Back to Journals » Clinical Ophthalmology » Volume 19
Profile and Management Outcomes of Neurotrophic Keratitis at A Tertiary Eye Hospital in Saudi Arabia: A Cohort Study
Authors Al Azaz R ![]() , Khandekar R
, Khandekar R ![]() , Al Ghadeer H
, Al Ghadeer H
Received 15 May 2025
Accepted for publication 29 September 2025
Published 15 October 2025 Volume 2025:19 Pages 3815—3826
DOI https://doi.org/10.2147/OPTH.S540546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Rand Al Azaz,1 Rajiv Khandekar,2 Huda Al Ghadeer3
1Ophthalmology Department, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia; 2Research Department, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia; 3Emergency Department, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia
Correspondence: Huda Al Ghadeer, King Khaled Eye Specialist Hospital and Research Center, PO Box 7191, Riyadh, 11462, Saudi Arabia, Tel +966 1 4821234 ext. 2500, Email [email protected]
Purpose: To evaluate the neurotrophic keratitis (NK) profile, management outcomes, and determinants at a tertiary eye hospital in Saudi Arabia.
Methods: This historical cohort comprised patients with the ICD-10 code of H16.239 who presented and were treated from 2014 to 2024. The classification of NK based on Mackie’s criteria; NK was classified into stages 1– 3. Demographic data, NK etiology, and both medical and surgical therapeutic interventions were analyzed. We correlated these outcomes with the etiology, stages, and treatment modalities.
Results: The cohort had 94 eyes of 80 NK patients in stage 1 (6, 6%), stage 2 (69, 74%), and stage 3 (19, 20%). Seventy-Three (77.7%) eyes showed reduced corneal sensation, 14 (15%) eyes showed intact corneal sensation, and 7 (7.4%) eyes showed no discernible corneal sensation. Herpes zoster (22.5%) was the most common infectious etiology followed by herpes simplex (2.5%). Trigeminal palsy was observed in 24 (30%) eyes. Iatrogenic NK was present in 12 (15%) eyes. Decreased vision (88.1%), redness of the eyes (47.6%), and swollen lids (34.5%) were the main symptoms. The most frequently performed procedures included amniotic membrane transplantation (AMT) (45.7%), tarsorrhaphy (36.2%), and corneal gluing (17%). At the last follow-up after management, the Best Corrected Visual Acuity (BCVA) was 1.5 logMAR in eyes affected by NK. At presentation (78.2%) and after treatment (38.2%), eyes with NK had severe visual impairment (SVI).
Conclusion: The management of NK presents significant challenges but offers potential rewards, as it facilitates ocular preservation and may enable visual restoration following initial therapeutic intervention.
Keywords: cornea, corneal neurotization, neurotrophic keratitis, ocular surface disease
Introduction
In Neurotrophic Keratitis (NK), corneal epitheliopathy leads to an epithelial defect with or without stromal ulceration, accompanied by reduced or absent corneal sensation. It is associated with several systemic and ocular disorders.1 NK is a relatively uncommon condition, with a prevalence of less than 11 per 10,000. The underlying etiology of NK includes herpes simplex (6%), herpes zoster (12.8%), and surgery for trigeminal neuralgia (2.8%).2 Systemic diseases, trauma, surgery, topical drug toxicity, and abuse of contact lenses are other known risk factors for NK.3,4
The management aims to halt and reverse the progression of NK, depending on the stage of NK at presentation. For eyes with mild NK, treatment focuses on preventing epithelial defect formation and accelerating the healing process. For moderate NK, halting further damage to the corneal stroma and reepithelialization of the defect are targeted. In severe NK, preventing perforation, restoring the anatomical contour of the globe, and providing alternatives for future visual rehabilitation are the expected outcomes. Medical treatments aim to prevent infections, reduce inflammation, provide tear substitutes, utilize biological substitutes to cover and heal defects, and regenerate the corneal nerve plexus. Surgeries include tarsorrhaphy, AMT, debridement of damaged corneal stroma, using tissue sealant to plug perforation, plugging the puncta, conjunctival flaps, and therapeutic keratoplasty.1,5–7
Studies on NK included ophthalmic manifestations in dermatological conditions due to both Herpes zoster and herpes simplex infections.8–10 A study in Bahrain found that amniotic membrane treatment was effective in treating 32 nonhealing corneal ulcers. However, NK in these cases was not reported.11 To the best of our knowledge, the profile and management outcomes of NK in the Arab population remain undocumented.
We present the profile and management outcomes of NK patients treated between 2014 and 2024 at our institution in central Saudi Arabia.
Methods
This study received approval from the Ethics Committee at King Khaled Eye Specialist Hospital and Research Center (KKESH&RC). Written informed consent was obtained from all participants. Throughout the study, we adhered to the principles outlined in the Declaration of Helsinki. To protect participants’ privacy, we implemented measures to anonymize their identities.
This historical cohort study was conducted at KKESH&RC in Riyadh, Saudi Arabia from 2014 to 2024. The target population comprised all patients identified through electronic medical records with the (ICD-10) code of H16.239, who presented and were treated at KKESH&RC during the study period. Additionally, cases of Herpes zoster keratoconjunctivitis (B02.33), Herpes simplex keratitis (B00.52), and trigeminal nerve palsy (G50.9) were reviewed to determine if any exhibited features of NK.12 The information on NK patients before diagnosis was retrospectively collected, while the details of management and their outcomes were prospectively collected in this cohort.
