Back to Journals » Journal of Pain Research » Volume 12
Primary care patients’ use of conventional and complementary medicine for chronic low back pain
Authors Rodondi PY ![]() , Bill AS, Danon N
, Bill AS, Danon N ![]() , Dubois J
, Dubois J ![]() , Pasquier J
, Pasquier J ![]() , Matthey-de-l'Endroit F
, Matthey-de-l'Endroit F ![]() , Herzig L, Burnand B
, Herzig L, Burnand B ![]()
Received 9 January 2019
Accepted for publication 21 May 2019
Published 10 July 2019 Volume 2019:12 Pages 2101—2112
DOI https://doi.org/10.2147/JPR.S200375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Erica Wegrzyn
Pierre-Yves Rodondi,1,2 Anne-Sylvie Bill,1 Nadia Danon,3 Julie Dubois,1,2 Jérôme Pasquier,1 Florence Matthey-de-l’Endroit,1 Lilli Herzig,1 Bernard Burnand1
1Center for Primary Care and Public Health (Unisanté), University of Lausanne, Lausanne, Switzerland; 2Institute of Family Medicine, University of Fribourg, Fribourg, Switzerland; 3Pain Center and Center for integrative and complementary medicine, Department of Anesthesiology, Lausanne University Hospital and Faculty of Biology and Medicine, University of Lausanne, Lausanne, Switzerland
Purpose: To investigate among primary care patients and their physicians in western Switzerland the prevalence of use, perceived usefulness, and communication about common treatments for chronic or recurrent low back pain (crLBP) including complementary medicine (CM).
Patients and methods: A cross-sectional cluster observational study involving 499 crLBP patients visiting 45 primary care physicians (PCPs) was conducted from November 1, 2015, to May 31, 2016. Patients and primary care physicians completed questionnaires about lifetime use and usefulness of 30 crLBP therapies. We conducted multivariate analyses of factors associated with therapy use, including sociodemographic variables, pain duration, insurance coverage, and primary care physicians’ characteristics.
Results: The five most frequent modalities used at least once by patients were physiotherapy (81.8%), osteopathic treatment (63.4%), exercise therapy (53.4%), opioids (52.5%), and therapeutic massage (50.8%). For their PCPs, the five most useful therapies were physiotherapy, osteopathic treatment, yoga, meditation, and manual therapy. In multivariate analysis, the use of physiotherapy was significantly associated with longer pain duration; osteopathic treatment was associated with age under 75 years, female gender, higher education, and CM insurance coverage. Exercise therapy was associated with non-smoking and longer pain duration. Smokers were more likely and patients of PCPs with CM training were less likely to have used opioids. During their lifetime, 86.6% of the participants had used at least one CM therapy to manage their crLBP, with a mean of 3.3 (SD=2.9) therapies used per participant; 46.1% of participants reported that their PCP did not enquire about CM use. Among CM users, 64.7% informed their PCP about it.
Conclusion: Patients with crLBP use a variety of treatments, including self-prescribed and unreimbursed therapies, most frequently physiotherapy and osteopathy. The results suggest that PCPs should systematically discuss with their patients the treatments they tried to manage crLBP, including CM.
Keywords: chronic low back pain, lifetime use, treatments
Introduction
Low back pain (LBP) affects individuals of all ages and is considered to cause more years lived with disability than any other health condition worldwide.1,2 The contribution of LBP to disability is likely to increase in the context of the aging population.1 While the vast majority of LBP episodes resolve within 2–4 weeks, a third of patients will experience recurrent episodes within 1 year or chronic LBP, the prevalence of which is increasing.3–5 Unfortunately for this population, coping with back pain might be a lifetime challenge6 and these recurrent episodes and chronic cases are responsible for most of the health expenses related to LBP.7 In addition, the intensity of LBP can vary in individuals over time without any active treatment.
The number of therapies available to manage chronic or recurrent LBP (crLBP) is broad, ranging from surgery to pharmacotherapy and to non-pharmacological treatments.8,9 The effectiveness and safety of pharmacotherapy has, however, been challenged, including the use of acetaminophen, NSAIDs, anticonvulsants (eg, gabapentin, pregabalin), and opioids.10–14 On the other hand, evidence is emerging regarding the benefits of some non-pharmacological or complementary medicine (CM) treatments to improve crLBP outcomes. CM is defined as a group of diverse medical and health-care systems, practices, and products that are not generally considered part of conventional medicine.15
Indeed, recent studies have shown beneficial effects of yoga,16 acupuncture,17 osteopathic treatment,18 hypnosis,19 Taï chi,20 therapeutic massage,21 and exercise therapy22 for crLBP.
Given these recent findings, in 2017, the American College of Physicians shifted its guidelines for crLBP management by recommending as first-line options non-pharmacological therapies, including exercise (pain and function: small effect, moderate-quality evidence), acupuncture (pain and function: moderate effect, moderate-quality evidence), mindfulness-based stress reduction (pain and function: small effect, moderate-quality evidence), tai chi (pain: moderate effect, low-quality evidence; function: small effect, low-quality evidence) and yoga (pain and function: small to moderate effect, low-quality evidence), and recommending pharmacological treatment, like NSAIDs (pain: small effect, moderate-quality evidence; function: small effect, low-quality evidence) only following an inadequate response to first-line non-pharmacological interventions.23 However, this recommendation is based on moderate-quality evidence and most of the data on these therapies have only shown short-term effects.
CrLBP is a frequent reason for patients to seek physiotherapy, exercise therapy, and CM.24,25 In Switzerland, the lifetime prevalence of CM use for crLBP among patients consulting at a tertiary pain center was 77.3%,26 with osteopathic treatment, therapeutic massage, and acupuncture being the most frequently used therapies. Acupuncture, homeopathy, herbal medicine, hypnosis, Chinese herbs, and anthroposophic medicine are reimbursed by mandatory basic health insurance in Switzerland if provided by a physician. In addition, there are four main groups of manipulative therapies in Switzerland, provided by four different professions with specific training: manual medicine provided by trained physicians, chiropractic by chiropractors, physiotherapy by physiotherapists, and osteopathy by osteopaths. Manual therapy and chiropractic are reimbursed by mandatory basic health insurance, as well as physiotherapy if prescribed by a physician. Osteopathy and all other CM therapies require supplementary insurance in order to be covered (see Table 3, second column for insurance coverage).27 In 2012, about 60%28 of the Swiss population had supplementary health insurance for CM. Many different supplementary health insurance schemes are available in Switzerland, and the offer is heterogeneous across health insurance companies. Since CM that is not covered by basic health insurance does not require a medical prescription, access to most forms of CM is self-prescribed and consumption of CM services is not available in routine statistics. The concomitant use of CM and conventional medicine is frequent in Switzerland29 and in the US, especially for LBP.25,26 A recent meta-analysis revealed a 33% disclosure rate for biologically based CM.30 Reasons for non-disclosure often included the patients’ fear to be disapproved by their physician, or the fact that the physician did not ask. Reasons for disclosure often included the fact that the physician asked. The authors of this review concluded that disclosure of CM use to physicians should be encouraged to improve the safety and effectiveness of patient care. The disclosure rate of CM use for crLBP has been estimated at a Pain center (47%),26 but it is not known in private practice in Switzerland.
