Back to Journals » International Medical Case Reports Journal » Volume 19
Primary Squamous Cell Carcinoma of the Kidney Associated with Multiple Staghorn Calculi: A Case Report
Authors Marofi M ![]() , Kamal MI, Sediqi M, Bawarzai A
, Kamal MI, Sediqi M, Bawarzai A ![]() , Sarwary MF
, Sarwary MF ![]() , Modabber MH
, Modabber MH
Received 16 April 2026
Accepted for publication 27 June 2026
Published 3 July 2026 Volume 2026:19 617572
DOI https://doi.org/10.2147/IMCRJ.S617572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Maiwand Marofi 1,*, Mohammad Ibrahim Kamal2,3,*, Mahbobullah Sediqi1, Amjadzia Bawarzai 1, Mohammad Fahim Sarwary 1, Mohammad Hussain Modabber1
1Faculty of Medicine, Kabul University of Medical Sciences “Abu Ali Ibn Sina”, Kabul, Afghanistan; 2Department of Pathology, Ali Abad Teaching Hospital, Kabul, Afghanistan; 3Department of Pathology, Kabul Medical University of Medical Sciences “Abu Ali Ibn Sina”, Kabul, Afghanistan
*These authors contributed equally to this work
Correspondence: Maiwand Marofi, Faculty of Medicine, Kabul University of Medical Sciences “Abu Ali Ibn Sina”, Kabul, Afghanistan, Tel +93702545702, Email [email protected]
Background: Primary squamous cell carcinoma (SCC) of the kidney is an extremely rare malignancy, usually originating from the renal pelvis due to continuous irritation from infections and nephrolithiasis. However, it can also arise from parenchyma. It has rarely been reported in the literature. Renal squamous cell carcinoma often presents late with nonspecific symptoms such as flank pain and hematuria. It is typically linked to kidney stones, and because of its nonspecific clinical symptoms and radiological characteristics, patients often seek medical attention only in the advanced stages of the disease. This kidney neoplasm is aggressive in nature and usually has a poor prognosis. Most patients present with an advanced stage of the disease, and it has an unfavorable outcome. In this report, we cover a case of primary squamous cell carcinoma with staghorn kidney stones in a 70-year-old patient.
Case Presentation: The present case is a 70-year-old man who presented to the Emergency Department of Ali Abad Teaching Hospital, Kabul, with complaints of flank pain and anorexia. The hospital performed laboratory, ultrasound, and histopathological examinations. Ultrasound showed an enlarged kidney with several staghorn stones, and pus was noted in the renal collecting system. The patient underwent laparotomous radical nephrectomy due to suspicion of renal cell carcinoma. Histopathological examinations showed evidence of keratin pearl formation, stromal invasion, and areas of necrosis, supporting the diagnosis of renal squamous cell carcinoma. No clinically apparent primary tumor was identified outside the kidney. The patient was then referred to the oncology department. Despite appropriate medical therapy, the patient died after 2 months of follow-up.
Conclusion: Primary squamous cell carcinoma of the kidney is a rare and highly aggressive malignancy strongly associated with chronic nephrolithiasis. Early detection remains challenging due to nonspecific clinical and radiological features. Clinicians should consider the possibility of renal squamous cell carcinoma in patients presenting with renal masses, nephrolithiasis, and flank pain. Also, this malignancy should remain a differential diagnosis of xanthogranulomatous pyelonephritis in patients with persistent kidney stone disease. It is often diagnosed postoperatively after nephrectomy.
Keywords: kidney neoplasm, squamous cell carcinoma, nephrolithiasis, staghorn calculi
Introduction
Squamous cell carcinoma of the kidney is a rare renal tumor that is often associated with renal stones.1 About 4–5% of malignant tumors occur in the kidney, of which approximately 85–94% are carcinomas (adenocarcinoma, clear cell adenocarcinoma) except for primary squamous cell carcinoma, which is usually seen with kidney stones. Squamous cell carcinoma can arise in many epithelial tissues, but it is extremely rare in the kidney.2,3 It accounts for less than 1% of kidney tumors, most of which are reported in the bladder and urethra in men.4 It is usually accompanied by squamous metaplasia due to chronic irritation, a history of nephrolithiasis, and/or recurrent urinary tract infections.4 Because the symptoms are usually vague and nonspecific, renal squamous cell carcinoma is commonly detected late.5,6 This neoplasm is often diagnosed at an advanced stage.7 Therefore, it has been associated with poor outcomes.8 The mean overall survival for patients with SCC is nearly 5 months.9 A retrospective study of 14 patients who underwent surgical treatment for renal cancers between 2015 and 2021 demonstrated that most patients with renal SCC were male (71.4%), and flank pain was the most common presenting symptom (78.6%).9 Due to uncommonness and unclear manifestation, squamous cell carcinoma of the kidney is often discovered incidentally during histopathological examination after nephrectomy. Although the primary renal SCC is a rare neoplasm, it should be considered in patients with long-standing nephrolithiasis and flank pain. We reported an incidentally detected case of primary SCC of the kidney associated with staghorn calculi.