To calculate the sample size for a cohort study, we assumed that the deterioration of BCVA by more than 15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters (3 lines) could occur in 22.5% of cases after the management, compared to 45% of eyes with SVI before treatment.13 To achieve a 95% confidence interval and 80% power in a cohort study, we needed to evaluate at least 76 cases of NK. We used OpenEpi software to estimate the sample size for a single-arm cohort study.14
The demographic information of the patients included their age at presentation, gender, affected eye, and laterality. We documented the ocular cause of NK, the status of the 5th nerve, systemic conditions, iatrogenic and injury causes, use of topical medications. We measured uncorrected visual acuity (UCVA) and BCVA for distance using Snellen charts at distances of 3 and 1 meters, and vision was recorded using logMAR values. We also assessed the NK-affected eye’s light perception in four quadrants. Symptoms, corneal sensation, and complications were documented. At our institute, all cases of keratitis are treated. After taking aseptic precautions, we tested corneal sensation in both eyes using a handheld esthesiometer (Cochet-Bonnet, USA). The filament length was gradually reduced on the cornea until the patient reported a feeling of touch, and a quantitative assessment of corneal sensation was recorded.15,16 A detailed slit-lamp biomicroscopic assessment (Topcon, USA) was performed to evaluate the tear film, cornea, and conjunctiva. Fluorescein staining was used to assess the extent of the epithelial defect. Clinical findings were used to determine the stage of NK in each eye.17 Mackie’s classification has been used to categorize NK into three stages: stage 1, superficial punctate keratopathy; stage 2, recurrent or persistent oval or circular epithelial defects; and stage 3, corneal ulcer with stromal involvement.3
For mild cases of NK, medical therapy was initiated. A combination of medical and surgical procedures was initiated for moderate and severe NK cases. If complications, such as infective keratitis, were present, the patient was hospitalised. Corneal scrapings were collected from the undermined edge of the corneal defect for culture and sensitivity testing. Broad-spectrum topical antibiotics were started, and if a fungal infection was suspected, antifungal topical medication was added. The type, frequency, and duration of medication usage were recorded. Corneal gluing was performed in sixteen patients in our study. Corneal gluing with cyanoacrylate tissue adhesive is best used with the operating microscope under aseptic conditions. Topical anaesthetics should be used. An eye speculum must be employed to achieve optimal exposure. The slough epithelium is gently removed from the site using the cellulose sponge. A one millimetre syringe is used to withdraw glue using a 20-gauge needle. A Rycroft cannula (27 gauge) is placed over the tip of the syringe. The plunger is pushed in until a small drop of glue is visible at the tip of the cannula. The area of perforation is dried, and the drop is allowed to touch gently over the perforated area. A bandage contact lens was subsequently placed. Tarsorrhaphy is a surgical procedure where the upper and lower eyelids are wholly or partially sewn together. Tarsorrhaphy is performed to protect the cornea by reducing exposure and promoting healing. AMT is a surgical procedure that involves transplanting the innermost layer of the placenta, known as the amniotic membrane, onto the ocular surface. This membrane consists of a thick basement membrane and an avascular stromal matrix, making it highly beneficial for healing and regeneration. Therapeutic penetrating keratoplasty refers to replacing a diseased host cornea with a full-thickness donor corneal tissue to eliminate focal infectious disease. Corneal neurotization is a novel surgical technique used to restore corneal sensation. It involves transferring healthy nerves to the cornea to re-establish sensation. Post-treatment BCVA was measured using the same method as at presentation. A significant improvement was considered if visual acuity improved by more than three lines on the Snellen chart. If the eye became phthisical, it was classified as an anatomical failure of therapy. The status of the cornea at the last follow-up was also noted.
The data was collected using a Microsoft Excel® spreadsheet. After removing duplicates and performing consistency checks, the data were transferred to the Statistical Package for the Social Sciences (SPSS 25) (IBM, NY, USA). Qualitative variables were presented as numbers and percentages. Normally distributed numerical variables were presented as mean and standard deviation. For a small subsample, numerical data were presented as median, interquartile range (IQR), and minimum and maximum values. The outcome variable, eyes with SVI at the last follow-up after management, was analyzed in relation to independent variables to estimate relative risk, 95% confidence interval, and two-sided p-value. A p-value of <0.05 was considered statistically significant. The study site is the center of excellence for eye care in the country, and all suspected NK cases are referred to our cornea subspecialty unit for management. The adult Saudi population of 2019 (mid-study population) was used as the denominator for calculating the annual incidence.
Results
Our cohort comprised 94 eyes from 80 individuals with NK. The annual incidence of NK was 2.84 per 10 million Saudi population.