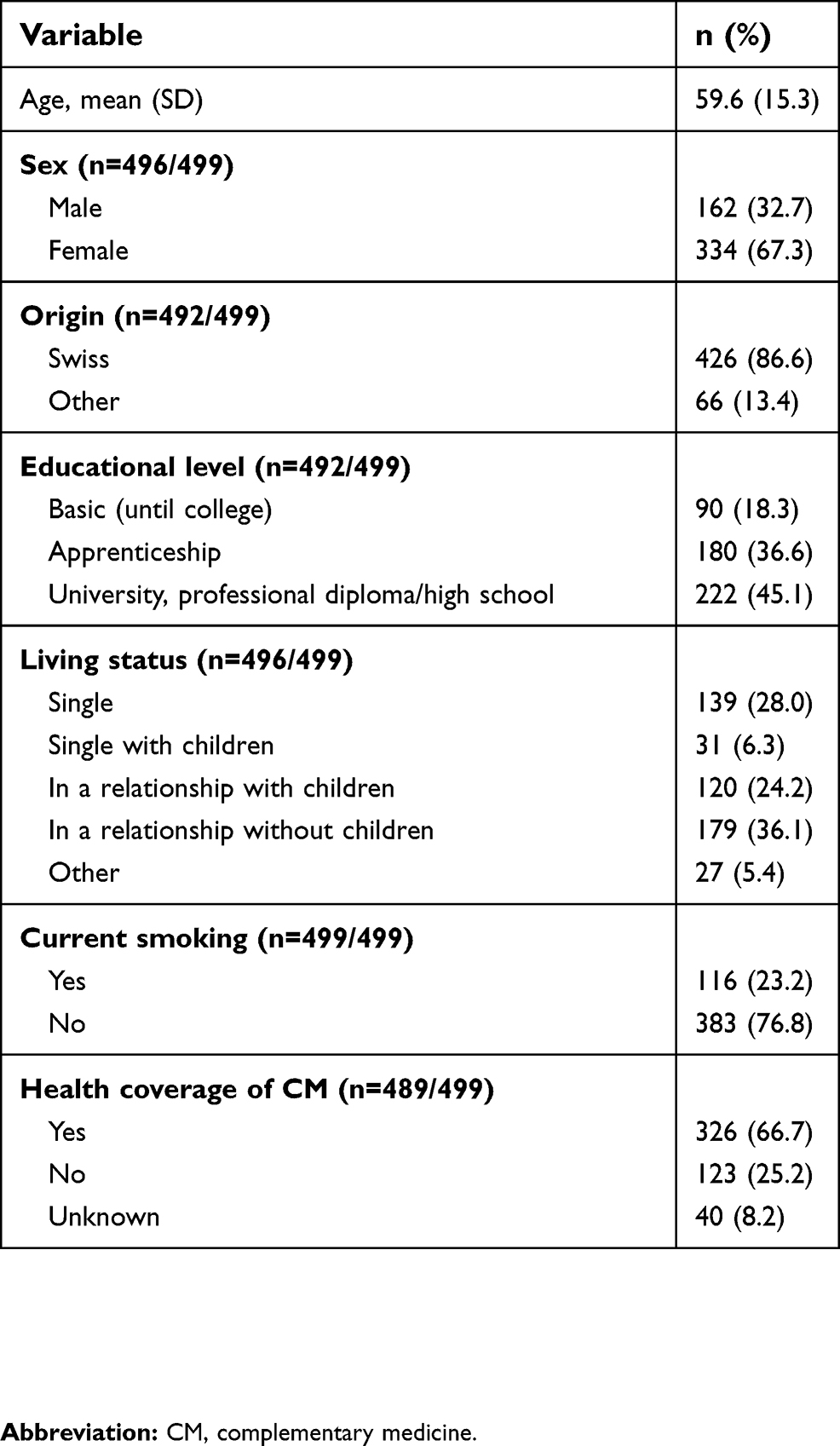 |
Table 1 Patients’ socio-demographic characteristics (N=499) |
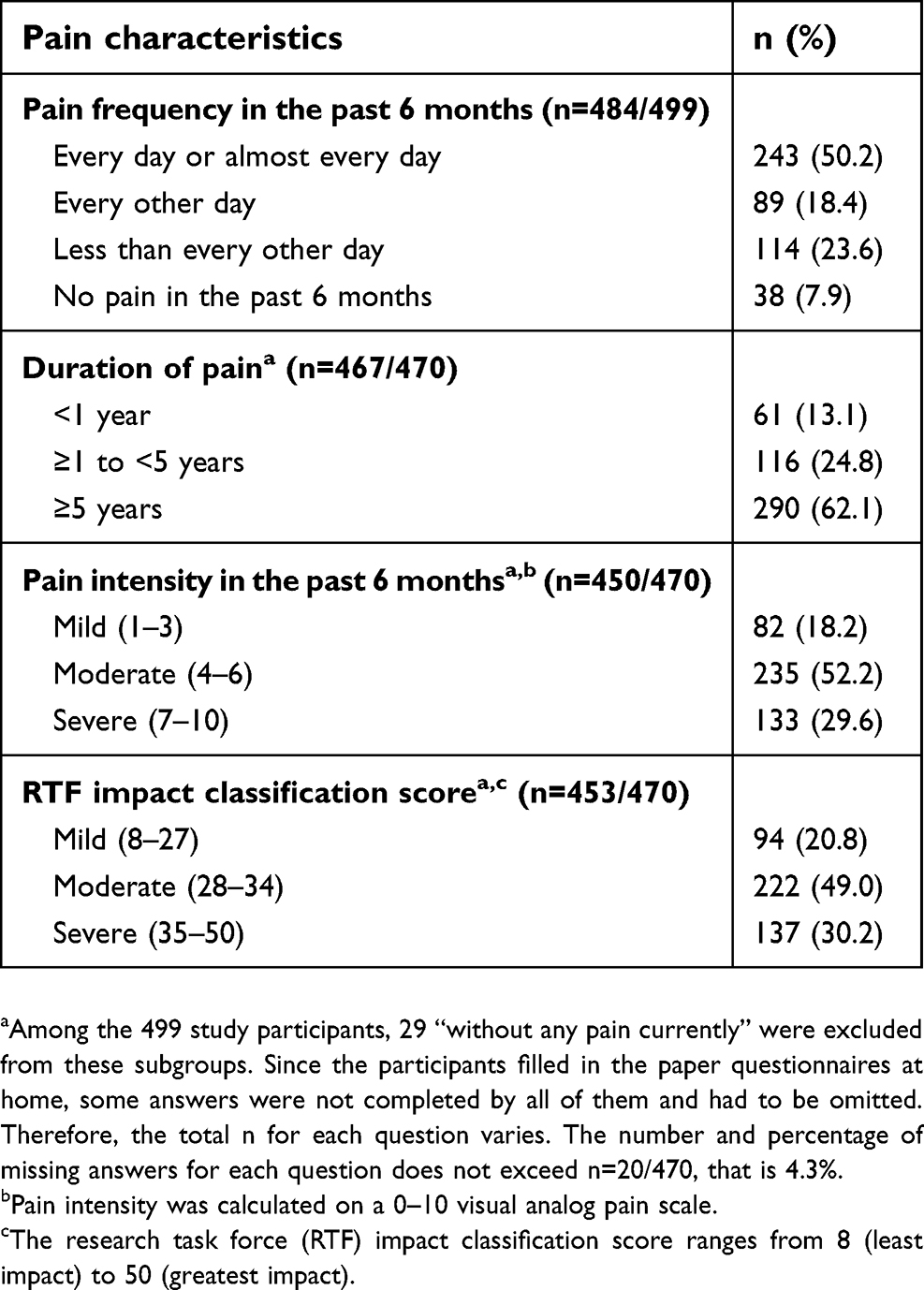 |
Table 2 Participants’ pain characteristics (N=499) |
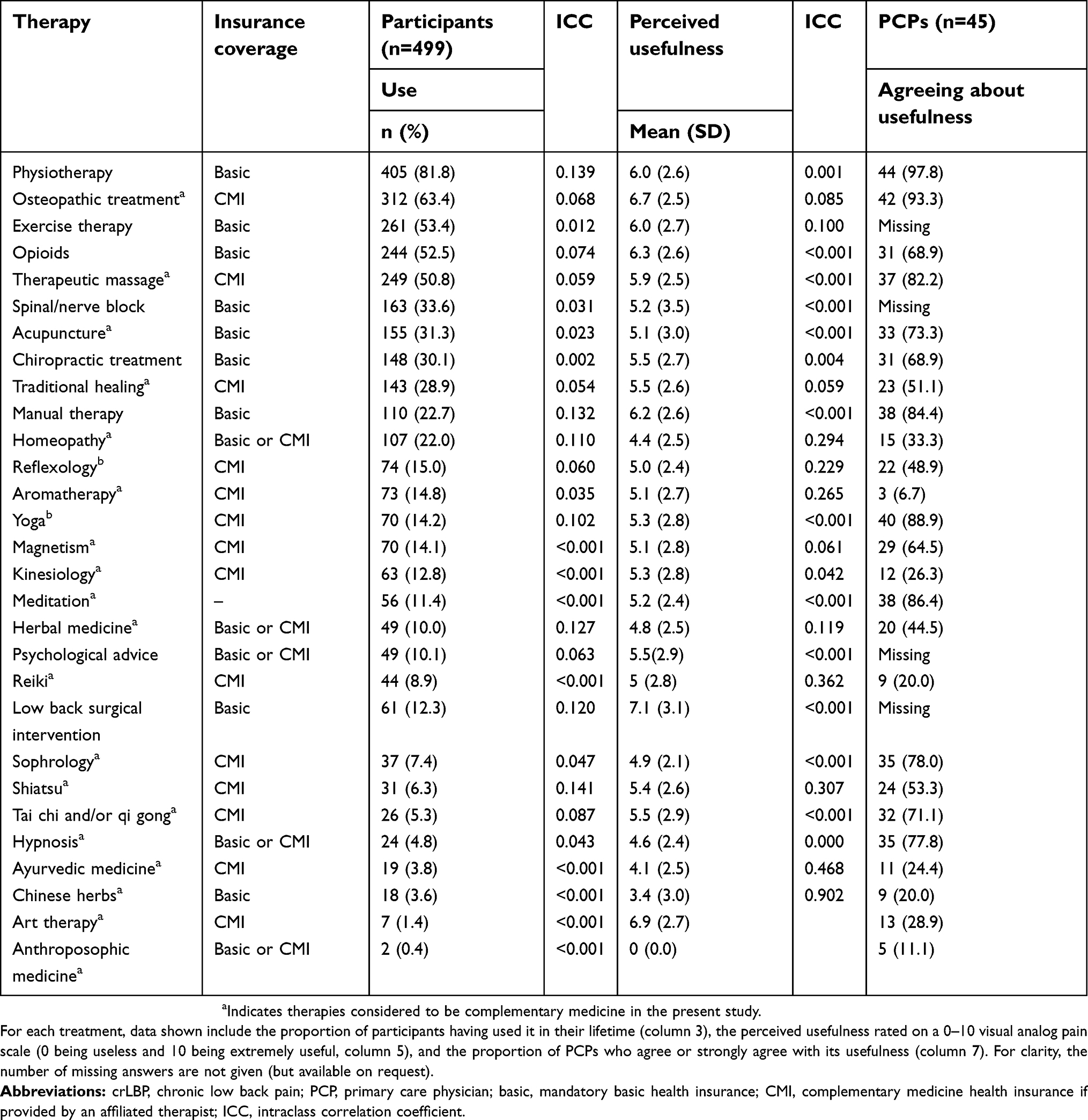 |
Table 3 Lifetime use of assessed therapies and their perceived usefulness in crLBP management (minimal number of responses for therapy, n=485) |
To the best of our knowledge, no population-based studies have specifically examined the use of a diversity of treatments for the management of crLBP in primary care. Thus, we aimed to provide insights into the use of a wide range of treatments for crLBP, including a detailed list of CM therapies, independently of whether they had been prescribed by a physician and the patient had been reimbursed. Our main objective was to assess the prevalence of use of the most common crLBP treatments by primary care patients and to describe perceived usefulness of both patients and their primary care physicians (PCPs) in western Switzerland. Furthermore, we explored associated variables with therapies used for crLBP. Our secondary objective was to describe PCP-patient communication about CM use for crLBP management.
