Back to Journals » Drug Design, Development and Therapy » Volume 18
Programmed Intermittent Epidural Bolus vs Manual Epidural Bolus for Labor Analgesia Initiation: A Randomized Non-Inferiority Trial
Authors Lu Y, Zhang Y, Zheng Y, Song Y ![]() , Zang Y, Liu Z, Xu Z
, Zang Y, Liu Z, Xu Z
Received 27 July 2024
Accepted for publication 5 November 2024
Published 7 November 2024 Volume 2024:18 Pages 5063—5072
DOI https://doi.org/10.2147/DDDT.S488920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Yan Lu,1,* Yueqi Zhang,1,* Yuhan Zheng,1,* Yujie Song,1 Yu Zang,2 Zhiqiang Liu,3 Zhendong Xu1
1Department of Anesthesiology, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China; 2Department of Anesthesiology, Yangpu Hospital, School of Medicine, Tongji University, Shanghai, 200090, People’s Republic of China; 3Department of Anesthesiology, Obstetrics and Gynecology Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhendong Xu, Department of Anesthesiology, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China, Email [email protected]
Purpose: Typically, labor analgesia is initiated with a manual loading dose. The programmed intermittent epidural bolus (PIEB) effectively maintains labor analgesia. However, no PIEB method has been studied for the initial loading dose. This study aimed to compare the effectiveness of loading doses administered via a PIEB versus a manual bolus.
Patients and Methods: In total, 164 full-term singleton parturients were randomly assigned to receive a 12 mL loading dose (0.1% ropivacaine and 0.3 μg·mL− 1 sufentanil) via manual or pump-driven injection. A standardized maintenance protocol was employed. The primary outcome was the percentage of parturients with adequate analgesia 20 min after the initial epidural injection. Adequate analgesia was defined as a numeric rating score (NRS) of ≤ 3 during two consecutive uterine contractions, without an additional analgesia request. Kaplan–Meier survival curves were constructed for the time interval needed to achieve adequate analgesia. A non-inferiority analysis was conducted by comparing the 90% confidence interval of the pain score difference with the non-inferiority margin.
Results: The percentage of parturients achieving adequate analgesia was comparable (75.61% manual injection vs 76.83% pump injection, P=0.05 for non-inferiority). The median NRS was similar, except at 2 min (7 [5– 8] manual injection vs 8 [6– 9] pump injection, P=0.04). Median time to adequate analgesia, median ropivacaine consumption, median duration of epidural analgesia, incidence of requests for patient-controlled epidural analgesia (PCEA), median number of PCEA boluses, percentage of bilateral S2 blocks at 20 min, incidence of breakthrough pain, percentage of highest block level ≥T6 at 20 min, adverse effects, and obstetric and neonatal outcomes were similar between the groups.
Conclusion: Within 20 min of administering a loading dose through a PIEB pump, non-inferior analgesia comparable to that achieved with manual injection was observed. This hands-free approach could help mitigate the impact of individual operational differences on analgesic efficacy.
Registration: This trial was registered at chictr.org.cn (ChiCTR2300074063).
Keywords: epidural, labor analgesia, loading dose, programmed intermittent epidural bolus
Introduction
Epidural analgesia is widely recognized as the gold standard for labor pain relief.1 In epidural labor analgesia, a loading dose of the drug is often administered to alleviate pain rapidly and effectively when an epidural catheter is first placed.2 The loading dose is a relatively large initial amount of the local anesthetic agent administered to quickly achieve the desired analgesia.3 It helps establish a baseline level of pain relief before transitioning to continuous infusion or other delivery methods.4 The loading dose, a crucial component of the analgesic regimen, is typically administered manually.5 However, manual bolus delivery is operator-dependent and influenced by many factors, such as fatigue, administrator strength, and personal habits of the administrator. Administrators’ fatigue may reduce accuracy and reliability. Manual bolus dosing is less precise than that delivered by automated or controlled systems, increasing the risk of errors such as under- or over-dosing. This may pose a threat to patient safety and treatment outcomes.6,7 In addition, personalized habits or physical strength can lead to inconsistent injection pressure, which can result in potentially ineffective treatment or adverse reactions.8 Although manual drug delivery is still widely used, its limitations highlight the urgent need for more standardized and reliable drug delivery methods in healthcare settings.