Demography and Clinical Presentation
Table 1 presents the characteristics of patients with NK. There were 13 (16.3%) children under the age of 15 with NK. Two-thirds of them were males. In two-thirds of patients, the etiology of NK was not known. One in eight patients with NK had diabetes. We noted NK in 37 right eyes, 29 left eyes, and bilateral in 14 eyes. Among the fourteen bilateral NK cases, the etiologies were determined in nine patients. There was one case of stroke, one case of face damage, four cases of congenital conditions, and three cases of Riley-Day syndrome. There were 6 (6%), 69 (74%), and 19 (20%) eyes with mild, moderate, and severe stages NK respectively. Two-thirds of eyes had stage 2 NK. Figures 1 and 2
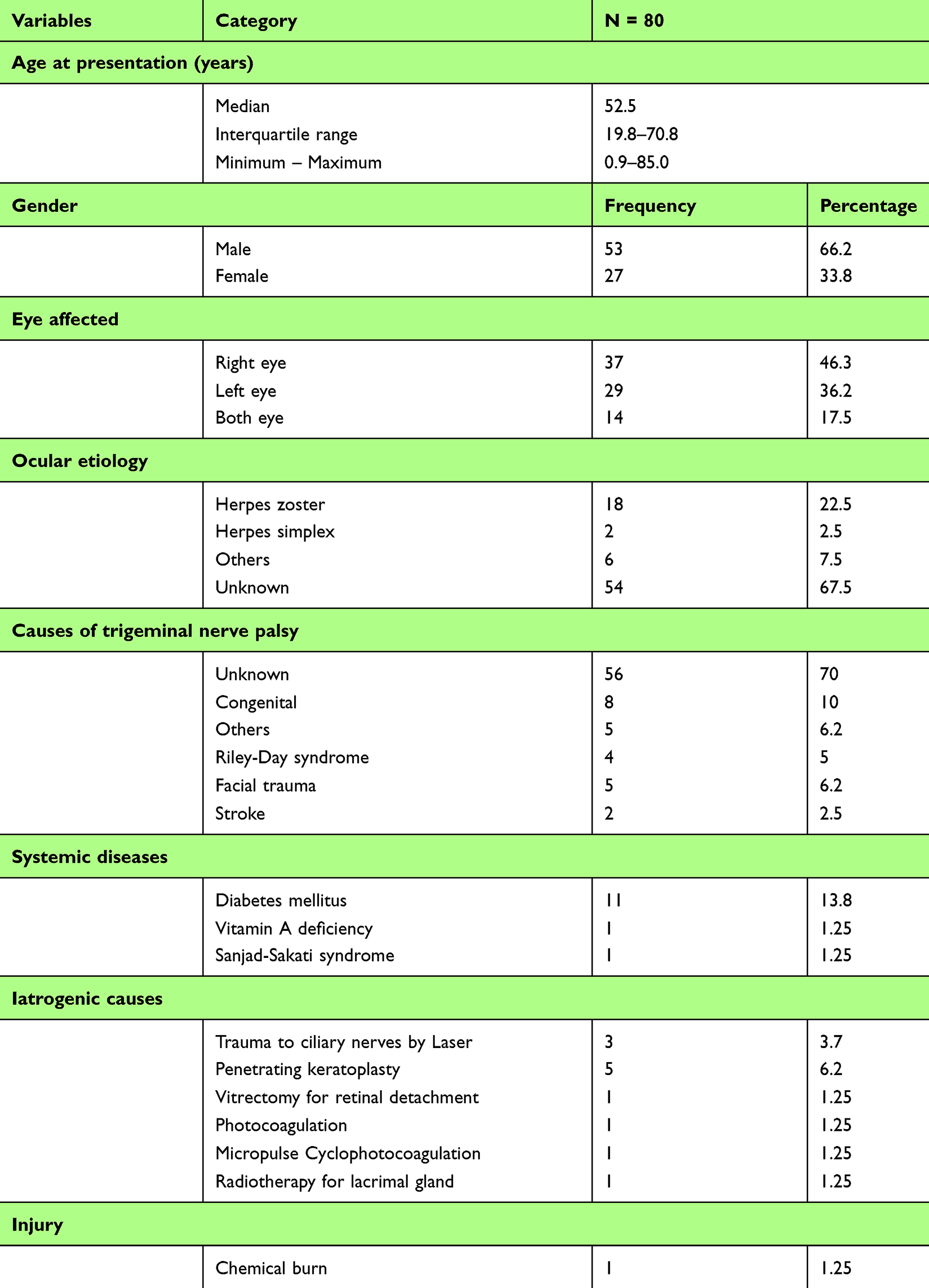 |
Table 1 Profile of Patients with Neurotrophic Keratitis (NK) |
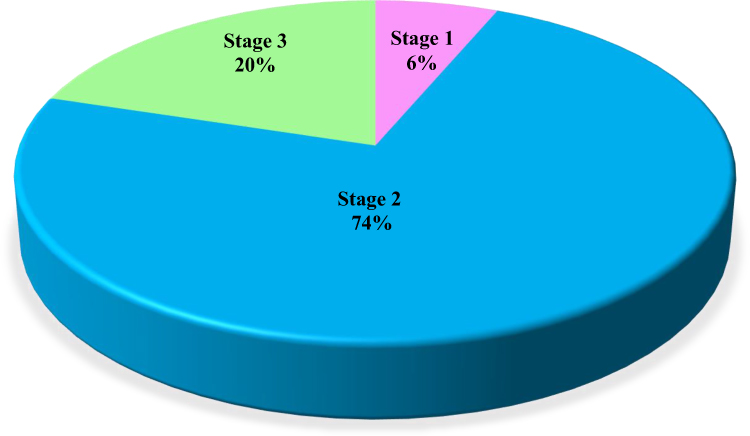 |
Figure 1 Distribution of stages of Neurotrophic Keratitis (NK). |
 |
Figure 2 Neurotrophic Keratitis (NK). (A) Stage 1: superficial punctate keratopathy with scattered small areas of dried epithelium (Gaule spots). (B) Stage 2: a persistent corneal epithelial defect with fluorescein staining, smooth, rolling edges, and stromal edema. (C) Stage 3: corneal ulcer with corneal perforation. |
The presenting symptoms of NK were reduced vision (74; 88.1%), red eyes (40; 47.6%), swollen eyelids (29; 34.5%), corneal opacity (22; 26.2%), intolerance to light (12; 14.3%), eye pain (10; 11.9%), and tearing (7; 8.3%). Seventeen patients (20.2%) with NK showed no symptoms. Corneal sensations were lost in 73 (77.7%), intact in 14 (15%), and undetermined in seven (7.4%) eyes with NK at presentation.
Treatment Modalities
Nonsurgical treatment included discontinuation of all topical medications (6; 6.4%), preservative-free artificial tears (93; 98.9%), autologous serum tears (57; 60.6%), corneal or scleral therapeutic contact lenses (48, 51.1%), N-acetylcysteine (3, 3.2%), vitamin C supplements (2; 2.1%). Table 2 presents the topical and systemic drugs delivered to the NK patients. Topical antibiotics included Ofloxacin (2.5%), Vigamox (72.5%), others (16.2%), combinations (2.5%), and not known (6.2%). Table 3 displays the surgical procedures performed on 94 eyes with NK as the first, second, and subsequent stages. AMT Figure 3 and tarsorrhaphy were the main procedures performed to manage NK.
