demulcent: propylene glycol (PG; 0.6%; lubricant), and inactive ingredients: dimyristoyl phosphatidyl glycerol (anionic polar phospholipid), edetate disodium, mineral oil, polyoxyl 40 stearate, sorbitan tristearate, sorbitol, boric acid, HPG, and polyquaternium-1 (Polyquad®; preservative).15 Preservative-free formulation option is also available for PG-HPG nanoemulsion lubricant eye drops.
PG-HPG nanoemulsion lubricant eye drops (SystaneTM Complete) have similar components as that of PG-HPG microemulsion lubricant eye drops (SystaneTM Balance). However, PG-HPG nanoemulsion lubricant eye drops contain 3-fold higher concentration of HPG which enhances ocular retention of the demulcent.24 Moreover, its nanodroplets (<100 nm) help to optimize coverage area of phospholipid delivered to the tear film which improves tear film stability;24,25 it can be used to provide temporary relief of dry eye symptoms.24,26
Mechanism of PG-HPG Nanoemulsion Lubricant Eye Drops
HPG is a pH-sensitive gelling agent, and cross-links with borate ions through a condensation reaction that can occur both intramolecularly and intermolecularly.7,15,22 HPG exhibits low viscosity in solutions at pH 7 but increases in viscosity (from 10 cp to 10,000 cp) when exposed to the tear film (pH 7.5), due to the formation of a soft, thin, cross-linked in situ gel matrix with borate ions.22,27,28 Factors that control the gelation process include HPG and borate concentrations, and pH.22 HPG preferentially binds to the hydrophobic areas of the surface epithelium.22 The in situ gel matrix, due to bio-adhesive property, prolongs retention of demulcents (PG) on the damaged ocular surface.20,22,29 The layer of adsorbed HPG molecules forms a scaffold that holds the in situ gel; the gel layer spreads over cornea and conjunctiva (along with retained demulcents), and lubricates the eye, reduces tear film desiccation, enhances tear-film stabilization, and allows the repair of ocular surface epithelium.17,20,22,27 The non-Newtonian characteristics (shear-thinning behavior) of HPG causes an increase in viscosity between blinks and a decrease in viscosity during blinks; which is advantageous for longer retention on the eye and comfort on the ocular surface.15,29–31 HPG in lubricant eye drops, owing to the characteristics described previously, lowers tear osmolarity and corneal dryness to provide long-lasting relief from DED symptoms.17,32–37 Overall, in situ HPG/borate gel complex prolongs the retention of demulcent (PG), enhances tear film stability and protects the ocular surface, thereby reducing the symptoms of DED.
Moreover, nanosized droplets of oil-in-water nanoemulsion serves as better depot for delivery of dimyristoyl phosphatidyl glycerol, an anionic phospholipid.24 Dimyristoyl phosphatidyl glycerol migrates toward the top of the tear film, and fuses with the tear lipids to supplement the gaps developed due to tear film lipid insufficiency; replenishing the tear film lipid layer.38 Therefore, PG-HPG nanoemulsion lubricant eye drops serve as tear replacement solution in patients with DED due to lipid deficiency, aqueous deficiency, and/or mixed dry eye.24
Multidose Preservative-Free PG-HPG Nanoemulsion with Novelia
DED is chronic and progressive in nature, and may require repeated and long-term application of lubricant eye drops.39 Thus, to maintain the sterility of multidose lubricant eye drops, antimicrobial preservatives such as benzalkonium chloride and polyquaternium-1 are commonly used in the formulations.39 Polyquaternium-1 (Polyquad®, Alcon Inc., Fort Worth, TX, USA) is a quaternary ammonium compound with antimicrobial activity similar to benzalkonium chloride.40 Although both preservatives are effective, several studies demonstrated that polyquaternium-1 is less cytotoxic to ocular surface and more safe than benzalkonium chloride.41–43 Polyquaternium-1 is safe for mammalian cells owing to its large molecular size that reduces cell penetration.39,40 However, the possible effects of polyquaternium-1 on the tear film, and tolerance in patients with dry eye remain to be fully investigated.10
Long-term application of artificial tears containing preservatives can cause epithelial damage and ocular surface alteration.44 Several studies have suggested that non-preserved drops should be used, whenever possible, to avoid eye irritation.39 TFOS DEWS II also recommends using non-preserved eye drops to minimize preservative-induced toxicity.7 Overall, preservative-free drops may be a better choice for patients who have pre-existing ocular surface conditions and/or need frequent instillation of eye drops in DED.
Preservative-free lubricant eye drops are dispensed in either unit dose or multidose systems. Unit dose vials are expensive, bulky, and difficult-to-use.45 Further, although the multidose preservative-free bottles improve patient compliance and limit wastage, they have challenges of filtering solution/air and avoiding bacterial entry.45,46 Therefore, multidose bottles with an intelligent design comprising unidirectional valves and a venting system (to maintain sterility of product, and to avoid contamination) are used to deliver safe, preservative-free eye drops.47 Novelia (Novelia®, Nemera, La Verpillière, France) is one such multidose system that avoids the need for preservatives in the formulation, and prevents contamination over the duration of treatment.46 One of the features of Novelia include the silicone membrane barrier system and a non-return valve.46 The non-return valve in the system restricts the back flow of the contaminated liquid once dispensed from the container, thus removing the need to filter the liquid; the silicone membrane is made of solid, non-porous material that filters air and prevents entry of contaminated air.46
The previously-mentioned properties of formulation components, and mechanisms of action make PG-HPG nanoemulsion an ideal lubricating eye drop with a prolonged retention, and sustained lubrication to improve signs and symptoms in DED. This has been further supported by preclinical and clinical evidence as follows.
Preclinical and Clinical Studies of PG-HPG Nanoemulsion Lubricant Eye Drops in the Treatment of DED
A literature search was performed systematically using PubMed database, to identify pre-clinical and clinical studies reporting the efficacy/effectiveness and safety of PG-HPG nanoemulsion lubricant eye drops in alleviating the signs and symptoms of dry eye in patients with DED. Search strings used in the database were:
1. (((dry eye) OR (dry eye syndrome) OR (dry eye disease)) AND ((artificial tears) AND (lubricant)));
2. (((Propylene glycol) AND (hydroxypropyl guar)) AND ((artificial tears) OR (lubricant) OR (lubricant eye drops)));
3. (((Propylene glycol) AND (hydroxypropyl guar)) AND ((Dry eye) OR (Dry eye disease) OR (Dry eye syndrome))); and
4. (((Dry eye) OR (dry eye syndrome) OR (dry eye disease)) AND ((artificial tears) OR (lubricant) OR (lubricant eye drops) OR (eye drops)) AND (Systane Complete) OR ((HP guar) OR (hydroxypropyl guar))).