The programmed intermittent epidural bolus (PIEB) was introduced for the maintenance of labor analgesia in 2006.9 Compared with continuous epidural infusion, PIEB not only offers better diffusion of the local anesthetic solution in the epidural space, leading to lower anesthetic consumption, reduced motor blockade, improved quality of analgesia, and fewer interventions by the anesthetist, but it also shows no significant differences in obstetric and newborn outcomes.10–13 As a result, it has already become the routine method for maintaining labor analgesia in our hospital. We previously found that a PIEB not only achieved a satisfactory analgesic effect but also mitigated the impact of individual variations in operational techniques.14 Given the ability of a PIEB to generate elevated pressure during automated boluses, we explored its use in the initiation of epidural labor analgesia. We hypothesized that the analgesic effect of the loading dose delivered by the PIEB pump would be non-inferior to that achieved manually. To test our hypothesis, we conducted a randomized, single-blind, non-inferiority trial.
Materials and Methods
Study Population
The Ethics Committee of Shanghai First Maternity and Infant Hospital (No: KS22303, approval date: November 2, 2022) approved this study and written informed consent was obtained from all subjects participating in the trial. Prior to patient enrollment, this trial was registered at chictr.org.cn (ChiCTR2300074063, principal investigator: Yan Lu, date of registration: July 28, 2023) and conducted in accordance with the Declaration of Helsinki. This study followed the guidelines outlined in the Consolidated Standards of Reporting Trials (CONSORT) statement. We included women meeting the following inclusion criteria: American Society of Anesthesiologists physical status II, aged between 20 and 40 years, singleton parturient, at 37–42 weeks of gestation, with cervical dilation <5 cm, and a numeric rating score (NRS) >5 (0=no pain; 10=worst imaginable pain) at the time of request for epidural labor analgesia. The exclusion criteria included contraindications to neuraxial labor analgesia, gestational diabetes, gestational hypertension, pre-eclampsia, known major fetal abnormalities, body mass index >35 kg·m−2, or the use of opioids or sedatives within 4 h preceding epidural analgesia.
Randomization and Concealment of Group Assignments
The patients were randomly assigned using a 1:1 allocation ratio. This allocation was performed without stratifying the factors. Allocation concealment was rigorously maintained using opaque, sealed envelopes prepared by staff members not directly involved in the study. Based on the assigned groups, the anesthetist responsible for catheter placement was not blinded to the intervention. However, to maintain the integrity of the study, all other personnel, including the nurse conducting cervical examinations and pain assessments upon request for labor analgesia, the nurse anesthetist overseeing follow-ups and analgesic management as the outcome assessor, and the study participants themselves, remained unaware of the group allocation.
Epidural Catheter Placement
Participants received an 18-G intravenous catheter, and lactated Ringer’s solution was administered before initiating analgesia. Standard monitoring, including electrocardiography and non-invasive blood pressure, pulse oxygen saturation, and fetal heart rate measurements, was applied.
Neuraxial analgesia commenced with the parturient positioned in the right lateral decubitus position, using a 17-G Tuohy needle (Foshan Special Medical, Foshan, China) at the L2–L3 interspace. We used spinal ultrasound to precisely identify the interspace of the puncture. We also employed a loss-of-resistance technique to locate the epidural space, after which an epidural catheter (multi-orifice, 19-G, stainless steel impregnated; Foshan Special Medical) was inserted 4 cm into the epidural space. Subsequently, we administered a test dose of 1.5% lidocaine with 15 μg epinephrine (3 mL). The parturient was then repositioned in the supine position with left uterine displacement. We excluded parturients with a positive response to the test dose from further analysis.
Initiation and Maintenance of Labor Analgesia
Three minutes after being administered the test dose, the manual group received a 12 mL loading dose of 0.1% ropivacaine with 0.3 μg·mL−1 sufentanil, administered in 6-mL aliquots every min over 2 min. The pump group was administered an initial dose of 12 mL of the same solution using a PIEB pump over a duration of 2 min, with the infusion rate set at 360 mL·h−1 (Apon ZZB-IV; Jiangsu Apon Medical Technology, Jiangsu, China). The pump was programmed to administer 10 mL of PIEBs every 45 min, starting 1 h after the loading dose. We defined analgesia initiation as the time of the loading dose administration. In addition to receiving the programmed bolus, all participants were equipped with patient-controlled epidural analgesia (PCEA) set to 8 mL boluses with a 10-min lockout interval between the PCEA or PIEB/PCEA boluses. The participants were instructed not to use the PCEA until 30 min after the loading dose.
