Back to Journals » Risk Management and Healthcare Policy » Volume 14
Prevention of Occupational Hazards Among Sanitary Workers: Knowledge, Attitude, and Practice Survey in Bulehora, West Guji Zone, Oromia, Ethiopia
Authors Degavi G ![]() , Dereso CW, Shinde S
, Dereso CW, Shinde S ![]() , Adola II SG
, Adola II SG ![]() , Kasimayan P
, Kasimayan P ![]()
Received 4 March 2021
Accepted for publication 10 May 2021
Published 31 May 2021 Volume 2021:14 Pages 2245—2252
DOI https://doi.org/10.2147/RMHP.S308323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Girish Degavi,1 Chala Wata Dereso,2 Sanjay Shinde,1 Shiferaw Gelchu Adola II,1 Pandiarajan Kasimayan1
1Department of Nursing, College of health and medical science, Bulehora University, Hegremariam, Oromia, Ethiopia; 2Bulehora University, Hegremariam, Oromia, Ethiopia
Correspondence: Girish Degavi
Department of Nursing, College of health and medical science, Bulehora University, Hegremariam, Oromia, Ethiopia
Tel +251-966686212
Email [email protected]
Introduction: The production of waste is due to the result of commercial activities, consumption, and utilization of products or materials. It is further believed that mainly solid waste includes non-harmful waste which may be from households, mainly kitchens, and even from organizations and institutions, shops and various types of markets, and manufacturing industries. Solid waste handling, management, and accurate and appropriate disposal is a hot topic relating to public and environmental health concerns.
Methods: A cross-sectional quantitative study design was incorporated to assess knowledge, attitude, and practice and associated factors regarding prevention of occupational risks and health hazards among sanitary workers in Bulehora University, a government organization in West Guji Zone, Ethiopia. One hundred and ninety-one solid waste handlers found to be working in this institution were included in the study.
Results: The response rate of samples in the present study was found to be 94.4%, of which the majority were females, which accounted for 79.7%. The median age of the study samples was 29 years. It was found that 64% of study samples stated good knowledge of the prevention of occupational health risks. About 76.4% of solid waste collectors had a good attitude and only 8.9% showed good practice regarding prevention of occupational health hazards. Job dissatisfaction was found to be a statistically significant factor along with the use of personal protective equipment (PPE) in implementing good practice work patterns among sanitation workers, even though they had been provided with basic personal protective equipment.
Conclusion: The study concluded that there is a need for development of plans on implementation of basic occupational health services while enforcing the provision of personal protective equipment and supervising solid waste collectors.
Keywords: occupational hazards, sanitary workers, West Guji Zone, Bulehora University
Introduction
For many years urbanization has become an inescapable pattern in developing nations with rapid financial developments. Because of urbanization, a huge populace has amassed in urban areas causing numerous sanitation issues including a ton of trash, messy roads, and impeded drain channels which enormously increase the sanitation laborers’ workload and work hours.1
The working conditions of satiation laborers have remained practically unaltered for longer than a century. Aside from the social barbarities that these laborers face they are presented with certain medical issues by their occupation.2 These health dangers incorporate exposure to unsafe gases, for example, methane and hydrogen sulfide, cardiovascular degeneration musculoskeletal issues like osteoarthritic changes and intervertebral disc herniation, disorders like hepatitis, leptospirosis, and helicobacter skin issues, respiratory issues, and altered respiratory parameters.3
When it comes to street cleaners, they have to overcome many issues revolving around sanitation infrastructure and the arrangement of services related to sanitation.4 Sanitation laborers offer fundamental public support yet regularly at the expense of their pride, security, wellbeing, and lifestyle.5 They are the absolute most weak and vulnerable workforce. They are extremely undetectable, unquantified and segregated, and face considerable difficulties which come from this major absence of affirmation. Sanitation laborers are exposed to occupational and environmental hazards possibly resulting in health ailments, injury, and even death.6
The aim of this study was that sanitation workers and their immediate employers would profit from this wellspring of data and get imaginative recommendations for controlling risks. There are many issues among laborers in hereditary legacy, constitutions, and infection susceptibility. In any case, the modern sanitation worker will have to arrange all those aspects related to health hazards for the betterment of his life holistically.3–5
The characteristics of metropolitan waste are contrasting between developing and industrialized nations, and bigger and smaller towns.3 It has been assessed that in developing nations, the degree of natural waste is moderately high, constituting between 40–70% of strong waste in developing nations. The expanding utilization of plastics as bundling material, and other inorganic materials have made waste disposal difficult. Accordingly, due to the capability of natural waste the safety of the laborers and workers who are working without proper PPE needs to be addressed urgently.7
Sanitation workers do not use PPE even if it is provided. The reason which motivates them to avoid using it is the misconception that using any kind of PPE while at work means that they are no longer physically strong enough and able to endure the strenuous and challenging work of being a sanitary worker, which causes fear of losing their job. The PPE provided by various institutions may not be adequate, and also they are not provided frequently, even after the PPE gets torn or damaged and inappropriate to use, which is against the safety protocol. Apart from this, the economic state of workers makes this equipment unaffordable to them. These bunches of existing problems in relation to the use of PPE in turn expose the sanitation health workers to hazardous materials and diseases which are preventable with the use of simple protective equipment to some extent.8
The employee plays a major role in the occupational hygiene program. They are excellent sources of data on work processes, methods, and the ones who can identify apparent dangers of sanitation workers’ everyday tasks.