Figure 1 describes the flow chart of literature screening process, with key inclusion and exclusion criteria. Articles were screened for studies published from January 2017 to February 2022 and in English language. After removing duplicates, 236 articles were identified; of these, 9 relevant articles with preclinical or clinical studies were included after screening (Figure 1). Moreover, 1 abstract was identified using the same inclusion criteria from Google Scholar, and was considered for inclusion in this review. A total of 10 studies (preclinical and clinical) were evaluated and reviewed with common consensus of all authors. Tables 1–3 represent the methods, population, treatment, outcomes and results of preclinical and clinical studies.
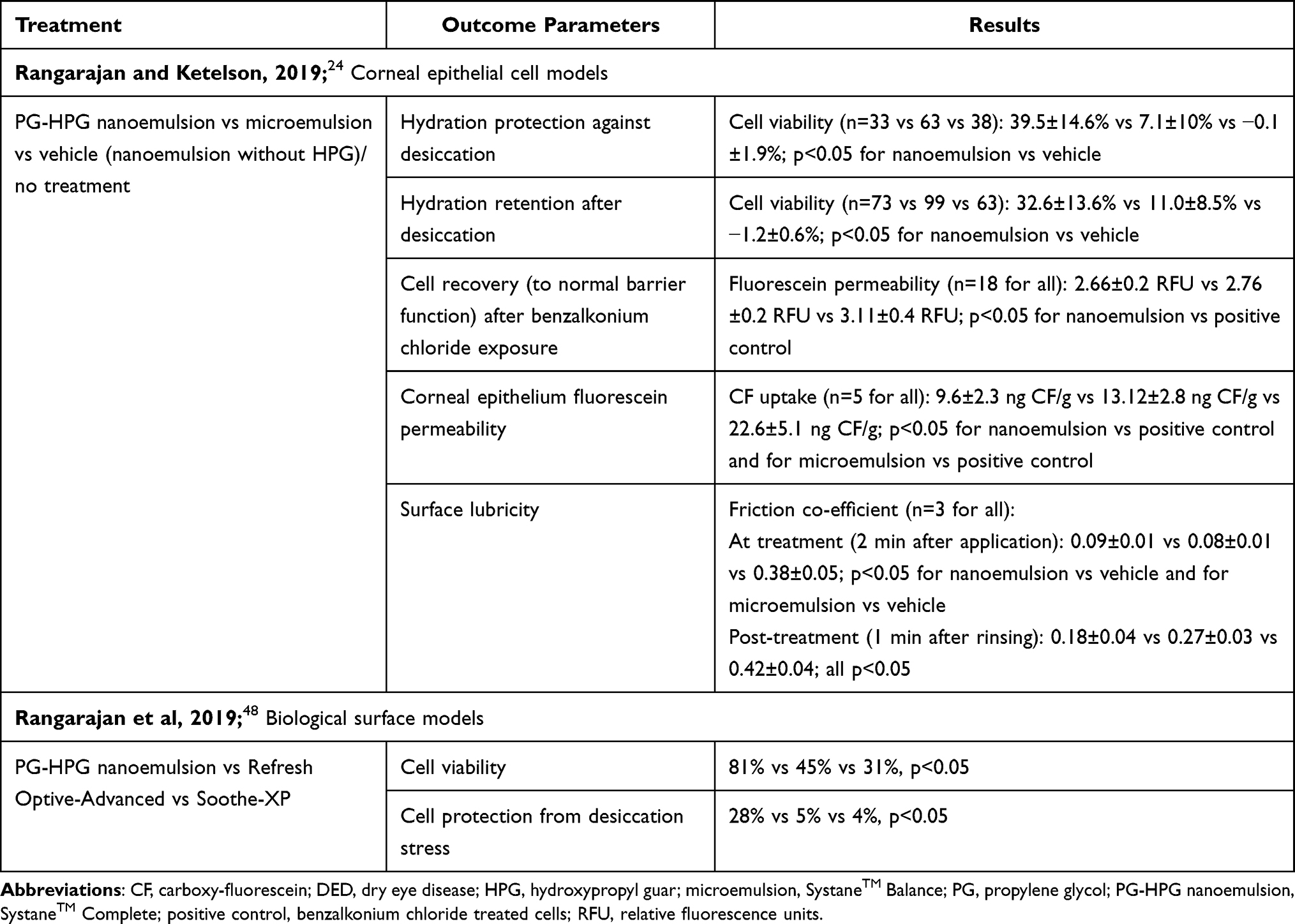 |
Table 1 Preclinical Studies of PG-HPG Nanoemulsion Lubricant Eye Drops in the Treatment of DED |
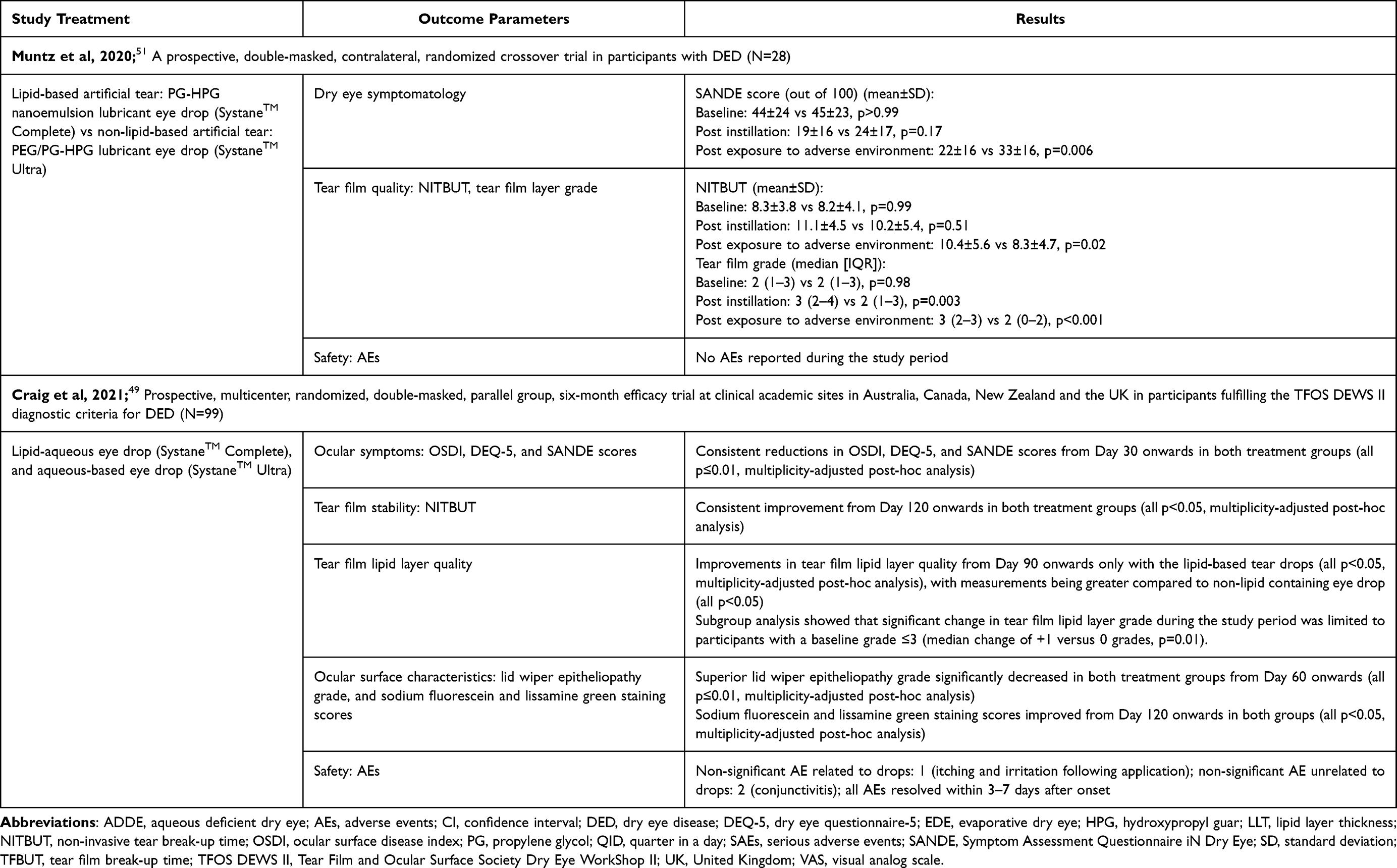 |
Table 2 Clinical Studies of PG-HPG Nanoemulsion Lubricant Eye Drops in the Management of DED |
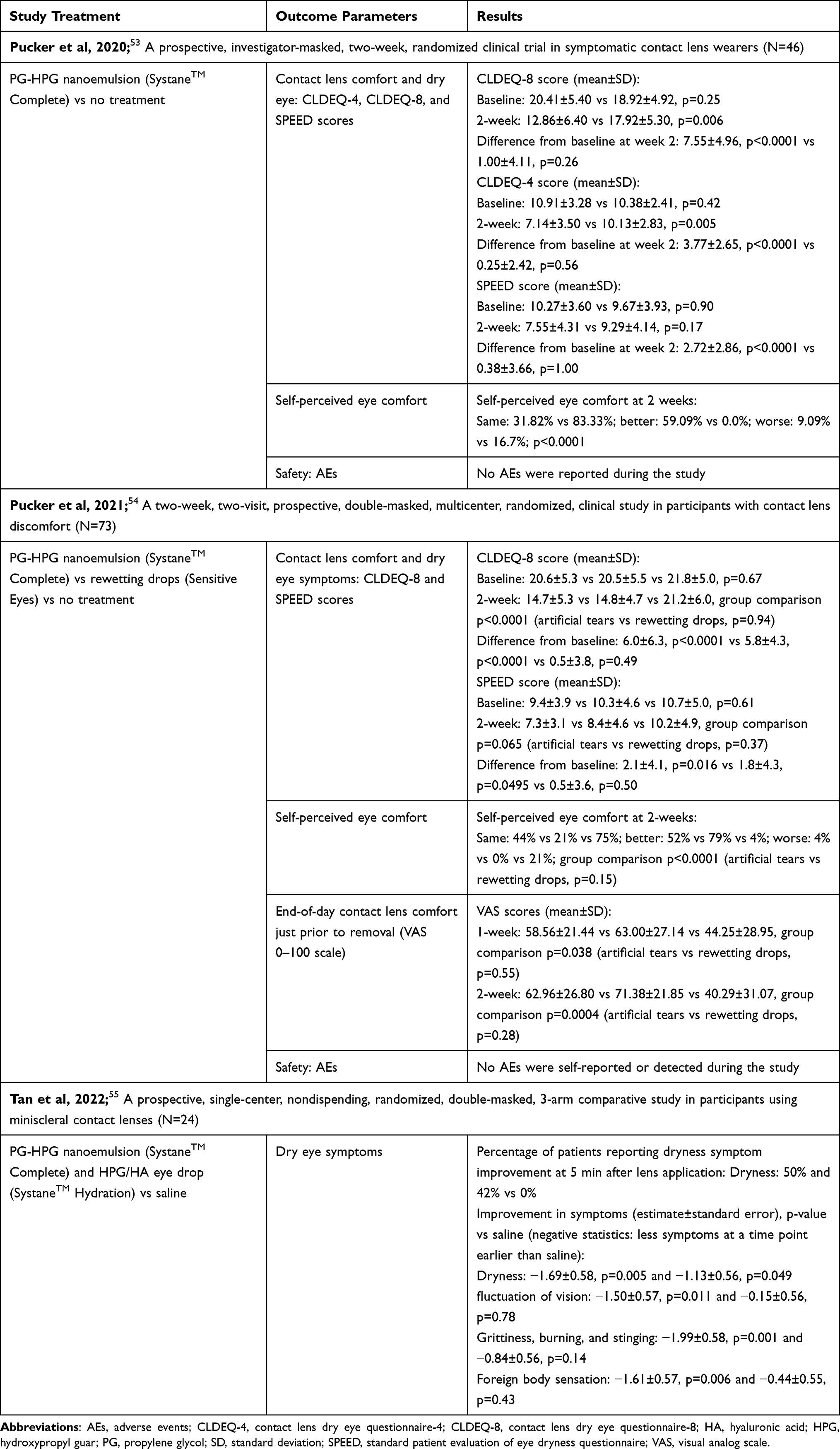 |