Methods
Study design
This cross-sectional study was conducted in a series of primary care practices of the western French-speaking part of Switzerland from November 1, 2015, to May 31, 2016. PCPs recruited consecutive consenting patients with crLBP during regular medical visits (Figure 1).
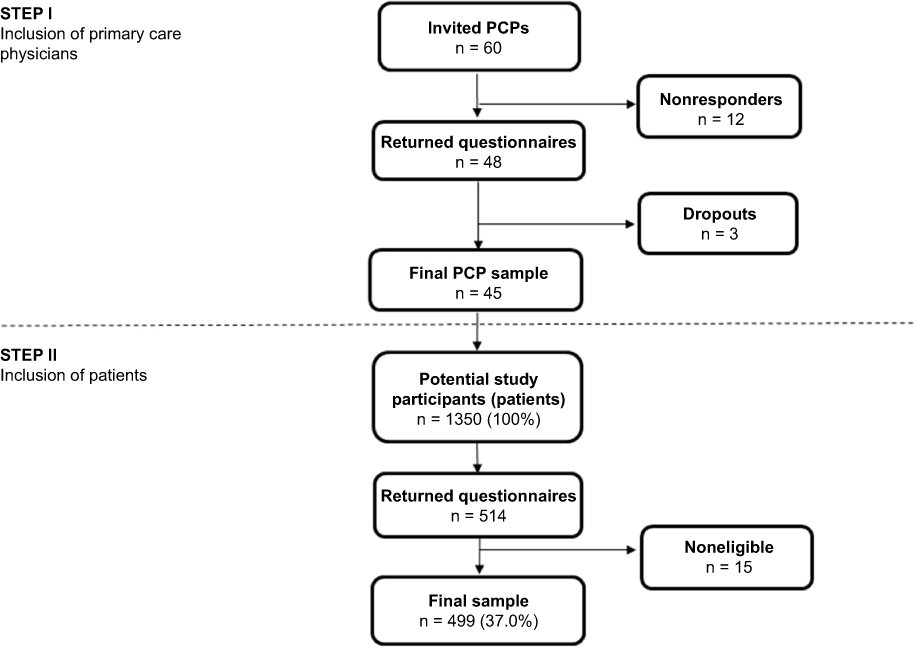 |
Figure 1 Flow chart of study participants.Abbreviation: PCP, primary care physicians. |
Setting and participants
PCPs were recruited from small or large practices in both urban and rural settings, in the different regions of the French part of Switzerland. The enrolled physicians completed and returned the paper questionnaire, which was an inclusion criterion for enrolling participants in the study. Eligible participants had crLBP, were 18 years of age or more, and were able to read and understand French. CrLBP was defined as pain lasting or recurring for 3 months or more31 and recurring LBP was defined as ≥2 episodes of LBP during the previous year, with a significant impact on the patient’s daily life.
During the study period, the PCP screened each visiting patient for the presence of crLBP, regardless of the reason for consultation, and handed out the questionnaire to 30 consecutive eligible patients. Patients were asked to complete the questionnaire at home and to return it in the prestamped envelope to the research team. Patients were entirely anonymous to the research team. Participation to the survey was voluntary. For each physician, the study ended after they had distributed 30 patient questionnaires or after 4 months following the recruitment of the first patient. As the questionnaires were anonymous, no informed consent had to be signed. By filling out the survey, participants gave implied consent. The study protocol and the questionnaires were approved by the committee on medical research ethics of the Canton of Vaud (ID Nb. 303/15).
Sample size calculation
For the sample size estimation, we relied on the 59% prevalence of CM use for cLBP according to US data.25 Given the cluster (physician) design of the study, we used an intracluster correlation of 0.03. In order to get a 5% width CI around the estimate, the number of patients needed amounted to 480.
Development of the questionnaire
The patient and the PCP questionnaires were based on previously published instruments.26,32,33 Questionnaires are provided in the supplementary material 1 and 2. Both questionnaires were cognitively tested. This test aimed to assess how respondents understood the intent and meaning of survey items and whether their answers agreed with the interpretations of the researchers. A convenience sample of 10 volunteer crLBP patients and 10 healthy volunteers from the general population with a wide range of sociodemographic features took part in the cognitive interviews. The 10 volunteer patients with crLBP did not take part in the study. Amendments were made to the questionnaire to improve comprehension of the survey items. We evaluated the stability of the questionnaire by means of a test–retest reliability procedure. Seven patients were asked if they would agree to provide their postal address in order to send them the same questionnaire 2 weeks after we had received their first-completed questionnaire. Although the seven patients completed the retest, the number of participants was too low to perform a concordance or reliability measurement by item. However, we observed a mean agreement of 87% between the first and the second questionnaire.
Variables
We developed two questionnaires. The patients questionnaire that was divided into several sections, which explored the following: 1) sociodemographic and lifestyle data, 2) duration and burden of LBP, 3) pain interference with normal activities and functional status, and 4) patients’ lifetime use and perception of usefulness of 30 therapies specifically for crLBP, 21 of which were CM therapies. Therapies chosen for the questionnaire were based on the potentially most used therapies according to different factors: prevalence of use, reimbursement by the Swiss healthcare system or scientific evidence. All therapies considered as CM in the present study are indicated with a superscript letter in Table 3. As recommended in the report of the National Institutes of Health task force on research standards for crLBP,34 we used the research task force impact classification scoring tool to determine the impact of crLBP on respondents’ daily life. PROMIS (Patient Reported Outcomes Measurement Information System) scores for pain intensity, physical function, and pain interference34,35 were part of this measurement tool. Current smoking was assessed with the question: “Do you currently smoke, even occasionally?” (answer: yes/no).36,37 The PCP questionnaire was divided into 4 sections exploring: 1) socio-demographic data, 2) PCPs’ perception of usefulness of 25 therapies specifically for crLBP, 23 of which were CM therapies, and their reported prescribing behavior, 3) PCPs’ perceived usefulness of CM in general and of specific CM treatments and their recommendations, and 4) PCP’s attitude towards use of CM.