After administering the loading dose, all data were collected by another anesthetist blinded to the assigned groups. NRSs, sensory blockade levels to cold, and motor strength were recorded at 2-min intervals during the initial 20 min and subsequently at 30 min. Motor strength was evaluated using the modified Bromage score, with scores of 0, 1, 2, and 3 indicating no impairment, inability in raising the extended leg but able to move the knees and feet, inability to raise the extended leg and flex the knees but able to move the feet, and inability to flex the ankle, feet, or knees (complete block), respectively.15 We defined motor blockade as a modified Bromage scale score of ≥1. Sensory blockade levels to cold were assessed bilaterally at the mid-clavicular line from the caudal to cephalad direction, with the upper sensory blockade level determined by the point at which the parturients first perceived the cold sensation. For the lower extremities, we evaluated dermatomal levels by stimulating specific locations, including the inguinal crease at the mid-clavicular line (L1), anteromedial thigh (L2), medial femoral condyle above the knee (L3), medial malleolus (L4), dorsum web between the great and second toes (L5), lateral calcaneus (S1), and midpoint of the popliteal fossa (S2). Dermatomal levels on the torso were assessed at the mid-clavicular line, considering both the left and right sides.
In accordance with the standard of care at our institution, we conducted non-invasive blood pressure measurements every 2 min during the initial 20 min and subsequently at 30-min intervals. Continuous monitoring included maternal heart rate, pulse oximetry, and fetal heart rate assessments. Instances of maternal hypotension and fetal bradycardia were recorded and appropriately addressed. We defined maternal hypotension as systolic blood pressure <90 mm Hg or <80% of the baseline. Fetal bradycardia was characterized by a heart rate <110 bpm sustained for >10 min. If delivery occurred within 1 h of epidural catheterization, the parturient was excluded from the analysis. Observations were conducted for a duration of 6 h from the initiation of epidural analgesia or until full dilation of the maternal cervix occurred. Information pertaining to analgesic use was systematically collected from the pumps.
Inadequate Analgesia Management
In our study, inadequate analgesia was operationally defined as an NRS >3, or if the participant requested additional medication. In cases of perceived inadequate analgesia 30 min after the loading dose was administered, the participant was encouraged to self-administer a PCEA bolus. If the participant experienced pain or if unilateral blockade persisted following two PCEA boluses within the 20-min timeframe, a provider bolus of 5 mL of 0.2% ropivacaine was manually administered. An additional 5 mL was administered after a 10-min interval if deemed necessary. In the absence of an observable improvement in analgesia, the epidural catheter was replaced, leading to the exclusion of the parturient from the analysis.
Outcome Assessment
The primary outcome was the percentage of participants in the two groups who received adequate analgesia 20 min after the initial epidural bolus administration. Adequate analgesia was defined as an NRS ≤3 during two consecutive uterine contractions and no request for additional analgesia. Figure 1 details the timing of data collection.
 |
Figure 1 Schematic of epidural dosing and NRS data collection. NRS, numeric rating score. |
Secondary outcomes included the time to adequate analgesia, ropivacaine consumption, request for PCEA, bilateral sacral blockade (S2) within 20 min, incidence of breakthrough pain, highest block level ≥T6, and adverse effects.
Sample Size Calculation
The sample size estimation was based on the primary outcome. Data from a pilot study that included 28 patients in each group suggested that the percentages of parturients who achieved adequate analgesia within 20 min were 78.6% and 71.4% with the manual and pump methods, respectively. We calculated a sample size of 78 per group, given an alpha error of 5% (one-sided) and a power of 80%, with a non-inferiority limit of −10%. Following expert consultation and literature review, the non-inferiority margin for pump-initiated analgesia was set at 10% below the proportion of parturients in the manual loading dose group who achieved adequate analgesia within 20 minutes.16 Considering a possible dropout rate of 20%, we decided to enroll 82 parturients per group.