Table 3 Clinical Studies of PG-HPG Nanoemulsion Lubricant Eye Drops in Improvement of Contact Lens Discomfort |
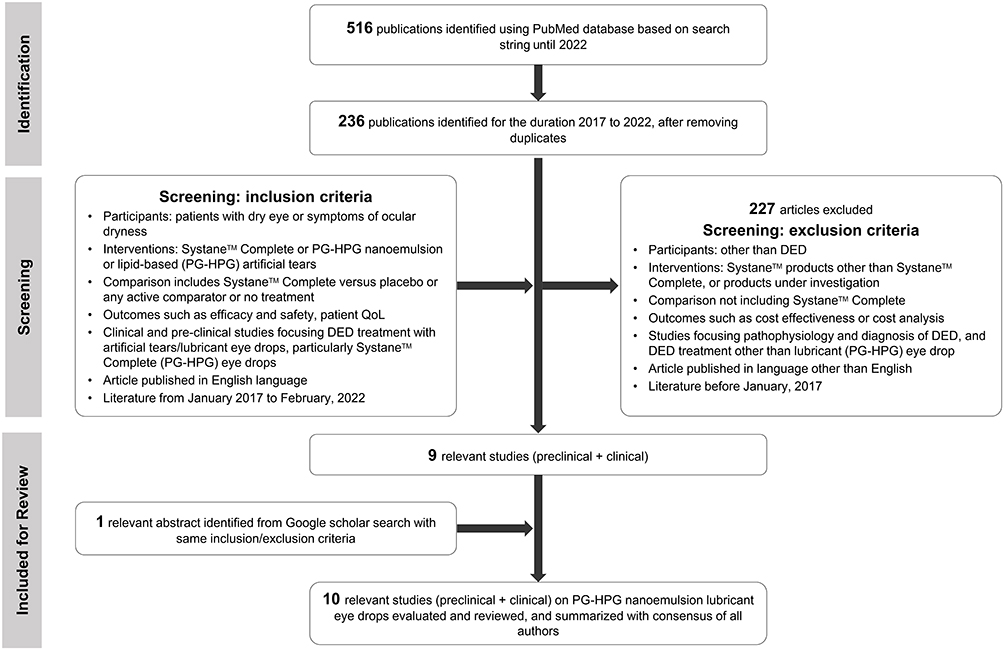 |
Figure 1 Flow chart of literature screening strategy, with key inclusion and exclusion criteria. Search strings: 1. (((dry eye) OR (dry eye syndrome) OR (dry eye disease)) AND ((artificial tears) AND (lubricant))); 2. (((Propylene glycol) AND (hydroxypropyl guar)) AND ((artificial tears) OR (lubricant) OR (lubricant eye drops))); 3. (((Propylene glycol) AND (hydroxypropyl guar)) AND ((Dry eye) OR (Dry eye disease) OR (Dry eye syndrome))); and 4. (((Dry eye) OR (dry eye syndrome) OR (dry eye disease)) AND ((artificial tears) OR (lubricant) OR (lubricant eye drops) OR (eye drops)) AND (Systane Complete) OR ((HP guar) OR (hydroxypropyl guar))). Abbreviations: DED, dry eye disease; HPG, hydroxypropyl guar; PG, propylene glycol; QoL, quality of life. |
Preclinical and clinical studies have demonstrated that PG-HPG nanoemulsion lubricant eye drops are associated with improvements in the signs and symptoms of dry eye, and are well tolerated in patients with DED, irrespective of its subtypes.
