Back to Journals » International Medical Case Reports Journal » Volume 18
Primary Psoas Muscle Multiple Hydatid Cysts, Presenting as a Psoas Abscess: A Rare Case Report
Authors Nazari FA, Baset GY ![]() , Frahmand F, Ahmadi MA, Rafat A, Amini J
, Frahmand F, Ahmadi MA, Rafat A, Amini J ![]()
Received 24 June 2025
Accepted for publication 29 November 2025
Published 11 December 2025 Volume 2025:18 Pages 1599—1604
DOI https://doi.org/10.2147/IMCRJ.S549343
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Fareed Ahmad Nazari,1 Ghulam Yahia Baset,1 Fraidon Frahmand,2 Mirza Ali Ahmadi,3 Asmatullah Rafat,3 Jawad Amini3
1Department of Emergency Surgery and Trauma, Kabul University of Medical Science, Ali Abad University Hospital, Kabul, Afghanistan; 2Maternal and Child Health Department, Kabul University of Medical Science, Kabul, Afghanistan; 3Department of Abdominal Surgery, Kabul University of Medical Science, Ali Abad University Hospital, Kabul, Afghanistan
Correspondence: Ghulam Yahia Baset, Email [email protected]
Abstract: Hydatid disease is an anthropozoonosis, caused by the larval stage of parasitic tapeworm Echinococcus granulosus. Every organ of the human body can be affected by the Echinococcus granulosus but mostly the liver is involved. Hydatid disease of the muscles is not common, and the involvement of the psoas muscle is very rare. This is a case of a 45-year-old male presented to the emergency department with left flank pain, fever and left leg weakness since 6 months. A total of three hydatid cysts were found in the psoas muscle, extending to the left iliac fossa across the psoas muscle.
Keywords: hydatid disease, psoas muscle, anthropozoonosis, Echinococcus granulosus
Introduction
Hydatid disease, is an anthropozoonosis caused by the larval stage of parasitic tapeworm Echinococcus. Among the known species of Echinococcus, E. granulosus is the most prevalent and is mainly responsible for echinococcosis.1 Hydatidosis has the ability to infect different organs of the human body. The liver is the most commonly affected organ (50–70%), followed by the lungs (20–30%). Hydatid disease of the muscle tissues is uncommon, and its occurrence in the psoas muscle, especially development of multiple cysts, is very rare and exceptional even in endemic regions, representing only 1–3% of cases.2 The rarity of muscular hydatid cyst, including the psoas muscle hydatid cyst, can be explained by the difficulty of developing the parasitic larvae due to lactic acid production as a result of muscle contractions during activities, which makes an inadequate condition for embryophore development.3 Psoas muscle hydatid cyst can have several complications including peritoneal fistula formation, infection, hydronephrosis and compression of neighboring structures with dangerous consequences, like an anaphylactic shock or peritoneal hydatidosis.3 The clinical presentation of psoas hydatid cyst, especially multiple cysts as in our case, can vary widely, making its diagnosis challenging.2 We present a 45-year-old male from a rural area with multiple primary hydatid cysts of the left psoas muscle presenting with left flank pain and left leg weakness, which was confused with psoas abscess.
Case Presentation
A 45-year-old male presented to the emergency department of Ali Abad University Hospital, Kabul University of Medical Sciences, with left flank pain, and fever since 6 months. The pain was dull in nature with no radiation. Fever was of low grade and intermittent. Physical examination revealed mild tenderness in left flank area on deep palpation during bimanual examination. There was no mass lesion. Vital signs were within normal limits.
Ultrasonography of the abdomen revealed a complex cystic collection in left flank area with septations measuring 4×6 cm in diameter suggestive of psoas abscess. MRI of the lumber spine revealed a complex lobulated cystic mass in the retroperitoneal region of the left flank measuring 7.5×6.8 cm in axial diameter and with regular borders extending to the left iliac fossa, suggestive of psoas abscess (Figure 1).
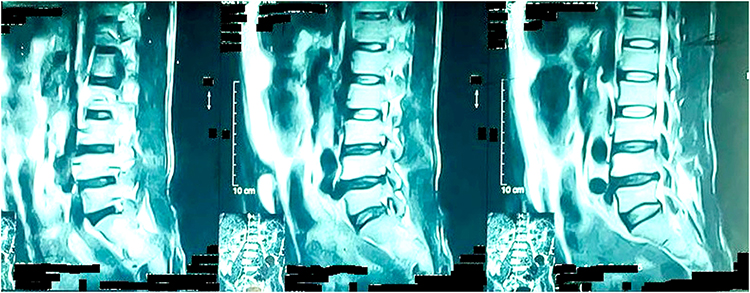 |
Figure 1 MRI (magnetic resonance imaging) of lumber. |
The patient was planned as an emergency case for drainage of the abscess. Under General anesthesia, an oblique incision was made in left flank in order to provide access to the retroperitoneum and to the psoas muscle. The psoas muscle was exposed and needle puncture was performed to aspirate puss for localization of the abscess but surprisingly a clear fluid was aspirated instead of puss (Figure 2). An incision was made on the area, and daughter cysts, laminated membrane and hydatid fluid were found (Figure 3). After evacuation of all daughter cysts, hydatid fluid and laminated membrane, it was found that two other hydatid cysts were also present underneath with separate laminated membranes which contained their own daughter cysts and hydatid fluid; a total of 3 hydatid cysts were there which were extended to the left iliac fossa across the psoas muscle (Figure 4). All 3 hydatid cysts were completely drained carefully without spillage of the fluid, their contents were sent for histopathology, the remaining cavities were washed with hypertonic saline solution and a drain tube was inserted inside the cavity.