Statistical Analysis
The R language (R V.4.1.2; R Foundation for Statistical Computing, Vienna, Austria) was used to implement the statistical analysis. The normality of continuous data was assessed using the Shapiro–Wilk test. Normally distributed data are presented as mean (standard deviation) and were analyzed among the groups using the t-test. For skewed data, summary statistics are presented as the median (interquartile range, IQR) and were compared using the Mann–Whitney U-test. Categorical variables are reported as frequencies (percentages) and were compared using the χ2 test. Kaplan–Meier survival curves were constructed for the time interval needed to achieve adequate analgesia. Both Hedges’ g and Cliff’s delta are standardized measures of effect size, with the latter being used for ordinal and non-parametric data. A non-inferiority analysis was conducted by comparing the 90% confidence interval (CI) of the pain score difference with the non-inferiority margin. P values of <0.05 were considered significant.
Results
As shown in Figure 2, 184 patients were approached between July 2023 and October 2023. A total of 164 patients were randomized in a 1:1 ratio to receive either manual or pump injections. Sixteen patients did not meet the inclusion criteria, and four declined to participate. Therefore, we collected data for analysis from 164 patients. No clinically relevant differences in demographic or baseline characteristics were observed between the two groups (Table 1).
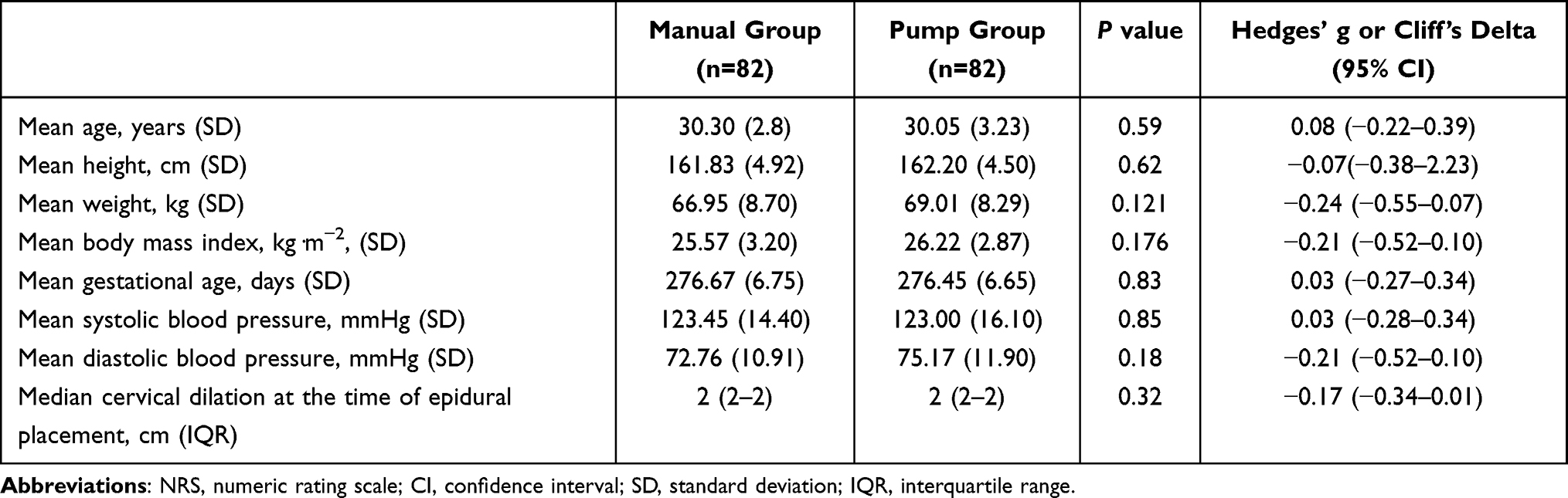 |
Table 1 Maternal Demographic and Baseline Characteristics |
 |
Figure 2 Flow chart showing study participant recruitment. |
Primary Outcome
The percentages of parturients with adequate analgesia 20 min after the loading dose was administered were 75.61% and 76.83% in the manual and pump groups, respectively (Table 2). The lower limit of the one-sided 90% CI for the difference was −9%, which was higher than the predefined margin of non-inferiority of −10% (P=0.05), demonstrating the non-inferiority of the pump to manual injection in terms of adequate analgesia.