Preclinical Evidence
Long-lasting Lubrication and Ocular Surface Protection with PG-HPG Nanoemulsion Eye Drops
Preclinical evaluation using different corneal epithelial models demonstrated the effectiveness of PG-HPG nanoemulsion artificial tear formulation compared to vehicle/control and microemulsion for treatment of DED (Table 1).24 In human corneal epithelial cells, PG-HPG nanoemulsion showed higher hydration protection and retention against desiccation compared to vehicle (approximately 32- to 40- fold higher; p<0.05) and microemulsion (approximately 3- to 5.5-fold higher; p<0.05).24 PG-HPG nanoemulsion showed higher cell recovery at 48 hours after benzalkonium chloride-exposure of human corneal epithelial cells (p<0.05 for PG-HPG nanoemulsion vs positive control).24 Moreover, in simulated blinking experiment, surface friction in bovine pericardial samples was significantly lower with PG-HPG nanoemulsion versus microemulsion and versus vehicle, during posttreatment (1 minute after removal of treatment; both p<0.05).24 Additionally, elastic filament strength was significantly higher with PG-HPG nanoemulsion versus microemulsion and versus vehicle (polymer filament break-up time [PFBUT] at 10−1 s shear rate: 0.031±0.008 s vs 0.016±0.005 s vs 0.017±0.001 s, both p<0.05).24 Overall, PG-HPG nanoemulsion (vs vehicle and/or microemulsion) showed greater hydration protection and retention, higher cell recovery, better cell barrier function, higher surface lubricity, and increased elastic filament strength in corneal epithelial models.24 In another preclinical study, Rangarajan et al48 assessed the performance of phospholipid containing PG-HPG nanoemulsion in comparison to two other lipid-containing artificial tears (Refresh Optive-Advanced; and Soothe-XP) using biological surface models. PG-HPG nanoemulsion (vs Refresh Optive-Advanced, and vs Soothe-XP) showed significantly (p≤0.05) greater cell viability and cell protection against desiccation, and improved lubrication. These results suggest that the phospholipid containing PG-HPG nanoemulsion provides long-lasting lubrication and surface protection in the eye, compared to other lipid-containing eye drops (Table 1).48
Clinical Evidence
PG-HPG Nanoemulsion Lubricant Eye Drops in the Treatment of All DED Subtypes
Recently, Craig et al49 demonstrated the treatment of DED according to disease subtype and severity. In a multicenter, double-masked, parallel group, randomized controlled trial, 99 participants (mean age, 44±16 years; 64% female) with DED were enrolled. Participants instilled either lipid-based PG-HPG nanoemulsion drops (SystaneTM Complete) or non-lipid-based aqueous drops (SystaneTM Ultra) ≥4 times daily for 6 months; dry eye symptomology, and tear film and ocular surface characteristics were assessed.49 Both treatments demonstrated sustained reduction in DED symptoms (Ocular Surface Disease Index [OSDI], Dry Eye Questionnaire-5 [DEQ-5], and Symptom Assessment Questionnaire iN Dry Eye [SANDE] scores) from Day 30 onwards (all p≤0.01) and decreased superior lid wiper epitheliopathy grades from Day 60 onwards (all p≤0.01) (Table 2).49 Further, non-invasive tear film breakup time (NITBUT), and sodium fluorescein and lissamine green staining scores consistently improved from Day 120 onwards in both groups (all p<0.05).49 Tear film lipid layer grades increased only with PG-HPG nanoemulsion eye drops (from Day 90 onwards); with significantly greater improvement in patients with low lipid layer thickness at baseline (lipid layer grade ≤3; p=0.01).49 Hence, both lipid-based and non-lipid-based artificial tears provided symptom relief within a month.49 Improvements in the tear film stability and ocular surface characteristics were slower than the symptomatic improvements.49 Further, both formulations showed long-term efficacy and a good tolerability profile across DED subtypes; however, improvement in tear film lipid layer grade was observed only with PG-HPG nanoemulsion drops; particularly in subgroup of patients with evaporative DED due to tear lipid insufficiency (with baseline lipid layer grade ≤3) (Table 2).49 In line with this study, data from previous clinical trials also demonstrated similar findings with PG-HPG nanoemulsion (SystaneTM Complete) for the treatment of dry eye symptoms in all DED types.38,50 In a Phase IV, open-label, single-arm, multicenter trial, patients with DED (N=134; 56.6±14.8 years; 75.4% female) instilled one drop of PG-HPG nanoemulsion in each eye, twice daily for 28 days.50 The instillation of PG-HPG nanoemulsion eye drops increased tear film break-up time (TFBUT) by 1.5±2.8 seconds at 14 days; and the improvement remained consistent through 28 days (Table 2).50 It also improved (decreased) ocular discomfort at 14 days (mean±SD change in visual analog scale [VAS] score, −17.3±24.80).50 Moreover, subgroup analysis of patients with ADDE, EDE, and mixed DED indicated that PG-HPG nanoemulsion was effective and well tolerated in all three types of DED. PG-HPG nanoemulsion improved tear film stability, and signs and symptoms of DED.50
The short-term effects of PG-HPG nanoemulsion were assessed by Silverstein et al.38 The study reported that a single drop of PG-HPG nanoemulsion provided immediate and sustained symptom relief up to 8 hours, and was well tolerated in all DED subtypes (Table 2). In the overall cohort, improvement in dry eye symptom scores (VAS) was observed as early at 0 hours and lasted until 8 hours after eye drop instillation on Day 1 (median change in symptom score from baseline [95% CI], −1.0 [−3.0, −1.0] at 0 hours, −2.0 [−3.0, −2.0] at 4 hours, and −2.0 [−2.0, −1.0] at 8 hours).38 A majority of patients (>80%) had a soothing sensation as early at 0 hours which persisted throughout 8 hours (median soothing sensation score on VAS, 3 at 0 hours, 3 at 4 hours, and 3.5 at 8 hours; range, 0–10). Subgroup analyses demonstrated improvements in dry eye symptom scores and soothing sensation scores, over 8 hours, in all dry eye subtypes (ADDE, EDE, and mixed DED) that were comparable to the overall cohort (Table 2).38 A majority of patients (>92%) had no or minimal symptoms of burning sensation, stinging sensation, blur and foreign body sensation on a tolerability assessment (Table 2).38 Overall, PG-HPG nanoemulsion lubricant eye drops were effective in the improvement of ocular symptoms and tear film stability, and well tolerated in DED patients, regardless of its types; provided prominent improvement of lipid layer grade in patients with EDE due to tear lipid insufficiency.38,49,50