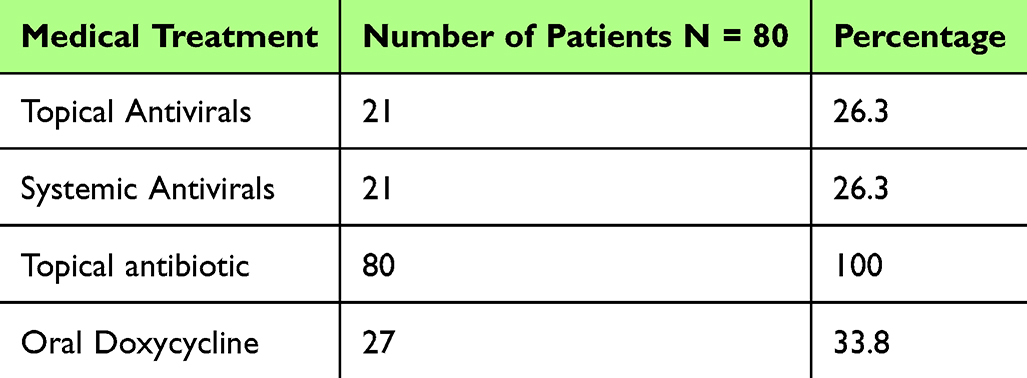 |
Table 2 Medical Treatment of Patients with Neurotrophic Keratitis (NK) |
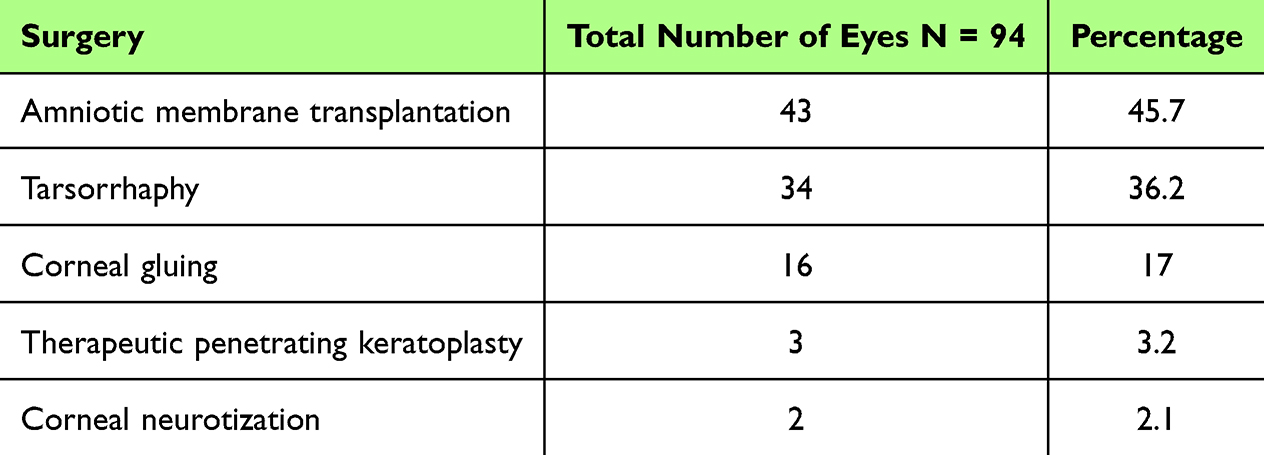 |
Table 3 Surgeries Performed on the Eyes with Neurotrophic Keratitis (NK) in Stages |
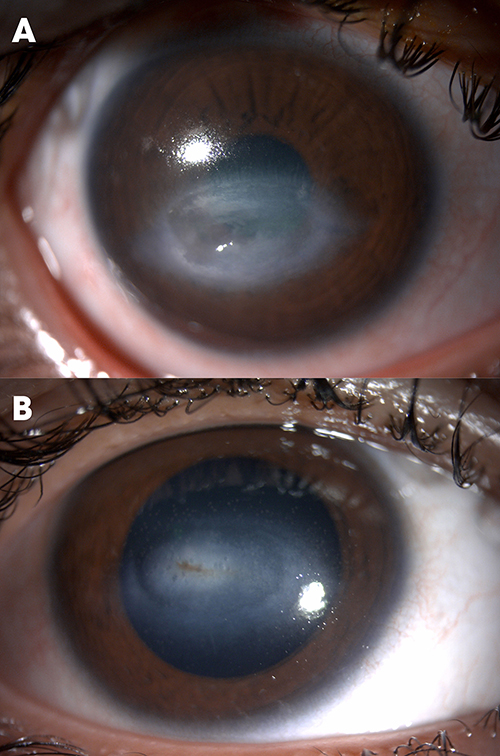 |
Figure 3 Neurotrophic keratitis (NK) stage 3 treated with amniotic membrane (A) before treatment. (B) after treatment. |
Figure 4 Demonstrate NK stage 2 before and after indirect corneal neurotization.
 |
Figure 4 Neurotrophic Keratitis (NK) stage 2 post indirect corneal neurotization OD from ipsilateral infraorbital nerve using a sural nerve interposition graft form left leg for neurotrophic keratopathy (A) before treatment. (B) after treatment. |
Complications
The complications observed during NK management in our study included corneal scarring (85; 90.4%), corneal neovascularization (53; 56.4%), corneal thinning (17; 18.1%), secondary bacterial keratitis (16; 17%), vision loss (13, 13.8%), corneal perforation (12; 12.8%), corneal melting (7; 7.4%), and glaucoma (7;7.4%).