 |
Table 2 Outcomes |
Secondary Outcomes
The NRSs were comparable between the groups, except for those at 2 min, as shown in Figure 3 (7 (IQR: 5–8) in the manual group vs 8 (IQR: 6–9) in the pump group). Figure 4 shows the Kaplan–Meier curves for the time required to achieve adequate analgesia after the loading dose was administered. The median time to adequate analgesia was similar between the groups (Table 2).
 |
Figure 3 NRS over the first 30 min following the initiation of neuraxial labor analgesia. NRS, numeric rating score. Data are median (interquartile range). The NRS did not differ between the groups, except at 2 min (P=0.04). N is the number of patients in labor at each time measurement. Manual group (▪); pump group (•); *P=0.04. |
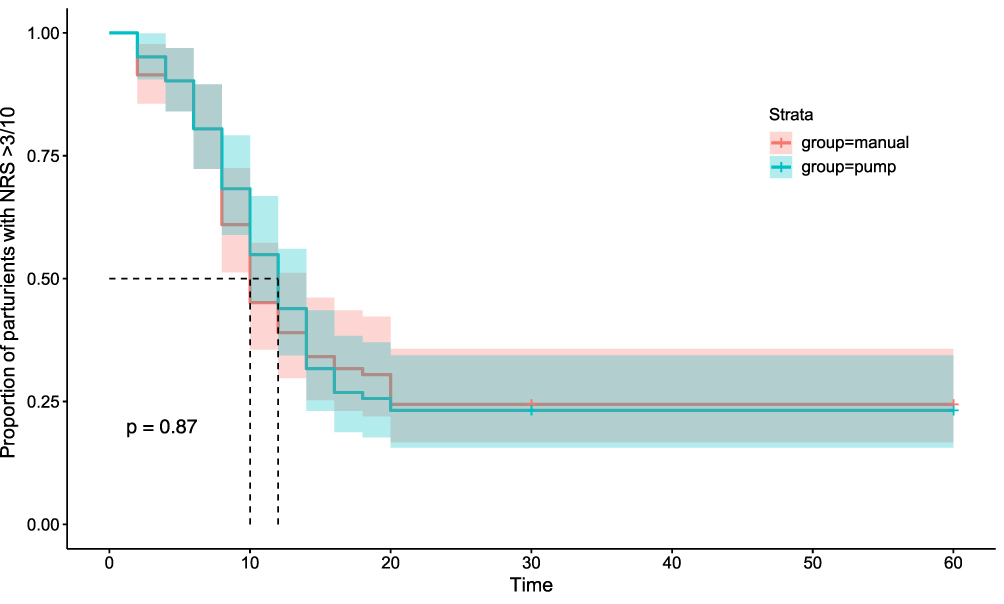 |
Figure 4 Kaplan–Meier curves for time to achieving adequate analgesia. |
Other secondary outcomes, including median ropivacaine consumption, median duration of epidural analgesia, incidence of requests for PCEA, median number of PCEA boluses, percentage of bilateral S2 blocks at 20 min, incidence of breakthrough pain, percentage of highest block level ≥T6 at 20 min, and adverse effects including hypotension, nausea/vomiting, pruritus, shivering, and fetal bradycardia, were similar between the groups (Table 2). Additionally, obstetric and neonatal outcomes were not significantly different between the two groups (Table 2).
Discussion
Our study demonstrated that administering a loading dose through a PIEB pump provided non-inferior analgesia comparable to that achieved with manual injection within 20 min of initiating epidural analgesia. While manual injection initially produced a superior analgesic effect at the 2-min point, this advantage did not persist over time, with no discernible difference in analgesia thereafter. Additionally, the injection loading dose with a PIEB pump provides a hands-free approach, mitigating the impact of human variability on analgesic efficacy due to individual operational differences.