PG-HPG Nanoemulsion Lubricant Eye Drops in Prophylactic Treatment of DED Under Environmental Conditions
In a prospective, double-masked, contralateral, randomized cross-over trial (N=28; mean age, 29±9 years; 57% female), lipid-based (PG-HPG nanoemulsion; SystaneTM Complete) and non-lipid-based (SystaneTM Ultra) artificial tear drops were evaluated for their prophylactic benefits in a simulated adverse environment.51 Both eye drops improved the SANDE scores and NITBUT after instillation. After adverse environment exposure, the improvement in SANDE scores (p=0.006) and NITBUT (p=0.02) were significantly greater with lipid-based compared to non-lipid-based artificial tear drops (Table 2).51 Moreover, improvement in tear film lipid layer grades after adverse environment exposure was greater in patients treated with lipid-based artificial tear drops than those with non-lipid-based artificial tear drops (p<0.001).51 In this study, lipid containing PG-HPG nanoemulsion lubricant eye drops had superior prophylactic efficacy against adverse environment exposure in patients with DED.51
PG-HPG Nanoemulsion Lubricant Eye Drops in Treatment of DED with Low Lipid Layer Thickness
A study by Weisenberger et al52 evaluated the effects of two eye drops (PG-HPG nanoemulsion and non-emollient) on lipid layer thickness (LLT) and dry eye symptoms. Part 1 was a double-masked, cross-over, randomized study in which diurnal effects of single-drop instillation were evaluated. This was followed by Part 2, an observational study, which assessed the effects of 1-month use of nanoemulsion eye drops in all subjects. Overall, 20 subjects (mean age, 45.6±7.9 years, 15 female) completed the study. Of this, 15 subjects with low baseline LLT (<50 nm) had a significant increase in LLT at 15 min after instillation of PG-HPG nanoemulsion eye drops (overall, 8.51±13.95, p=0.03 vs baseline; inferior third, 9.15±14.60, p=0.03 vs baseline); LLT values did not increase significantly with the non-emollient eye drops.52 In all subjects, both eye drops showed improvement (reduction) in ocular dryness up to 6 h after instillation (change in VAS scores [±SD] from baseline: PG-HPG nanoemulsion eye drops, 8.6±16.7 mm, p=0.03; non-emollient eye drops, 9.8±19.9, p=0.02). However, 1-month observational study revealed no significant improvement in LLT with 1-month use of PG-HPG nanoemulsion QID (4 times in a day). Further, significant improvement in dryness was observed even after 1-month QID use of PG-HPG nanoemulsion (change in VAS scores [±SD] from baseline to 1 month: 10.2±21.2; p=0.045).52 PG-HPG nanoemulsion also improved ocular surface symptoms as indicated by a decrease in OSDI score from baseline to 1-month post-eye drop QID use (5.3 units, p=0.03).52
In this study, PG-HPG nanoemulsion was associated with short-term changes in LLT, with no effects sustained over 1 month of QID use.52 However, a study by Craig et al49 showed consistent improvement in tear film lipid layer grades from 90 days onwards with daily use of PG-HPG nanoemulsion. Moreover, a study by Muntz et al51 also demonstrated improvement in tear film lipid layer grades with the use of PG-HPG nanoemulsion eye drops, with the effect being sustained even after exposure to adverse environment. Overall, both single dose and sustained use of PG-HPG nanoemulsion eye drops demonstrated improvement in dry eye symptoms (Table 2).52
PG-HPG Nanoemulsion Lubricant Eye Drops in Improvement of Contact Lens Discomfort
In a prospective, investigator-masked, 2-week, randomized clinical trial,53 46 adult subjects (symptomatic Contact Lens Dry Eye Questionanire-8 scores [CLDEQ-8 scores] ≥12) were recruited to evaluate PG-HPG nanoemulsion eye drops in treating contact lens discomfort. Subjects were randomized to either no treatment (n=24; mean age, 28.8±11.2 years; 20.8% female) or to PG-HPG nanoemulsion eye drops (before and after contact lens use; n=22; mean age, 32.7±13.1 years; 9.1% female). Clinical signs and symptoms at baseline and 2 weeks were assessed (Table 3). Subjects using PG-HPG nano-emulsion eye drops had significantly better symptom scores (CLDEQ-4, CLDEQ-8 and standard patient evaluation of eye dryness questionnaire [SPEED] scores) at 2 weeks compared to baseline (p<0.0001); whereas, symptoms did not differ significantly in the group without treatment (p>0.05).53 Moreover, CLDEQ-8 and CLDEQ-4 scores at 2 weeks were significantly better in subjects with PG-HPG nanoemulsion than those without treatment (12.86±6.40 vs 17.92±5.30, p=0.006; and 7.14±3.50 vs 10.13±2.83, p=0.005, respectively); SPEED scores at 2 weeks were similar between both groups (p=0.17). Clinical signs (such as NITBUT, corneal staining, and Schirmer’s test) were not significantly different at 2 weeks versus baseline in either group (all p>0.05). Similarly, at 2 weeks, clinical signs were not significantly different between the two groups (all p>0.05).53 Further, more subjects reported “better” perceived eye comfort at 2 weeks with PG-HPG nanoemulsion eye drops than those without treatment (59.09% vs 0.0%, p<0.001).53 These data suggest that PG-HPG nanoemulsion application before and after contact lens wear could be used to improve contact lens discomfort in symptomatic subjects who wear contact lenses.53
Another prospective, 2-week, double-masked, randomized, clinical trial compared PG-HPG nanoemulsion (SystaneTM Complete) vs rewetting drops (Sensitive Eyes®) vs no treatment in 73 participants (mean age, 30.3±11.5 years; 18% male) with contact lens discomfort and CLDEQ-8 scores ≥12.54 The study reported significant improvement in CLDEQ-8 scores at 2 weeks compared to baseline in both PG-HPG nanoemulsion and rewetting drops groups (6.0±6.3, p<0.0001 and 5.8±4.3, p<0.0001, respectively), but not in the control group (p=0.49). CLDEQ-8 scores at 2 weeks were similar between PG-HPG nanoemulsion and rewetting drops groups (p=0.94). End-of-day contact lens comfort just before removal of contact lens was also significantly better with both PG-HPG nanoemulsion and rewetting drops versus control group after 2 weeks (62.96±26.80 and 71.38±21.85 vs 40.29±31.07, group p=0.0004); comfort experienced by subjects was similar between PG-HPG nanoemulsion and rewetting drops (p=0.28).54 Moreover, no safety concerns were reported with PG-HPG nanoemulsion eye drops when instilled in the eyes before, during, and after daily disposable contact lens wear.54
