Back to Journals » OncoTargets and Therapy » Volume 13
Prognostic Values of LDH and CRP in Cervical Cancer
Authors Wang H, Wang MS, Zhou YH, Shi JP, Wang WJ ![]()
Received 17 October 2019
Accepted for publication 20 January 2020
Published 11 February 2020 Volume 2020:13 Pages 1255—1263
DOI https://doi.org/10.2147/OTT.S235027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjay Singh
Han Wang,1,* Meng-Sen Wang,2,* Yong-Heng Zhou,1,* Jian-Ping Shi,3 Wen-Jie Wang3
1Department of Oncology, Jining Cancer Hospital, Jining, Shandong, People’s Republic of China; 2Department of Oncology, Jining No. 1 People’s Hospital, Jining, Shandong, People’s Republic of China; 3Department of Radio-Oncology, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen-Jie Wang
Department of Radio-Oncology, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, Jiangsu 215001, People’s Republic of China
Tel +86-512-62364922
Fax +86-512-62362502
Email [email protected]
Purpose: Cervical cancer is one of the deadliest tumors among women in China. C-reactive protein (CRP), an indicator of inflammation, and lactate dehydrogenase (LDH), an enzyme ubiquitously expressed in cells, both play important roles in tumor growth and metastasis.
Patients and Methods: Based on pre-radiotherapy LDH and CRP median levels, we divided patients into four groups: high LDH and CRP group, high LDH group, high CRP group, and low LDH and CRP group. Then, based on pre-/post-radiotherapy LDH and CRP ratios, we divided patients into four groups: high LDH and CRP ratio group, high LDH ratio group, high CRP ratio group, and low LDH and CRP ratio group. Kaplan–Meier (KM) curves were constructed to show overall survival (OS). A multivariate Cox regression model was employed to identify the independent risk factors.
Results: High pre-radiotherapy LDH and CRP levels and increased pre-/post-radiotherapy LDH and CRP ratios were correlated with worst OS compared with the other three groups.
Conclusion: LDH and CRP were correlated with outcomes in patients with locally advanced cervical cancer.
Keywords: cervical cancer, LDH, CRP, prognosis, OS
Introduction
With 98,900 new cases and 30,500 deaths each year, cervical cancer is one of the most common and lethal tumors affecting women in China.1 Numerous high-risk factors, such as HPV infection, malnutrition, smoking, and multiple sexual partners, are tightly correlated with the initiation and progression of cervical cancer.2,3 Pathologically, cervical cancer can be divided into squamous cell carcinoma, adenocarcinoma, and small cell carcinoma, with squamous cell carcinoma accounting for 80% of the total. Surgery is widely accepted as the first-line therapy for early-stage cervical cancer, while patients with local advanced cervical cancer are usually given concurrent chemoradiotherapy (CCRT).4,5
C-reactive protein (CRP) was discovered in 1930 and well-characterized as an indicator of systemic inflammation.6,7 Inflammation plays an important role in the development of cervical cancer, and can also affect cervical tissue remodeling, as well as the release of cytokines and chemokines, among other processes.8 CRP is associated with the prognosis of a variety of cancers, including cervical squamous cell carcinoma.9–13 LDH is a ubiquitous cellular enzyme, and comprises the rate-limiting step in the conversion of pyruvate to lactic acid under anaerobic conditions.14 The level of serum LDH is associated with the prognosis of several cancers, including nasopharyngeal, colon, and lung cancers.15,16 We previously found that in early operable cervical cancer, high levels of CRP and LDH were correlated with poor prognosis.13
In our present study, elevated serum CRP and LDH levels were correlated with worse prognosis in locally advanced cervical cancer patients. Our aim is to predict patient outcomes through a combined evaluation of CRP with LDH levels.
Materials and Methods
Subjects
This retrospective study included a total of 150 patients with locally advanced squamous cell cervical cancer who were admitted to the Jining Cancer Hospital from 2013 to 2015 and the Affiliated Suzhou Hospital of Nanjing Medical University in 2015. All patients were staged according to the International Federation of Gynecology and Obstetrics (FIGO) criteria,17 and the main predictor of the study was overall survival (OS). The median age of patients was 59 years (range 24 to 75). The study was approved by the Ethics Committee of Jining Cancer Hospital and the Affiliated Suzhou Hospital of Nanjing Medical University, and all patients signed informed consent. Our study was conducted in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: a) Patients presenting with cervical cancer according to FIGO stage 1B2, IIA2, IIB, IIIA, and IIIB; b) eastern cooperative oncology group (ECOG) score of 0–1; c) squamous cell carcinoma confirmed by histopathology; d) 18–75 years of age.