Visual Outcomes
The median BCVA at the time of the initial examination with a sample size of 94, was 1.5 logMAR. The interquartile range (IQR) for BCVA was 0.9 to 1.6, while the range of BCVA values observed ranged from 0.0 to 1.9. The median best corrected visual acuity at the final follow-up with a sample size of 94, was 1.5 logMAR. The interquartile range (IQR) was 1.15 to 1.6, and the range of values observed ranged from 0.0 to 2.0. There was no significant difference in the visual acuity (VA) after 28 months of treatment compared to VA at the beginning of treatment in the same eye. The value of Z was −0.342 and the p-value of the Wilcoxon test was 0.732. The percentage of eyes with NK that had vision worse than 1.3 logMAR (considered blind according to the WHO standard) increased from 56.4% to 64.9%. At the final follow-up assessment, 73 eyes exhibited SVI, whereas 21 eyes demonstrated vision >1 logMAR. At last visit, the visual outcome of 55 surgically treated NK cases was a median of 1.5 (IQR 1.4; 1.6) logMAR, while 38 eyes treated medically had a median vision of 1.5 (IQR 0.83; 1.6) logMAR. Vision information was missing in two eyes. The visual outcome of medically vs medically and surgically treated eyes with NK was not significantly different (Mann Whitney U-test; z −1.5, P = 0.16).
Among the medically treated group, complications were corneal scarring (63.8%), secondary bacterial keratitis (16.3%), corneal perforation (10%), corneal melting (6.3%), corneal neovascularization (1.3%), and corneal thinning (1.3%).
The visual impairment grades at the final follow-up examination of 94 eyes with NK were analyzed in relation to the demographic characteristics and variables present at initial presentation. Table 4
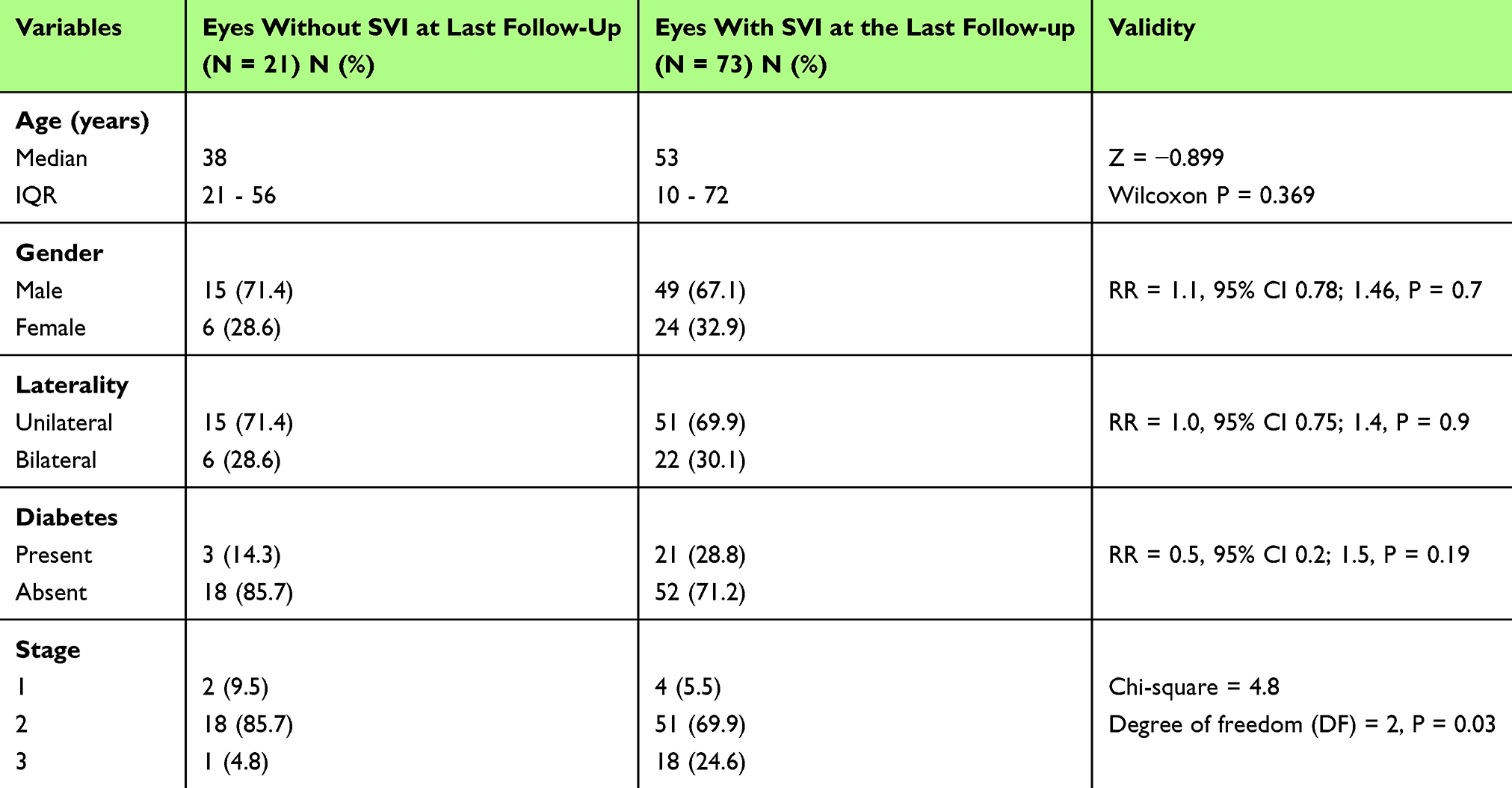 |
Table 4 Determinants of Severe Visual Impairment (SVI) After Managing Neurotrophic Keratitis (NK) |
Discussion
Summary of Main Findings
NK is a relatively uncommon ocular condition with an annual incidence of 2.84 per 10 million in the Saudi population. Despite standard management protocols, NK results in severe visual impairment. Early diagnosis through routine corneal sensation testing in cases of keratitis coupled with adherence to standard management protocols facilitates rapid recovery and preservation of residual vision. We found that prolonged management and constant monitoring allowed the cornea to heal, and the patients were potential candidates for low-vision rehabilitation.