Administering a loading dose has emerged as a pivotal strategy for promptly achieving effective pain relief, particularly in the initial stages of labor. This underscores the need for a relatively substantial dose of analgesics to achieve swift and pronounced pain alleviation.17,18 Prior to the introduction of the PIEB pump, sustained analgesia relied primarily on a continuous epidural infusion (CEI) pump.19 However, the CEI pump was limited in its capacity to administer large doses of medication at once. In previous studies, a PIEB was used only for the maintenance of analgesia.20,21 In some centers, a PIEB pump is used to administer the loading dose, which also produces good analgesia.14,22 However, no study has yet evaluated the differences between pump-administered loading doses and manually controlled administration. Therefore, we conducted this study. Furthermore, we found that the analgesic effect produced using the PIEB pump was not inferior to that achieved with manual administration, emphasizing the reliability and effectiveness of this delivery method.
We observed that manual injection initially provided superior analgesia at 2 min, but this advantage diminished over time; subsequently, no significant difference was found in analgesic effectiveness. This observation may be attributed to the elevated pressure applied during manual injection as opposed to that during pump-driven administration. A previous study demonstrated that higher push pressures lead to more efficient local anesthetic distribution and enhanced pain relief, potentially contributing to the initial superiority of manual injections in our study.23 This study also highlights that manual bolus administration is operator-dependent and influenced by various factors, in contrast to machine bolus administration.8 Owing to the current high workload in the delivery room, long working hours of anesthesiologists, fatigue, and other factors, discrepancies are more likely to occur.24 The advantage of machine administration is the reduction of an anesthesiologist’s workload and work intensity while still providing a more uniform administration rate and analgesic effect.25
Previous studies have administered loading doses through manual injection using varying dosages; however, manual injection was conducted intermittently rather than as a single, continuous administration.26–29 In our study, manual injection remained consistent with that in previous studies, in 6-mL aliquots administered every min over 2 min.15 However, in contrast, the pump injection method in our investigation involved delivering the entire 12-mL dosage simultaneously. Administering a substantial dose simultaneously may result in a heightened level of anesthesia, potentially leading to increased maternal side effects and adverse fetal outcomes. However, our study indicated that the method used in the pump group neither induced a high level of anesthesia nor did it increase maternal side effects or contribute to unfavorable fetal outcomes when compared with the method used in the manual group. Additionally, no significant difference was observed between the two groups in terms of ropivacaine consumption, number of PCEA boluses, or incidence of breakthrough pain. A previous study similarly reported that within the range of 5–20 mL, varying the administration volume of ropivacaine did not result in an increased incidence of adverse effects, which was consistent with the findings of our study.30
Our study had some limitations. First, initially designed as a single-blind study, the audibility of the pump administering the medication rendered the process noticeable. Second, we exclusively focused on nulliparous parturients in the early stages of labor with a cervical dilation of <5 cm when seeking epidural labor analgesia. Consequently, the outcomes may not be generalizable to other scenarios, including multiparous women or those with a larger cervical dilation. Third, the dose at which the pump administered the loading dose was chosen because no previous study had been conducted on such a dose, and it was consistent with the dose administered manually. It may be possible to follow up with a comparison of the effects of different loading doses. Finally, the pump’s delivery speed was 360 mL/h, but not all commercially available pumps can achieve this high rate, that could limit the generalizability of our results in different clinical settings.
Conclusion
In conclusion, our findings suggest that the administration of a loading dose through a PIEB pump provides analgesia that is non-inferior and comparable to that achieved with manual injection within the first 20 min of initiating epidural analgesia. Moreover, this approach comprises a hands-free method that could reduce the influence of individual operational variations on analgesic efficacy. Additional research is required to determine the optimal dose for initiating PIEB therapy.
Abbreviations
CEI, continuous epidural infusion; CI, confidence interval; IQR, interquartile range; NRS, numeric rating score; PCEA, patient-controlled epidural analgesia; PIEB, programmed intermittent epidural bolus.
Data Sharing Statement
The raw data are available upon reasonable requests to the corresponding authors.
Ethics Approval and Informed Consent
The Ethics Committee of Shanghai First Maternity and Infant Hospital (No: KS22303, approval date: November 2, 2022) approved this study, and written informed consent was obtained from all subjects participating in the trial.