The exclusion criteria were as follows: a) Non-squamous cell carcinoma of cervical histopathology; b) patient failed to complete CCRT; c) patients with abnormally elevated CRP levels combined with fever or neutrophil abnormalities.
Concurrent Chemoradiotherapy
Radiotherapy: All patients were administered external beam radiation therapy (EBRT), three-dimensional conformal radiation therapy (3D–CRT), or intensity-modulated radiation therapy (IMRT). A total dose of 45.0–50.4Gy in 25–28 fractions was prescribed. In intracavitary brachytherapy (ICBT), accumulative dose of 30–36Gy in 5–7 fractions was prescribed to point A.
Concurrent chemotherapy: The first-line regimen of concurrent chemotherapy was cisplatin(30–40mg/m2/week). Paclitaxel (60–80mg/m2/week) was prescribed for patients with renal insufficiency or those who could not tolerate cisplatin.
Evaluation of Patients
Magnetic Resonance Imaging (MRI) was performed every 3–6 months to assess the response and patients were assessed according to response evaluation criteria in solid tumors (RECIST) 1.1.18
Blood Samples
Peripheral venous blood was collected into a sterile EDTA tube; patients fasted for 8 hours and elbow venous blood was obtained between 07:00 and 07:30 to standardize the known impact of circulating hormones (circadian rhythm) on the CRP and LDH levels. Blood samples were examined using a hematology analyzer (Sysmex XE-2100; Sysmex, Kobe, Japan).
Follow-Up
Survival time was measured from the date of diagnosis until death or last clinical evaluation. The prognostic analyses were performed for OS. Patients were followed up for 8–77 months (median 39 months). The first follow-up was one month after radiotherapy, and continued until the patient died or end of the study in August 2019.
Statistical Analysis
All statistical analyses were performed using SPSS software version 19.0 (SPSS, IBM; Chicago, IL, USA) and GraphPad Prism version 8.0 (GraphPad Software, La Jolla, CA, USA). For analysis of survival data, Kaplan–Meier curves were constructed, and statistical analysis was carried out using the Log-rank test. The association between LDH and CRP was analyzed by Spearman’s rank correlation. Univariate and multivariate Cox regression analysis was employed to identify the independent risk factors associated with cervical cancer. The chi-square test was used to compare the categorical variables. All P-values<0.05 were considered significant.
Results
Clinical Features
Our study included 150 patients. The median age of the patients was 56 years and the median survival time was 38 months. Of the 150 patients enrolled, 70 presented with lymph node metastasis. At the time of diagnosis, 29 patients were stage IB2, 50 were stage IIA2–IIB, and 71 were stage III. All patients underwent first-line CCRT. The clinicopathological features are detailed in Table 1.
 |
Table 1 Clinicopathological Features |
The Relationship Between LDH and CRP Levels and Cervical Cancer Patient Survival Before Radiotherapy
The patients were divided into two groups according to the median levels of LDH or CRP. The high-LDH-level group had worse OS than the low-level group (P =0.013, Hazard Ratio [HR] 1.789; 95% CI = 1.118–2.864) (Figure 1A). The high-CRP-level group had worse OS than the low-level group (P =0.003, HR 2.028; 95% CI =1.265–3.251) (Figure 1B).
 |
Figure 1 The relationships between pre-radiotherapy levels of lactate dehydrogenase (LDH) and C-reactive protein (CRP) with prognosis. (A) LDH levels with OS. (B) CRP levels with OS. |
The Relationship Between the Pre-/Post-Radiotherapy Ratio of LDH or CRP with Cervical Cancer Patient Survival
The patients were divided into two groups according to pre-radiotherapy and post-radiotherapy LDH or CRP ratios. The group with a higher LDH ratio had worse OS than the group with a lower ratio(P <0.001, HR 2.838; 95% CI = 1.749–4.606) (Figure 2A). The group with a higher CRP ratio had worse OS than the group with a lower ratio (P <0.001, HR 2.510; 95% CI =1.557–4.046) (Figure 2B).