 |
Figure 2 Black arrow shows the hydatid cyst and white arrow shows the psoas muscle. |
 |
Figure 3 Daughter cysts in the cavity of the hydatid cyst. |
 |
Figure 4 Evacuated laminated membrane and daughter cysts. |
On the second post-operative day, liquid diet was started and Albendazole tablet 400 mg twice daily was also prescribed which thereafter continued for 21 days.
The histopathology report was compatible with our findings and confirmed the hydatid cyst. The patient was followed-up for 7 months with no complication or recurrence of the disease.
Discussion
Hydatid disease is a public health problem in endemic areas such as Mediterranean countries, the Middle East, New Zealand, India, South America, and Afghanistan; it is an emerging public health problem in the western world because of migration.3 The muscular hydatid cyst is uncommon. Its location in the Psoas muscle is even rarer and reported in less than 0.5% of cases.3 The disease occurs equally in males and females being more prevalent around the 4th to 5th decade of life.4
The cause of Hydatid disease is a parasitic tapeworm, Echinococcus granulosus most of the time, and Echinococcus alveolaris in some cases. The tapeworm lives in canids, which are infected by eating the viscera of sheep that contain hydatid cysts. Scolices, in the cysts, adhere to the small intestine of dogs and become adult taenia, which attach to the intestinal wall. Each worm sheds approximately 500 ova into the bowel. The grasses and farmlands are contaminated by dog feces containing ova of the tapeworm, then the ova are ingested by intermediate hosts such as sheep, cattle, pigs and humans . The ova have hard coverings that are dissolved by acid in the stomach. The released ovum then penetrates the intestinal mucosa and is carried by portal vein to the liver, where it develops into an adult cyst. Most ova are entrapped in the hepatic sinusoids, therefore 70% of hydatid cysts form in the liver. A few ova pass through the liver and are entrapped in the pulmonary capillary bed or enter the systemic circulation, forming cysts in the lung, spleen, brain, or bones. Primary cyst may localize anywhere in the body. They are commonly found in liver (55–77%) and lungs (20–30%), but cysts may be localized in the spleen or kidneys (2%), brain (1.5%), bone (1%), and heart (less than 1%). Location in the muscular tissue accounts for 2–3% of cases.5
The rarity of psoas muscle hydatid cyst can be explained by the muscle generally being very resistant to echinococcosis due to it having partitions that encapsulate the larva as well as the contractile activity of muscles and the production of lactic acid in muscles which can destroy the larva.6 Psoas muscle involvement is often primary and occurs via arterial infusion, rarely secondary to an adjacent organ’s complicated hydatid cyst.3
Psoas muscle hydatid cyst is asymptomatic most of the time. It produces symptoms only when secondary changes occur among which secondary infection is most common. Rupture of the cyst can lead to spreading of daughter cysts or may lead to anaphylactic reaction. Compressive signs and symptoms may be present.4
Diagnosis is made according to the history, physical examination, radiologic examinations, and serologic tests. Ultrasonography is the first-line examination with diagnostic reliability estimated at 96%. The ultrasound appearance reproduces the stages of Gharbi’s classification and reflects the evolutionary stage of the disease.5
CT-scan of the abdomen is more accurate in identifying hydatid cyst of the psoas muscle.5 MRI is the most reliable diagnostic modality which typically shows a multivesicular cyst with daughter cysts. Histopathology is essential for final postoperative confirmation of the disease.7 Serologic tests may be helpful in diagnosis of psoas muscle hydatid cyst. Eosinophilia is present in 20–50% of cases of hydatid cyst. This is especially enhanced in case of cracking of the cyst. Sero-immunological reactions enhance the diagnosis. Indirect hemagglutination test is the most sensitive reaction with sensitivity up to 70%.5
Differential diagnoses of psoas muscle hydatid cyst include a wide range of neoplastic and non-neoplastic diseases, like soft tissue tumors, abscesses, and hematomas.7
Complications of hydatid cyst of psoas muscle include peritoneal fistula, infection, hydronephrosis and compression of neighboring structures. These complications may be associated with serious consequences, such as anaphylactic shock or peritoneal hydatidosis.8
Treatment of Hydatid cyst mainly include percutaneous drainage of the cyst known as PAIR (Puncture, Aspiration of cyst content, Injection of scolicidal agent and Re-aspiration), pericystectomy, enucleation, marsupialisation, drainage of cyst, omentoplasty; among which the last two can be done for intra-abdominal Hydatid cyst only.4