A very recent prospective, single-center, nondispensing, randomized, double-masked, three arm study evaluated filling solutions for the application of miniscleral contact lenses in participants (N=24; average age, 29.3±5.4 years; 13 female; 11 male).55 The study compared PG-HPG nanoemulsion (SystaneTM Complete), HPG/HA eye drops (SystaneTM Hydration), and no treatment (saline). Results demonstrated that PG-HPG nanoemulsion eye drop instillation in combination with non-preserved saline for application of miniscleral contact lenses during 6 hours of wear effectively improved subjective dryness (estimates±standard error [SE], −1.69±0.58, p=0.005); grittiness/burning/stinging (−1.99±0.58, p=0.001), and foreign body sensation (−1.61±0.57, p=0.006); and fluctuating vision (−1.50±0.57, p=0.011) compared to saline.55 Dryness symptoms improved faster with PG-HPG nanoemulsion and HPG/HA eye drops than saline, as indicated by higher percentage of patients reporting improvement in dryness at 5 min after lens application (50% vs 42% vs 0%).55 In this study, PG-HPG nanoemulsion eye drops (along with saline) were effective in improving various symptoms faster than saline, whereas HPG/HA eye drops only improved symptoms of dryness.55 Overall, PG-HPG nanoemulsion lubricant eye drops improved subjective outcomes of symptoms and comfort, and was well tolerated in patients with daily contact lens wear.53–55
Cumulatively, preclinical evidence showed that PG-HPG nanoemulsion lubricant eye drops provide better hydration retention and protection, greater cell viability, long-lasting lubrication, and ocular surface protection compared to other lipid-containing formulations (eg, Refresh Optive-Advanced, Soothe-XP) or microemulsion lubricant eye drops.24,48 Clinical evidence demonstrated that PG-HPG nanoemulsion lubricant eye drops were effective in the improvement of ocular symptoms and tear film stability, and well tolerated in subjects with DED, regardless of its subtypes (EDE, ADDE, and mixed DED).38,49,50 Additionally, PG-HPG nanoemulsion lubricant eye drops improved LLT, in subjects with low baseline LLT (<50 nm), compared to non-emollient lubricant eye drops.49,52 PG-HPG nanoemulsion lubricant eye drops also improved subjective outcomes of symptoms and comfort similar to rewetting drops (Sensitive Eyes®), but better than other lubricant eye drops (SystaneTM Hydration)/saline, and was well tolerated in patients with daily contact lens wear.53–55
Other lipid-based lubricant eye drops (including emulsions) have been reported to mimic the composition of the tear film, and provide ocular surface benefits to improve DED, particularly in subjects with EDE associated with MGD.12,56 Further, a systematic review reported that lipid-containing lubricants (liposomal lid sprays and lipid-containing eye drops) are effective in improving signs of dry eye.18 Preclinical evidence of liposome-based artificial tear formulations showed the potential to serve as a tear substitute by replenishing the tear film lipids, restoring the tear film, protecting corneal epithelium, and demonstrating good tolerance.12,57,58 A pilot clinical study in patients with mild-to-moderate DED reported that a new formulation of eye drops (combination of viscosity-enhancing HA, trehalose, and cationic liposomes containing stearyl amine and phospholipids) improved objective signs and subjective symptoms.59 However, there is a need for large-scale controlled clinical studies to obtain more robust evidence on the efficacy.59
The limitations of this review need to be acknowledged. The scope of the literature search was limited in obtaining and presenting evidence of PG-HPG nanoemulsion lubricant eye drops since 2017. Further, there is a paucity of evidence showing head-to-head comparison of PG-HPG nanoemulsion lubricant eye drops with other lipid-based and/or liposome-based lubricant eye drops to infer comparative efficacy.
Summary
DED is a multifactorial condition with ADDE, EDE, and mixed etiologies. Artificial tears are the backbone in the management of DED. Lipid-based lubricant eye drops with viscoelastic characteristics are beneficial in providing temporary relief of dry eye symptoms. PG-HPG and borate components in PG-HPG nanoemulsion lubricant eye drops form a thin viscoelastic layer that prolongs retention of demulcent; thus, provides long-term surface hydration and moisture retention, and ocular surface protection by improving cell barrier functions and cell recovery, and temporary relief of symptoms in DED. Moreover, it provides tear film stability between and during blinks owing to viscoelastic properties of HPG. Further, PG-HPG nanoemulsion formulation helps to optimize ocular surface coverage of lipids that is beneficial in replenishing the tear film lipid layer. Additionally, PG-HPG nanoemulsion lubricant eye drops in the form of multidose preservative-free system (with Novelia® bottles) is effective, convenient, and well tolerated in DED patients who have intolerance to preservatives with long-term eye drop use.
Clinically, PG-HPG nanoemulsion lubricant eye drops have been shown to improve dry eye symptoms, enhance tear film stability, and lipid layer thickness; hence, they help to restore eye surface health and provide symptom relief in patients with DED, regardless of subtypes. Moreover, PG-HPG nanoemulsion relieves ocular dryness and discomfort associated with daily contact lens wear, and in prophylactic treatment of dry eye against adverse environmental conditions. Conversely, other lipid-based and/or liposome-based lubricant eye drops, shown to mimic tear film composition, provide ocular surface benefits and improve signs of dry eye; however, large-scale controlled clinical studies are required to obtain more robust evidence on the efficacy.
With over a demi-decade of usage, PG-HPG nanoemulsion lubricant eye drops are effective, convenient to use, and well tolerated in DED, regardless of its subtypes.
Acknowledgments
Writing, editorial, and formatting assistance was provided by Sonali Dalwadi, PhD, and Sudha Korwar, PhD, from Indegene Pvt. Ltd. which was contracted and funded by Alcon. Alcon was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Writing, editorial support, and formatting assistance was provided by Indegene Pvt. Ltd. which was contracted and funded by Alcon.