Strength of the Present Research Paper
To our knowledge, this is the first study on NK on an extensive series of Arab patients. The clinical presentations and therapeutic approaches described in this study, both medical and surgical, may prove beneficial to corneal surgeons and general ophthalmologists in facilitating early detection, implementing appropriate management strategies, and providing informed counsel to patients and caregivers regarding potentially limited visual outcomes. Data from a tertiary eye hospital with facilities for therapeutic keratoplasty, experienced corneal surgeons, and availability of laboratory and radiological imaging services suggest that the outcomes of NK reflect the limitations of standard management in vision restoration.
Comparison of the Primary Outcomes with the Literature
The present study reports the annual incidence of NK in Saudi Arabia is 2.84 per 10 million population. This incidence was significantly lower than the 11/10,000 observed in France between 2009 and 2017, as well as the 0.1–0.3/10,000 reported in Germany.3,4 In the absence of direct evidence, Sacchetti et al estimated the incidence of NK in the UK by extrapolating data on underlying causes of NK. They predicted that the incidence of NK would be less than 1.6/10,000.6
The lower incidence of type 1 HSV, one of the primary underlying causes of NK in the Middle Eastern region compared with African and Southeast Asian countries, may account for the reduced rates of NK observed in the present study.9 The etiology of NK is unknown in two-thirds of the cases, which warrants further investigation. Although NK is characterized as rare, it is considered significantly underdiagnosed. Expert consensus identifies most cases accurately, showing that knowledge of the characteristic signs and symptoms of the disease leads to the correct diagnosis and treatment of this condition.18 Since many of these patients had been treated by other ophthalmologists before being referred to us, the underlying infectious etiology could not be elicited appropriately.
The current study investigated NK in patients with a median age of 52.5 years with a male predominance (two-thirds). In contrast, a large cohort study of NK patients in the USA reported a mean age of 68 years, with females comprising nearly 60% of the population.19 Furthermore, research on NK in the Hispanic population in California reported a mean age of 80 years, with 55% of the subjects being female.20
Our study observed male predominance and a younger age of presentation among NK patients, which differed from other studies and warrants further investigation. Males may have a greater preponderance for NK. The exact cause of this discrepancy between the genders remains indeterminate.4,21
Corneal sensation assessment is a crucial diagnostic test for NK. In our study, 77% of the eyes with NK had lost corneal sensation. However, 15% of the patients demonstrated had normal sensation. We observed no significant correlation between corneal sensation and the stage of NK or visual impairment. Corneal sensation in NK may be linked to its underlying etiology. Herpes zoster keratitis is known to result in loss of corneal sensation.22 In our study, we used the Cochet-Bonnet esthesiometer, which provides quantitative measurement of the corneal sensation. The Belmonte aesthesiometer uses a non-contact technique which could be a future mode of assessment and monitoring progress in corneal sensation.15 The role of viable corneal sensation and viable transfer of impulses through the nerve plexus is established. The cornea is innervated by the trigeminal nerve, which has 300–600 times greater fibres than in the skin.23 They are essential for the blink reflex and protect the corneal surface from damage. To initiate the repair system after epithelial injury, it is crucial to establish communication between neuronal cells and epithelial cells.24 If the healing process is impeded or delayed, the stroma is susceptible to enzymatic degradation, melting, and perforation. Consequently, epithelial and tear film alterations develop in mild NK. Moderate NK is typically associated with epithelial defects, whereas severe NK is distinguished by stromal ulceration and perforation.25
Seventy-four percent of eyes with NK presented with stage 2 changes, whereas 20% presented with advanced stage 3. General ophthalmologists should thoroughly evaluate corneal ulcers to rule out the possibility of NK, particularly in the presence of known risk factors, and promptly refer patients to a corneal specialist for further management.