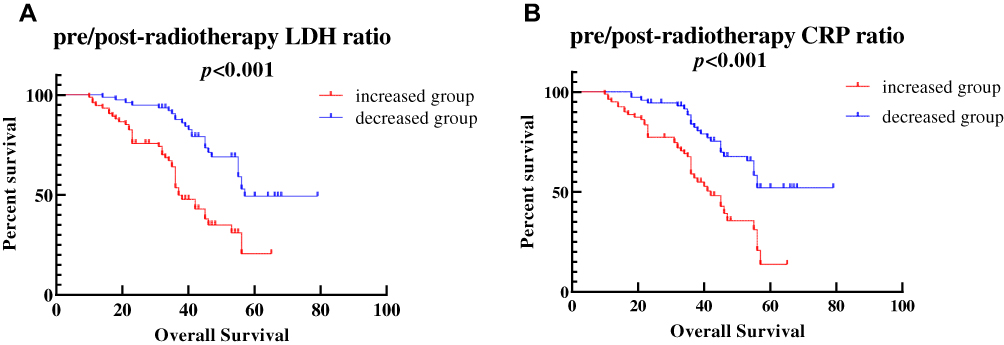 |
Figure 2 The relationships between pre-/post-radiotherapy lactate dehydrogenase (LDH)and C-reactive protein (CRP)ratios and prognosis. (A) LDH ratios with overall survival (OS). (B) CRP ratios with OS. |
The Relationship Between High Levels of Both LDH and CRP or High Pre-/Post-Radiotherapy Ratios of Both LDH and CRP with Survival of Cervical Cancer Patients
In pre-radiotherapy, the patients were divided into the following four groups based on LDH and CRP levels in median: high LDH and CRP group, high LDH group, high CRP group, and low LDH and CRP group. The high LDH and CRP group had the worst OS among the four groups (P =0.002) (Figure 3A).
 |
Figure 3 The relationships between different groups and prognosis. (A) The overall survival (OS) according to different pre-radiotherapy groups. (B) The OS according to different pre/post-radiotherapy groups. |
For the pre-/post-radiotherapy ratio, the patients were divided into the following four groups, based on the LDH or CRP ratios: high LDH and CRP ratio group, high LDH ratio group, high CRP ratio group, and low LDH and CRP ratio group. The high LDH and CRP ratio group had the worst OS of the four groups (P <0.001) (Figure 3B).
Cox Regression Analysis of Pre-Radiotherapy Parameters
In univariate analysis, high FIGO stage (HR 1.889; 95% CI = 1.345–2.653; P<0.001) and high LDH and CRP levels (HR 1.723; 95% CI = 1.265–2.348; P<0.001) were significant risk factors for worse prognosis (Figure 4A). In multivariate analysis, high FIGO stage (HR 1.817; 95% CI = 1.288–2.565; P<0.001) and the high LDH and CRP levels (HR 1.632; 95% CI = 1.186–2.244; P=0.003) were found to be independently associated with worse survival (Figure 4B).
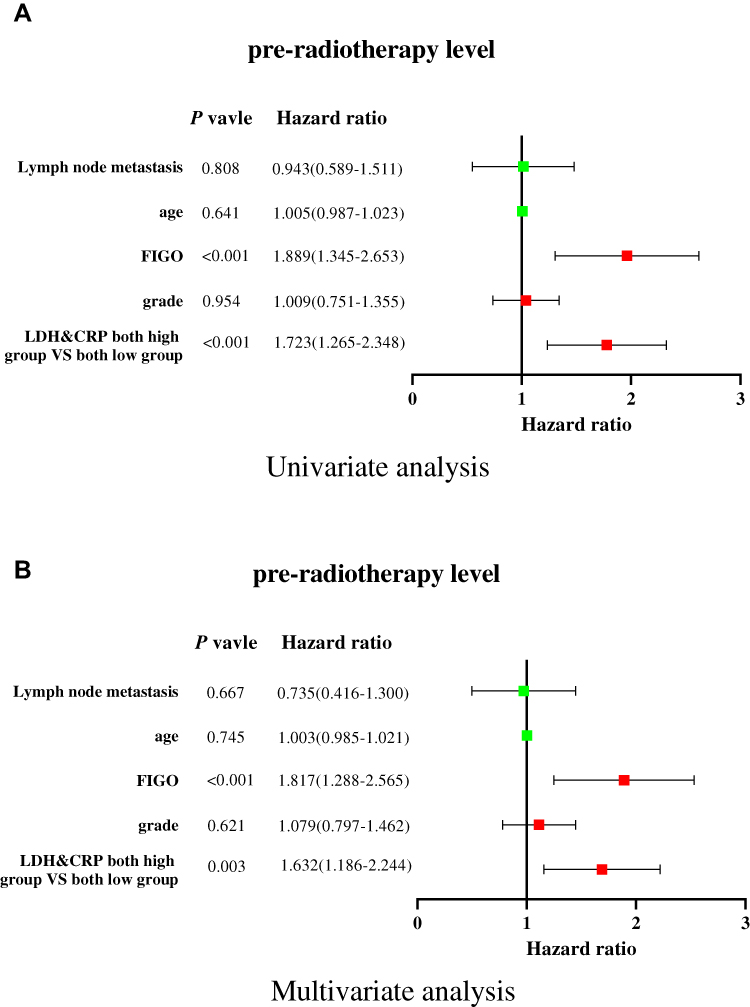 |
Figure 4 Cox regression analysis of pre-radiotherapy lactate dehydrogenase (LDH) and C-reactive protein (CRP) levels with prognosis. (A) Univariate analysis. (B) Multivariate analysis. |
Cox Regression Analysis of Pre-/Post-Radiotherapy Ratio Parameters