Disclosure
The authors are employees of Alcon. The authors received no direct compensation related to the development of the manuscript. The authors report no other conflicts of interest in this work.
References
1. Dry eye redefined: TFOS DEWS II report; 2017. Available from: https://www.tfosdewsreport.org.
2. Pucker AD, Ng SM, Nichols JJ. Over the counter (OTC) artificial tear drops for dry eye syndrome. Cochrane Database Syst Rev. 2016;2016(2). doi:10.1002/14651858.CD009729.pub2
3. Craig JP, Nelson JD, Azar DT, et al. TFOS DEWS II report executive summary. Ocul Surf. 2017;15(4):802–812. doi:10.1016/j.jtos.2017.08.003
4. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
5. Al-Mohtaseb Z, Schachter S, Lee BS, Garlich J, Trattler W. The relationship between dry eye disease and digital screen use. Clin Ophthalmol. 2021;15:3811–3820. doi:10.2147/OPTH.S321591
6. Papas EB. The global prevalence of dry eye disease: a Bayesian view. Ophthalmic Physiol Opt. 2021;41(6):1254–1266. doi:10.1111/opo.12888
7. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
8. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
9. Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31(5):472–478. doi:10.1097/ICO.0b013e318225415a
10. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15(3):511–538. doi:10.1016/j.jtos.2017.05.004
11. Mohamed HB, Abd El-Hamid BN, Fathalla D, Fouad EA. Current trends in pharmaceutical treatment of dry eye disease: a review. Eur J Pharm Sci. 2022;175:106206. doi:10.1016/j.ejps.2022.106206
12. Agarwal P, Craig JP, Rupenthal ID. Formulation considerations for the management of dry eye disease. Pharmaceutics. 2021;13(2):1–19. doi:10.3390/pharmaceutics13020207
13. Aragona P, Giannaccare G, Mencucci R, Rubino P, Cantera E, Rolando M. Modern approach to the treatment of dry eye, a complex multifactorial disease: a P.I.C.A.S.S.O. board review. Br J Ophthalmol. 2021;105(4):446–453. doi:10.1136/bjophthalmol-2019-315747
14. Şimşek C, Doğru M, Kojima T, Tsubota K. Current management and treatment of dry eye disease. Turkish J Ophthalmol. 2018;48(6):309–313. doi:10.4274/tjo.69320
15. Garofalo R, Kunnen C, Rangarajan R, Manoj V, Ketelson H. Relieving the symptoms of dry eye disease: update on lubricating eye drops containing hydroxypropyl-guar. Clin Exp Optom. 2021;104(8):826–834. doi:10.1080/08164622.2021.1925208
16. Srinivasan S, Manoj V. A decade of effective dry eye disease management with Systane Ultra (polyethylene glycol/propylene glycol with hydroxypropyl guar) lubricant eye drops. Clin Ophthalmol. 2021;15:2421–2435. doi:10.2147/OPTH.S294427
17. Baudouin C, Galarreta DJ, Mrukwa-Kominek E, et al. Clinical evaluation of an oil-based lubricant eyedrop in dry eye patients with lipid deficiency. Eur J Ophthalmol. 2017;27(2):122–128. doi:10.5301/ejo.5000883
18. Lee SY, Tong L. Lipid-containing lubricants for dry eye: a systematic review. Optom Vis Sci. 2012;89(11):1654–1661. doi:10.1097/OPX.0b013e31826f32e0
19. Geerling G, Baudouin C, Aragona P, et al. Emerging strategies for the diagnosis and treatment of meibomian gland dysfunction: proceedings of the OCEAN group meeting. Ocul Surf. 2017;15(2):179–192. doi:10.1016/j.jtos.2017.01.006
20. Benelli U. Systane® lubricant eye drops in the management of ocular dryness. Clin Ophthalmol. 2011;5(1):783–790. doi:10.2147/OPTH.S13773
21. Eftimov P, Yokoi N, Melo AM, Daull P, Georgiev GA. Interactions of meibum and tears with mucomimetic polymers: a hint towards the interplay between the layers of the tear film. Int J Mol Sci. 2021;22(5):1–15. doi:10.3390/ijms22052747
22. Springs C. Novel ocular lubricant containing an intelligent delivery system: details of its mechanism of action. Dev Ophthalmol. 2010;45:139–147. doi:10.1159/000315027
23. Yeh TN, Ketelson HA, Affairs AM, America N, Worth F. White paper: evolution of Systane® artificial tears. Available from: https://us.alconscience.com/sites/g/files/rbvwei1736/files/pdf/Evolution-of-Systane®-Artificial-Tears-US-SYD-2000005.pdf.
24. Rangarajan R, Ketelson H. Preclinical evaluation of a new hydroxypropyl-guar phospholipid nanoemulsion-based artificial tear formulation in models of corneal epithelium. J Ocul Pharmacol Ther. 2019;35(1):32–37. doi:10.1089/jop.2018.0031
25. Ramamoorthy P. White paper: an overview of the current consensus, clinical impact and management of dry eye; 2018. Available from: https://alconscience.com/wp-content/uploads/2019/01/1811A23-US-SYS-18-E-2312_Dry-Eye-White-Paper_LR.pdf.
26. Systane Complete drug facts (nih.gov). Available from: https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=2df0de02-a3e2-471a-9e10-040c3fba75fe&type=display.