Currently, PAIR is the preferred method of treatment for anatomically and surgically appropriate hydatid cyst including psoas muscle hydatid cyst. Efficacy of PAIR in treatment of Hydatid cyst is more than 75%.4
Surgery is standard in the treatment of hydatid cyst of the psoas, which can be via open or laparoscopic approach. The open approach can be extraperitoneal through a lumbar incision or transperitoneal through a median laparotomy incision. Radical treatment of psoas muscle hydatid cyst is total pericystectomy if possible. Adhesions of the cyst to the vascular and nervous elements, as well as vertebral involvement may make pericystectomy difficult or even dangerous. In such cases, resection of the prominent dome of the cyst along with lavage and drainage of the cyst cavity may be sufficient.9
Another method of the therapy of hydatid cyst is chemotherapy with Albendazole or Mebendazole which is effective at shrinking the cyst. However, disappearance of the cyst with chemotherapy is seen in fewer than 50% of cases. Pre-operative chemotherapy may decrease the risk of spillage of hydatid fluid and daughter cysts during the operation and is a safe practice.4
If the hydatid cyst is untreated, it usually follows three courses: 1) The parasite dies, the fluid is absorbed, the cyst layers shrink, and new tissue forms, 2) super-infection occurs, and serious symptoms that can result in death can be seen due to invasion of the cyst wall into adjacent structures, or 3) death occurs following rupture of the cyst. Spontaneous healing is rarely seen.10 Hydatid cyst, including hydatid cyst of the psoas muscle recurrence rates is approximately 10%.7
Conclusion
Hydatid disease of the muscles is uncommon, and its occurrence in the psoas muscle, especially development of multiple cysts, is considered very rare and exceptional even in endemic regions. It should be considered in differential diagnosis of all cystic masses of psoas muscle. Currently, PAIR is the preferred method of treatment for anatomically and surgically appropriate hydatid cyst including psoas muscle hydatid cyst.
Ethical Approval
This report does not contain any personal information that could lead to the identification of the patient. Therefore, it is exempt from ethical approval of our institution.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Acknowledgment
The authors would like to express their sincere gratitude to the patient’s guardians for providing consent to include the case details and photographs in this publication.
Funding
The authors declare that his work is not funded by any institution, organ, or government and he has no financial support.
Disclosure
The authors have no potential conflicts of interest to disclose.
References
1. Ciobotaru OC, Duca O-M, Ciobotaru OR, et al. Hydatid cysts of the psoas muscle: insights from the past five years. Life. 2024;14(10):1331. doi:10.3390/life14101331
2. Arab H, Alsaffaf Y, Kattan O, Khallouf S. Two hydatid cysts in the psoas muscle of a 40-year-old female: a rare case report. Int J Surg Case Rep. 2024;121:109985. doi:10.1016/j.ijscr.2024.109985
3. Chaouch MA, Faidi B, Hdira M, et al. A case report of primary multiple hydatid cysts of psoas muscle: an exceptional location. IDCases. 2022;30:e01637. doi:10.1016/j.idcr.2022.e01637
4. Galani K, Trivedi B, Vaghela J. A rare case presentation of hydatid cyst in ilio-psoas muscle. Int J Res Med Sci. 2018;6(9):3182–3185. doi:10.18203/2320-6012.ijrms20183667
5. Chincholkar RG, Tongale RV. Primary hydatidosis of psoas muscle: rare entity. Inter Surg J. 2022;9(5):1110–1113. doi:10.18203/2349-2902.isj20221168
6. Dabbagh M. Hydatid cyst of the psoas: a report of 3 cases. Asian J Case Rep Surg. 2023;6(2):421–427.
7. Barchid A, Laiz A, Yasough I, et al. Hydatid disease with psoas and gluteal muscleinvolvement causing cauda equina compression: a case report. Cureus. 2024;16(11):e74029. doi:10.7759/cureus.74029
8. Gokce K, Dgan D, Ilhan FM, Midi A. Giant hydatid cyst originating from psoas muscle extending to the iliac bone, inguinal, and femoral canals: a case report and current literature review. Med Bull Haseki. 2023;61:379–383. doi:10.4274/haseki.galenos.2023.9518
9. Mhand M, Ramdani A, Khomssi N, et al. Hydatid cyst of the psoas: case report and review of literature. Ann Med Surg. 2023;85:453–455. doi:10.1097/MS9.0000000000000087
10. Duman K, Poyrazoglu Y. Atypical hydatid cyst with psoas muscle location: case report. Arch Clin Exp Surg. 2017;6(2):108–111. doi:10.5455/aces.20151012124555
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.