Statistical analysis
Statistical analyses were performed using R version 3.5.0. We considered that missing values occurred completely at random and proceeded to complete cases analyses. Results were expressed as means (SD) or as percentages. Intraclass correlation coefficients (ICC) were calculated for Tables 3 and 4 in order to quantify the cluster effect. ICC are estimated using mixed models. ICC is defined as the ratio of between-cluster variance to total variance. The variances are estimated using regression model with random intercept and no other predictors. Multivariate analysis was performed using logistic regression and results were expressed as OR and 95% CI. We performed multivariate analyses for the therapies used by at least 20% of participants. The response variable was the use or not of the therapy and the explicative variables were patients’ age, gender, education, smoking habits, pain duration, CM insurance coverage, the PCPs’ gender, age, and training in CM. These explicative variables were selected because they were often associated with therapy use in other studies.25,26,38 Since the ICC were not negligible in univariate analyses, a random effect was considered to take account of the cluster design.39
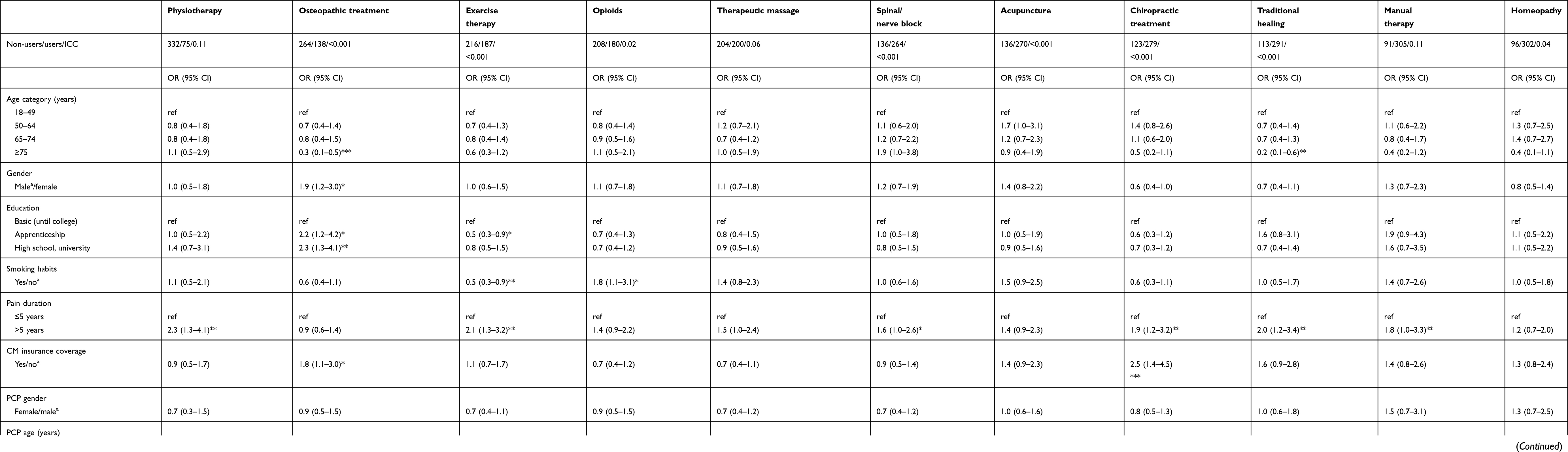 |
Table 4 Multivariate associations of lifetime use of therapies by patients living with chronic low back pain, for therapies used by at least 20% of participants, according to sociodemographic variables, pain duration, insurance coverage, and PCP characteristics |
Results
Response rate
Of 149 PCPs contacted, 60 agreed to participate and 45 eventually did (Figure 1). A total of 514 completed patient questionnaires were returned, 15 of which could not be included because the two PCPs associated with the patients did not return their own questionnaire. Thus, the patient response rate was 37% (499 of 1350). Selected sociodemographic characteristics are summarized in Table 1. Over half of the participants (n=272, 55%) were unemployed, most of these being retired (n=205, 75%).
LBP characteristics
Pain characteristics are presented in Table 2. For most participants, crLBP had been an ongoing problem for >5 years. Almost a third of the participants experienced severe LBP and half experienced moderate LBP in the 6 months before completing the questionnaire. Half of the participants had experienced LBP every day or nearly every day during the 6 months before completing the survey. The impact score of LBP on daily living was rated as moderate or severe by 79.2% of study participants.
Therapies used to manage crLBP
The top 5 therapies used by patients for crLBP during their lifetime were physiotherapy, followed by osteopathic treatment, exercise therapy, opioids and therapeutic massage (Table 3). Overall, the mean number of different therapies used by each participant was 6.5 (SD=3.9). Table 3 shows which treatments are reimbursed by basic or CM health insurance in Switzerland. The therapies most often used by patients are not always reimbursed by basic health insurance coverage. Among the top 5 therapies used to relieve crLBP during a patient’s lifetime, no medical prescription is required for osteopathic treatment and therapeutic massage. Among the therapies used by at least 20% of participants (ie, 11 therapies), the five therapies rated by the patients (who used those therapies) as being most helpful for this condition were osteopathic treatment, opioids, manual therapy, physiotherapy, and exercise therapy. Among these 11 frequently used therapies, only homeopathy received a mean perceived usefulness score under 5 points (on a 0–10 visual analog scale) according to the patients. Among 25 therapies, the five therapies rated as being most useful according to PCPs were physiotherapy, osteopathic treatment, yoga, meditation, and manual therapy. Regarding the group of therapies considered as CM specifically, 86.6% of the participants had used at least one of them to manage their crLBP during their lifetime, with a mean of 3.3 (SD=2.9) CM therapies used per participant. In the previous 12 months, 61.1% of participants reported any CM use for crLBP.