Medical management of eyes with NK primarily involves the use of preservative-free artificial tears and application of autologous serum. The commonly used preservative benzalkonium chloride is known to cause an inflammatory response in the eyes and a toxic effect on the ocular surface, resulting in delayed healing after long-term use.26 Autologous serum tears have been shown to be effective in dry eyes and NK in patients with herpes zoster as the underlying etiology.2,22,27
Autologous serum is an eye drop that is derived from the patient’s blood. The serum is produced by extracting blood from the patient, coagulation, centrifugation, and dilution with sterile saline. It is subsequently stored in the freezer. The concentration of autologous serum should typically be between 20% and 50%. While the components are nearly identical to those of basal tears, autologous serum generally contains a higher concentration of each component than basal tears.28
In our study, one-third of the eyes with NK underwent tarsorrhaphy, which corresponds to Trinh et al’s report of 35% of the eyes with NK managed with this technique.29 This surgical procedure prevents eyelid blinking and external agents from damaging the lid aperture, thereby providing the ocular surface with an opportunity to heal.1
In our study, 43% of the NK eyes underwent AMT. Of these, AMT was the 1st surgical procedure in 28%. In this study, SVI was not associated with AMT-treated eyes. Roumeau et al’s meta-analysis observed that nerve growth factor eye drops, and AMT improved visual acuity in eyes with NK.30
In the current study, three eyes presenting with a severe NK affecting the central cornea underwent therapeutic keratoplasty as a secondary surgical intervention. The use of tectonic keratoplasties has significantly declined due to the development of novel surgeries for corneal nerve regeneration and improved surgical procedures such as the Boston keratoprosthesis for visual rehabilitation. This decrease can be mainly attributed to the higher rate of rejection.5
In our study, two eyes underwent corneal neurotization. Corneal neurotization is a novel surgical technique used to restore corneal sensation in patients with neurotrophic keratopathy.6
It has demonstrated significant efficacy in restoring corneal sensation, improving visual acuity, and promoting corneal epithelial health. Various methods for corneal neurotization are available, including direct nerve transfers and indirect neurotization by interposition nerve grafts.31–34
The direct method regenerates the corneal nerve plexus by using the supratrochlear or supratemporal branches of the trigeminal nerve. This method sacrifices the other trigeminal nerve branches, leading to aesthetic concerns. In the indirect method of corneal neurotization, surgeons employ the sural nerve of the leg for nerve fibril regeneration. This procedure is a time-intensive multi-specialty surgery but demonstrates nearly 100% efficacy in restoring corneal sensation and healing of NK.1,31–34
Upon suspicion of NK, various etiologies must be thoroughly investigated, and medications that contain preservatives that are potentially toxic to the cornea should be discontinued. Clinical examinations should assess for dryness, ocular surface disease, and lagophthalmos, while NK should be graded according to the Mackie staging system to determine management strategies. All patients must receive rapid treatment and be constantly monitored.3 Nonetheless, major progress in prevention, early identification, and successful treatment of the disease is necessary.3
The climate in Saudi Arabia is typically hot in the summer and cold in the winter. Most modern cities are climate-controlled indoors, with limited exposure to extreme temperatures. Humidity is very low in all places except the coastal area. It is challenging to explain the relationship between temperature and humidity elements in Saudi Arabia with NK.
Limitations of the Present Study
Our study has several limitations including that NK is a rare condition. Hence, we are only able to enrol a cohort of 80 patients (94 eyes) with NK. We encourage judicious interpretation of the association of outcomes within subgroups due to the small subsample sizes and potential bias due to the involvement of multiple corneal surgeons who assessed and managed NK. We predicted the incidence of NK in the population under the assumption that all NK cases were referred to our centre in Saudi Arabia. However, if other institutions treated mild NK cases instead of referring to our facility, this estimate might be conservative. We were unable to investigate the etiology and risk factors of NK progression because we did not gather data on the progression of NK from mild to moderate and severe stages during treatment.
Conclusions
Management of NK aims to preserve the anatomic configuration of the eyeball and initiate vision restoration procedures once the keratitis has healed. One in four eyes with NK was not legally blind, and only one eye was phthisical after NK management. Effective treatment of keratitis has the potential to restore vision. This emphasizes the importance of corneal surgeons embracing innovative treatment approaches and providing lifelong follow-up care, as these patients may require future interventions to improve vision.
Abbreviations
NK, Neurotrophic keratitis; AMT, Amniotic membrane transplantation; BCVA, Best corrected visual acuity; SVI, Severe visual impairment; UCVA, Uncorrected visual acuity.
Ethical Statement
The study was authorized by the King Khaled Eye Specialist Hospital and research canter’s local ethical board and followed the Helsinki Declaration’s tenets. All participants’ parents/guardians have provided written informed consent for their children to participate in this study.
Acknowledgment
We would like to thank Muneera Fahad Al Futais, the Clinical Research Coordinator for her contribution to this Research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper received no funding.
Disclosure
The researchers declared that they were not involved in any conflicts of interest.
No further financial interests in the submitted work have been reported by any of the authors.
References
1. Dua HS, Said DG, Messmer EM, et al. Neurotrophic keratopathy. Prog Retin Eye Res. 2018;66:107–131. doi:10.1016/j.preteyeres.2018.04.003
2. Pérez-Bartolomé F, Botín DM, de Dompablo E, de Arriba P, Montiel FA, Negrete FM. Post-herpes neurotrophic keratopathy: aetiopathogenesis, clinical signs and current therapies. Archivos de la Sociedad Española de Oftalmología. 2019;94(4):171–183. doi:10.1016/j.oftal.2019.01.002
3. Saad S, Abdelmassih Y, Saad R, et al. Neurotrophic keratitis: frequency, etiologies, clinical management and outcomes. Ocular Surf. 2020;18(2):231–236. doi:10.1016/j.jtos.2019.11.008
4. Roth M, Dierse S, Alder J, Holtmann C, Geerling G. Incidence, prevalence, and outcome of moderate to severe neurotrophic keratopathy in a German tertiary referral center from 2013 to 2017. Graefes Arch Clin Exp Ophthalmol. 2022;260(6):1961–1973. doi:10.1007/s00417-021-05535-z
5. NaPier E, Camacho M, McDevitt TF, Sweeney AR. Neurotrophic keratopathy: current challenges and future prospects. Annals of Medicine. 2022;54(1):666–673. doi:10.1080/07853890.2022.2045035
6. Sacchetti M, Lambiase A. Diagnosis and management of neurotrophic keratitis. Clin Ophthalmol. 2014;8:571–579. doi:10.2147/OPTH.S45921
7. Lee YC, Kim SY. Treatment of neurotrophic keratopathy with nicergoline. Cornea. 2015;34(3):303–307. doi:10.1097/ICO.0000000000000348
8. Alakloby OM, AlJabre SH, Randhawa MA, Alzahrani AJ, AlWunais KM, Bukhari IA. Herpes zoster in eastern Saudi Arabia: clinical presentation and management. J Drugs Dermatol. 2008;7(5):457–462.
9. James C, Harfouche M, Welton NJ, et al. Herpes simplex virus: global infection prevalence and incidence estimates, 2016. Bull World Health Organ. 2020;98(5):315–329. doi:10.2471/BLT.19.237149
10. Aziz AA. Herpes zoster in Al-Baha region (Saudi Arabia): clinical presentation and management. EC Emerg Med Crit Care. 2020;4:01–06.