Acknowledgments
The authors acknowledge the statistician, Kechen Fan, for assisting with statistical analysis in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the grants of Science and Technology Commission of Shanghai Municipality (22Y11905900).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hawkins JL. Epidural analgesia for labor and delivery. N Engl J Med. 2010;362(16):1503–1510. doi:10.1056/NEJMct0909254
2. Scrutton MJ, Porter JS, O’Sullivan G. Comparison of three different loading doses to establish epidural analgesia in labour. Int J Obstet Anesth. 1998;7(3):165–169. doi:10.1016/S0959-289X(98)80005-8
3. Casellato JF, Balki M, Wang A, Ye XY, Downey K, Carvalho JCA. Differential sensory block during labour epidural analgesia: a prospective observational study to investigate the relationship of lower and upper sensory block levels to cold, pinprick, and light touch. Can J Anaesth. 2024;71(6):802–807. doi:10.1007/s12630-023-02638-5
4. Janes EF, McCrory JW. The loading dose in continuous infusion extradural analgesia in obstetrics. Br J Anaesth. 1991;67(3):323–325. doi:10.1093/bja/67.3.323
5. Bittencourt R, Arzola C, Zakus P, Downey K, Ye XY, Carvalho JCA. A biased coin up-and-down sequential allocation trial to determine the optimum programmed intermittent epidural bolus time interval between 5 mL boluses of bupivacaine 0.125% with fentanyl 2 µg·mL-1. Can J Anaesth. 2019;66(9):1075–1081. doi:10.1007/s12630-019-01407-7
6. Redfern N, Bilotta F, Abramovich I, Grigoras I. Fatigue in anaesthesiology: call for a change of culture and regulations. Eur J Anaesthesiol. 2023;40(2):78–81.
7. Scholliers A, Cornelis S, Tosi M, et al. Impact of fatigue on anaesthesia providers: a scoping review. Br J Anaesth. 2023;130(5):622–635. doi:10.1016/j.bja.2022.12.011
8. Younger JD, Faryami A, Prasad M, et al. Direct comparison of peak bulk flow rate of programmable intermittent epidural bolus and manual epidural bolus using a closed-end multiorifice catheter: an experimental study. Anesth Analg. 2023;136(6):1198–1205. doi:10.1213/ANE.0000000000006268
9. Roofthooft E, Barbé A, Schildermans J, et al. Programmed intermittent epidural bolus vs. patient-controlled epidural analgesia for maintenance of labour analgesia: a two-centre, double-blind, randomised study†. Anaesthesia. 2020;75(12):1635–1642. doi:10.1111/anae.15149
10. Carvalho B, George RB, Cobb B, McKenzie C, Riley ET. Implementation of programmed intermittent epidural bolus for the maintenance of labor analgesia. Anesth Analg. 2016;123(4):965–971. doi:10.1213/ANE.0000000000001407
11. Munro A, MacCormick H, Aidemouni M, Nash CM, George RB. A retrospective cohort comparison of programmed intermittent epidural bolus (PIEB) and continued epidural infusion (CEI) on delivery mode. Can J Anaesth. 2022;69(7):909–911. doi:10.1007/s12630-022-02268-3
12. Howle R, Ragbourne S, Zolger D, Owolabi A, Onwochei D, Desai N. Influence of different volumes and frequency of programmed intermittent epidural bolus in labor on maternal and neonatal outcomes: a systematic review and network meta-analysis. J Clin Anesth. 2024;93:111364. doi:10.1016/j.jclinane.2023.111364
13. Xu J, Zhou J, Xiao H, et al. A systematic review and meta-analysis comparing programmed intermittent bolus and continuous infusion as the background infusion for parturient-controlled epidural analgesia. Sci Rep. 2019;9(1):2583. doi:10.1038/s41598-019-39248-5
14. Yi J, Li Y, Yuan Y, et al. Comparison of labor analgesia efficacy between single-orifice and multiorifice wire-reinforced catheters during programmed intermittent epidural boluses: a randomized controlled clinical trial. Reg Anesth Pain Med. 2023;48(2):61–66. doi:10.1136/rapm-2022-103723
15. Wilson SH, Wolf BJ, Bingham K, et al. Labor analgesia onset with dural puncture epidural versus traditional epidural using a 26-gauge Whitacre needle and 0.125% bupivacaine bolus: a randomized clinical trial. Anesth Analg. 2018;126(2):545–551.