27. Petricek I, Berta A, Higazy MT, Németh J, Prost ME. Hydroxypropyl-guar gellable lubricant eye drops for dry eye treatment. Expert Opin Pharmacother. 2008;9(8):1431–1436. doi:10.1517/14656566.9.8.1431
28. Lu C, Kostanski L, Ketelson H, Meadows D, Pelton R. Hydroxypropyl guar-borate interactions with tear film mucin and lysozyme. Langmuir. 2005;21(22):10032–10037. doi:10.1021/la050988g
29. Ubels JL, Clousing DP, Van Haitsma TA, et al. Pre-clinical investigation of the efficacy of an artificial tear solution containing hydroxypropyl-guar as a gelling agent. Curr Eye Res. 2004;28(6):437–444. doi:10.1080/02713680490503787
30. Che Arif FA, Hilmi MR, Mohd Kamal K, Ithnin MH. Evaluation of 18 artificial tears based on viscosity and pH. Malaysian J Ophthalmol. 2020;2(2):96–111. doi:10.35119/myjo.v2i2.109
31. Arif FAC, Hilmi MR, Kamal KM, Ithnin MH. Comparison of immediate effects on usage of dual polymer artificial tears on changes in tear film characteristics. Malaysian J Med Heal Sci. 2021;17(3):252–258. doi:10.31436/imjm.v18i2.613
32. Maharana PK, Raghuwanshi S, Chauhan AK, Rai VG, Pattebahadur R. Comparison of the efficacy of carboxymethylcellulose 0.5%, hydroxypropyl-guar containing polyethylene glycol 400/propylene glycol, and hydroxypropyl methyl cellulose 0.3% tear substitutes in improving ocular surface disease index in cases of dry eye. Middle East Afr J Ophthalmol. 2017;24(4):202–206. doi:10.4103/meajo.MEAJO_165_15
33. Rolando M, Autori S, Badino F, Barabino S. Protecting the ocular surface and improving the quality of life of dry eye patients: a study of the efficacy of an HP-guar containing ocular lubricant in a population of dry eye patients. J Ocul Pharmacol Ther. 2009;25(3):271–277. doi:10.1089/jop.2008.0026
34. Sánchez MA, Arriola-Villalobos P, Torralbo-Jiménez P, et al. The effect of preservative-free HP-Guar on dry eye after phacoemulsification: a flow cytometric study. Eye. 2010;24(8):1331–1337. doi:10.1038/eye.2010.24
35. Jerkins G, Greiner JV, Tong L, et al. A comparison of efficacy and safety of two lipid-based lubricant eye drops for the management of evaporative dry eye disease. Clin Ophthalmol. 2020;14:1665–1673. doi:10.2147/OPTH.S256351
36. Ng A, Keech A, Jones L. Tear osmolarity changes after use of hydroxypropyl-guar-based lubricating eye drops. Clin Ophthalmol. 2018;12:695–700. doi:10.2147/OPTH.S150587
37. Moon SW, Hwang JH, Chung SH, Nam KH. The impact of artificial tears containing hydroxypropyl guar on mucous layer. Cornea. 2010;29(12):1430–1435. doi:10.1097/ICO.0b013e3181ca636b
38. Silverstein S, Yeu E, Tauber J, et al. Symptom relief following a single dose of propylene glycol-hydroxypropyl guar nanoemulsion in patients with dry eye disease: a phase IV, multicenter trial. Clin Ophthalmol. 2020;14:3167–3177. doi:10.2147/OPTH.S263362
39. Walsh K, Jones L. The use of preservatives in dry eye drops. Clin Ophthalmol. 2019;13:1409–1425. doi:10.2147/OPTH.S211611
40. Kathuria A, Shamloo K, Jhanji V, Sharma A. Categorization of marketed artificial tear formulations based on their ingredients: a rational approach for their use. J Clin Med. 2021;10(6):1–11. doi:10.3390/jcm10061289
41. Lee HJ, Jun RM, Cho MS, Choi KR. Comparison of the ocular surface changes following the use of two different prostaglandin F2a analogues containing benzalkonium chloride or polyquad in rabbit eyes. Cutan Ocul Toxicol. 2015;34(3):195–202. doi:10.3109/15569527.2014.944650
42. Ammar DA, Noecker RJ, Kahook MY. Effects of benzalkonium chloride- and polyquad-preserved combination glaucoma medications on cultured human ocular surface cells. Adv Ther. 2011;28(6):501–510. doi:10.1007/s12325-011-0029-x
43. Kahook MY, Noecker R. Quantitative analysis of conjunctival goblet cells after chronic application of topical drops. Adv Ther. 2008;25(8):743–751. doi:10.1007/s12325-008-0078-y
44. Zhang X, Vimalin Jeyalatha M, Qu Y, et al. Dry eye management: targeting the ocular surface microenvironment. Int J Mol Sci. 2017;18(7):1–28. doi:10.3390/ijms18071398
45. Sellier F. User testing: critical for truly understanding patient needs. ONdrugDelivery Mag. 2019;94:36–38.
46. Davidson Z. Developing an efficient ophthalmic device combination product. ONdrugDelivery Mag. 2020;104:16–19.
47. Petit Ben Saidane L, Quaglia B. How to deliver preservative-free eye drops in a multidose system with a safer alternative to filters? Invest Ophthalmol Vis Sci. 2017;58(8):4460.
48. Rangarajan R, Ketelson H, Do R, et al. Characterization of a new phospholipid containing nanoemulsion lubricant eye drop for dry eye. Invest Ophthalmol Vis Sci. 2019;60(9):303.
49. Craig JP, Muntz A, Wang MTM, et al. Developing evidence-based guidance for the treatment of dry eye disease with artificial tear supplements: a six-month multicentre, double-masked randomised controlled trial. Ocul Surf. 2021;20:62–69. doi:10.1016/j.jtos.2020.12.006
50. Yeu E, Silverstein S, Guillon M, et al. Efficacy and safety of phospholipid nanoemulsion-based ocular lubricant for the management of various subtypes of dry eye disease: a phase iv, multicenter trial. Clin Ophthalmol. 2020;14:2561–2570. doi:10.2147/OPTH.S261318
51. Muntz A, Marasini S, Wang MTM, Craig JP. Prophylactic action of lipid and non-lipid tear supplements in adverse environmental conditions: a randomised crossover trial. Ocul Surf. 2020;18(4):920–925. doi:10.1016/j.jtos.2020.08.004
52. Weisenberger K, Fogt N, Swingle Fogt J. Comparison of nanoemulsion and non-emollient artificial tears on tear lipid layer thickness and symptoms. J Optom. 2020;14(1):20–27. doi:10.1016/j.optom.2020.03.002
53. Pucker AD, McGwin G, Franklin QX, Nattis A, Lievens C. Evaluation of Systane Complete for the treatment of contact lens discomfort. Contact Lens Anterior Eye. 2020;43(5):441–447. doi:10.1016/j.clae.2019.10.141
54. Pucker AD, McGwin G, Franklin QX, Dubey J, Nattis A, Lievens C. Application of Systane Complete for the treatment of contact lens discomfort. Contact Lens Anterior Eye. 2021;44(4):101399. doi:10.1016/j.clae.2020.12.004
55. Tan J, Peguda R, Siddireddy JS, Briggs N, Stapleton F. Subjective responses to various filling solutions in the posterior fluid reservoir of miniscleral lenses at application. Eye Contact Lens Sci Clin Pract. 2022;48(2):73–77. doi:10.1097/icl.0000000000000855
56. Garrigue JS, Amrane M, Faure MO, Holopainen JM, Tong L. Relevance of lipid-based products in the management of dry eye disease. J Ocul Pharmacol Ther. 2017;33(9):647–661. doi:10.1089/jop.2017.0052
57. Vicario-de-la-Torre M, Caballo-González M, Vico E, et al. Novel Nano-liposome formulation for dry eyes with components similar to the preocular tear film. Polymers. 2018;10(4):1–13. doi:10.3390/polym10040425
58. Acar D, Molina-Martínez IT, Gómez-Ballesteros M, Guzmán-Navarro M, Benítez-del-Castillo JM, Herrero-Vanrell R. Novel liposome-based and in situ gelling artificial tear formulation for dry eye disease treatment. Contact Lens Anterior Eye. 2018;41(1):93–96. doi:10.1016/j.clae.2017.11.004
59. Vigo L, Senni C, Pellegrini M, et al. Effects of a new formulation of multiple-action tear substitute on objective ocular surface parameters and ocular discomfort symptoms in patients with dry eye disease. Ophthalmol Ther. 2022;11(4):1441–1447. doi:10.1007/s40123-022-00518-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.