Multivariate analysis
In the continuity of the primary objective, we identified the factors associated with therapies used for crLBP by at least 20% of the participants during their lifetime. Table 4 shows the multivariate analysis of participants’ consumption patterns for those therapies, adjusted for patients’ age, gender, education, current smoking, pain duration, and CM insurance coverage, as well as for PCPs gender, age, and training in CM. Except for osteopathic treatment, which was used significantly more often by women, patient gender was not associated with the consumption of any therapy. Older age of patients (≥75 years) was negatively associated with the use of osteopathic treatment and traditional healing. A higher education was significantly associated with increased use of osteopathic treatment for crLBP. Current smoking was associated with significantly greater odds of having used opioids and significantly lower odds of having followed exercise therapy for crLBP. Respondents having experienced crLBP for >5 years were more likely to have resorted to physiotherapy, exercise therapy, spinal/nerve block, chiropractic treatment, traditional healing, and manual therapy than were respondents having experienced crLBP for <5 years. Respondents having CM insurance coverage were more likely to have used osteopathic treatment and chiropractic treatment for crLBP. Neither the PCPs’ age nor their gender was significantly associated with patients’ lifetime use of any therapy. Participants visiting a PCP who had training in CM were significantly less likely to have resorted to opioids during their lifetime to manage crLBP.
Patient-PCP communication
Regarding communication, 46.1% of the participants reported that their PCP did not enquire about their CM use. Among patients using CM (n=465), 64.7% spontaneously informed their PCP about their CM use. Among all patients, 42.7% reported that the PCP advised CM as a treatment option for crLBP. Most patients (80.4%) would be likely or very likely to try CM if their PCP offered such a treatment option.
Discussion
Patients with crLBP who visited their PCPs used a wide range of therapies, not always covered by basic health insurance, to manage their condition. The top five therapies used for crLBP during a patient’s lifetime were physiotherapy, osteopathic treatment, exercise therapy, opioids, and therapeutic massage. Study participants had used on average 6.5 therapies to manage their crLBP during their life. The use of physiotherapy was significantly associated with longer pain duration; osteopathic treatment was associated with age under 75 years, female gender, higher education, and CM insurance coverage. Exercise therapy was associated with non-smoking and longer pain duration. The PCPs’ age and gender were not associated with the use of specific crLBP treatments. Patients of PCPs who were trained in CM were significantly less likely to have used opioids for crLBP. Regarding communication, about a half of participants reported that their PCP did not enquire about their CM use.
It is difficult to find reliable comparative figures of crLBP treatment use. First, there is a paucity of studies on treatment use that includes both conventional and CM for crLBP. Second, existing estimates vary greatly, depending on clinical setting, period of observation, and CM definition. Osteopathic treatment and therapeutic massage were also among the most commonly used CM in another study in the same city and in an integrative review involving several countries (Australia, Belgium, Canada, Denmark, Germany, UK, and USA).26,40 Lifetime CM use for crLBP was higher in our study (86.6%) than in a study conducted in a tertiary spine orthopedic clinic in Hong Kong (72.3%).41 We also found a higher occurrence of CM use than that found in a pain center in Switzerland (77.3%).26 Our observation that those with crLBP often seek several different treatment options is consistent with the literature.26,40,42,43 Patients and their PCPs had different opinions when rating the usefulness of opioids: patients ranked opioids in second rank (among 11), while their PCPs ranked opioids after the tenth position (among 25 therapies).
Although previous studies reported that female gender, younger age, and higher education were associated with the use of CM therapies,25,44 among the therapies used by >20% of participants, these three predictors were associated only with osteopathic treatment.
We observed that the lack of coverage of some therapies by the mandatory basic health insurance in Switzerland did not prevent participants from using them. Indeed, some therapies excluded from basic health insurance coverage are among the most used, for example, osteopathic therapy and therapeutic massage. This might suggest that patients are satisfied with these therapies and willing to access them by signing up for supplemental CM insurance coverage or by paying out of pocket. Another explanation could be that having a supplemental insurance coverage for CM therapies could also be a reason why patients resort to CM in first place. Participants with CM insurance coverage were more likely to use chiropractic and osteopathic therapies, which seems surprising because chiropractic treatment is reimbursed by mandatory basic health insurance. One explanation is that patients who underwent osteopathic treatment might also have turned to chiropractic because it is covered by the basic health insurance scheme. However, the temporal sequence of the use of various treatments is not known in the present study.
Regarding PCP prescription practices in individuals presenting with crLBP, previous studies found that the gender of the treating practitioner influenced pain management practices for the treatment of back pain, which does not seem to be the case in our study.45,46 However, the link between PCPs’ age and gender and their referral patterns is not always clear in the literature.38,47 In our study, half of the participants indicated that their PCP inquired about CM use, whereas two-thirds of CM users told their PCP about it, which is consistent with previous findings in Switzerland.26 In the Hong Kong study, only one-third of CM users informed their PCPs of such use41 and the same proportion was obtained in the meta-analysis of disclosure rate for biologically-based CM.30 However, this meta-analysis was not focused on crLBP and included a large variety of populations and indications.
In primary care, the patient–PCP partnership and communication are of prime importance in the management of crLBP.48–50 An effective partnership between patients and PCPs may improve patients’ self-ability to manage their pain and could improve patients’ health outcomes particularly with the growing acceptation of the concept of patient-centered care in health-care services.50,51 Studies on nondisclosure of CM use consistently mention three main reasons for patients not informing their PCP:52 fear of a negative reaction from the PCP, the view that the PCP does not need to know about patient CM use and does not know much about CM, and the PCP not asking about CM use.30 PCPs should address the question of CM use with their patients more systematically.23 Physicians specialized in integrative and complementary medicine could help inform and guide PCPs and patients with crLBP about the most effective CM treatment options, their potential interactions with conventional therapies, and their side effects. PCPs should open the dialogue with their patients to inform them about effective care options and to establish together shared decision making about crLBP management.
In practice, crLBP patients use a wide range of treatments to manage their condition. Although the high frequency of use and perceived benefit of osteopathic therapy and therapeutic massage seem to be in accordance with rising evidence about the benefit of these therapies in the context of LBP,53,54 our results underline the fact that use of care is not systematically in accordance with the best currently available evidence. Indeed, therapies lacking evidence of effectiveness for crLBP may be overused, such as homeopathy or the frequent use of opioids to treat severe forms of crLBP, despite recent data showing no additional benefit of opioids relative to non-opioid medication.11 Conversely, treatment options may be underused, such as acupuncture, yoga and mindfulness-based stress reduction, as recent data showed a small to moderate effect, with yoga having the lowest quality of evidence.16,23 The guidelines of the American College of Physicians,23 which have provided a recent assessment of effective noninvasive treatments for crLBP (involving both CM and conventional therapies) could be an important tool in improving PCPs’ knowledge about effective treatments.