16. Vedagiri Sai R, Singh SI, Qasem F, et al. Onset of labour epidural analgesia with low-dose bupivacaine and different doses of fentanyl. Anaesthesia. 2017;72(11):1371–1378. doi:10.1111/anae.14000
17. Capogna G, Camorcia M, Stirparo S, Farcomeni A. Programmed intermittent epidural bolus versus continuous epidural infusion for labor analgesia: the effects on maternal motor function and labor outcome. A randomized double-blind study in nulliparous women. Anesth Analg. 2011;113(4):826–831. doi:10.1213/ANE.0b013e31822827b8
18. George RB, Allen TK, Habib AS. Intermittent epidural bolus compared with continuous epidural infusions for labor analgesia: a systematic review and meta-analysis. Anesth Analg. 2013;116(1):133–144. doi:10.1213/ANE.0b013e3182713b26
19. Ni F, Wu Z, Zhao P. Programmed intermittent epidural bolus in maintenance of epidural labor analgesia: a literature review. J Anesth. 2023;37(6):945–960.
20. Bullingham A, Liang S, Edmonds E, Mathur S, Sharma S. Continuous epidural infusion vs programmed intermittent epidural bolus for labour analgesia: a prospective, controlled, before-and-after cohort study of labour outcomes. Br J Anaesth. 2018;121(2):432–437. doi:10.1016/j.bja.2018.03.038
21. Sun C, Ren S, Chen C, et al. Pulse perfusion index for predicting intrapartum fever during epidural analgesia. J Clin Anesth. 2022;80:110852. doi:10.1016/j.jclinane.2022.110852
22. Lange EMS, Wong CA, Fitzgerald PC, et al. Effect of epidural infusion bolus delivery rate on the duration of labor analgesia: a randomized clinical trial. Anesthesiology. 2018;128(4):745–753. doi:10.1097/ALN.0000000000002089
23. Abramovich I, Matias B, Norte G, et al. Fatigue amongst anaesthesiology and intensive care trainees in Europe: a matter of concern. Eur J Anaesthesiol. 2023;40(8):587–595. doi:10.1097/EJA.0000000000001849
24. Ippolito M, Noto A, Lakbar I, et al. Peri-operative night-time work of anaesthesiologists: a qualitative study of critical issues and proposals. Eur J Anaesthesiol. 2024;41(1):34–42.
25. Wei Y, Wang Y, Zhao Y, Wu C, Liu H, Yang Z. High dosage of patient-controlled epidural analgesia (PCEA) with low background infusion during labor: a randomized controlled trial. J Pers Med. 2023;13(4):600. doi:10.3390/jpm13040600
26. Mazda Y, Arzola C, Downey K, Ye XY, Carvalho JCA. Programmed intermittent epidural bolus for labour analgesia: a randomized controlled trial comparing bolus delivery speeds of 125 mL·hr-1 versus 250 mL·hr-1. Can J Anaesth. 2022;69(1):86–96. doi:10.1007/s12630-021-02132-w
27. Casellato JF, Ye XY, Downey K, Carvalho JCA. Changes in sensory block level during a programmed intermittent epidural bolus regimen for labour analgesia: a prospective observational cohort study. Can J Anaesth. 2022;69(12):1471–1476. doi:10.1007/s12630-022-02318-w
28. Epsztein Kanczuk M, Barrett NM, Arzola C, Downey K, Ye XY, Carvalho JC. Programmed intermittent epidural bolus for labor analgesia during first stage of labor: a biased-coin up-and-down sequential allocation trial to determine the optimum interval time between boluses of a fixed volume of 10 mL of bupivacaine 0.0625% with fentanyl 2 μg/mL. Anesth Analg. 2017;124(2):537–541. doi:10.1213/ANE.0000000000001655
29. Song Y, Du W, Tao Y, et al. Optimum programmed intermittent epidural bolus interval time between 8 mL boluses of ropivacaine 0.1% with sufentanil 0.3 μg/mL with dural puncture epidural technique for labor analgesia: a biased-coin up-and-down sequential allocation trial. J Clin Anesth. 2022;79:110698.
30. Chan L, Lee BB, Ngan Kee WD. A randomised double-blinded controlled trial of the effect of diluent volume on the efficacy of a single dose of epidural ropivacaine for labour analgesia. Int J Obstet Anesth. 2006;15(3):201–205. doi:10.1016/j.ijoa.2005.11.001
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.