11. Al-Yousuf N, Alsetri H, Farid E, George SM. Amniotic membrane transplantation an experience of a locally prepared tissue. Transpl Res Risk Man. 2022;14:7–19. doi:10.2147/TRRM.S336917
12. World Health Organization. International statistical classification of diseases and related health problems 10th revision. ICD-10 Version: 2019. 2019.
13. Bonini S, Lambiase A, Rama P, et al. Phase II randomized, double-masked, vehicle-controlled trial of recombinant human nerve growth factor for neurotrophic keratitis. Ophthalmology. 2018;125(9):1332–1343. doi:10.1016/j.ophtha.2018.02.022
14. Dean AG, Sullivan KM, Soe MM. OpenEpi: open source epidemiologic statistics for public health, version. 2013. Available from: www.OpenEpi.com.
15. Crabtree JR, Tannir S, Tran K, Boente CS, Ali A, Borschel GH. Corneal nerve assessment by aesthesiometry: history, advancements, and future directions. Vision. 2024;8(2):34. doi:10.3390/vision8020034
16. Yang AY, Chow J, Liu J. Corneal innervation and sensation: the eye and beyond. Yale J Biol Med. 2018;91(1):13–21.
17. Versura P, Giannaccare G, Pellegrini M, Sebastiani S, Campos EC. Neurotrophic keratitis: current challenges and future prospects. Eye and Brain. 2018;10:37–45. doi:10.2147/EB.S117261
18. Dana R, Farid M, Gupta PK, et al. Expert consensus on the identification, diagnosis, and treatment of neurotrophic keratopathy. BMC Ophthalmol. 2021;21(1):327. doi:10.1186/s12886-021-02092-1
19. Bian Y, Ma KK, Hall NE, et al. Neurotrophic keratopathy in the United States: an intelligent research in sight registry analysis. Ophthalmology. 2022;129(11):1255–1262. doi:10.1016/j.ophtha.2022.06.019
20. Choi CJ, Liu L, Qian Y, Herrinton LJ. Neurotrophic keratopathy: clinical presentation and outcomes in 354 eyes in a community-based population. Eur J Ophthalmol. 2024;34(4):1085–1094. doi:10.1177/11206721231222949
21. Belmonte C, Giraldez F. Responses of cat corneal sensory receptors to mechanical and thermal stimulation. J Physiol. 1981;321:355–368. doi:10.1113/jphysiol.1981.sp013989
22. Abazari A, Abbouda A, Cruzat A, Cavalcanti B, Pavan-Langston D, Hamrah P. Corneal reinnervation in patients with severe neurotrophic keratopathy secondary to herpes zoster ophthalmicus after treatment with autologous serum tear drops. Cornea Open. 2024;3(1):e0029. doi:10.1097/coa.0000000000000029
23. Guerrero-Moreno A, Baudouin C, Melik Parsadaniantz S, Réaux-Le Goazigo A. Morphological and functional changes of corneal nerves and their contribution to peripheral and central sensory abnormalities. Front Cell Neurosci. 2020;14:610342. doi:10.3389/fncel.2020.610342
24. Semeraro F, Forbice E, Romano V, et al. Neurotrophic keratitis. Ophthalmologica. 2014;231(4):191–197. doi:10.1159/000354380
25. Eguchi H, Hiura A, Nakagawa H, Kusaka S, Shimomura Y. Corneal nerve fiber structure, its role in corneal function, and its changes in corneal diseases. Biomed Res Int. 2017;2017(1):3242649. doi:10.1155/2017/3242649
26. Rogov AG, Goleva TN, Sukhanova EI, et al. Mitochondrial dysfunctions may be one of the major causative factors underlying detrimental effects of benzalkonium chloride. Oxid Med Cell Longev. 2020;2020(14):8956504. doi:10.1155/2020/8956504
27. Vazirani J, Sridhar U, Gokhale N, Doddigarla VR, Sharma S, Basu S. Autologous serum eye drops in dry eye disease: preferred practice pattern guidelines. Indian J Ophthalmol. 2023;71(4):1357–1363. doi:10.4103/IJO.IJO_2756_22
28. Quinto GG, Campos M, Behrens A. Autologous serum for ocular surface diseases. Arg Bras Oftalmol. 2008;71(6 Suppl):47–54.
29. Trinh T, Santaella G, Mimouni M, et al. Assessment of response to multimodal management of neurotrophic corneal disease. Ocul Surf. 2021;19:330–335. doi:10.1016/j.jtos.2020.11.003
30. Roumeau S, Dutheil F, Sapin V, et al. Efficacy of treatments for neurotrophic keratopathy: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2022;260(8):2623–2637. doi:10.1007/s00417-022-05602-z
31. Saad S, Labani S, Goemaere I, et al. Corneal neurotization in the management of neurotrophic keratopathy: a review of the literature. J Fr Ophtalmol. 2023;46(1):83–96. doi:10.1016/j.jfo.2022.09.007
32. Crabtree JR, Mulenga C, Tran K, et al. Corneal neurotization: essentials for the facial paralysis surgeon. Facial Plast Surg. 2024;40(4):424–432. doi:10.1055/a-2272-6077
33. Serra PL, Giannaccare G, Cuccu A, et al. Insights on the choice and preparation of the donor nerve in corneal neurotization for neurotrophic keratopathy: a narrative review. J Clin Med. 2024;13(8):2268. doi:10.3390/jcm13082268
34. Aujla J, Tong JY, Curragh D, et al. Corneal neurotization for neurotrophic keratopathy: a multicentre experience. Ophthalmic Plastic Reconstructive Surg. 2024;11:10–97.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.