Among the limitations of our study, the use of crLBP-related care during a lifetime is prone to recall bias. Patients with crLBP may have preferentially indicated treatments used to alleviate acute episodes of LBP (in particular self-prescribed therapies). In addition, patients actively involved in their crLBP management may have participated more readily than less concerned patients. This potential selection bias might have led to an overestimation of the total number of therapies used. The high proportion of CM options in the questionnaire could also have led to an overestimation of CM use in comparison with conventional treatments (by drawing the patients’ attention to their past CM use). Because the participation rate was limited (33%), and the study did not have any comparison data about nonparticipants, the results of this study might not be generalizable. Despite the adjustment for education level and CM insurance coverage in multivariate analyses, we cannot exclude residual confounding by the financial situation of patients.55 We did not inquire about some pain medications, like the use of acetaminophen or NSAIDs. Such medication being the most prescribed and over-the-counter therapy used overall,56 we did not think that it was relevant to assess its lifetime use, which would certainly reach 100%. However, it could have influenced the ranking of our results concerning the most often used therapies. Our study focused on the prevalence of lifetime use of crLBP treatments and not the therapies used during the previous year only; such a measurement would have shown fewer treatment users. Neither did we ask questions about the frequency of use of each therapy. Another limitation is the lack of information about the exact circumstances in which patients used the mentioned therapies, notably how the LBP episodes were treated. The comparison between the perceptions of PCPs and patients regarding usefulness should be interpreted with great caution because the denominators differed (patients only rated the usefulness of therapies they had used, while physicians rated the usefulness of 25 therapies).
The study strengths include the use of a detailed and relatively comprehensive list of various treatment options, including crLBP treatments requiring no medical prescription, that is, data not available in routine statistics. In addition, we collected data about both the patients and their PCPs. Moreover, the choice of a private-practice-based study design is appropriate because, according to the literature, exclusive CM use for back pain is rare and those who experience back pain use CM alongside conventional medical therapies.40
Conclusion
Patients visiting their PCP used a wide range of treatments, including conventional and CM therapies for crLBP, and almost half of them did not have the opportunity to discuss these options with their PCP. This study did not reveal an obvious pattern between treatment use and factors such as age, education level and gender of participants. Equipped with this information, PCPs should routinely inquire their patients about their treatment use for their crLBP, including CM.
Abbreviation list
CM, complementary medicine; CrLBP, chronic or recurrent low back pain; ICC, intraclass correlation coefficient; LBP, low back pain; PCP, primary care physician.
Acknowledgments
The authors thank Prof. Isabelle Décosterd for her contribution to the design of the study. The authors acknowledge and express their gratitude to the patients and PCPs who participated in this study. This research project was supported by the Health Medicine Research program with a grant from the Swiss Academy of Medical Sciences and the Gottfried and Julia Bangerter-Rhyner Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Buchbinder R, Blyth FM, March LM, Brooks P, Woolf AD, Hoy DG. Placing the global burden of low back pain in context. Best Pract Res Clin Rheumatol. 2013;27(5):575–589. doi:10.1016/j.berh.2013.10.007
2. Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet (London, England). 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
3. Freburger JK, Holmes GM, Agans RP, et al. The rising prevalence of chronic low back pain. Arch Intern Med. 2009;169(3):251–258. doi:10.1001/archinternmed.2008.543
4. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037.
5. Machado GC, Maher CG, Ferreira PH, et al. Can recurrence after an acute episode of low back pain be predicted? Phys Ther. 2017;97(9):889–895.
6. Dunn KM, Hestbaek L, Cassidy JD. Low back pain across the life course. Best Pract Res Clin Rheumatol. 2013;27(5):591–600.
7. Gore M, Sadosky A, Stacey BR, Tai KS, Leslie D. The burden of chronic low back pain: clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine. 2012;37(11):E668–677.
8. Haldeman S, Dagenais S. A supermarket approach to the evidence-informed management of chronic low back pain. Spine J. 2008;8(1):1–7.
9. Mortimer M, Ahlberg G, Group MU-NS. To seek or not to seek? Care-seeking behaviour among people with low-back pain. Scand J Public Health. 2003;31(3):194–203.
10. Enthoven WT, Roelofs PD, Deyo RA, van Tulder MW, Koes BW. Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst Rev. 2016;2:CD012087. doi:10.1002/14651858.CD004158.pub3
11. Krebs EE, Gravely A, Nugent S, et al. Effect of opioid vs nonopioid medications on pain-related function in patients with chronic back pain or hip or knee osteoarthritis pain: the SPACE randomized clinical trial. JAMA. 2018;319(9):872–882. doi:10.1001/jama.2018.0899
12. Enke O, New HA, New CH, et al. Anticonvulsants in the treatment of low back pain and lumbar radicular pain: a systematic review and meta-analysis. CMAJ. 2018;190(26):E786–E793. doi:10.1503/cmaj.171333
13. Shaheed CA, Maher CG, Williams KA, Day R, McLachlan AJ. Efficacy, Tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med. 2016;176(7):958–968. doi:10.1001/jamainternmed.2016.1251
14. Machado GC, Maher CG, Ferreira PH, Day RO, Pinheiro MB, Ferreira ML. Non-steroidal anti-inflammatory drugs for spinal pain: a systematic review and meta-analysis. Ann Rheum Dis. 2017;76(7):1269–1278. doi:10.1136/annrheumdis-2016-210597
15. World Health Organization (WHO). Traditional, complementary and integrative medicine: definitions. Available from: http://www.who.int/traditional-complementary-integrative-medicine/about/en/.
16. Cramer H, Lauche R, Haller H, Dobos G. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29(5):450–460. doi:10.1097/AJP.0b013e31825e1492
17. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172(19):1444–1453. doi:10.1001/archinternmed.2012.3654
18. Franke H, Franke JD, Fryer G. Osteopathic manipulative treatment for nonspecific low back pain: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2014;15(1):286. doi:10.1186/1471-2474-15-286
19. Tan G, Rintala DH, Jensen MP, Fukui T, Smith D, Williams W. A randomized controlled trial of hypnosis compared with biofeedback for adults with chronic low back pain. Eur J Pain. 2015;19(2):271–280. doi:10.1002/ejp.545
20. Kong LJ, Lauche R, Klose P, et al. Tai Chi for chronic pain conditions: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2016;6:25325. doi:10.1038/srep25325
21. Chou R, Huffman LH, American Pain S, American College of P. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med. 2007;147(7):492–504.
22. van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Best Pract Res Clin Rheumatol. 2010;24(2):193–204. doi:10.1016/j.berh.2010.01.002
23. Qaseem A, Wilt TJ, McLean RM, Forciea MA, Clinical Guidelines Committee of the American College of P. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the american college of physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
24. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;(12): 1–23.
25. Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA 1998;280(18):1569–1575.
26. Dubois J, Scala E, Faouzi M, Decosterd I, Burnand B, Rodondi PY. Chronic low back pain patients’ use of, level of knowledge of and perceived benefits of complementary medicine: a cross-sectional study at an academic pain center. BMC Complement Altern Med. 2017;17(1):193. doi:10.1186/s12906-017-1708-1
27. https://www.ch.ch. Health insurance – Supplementary insurance. 2018; Available from: https://www.ch.ch/en/health-insurance-supplementary-insurance/.
28. Klein SD, Torchetti L, Frei-Erb M, Wolf U. Usage of complementary medicine in switzerland: results of the swiss health survey 2012 and development since 2007. PLoS One. 2015;10(10):e0141985. doi:10.1371/journal.pone.0141985
29. Busato A, Donges A, Herren S, Widmer M, Marian F. Health status and health care utilisation of patients in complementary and conventional primary care in Switzerland–an observational study. Fam Pract. 2006;23(1):116–124. doi:10.1093/fampra/cmi078
30. Foley H, Steel A, Cramer H, Wardle J, Adams J. Disclosure of complementary medicine use to medical providers: a systematic review and meta-analysis. Sci Rep. 2019;9(1):1573. doi:10.1038/s41598-018-38279-8
31. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
32. Sherman KJ, Cherkin DC, Connelly MT, et al. Complementary and alternative medical therapies for chronic low back pain: what treatments are patients willing to try? BMC Complement Altern Med. 2004;4:9.
33. Stussman BJ, Bethell CD, Gray C, Nahin RL. Development of the adult and child complementary medicine questionnaires fielded on the National Health Interview Survey. BMC Complement Altern Med. 2013;13:328. doi:10.1186/1472-6882-13-118
34. Deyo RA, Dworkin SF, Amtmann D, et al. Report of the National Institutes of Health task force on research standards for chronic low back pain. J Manipulative Physiol Ther. 2014;37(7):449–467. doi:10.1016/j.jmpt.2014.07.006
35. Deyo RA, Katrina R, Buckley DI, et al. Performance of a Patient Reported Outcomes Measurement Information System (PROMIS) Short form in older adults with chronic musculoskeletal pain. Pain Med. 2016;17(2):314–324.
36. Alkherayf F, Wai EK, Tsai EC, Agbi C. Daily smoking and lower back pain in adult Canadians: the Canadian Community Health Survey. J Pain Res. 2010;3:155–160.
37. Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between smoking and low back pain: a meta-analysis. Am J Med. 2010;123(1):87 e87–35.
38. Corbin Winslow L, Shapiro H. Physicians want education about complementary and alternative medicine to enhance communication with their patients. Arch Intern Med. 2002;162(10):1176–1181.
39. Kerry SM, Bland JM. The intracluster correlation coefficient in cluster randomisation. BMJ. 1998;316(7142):1455.
40. Murthy V, Sibbritt DW, Adams J. An integrative review of complementary and alternative medicine use for back pain: a focus on prevalence, reasons for use, influential factors, self-perceived effectiveness, and communication. Spine J. 2015;15(8):1870–1883.
41. Tsang VHM, Lo PHW, Lam FT, et al. Perception and use of complementary and alternative medicine for low back pain. J Orthop Surg (Hong Kong). 2017;25(3):2309499017739480.
42. Canizares M, Hogg-Johnson S, Gignac MAM, Glazier RH, Badley EM. Changes in the use practitioner-based complementary and alternative medicine over time in Canada: cohort and period effects. PLoS One. 2017;12(5):e0177307.
43. Broom AF, Kirby ER, Sibbritt DW, Adams J, Refshauge KM. Use of complementary and alternative medicine by mid-age women with back pain: a national cross-sectional survey. BMC Complement Altern Med. 2012;12:98.
44. Foltz V, St Pierre Y, Rozenberg S, et al. Use of complementary and alternative therapies by patients with self-reported chronic back pain: a nationwide survey in Canada. Joint Bone Spine. 2005;72(6):571–577.
45. Bernardes SF, Costa M, Carvalho H. Engendering pain management practices: the role of physician sex on chronic low-back pain assessment and treatment prescriptions. J Pain. 2013;14(9):931–940.
46. Weisse CS, Sorum PC, Dominguez RE. The influence of gender and race on physicians’ pain management decisions. J Pain. 2003;4(9):505–510.
47. Roter DL, Hall JA, Aoki Y. Physician gender effects in medical communication: a meta-analytic review. Jama. 2002;288(6):756–764.
48. Farin E, Gramm L, Schmidt E. The patient-physician relationship in patients with chronic low back pain as a predictor of outcomes after rehabilitation. J Behav Med. 2013;36(3):246–258.
49. Fu Y, Yu G, McNichol E, Marczewski K, Jose Closs S. The effects of patient-professional partnerships on the self-management and health outcomes for patients with chronic back pain: a quasi-experimental study. Int J Nurs Stud. 2016;59:197–207.
50. Darlow B, Dowell A, Baxter GD, Mathieson F, Perry M, Dean S. The enduring impact of what clinicians say to people with low back pain. Ann Fam Med. 2013;11(6):527–534.
51. Fu Y, McNichol E, Marczewski K, Closs SJ. Patient-professional partnerships and chronic back pain self-management: a qualitative systematic review and synthesis. Health Soc Care Community. 2016;24(3):247–259.
52. Robinson A, McGrail MR. Disclosure of CAM use to medical practitioners: a review of qualitative and quantitative studies. Complement Ther Med. 2004;12(2–3):90–98.
53. Kumar S, Beaton K, Hughes T. The effectiveness of massage therapy for the treatment of nonspecific low back pain: a systematic review of systematic reviews. Int J Gen Med. 2013;6:733–741.
54. Coulter ID, Crawford C, Hurwitz EL, et al. Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. Spine J. 2018;18(5):866–879.
55. Frass M, Strassl RP, Friehs H, Mullner M, Kundi M, Kaye AD. Use and acceptance of complementary and alternative medicine among the general population and medical personnel: a systematic review. Ochsner J. 2012;12(1):45–56.
56. Chou R, Deyo R, Friedly J, et al. Systemic pharmacologic therapies for low back pain: a systematic review for an american college of physicians clinical practice guideline. Ann Intern Med. 2017;166(7):480–492.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.