Case Presentation
A 70-year-old man presented with nearly 4 months of flank pain. Associated symptoms included persistent abdominal discomfort and loss of appetite. Physical examination revealed right flank tenderness. Initial assessments included laboratory tests and ultrasound imaging. Routine laboratory investigations, including liver and kidney function tests, fasting blood sugar, HBsAg, and HCV, were within normal limits, except for an elevated ESR (35/70 mm/h). Additional findings included WBC: 8800/mm3 and Hb: 12.3 g/dL. Ultrasound imaging revealed an enlarged right kidney with multiple staghorn calculi, and pus was also noted in the renal collecting system. Based on these clinical and radiological findings, the differential diagnosis included renal cell carcinoma and xanthogranulomatous pyelonephritis. Therefore, the patient underwent laparotomous radical nephrectomy, and the excised specimen was sent to the laboratory for histopathological evaluation. Grossly, the kidney was markedly deformed with multiple staghorn stones in the renal pelvis (Figure 1). Microscopic examination showed keratin pearl formation, stromal invasion, areas of necrosis, and occasional mitotic figures (Figure 2). These findings confirmed the diagnosis of squamous cell carcinoma of the kidney. Due to resource limitations, CT and MRI imaging could not be performed, and a comprehensive staging evaluation could not be completed. The patient was then referred to the oncology department for postoperative treatment. At the 2-month follow-up, the patient was reported deceased.
 |
Figure 1 A biopsy specimen from the patient’s kidney. (A) Gross appearance of the resected radical nephrectomy demonstrates a deformed kidney, and a tumor mass that has spread to the renal pelvis is also seen. (B) Gross specimen of the same kidney, showing multiple staghorn calculi. |
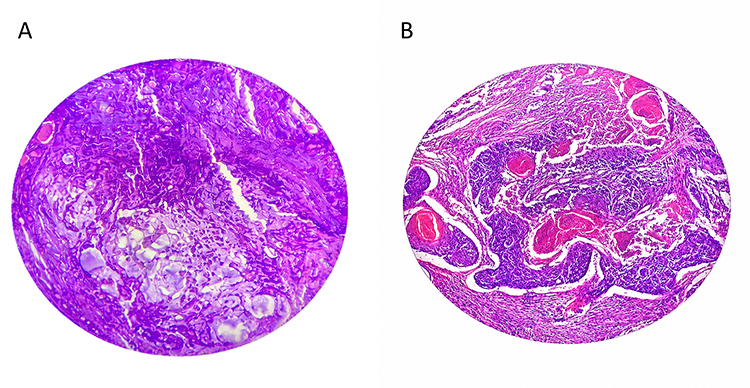 |
Figure 2 Histopathological findings of renal squamous cell carcinoma. (A) Microscopic examination demonstrating keratin pearl formation and malignant squamous differentiation. (B) Microscopic finding of the same lesion at a different field/magnification, showing atypical and dysplastic squamous cells, keratin pearl formation, stromal invasion, and areas of necrosis. |
Discussion
Squamous cell carcinoma of the kidney is one of the rarest malignant tumors of the urinary system,10 accounting for less than 1% of cases; it occurs most often in the bladder and urethra of men with a mean age of approximately 54 years. Studies have shown that kidney tumors are divided into two groups based on location: central and peripheral.11 In most cases, renal cell carcinomas occur in the central part of the kidney with metastasis to the surrounding lymph nodes. In contrast, peripheral zone carcinomas occur rarely. They are associated with involvement of the renal parenchymal tissue and invade the fat and muscle tissues surrounding the kidney before lymph node involvement and distant metastases. Based on radiologic and clinical findings, our patient had peripheral zone carcinoma.12 Although the etiology of this tumor is unknown, several factors are associated with its development, including genetic changes, phenacetin use, vitamin A deficiency, smoking (60% of cases), long-standing nephrolithiasis, chronic irritation, and infection.10 According to experts’ common belief, chronic kidney stones and inflammation cause persistent irritation, which subsequently results in squamous metaplasia and carcinogenesis.13 Clinical symptoms in these patients are nonspecific, and patients typically present with abdominal/flank pain, nausea, vomiting, and, in most cases, a history of kidney stones.10 Radiographic findings in these patients are not specific, as the clinical symptoms usually reveal the presence of kidney stones, hydronephrosis, and regional lymphadenopathy.14,15 Due to the nonspecific nature of clinical symptoms, the diagnosis is frequently delayed; therefore, the prognosis of this disease is poor. Also,16 Xanthogranulomatous pyelonephritis should be considered a differential diagnosis in patients presenting with renal masses and flank pain, particularly in the setting of chronic nephrolithiasis and persistent obstruction of the urinary tract. Similar to previous reports, our patient presented with vague symptoms like flank pain and anorexia, which delayed early diagnosis.8 Definitive diagnosis is established by microscopic confirmation.17 Currently, the most appropriate treatment for these patients is nephrectomy.5,6 Usually, patients with renal SCC present at an advanced stage of this aggressive cancer. Our patient lost his life within two months after radical nephrectomy.