The univariate analysis indicated that a high FIGO stage (HR 1.889; 95% CI = 1.345–2.653; P<0.001) and high ratios of both LDH and CR. (HR 2.339; 95% CI = 1.704–3.221; P<0.001) were significant risk factors for worse prognosis (Figure 5A). In multivariate analysis (Figure 5B), a high FIGO stage (HR 1.843; 95% CI = 1.298–2.616; P<0.001) and high ratios of both LDH and CRP (HR 2.373; 95% CI = 1.700–3.314; P<0.001) were found to be independently associated with worse survival.
 |
Figure 5 Cox regression analysis of pre-/post-radiotherapy lactate dehydrogenase (LDH) and C-reactive protein (CRP) ratios with prognosis. (A) Univariate analysis. (B) Multivariate analysis. |
The Correlation of LDH with CRP
The pre-radiotherapy LDH level had a positive correlation with the pre-radiotherapy CRP level (P <0.001, r=0.282) (Figure 6A). The post-radiotherapy LDH level had a positive correlation with the post-radiotherapy CRP level (P <0.001, r=0.390) (Figure 6B).
 |
Figure 6 The relationships between the levels of lactate dehydrogenase (LDH) and C-reactive protein (CRP). (A) Pre-radiotherapy levels of LDH and CRP. (B) Post-radiotherapy levels of LDH and CRP. |
The Correlation of LDH or CRP with Squamous Cell Carcinoma Antigen (SCC-Ag) Levels
The pre-radiotherapy LDH level had a positive correlation with the SCC-Ag level (P <0.001, r=0.617) (Figure 7A). The pre-radiotherapy CRP level also had positive correlation with the SCC-Ag level, as shown in Figure 7B (P <0.001, r=0.521). The post-radiotherapy LDH level had a positive correlation with the SCC-Ag level (P =0.020, r=0.422) (Figure 7C). The post-radiotherapy CRP level had a positive correlation with the SCC-Ag level (P =0.038, r=0.381) (Figure 7D).
 |
Figure 7 The relationships between the levels of lactate dehydrogenase (LDH)or C-reactive protein (CRP)and the level of squamous cell carcinoma antigen(SCC-Ag). (A) Pre-radiotherapy levels of LDH and SCC-Ag. (B) Pre-radiotherapy levels of CRP and SCC-Ag. (C) Post-radiotherapy levels of LDH and SCC-Ag. (D) Post-radiotherapy levels of CRP and SCC-Ag. |
Discussion
In this study, we found that patients with high levels of serum LDH and CRP before radiotherapy and patients with increased LDH and CRP ratios had a worse OS in cervical cancer.
CRP is an acute-phase protein produced and secreted by hepatocytes.19 Polterauer et al demonstrated that patients with high pre-treatment CRP levels(CRP>0.5mg/dL) had worse prognosis than those with low CRP levels (CRP<0.5mg/dL) in cervical cancer.20 Cervical cancer-associated molecules induced by inflammation include tumor necrosis factor (TNF), chemokines, interleukins, and reactive oxygen species (ROS).8 Inflammatory factors such as IL-6, IL-1, and TNF can induce CRP production in the liver as part of the inflammatory response,19 and the potential mechanisms involved primarily include the following: First, in cervical cancer, TNF can induce the production of amphiregulin, which further leads to the proliferation of cervical cancer cells, while IL-6 and IL-1 have roles in the growth and metastasis of cervical cancer cells.8 Second, the occurrence of cervical cancer is closely related to HPV infection (especially HPV16 and HPV18).3 Infection by HPV18 leads to DNA damage, increased production of nitric oxide (NO), and activation of cyclooxygenase-2 (COX-2)/prostaglandin (PG)/PG receptors in cervical tissue, which in turn results in local inflammation and tumor formation.8
Li et al showed that patients with a high level of LDH (LDH≥252μ/L) had worse recurrence-free survival.21 An increased serum LDH level leads to a cascade downstream of hypoxia-inducible factor1 (HIF-1), resulting in the secretion of vascular endothelial growth factor (VEGF) by tumor cells. In addition, increased HIF-1 activity further up regulates that of LDH, resulting in the formation of a positive feedback loop, and a tumor microenvironment that is conducive to tumor angiogenesis and metastasis.22,23 Furthermore, according to the Warburg effect, the serum level of LDH is positively correlated with glucose uptake, tumor tissue metabolism, and tumor invasiveness.24 Consequently, up regulation of serum LDH levels is tightly associated with poor outcome.21
Through further analysis, we found that the levels of LDH and CRP were positively correlated with the levels of SCC-Ag, one of the currently used prognostic indicators of cervical cancer. Duk et al found that SCC-Ag is associated with cervical cancer FIGO stage and tumor size,25 while Guo et al reported that cervical cancer patients with elevated levels of SCC-Ag(>2.75mg/mL) had worse prognosis.26
In the present study, patients were further divided into four groups, namely, a group with high levels of LDH and CRP, a group with a high level of LDH, a group with a high level of CRP, and a group with low levels of both LDH and CRP. The analysis showed that the group with high levels of both LDH and CRP had the worst prognosis among the four groups. In addition, we found that LDH levels were positively correlated with those of CRP. Few studies have combined these two indicators in outcome evaluation. In our previous study, we found that patients with high preoperative LDH or CRP levels had a worse prognosis in resectable cervical cancer; however, no association was found between the two serum parameters.
There were some limitations in our research. First, this was a retrospective study involving only two centers, and a multi-center study should be performed in future research. Second, we only evaluated systemic-inflammation related parameters, and other laboratory indicators should be combined in future investigations to improve cervical cancer prognosis.
Conclusion
In summary, for the first time, we used a combined evaluation of LDH and CRP levels to predict the prognosis of patients with cervical cancer after CCRT. In the present study, both high pre-radiotherapy LDH and CRP levels and increased pre-/post-radiotherapy LDH and CRP ratios were correlated with worst OS in locally advanced cervical cancer. These convenient clinical indicators may be combined in the near future to guide the personalized treatment of cervical cancer patients.
Acknowledgment
We thank Wei Shan for his assistance with statistical analyses.
Author Contributions
WJW conceived and designed the study. HW and YHZ collected the data. HW and MSW interpreted and analyzed the data. HW, MSW, and YHZ wrote the manuscript. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
2. Walboomers JM, Jacobs MV, Manos MM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189(1):12–19. doi:10.1002/(SICI)1096-9896(199909)189:1<12::AID-PATH431>3.0.CO;2-F
3. Crosbie EJ, Einstein MH, Franceschi S, Kitchener HC. Human papillomavirus and cervical cancer. Lancet. 2013;382(9895):889–899. doi:10.1016/S0140-6736(13)60022-7
4. Correction: concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N Engl J Med. 1999;341(9):708. doi:10.1056/NEJM199908263410923
5. Mikami M, Aoki Y, Sakamoto M, et al. Disease committee of Uterine C et al: surgical principles for managing stage IB2, IIA2, and IIB uterine cervical cancer (bulky tumors) in Japan: a survey of the Japanese Gynecologic Oncology Group. Int J Gynecol Cancer. 2014;24(7):1333–1340. doi:10.1097/IGC.0000000000000202
6. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003;111(12):1805–1812. doi:10.1172/JCI200318921
7. Mahmoud FA, Rivera NI. The role of C-reactive protein as a prognostic indicator in advanced cancer. Curr Oncol Rep. 2002;4(3):250–255. doi:10.1007/s11912-002-0023-1
8. Deivendran S, Marzook KH, Radhakrishna Pillai M. The role of inflammation in cervical cancer. Adv Exp Med Biol. 2014;816:377–399.