This case highlights the importance of considering the probability of renal squamous cell carcinoma in elderly patients with kidney stones and abdominal/flank pain. In addition, it underscores the diagnostic challenge of differentiating renal squamous cell carcinoma from chronic inflammatory renal diseases, such as xanthogranulomatous pyelonephritis, in patients with long-standing kidney stones.
Data Sharing Statement
Manuscript has no associated data.
Ethics Approval and Consent to Participate
Ethical approval was not required for this case report in accordance with institutional guidelines. Written informed consent was obtained from the patient’s family for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Makhlough A, Fouladi B, Shekarriz R, Akha O, Abedi S. Primary renal squamous cell carcinoma with staghorn stone. J Mazandaran Univ Med Sci. 2013;22(1):285–4.
2. Yousof A, Aldhilan A, Alamer A, Fahad A. Renal squamous cell carcinoma presented with bone metastasis and coexistence with xanthogranulomatous pyelonephritis: a case report. Urol Case Rep. 2014;2(2):35–37. doi:10.1016/j.eucr.2013.12.009
3. Singh V, Sinha RJ, Sankhwar SN, Mehrotra B, Ahmed N, Mehrotra S. Squamous cell carcinoma of the kidney—rarity redefined: case series with review of literature. J Cancer Sci Ther. 2010;2(4):55–56. doi:10.4172/1948-5956.1000028
4. Junejo NN, Kamal MH, Aquil S, Al Rahbi F, Al Badaai GAR, Siddiqui KM. Primary squamous cell carcinoma of the kidney: a case series. Oman Med J. 2025;40(1):e721. PMID: 40357431; PMCID: PMC12066939. doi:10.5001/omj.2025.04
5. Lina J, br KRM, Theresia Y, Fadillah Q. Squamous cell carcinoma of the kidney: a case report. BKKP. 2025;4(1):30–33.
6. Patel AM, Patel J, Jansari T, Thorat R. Incidentally detected primary squamous cell carcinoma of the kidney: case series with review of the literature. J Cancer Res Ther. 2023;19(Suppl 2):S928–S931. PMID: 38384082. doi:10.4103/jcrt.jcrt_1013_22
7. Sahoo TK, Das SK, Mishra C, et al. Squamous cell carcinoma of the kidney and its prognosis: a case report and review of the literature. Case Rep Urol. 2015;2015:469327. doi:10.1155/2015/469327
8. Variar P, Misra A, Siraj F. Primary squamous cell carcinoma of the renal pelvis: a case report series. Cureus. 2024;16(5):e60568. 60568. PMID: 38894774; PMCID: PMC11184534. doi:10.7759/cureus
9. Shah SAS, Mahar NA, Qureshi HH, et al. Squamous cell carcinoma of the kidney: a large case series. Oncology. 2023;37(6):246–249. PMID: 37343206. doi:10.46883/2023.25920997
10. Ghosh P, Saha K. Primary intraparenchymal squamous cell carcinoma of the kidney: a rare and unique entity. Case Rep Pathol. 2014;2014:256813. doi:10.1155/2014/256813
11. Lee TY, Ko SF, Wan YL, et al. Renal squamous cell carcinoma: CT findings and clinical significance. Abdom Imaging. 1998;23:203–208. doi:10.1007/s002619900324
12. Li MK, Cheung WL. Squamous cell carcinoma of the kidney. J Urol. 1987;138:269–271. doi:10.1016/S0022-5347(17)43116-8
13. Xiao J, Tan J, He L, Yin G. Renal calculus complicated with squamous cell carcinoma of renal pelvis: report of two cases. Can Urol Assoc J. 2015;9(5–6):E310–E312. doi:10.5489/cuaj.2441
14. Jain A, Mittal D, Jindal A, et al. Incidentally detected squamous cell carcinoma of renal pelvis in patients with staghorn calculi: case series with review of the literature. ISRN Urol. 2011;2011:620574.
15. Samanta DR, Chaitali B, Sasmita P, Ashis U, Abhijit D, Senapati SN. Primary squamous cell carcinoma of the kidney: report of two cases. Int J Med Res Health Sci. 2015;4(4):916–918.
16. Daoud N, Ismaiel N, Bashour G, Nammour A, Barri A, Alshehabi Z. Xanthogranulomatous pyelonephritis mimicking renal cell carcinoma: a case report. Ann Med Surg. 2023;85(4):1254–1257. PMID: 37113900; PMCID: PMC10129102. doi:10.1097/MS9.0000000000000474
17. Zheng ZH, Shao B, Xu CM, et al. Primary parenchymal squamous cell carcinoma of the kidney: a case report. World J Clin Cases. 2025;13(4):100037. PMID: 39917575; PMCID: PMC11586791. doi:10.12998/wjcc.v13.i4.100037
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.