9. Jabs WJ, Busse M, Kruger S, Jocham D, Steinhoff J, Doehn C. Expression of C-reactive protein by renal cell carcinomas and unaffected surrounding renal tissue. Kidney Int. 2005;68(5):2103–2110. doi:10.1111/j.1523-1755.2005.00666.x
10. Nozoe T, Saeki H, Sugimachi K. Significance of preoperative elevation of serum C-reactive protein as an indicator of prognosis in esophageal carcinoma. Am J Surg. 2001;182(2):197–201. doi:10.1016/S0002-9610(01)00684-5
11. Nozoe T, Matsumata T, Kitamura M, Sugimachi K. Significance of preoperative elevation of serum C-reactive protein as an indicator for prognosis in colorectal cancer. Am J Surg. 1998;176(4):335–338. doi:10.1016/S0002-9610(98)00204-9
12. Koch A, Fohlin H, Sorenson S. Prognostic significance of C-reactive protein and smoking in patients with advanced non-small cell lung cancer treated with first-line palliative chemotherapy. J Thorac Oncol. 2009;4(3):326–332. doi:10.1097/JTO.0b013e31819578c8
13. Wang WJ, Li Y, Zhu J, Gao MJ, Shi JP, Huang YQ. Prognostic values of Systemic Inflammation Response (SIR) parameters in resectable cervical cancer. Dose Response. 2019;17(1):1559325819829543.
14. Markert CL. Lactate dehydrogenase isozymes: dissociation and recombination of subunits. Science. 1963;140(3573):1329–1330. doi:10.1126/science.140.3573.1329
15. Souhami RL, Bradbury I, Geddes DM, Spiro SG, Harper PG, Tobias JS. Prognostic significance of laboratory parameters measured at diagnosis in small cell carcinoma of the lung. Cancer Res. 1985;45(6):2878–2882.
16. Scartozzi M, Giampieri R, Maccaroni E, et al. Pre-treatment lactate dehydrogenase levels as predictor of efficacy of first-line bevacizumab-based therapy in metastatic colorectal cancer patients. Br J Cancer. 2012;106(5):799–804. doi:10.1038/bjc.2012.17
17. Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105(2):103–104. doi:10.1016/j.ijgo.2009.02.012
18. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
19. Douglas JB, Silverman DT, Weinstein SJ, et al. Serum C-reactive protein and risk of pancreatic cancer in two nested, case-control studies. Cancer Epidemiol Biomarkers Prev. 2011;20(2):359–369. doi:10.1158/1055-9965.EPI-10-1024
20. Polterauer S, Grimm C, Tempfer C, et al. C-reactive protein is a prognostic parameter in patients with cervical cancer. Gynecol Oncol. 2007;107(1):114–117. doi:10.1016/j.ygyno.2007.06.001
21. Li J, Wu MF, Lu HW, Chen Q, Lin ZQ, Wang LJ. Pretreatment serum lactate dehydrogenase is an independent prognostic factor for patients receiving neoadjuvant chemotherapy for locally advanced cervical cancer. Cancer Med. 2016;5(8):1863–1872. doi:10.1002/cam4.779
22. Lu H, Forbes RA, Verma A. Hypoxia-inducible factor 1 activation by aerobic glycolysis implicates the warburg effect in carcinogenesis. J Biol Chem. 2002;277(26):23111–23115. doi:10.1074/jbc.M202487200
23. Harris AL. Hypoxia–a key regulatory factor in tumour growth. Nat Rev Cancer. 2002;2(1):38–47. doi:10.1038/nrc704
24. Sun X, Sun Z, Zhu Z, et al. Clinicopathological significance and prognostic value of lactate dehydrogenase A expression in gastric cancer patients. PLoS One. 2014;9(3):e91068. doi:10.1371/journal.pone.0091068
25. Duk JM, Groenier KH, de Bruijn HW, et al. Pretreatment serum squamous cell carcinoma antigen: a newly identified prognostic factor in early-stage cervical carcinoma. J Clin Oncol. 1996;14(1):111–118. doi:10.1200/JCO.1996.14.1.111
26. Guo Q, Zhu J, Wu Y, et al. Predictive value of preoperative serum squamous cell carcinoma antigen (SCC-Ag) level on tumor recurrence in cervical squamous cell carcinoma patients treated with radical surgery: a single-institution study. Eur J Surg Oncol. 2019:
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.