Methods
The present study was conducted at Bulehora University, West Guji Zone, Ethiopia, which is one of the public higher educational institutions established in 2009 G.C. and it is located in the Oromia region, West Guji Zone Bulehora town, 470 km south of Addis Ababa. There is a total of 16,000 students of different degree programs in addition to 4292 staff of which 1061 are academic staff, 2226 administrative staff, and 1005 temporary daily workers currently working in BHU. The total number of sanitary workers currently working in BHU is 292, of which 284 are female and 8 are male.
The institutional-based cross-sectional study was conducted from August 01, 2020, and September 30, 2020 G.C among sanitary workers in Bulehora University, Oromia region southern Ethiopia.
All sanitary workers working in the Bluehora University during that time who were available during the data collection period after calculating the sample size were included in this study using the systematic sampling technique. Sanitary workers who were on annual vacation, sick leave, and maternity leave and who did not volunteer to participate in this study were excluded from the study. The sample size was determined using a standard formula for single population proportion, Z (a/2) =1.96 (95% confidence level of the survey) P=60.8% knowledge of sanitary workers studies done in Addis Ababa which resulted in maximum sample size. d = degree error tolerated (5%) from Formula, no= (1.96)2 (0.608) (1–0.608)/(0.05)2= 366. Since the study population was less than 10,000, which 292 we use correction formula.9 After adding 10% for non-respondents, final sample size was decided as 191.
The systematic sampling technique was used in this study, sampling frame prepared from the list of the names of sanitary workers, then Kth interval calculated. The starting point identified by a simple random sampling technique. Finally, using Kth interval, study subjects were included in the sample.
Sociodemographic variables were recorded and questionnaire to assess knowledge of waste disposal, the attitude of sanitary workers, availability and utilization of PPE, personal hygiene, and a questionnaire regarding psychosocial related issues of solid waste collectors related to their work were conducted. Socio-demographic variables included gender, age, marital status, educational level, working experience. To measure the knowledge level of sanitary workers, 09 questions were used. These questions were answered by “Yes/No” and “I do not know” options. “Yes” was assigned 1 point and “No” was assigned 0 points. Then the mean scores of knowledge were calculated. Sanitary workers who scored greater than mean were considered as having good knowledge and those who scored less than the mean score were categorized as having poor knowledge toward solid waste handling. For the rest of the dependent variables, the same procedure was implemented.
Knowledge, attitude, and practice of sanitary workers were the dependent variables and independent variables in this study were: sociodemographic factors: age, sex, marital status, level of education (01 to 12) from elementary to higher secondary school education, monthly income, working condition factors including work experience, daily work hours, behavioral factors including kchat chewing, sleeping problems, alcohol drinking, job satisfaction, smoking, occupational safety factors, health and safety training and education, availability and utilization of PPE.
The quality of the data was assured by using standard, pre-tested questionnaires, proper data collection procedure, and reliability test. Prior to the actual data collection, pre-testing was done on 10% of the total study subjects at Dilla University who were not included in the actual study, and based on the findings necessary amendments were made regarding its consistency, clarity, and logical adequacy and the time it took to complete the questionnaire.
The data were coded, checked for errors, the missing value was dealt with and cleaned data (edited) were entered into Epi-Data version 4.4.3.1 and exported to SPSS Statistics Version 20 for analysis.
The results of descriptive statistics were summarized and presented by tables, charts, and graphs. Percentage, frequency, and mean were calculated. Bivariate logistic regression analysis was done to check the association between dependent and independent variables. Variables with association at p< 0.25 were entered into a multivariate logistic regression analysis to control confounding variables and determine the strength of association. Statical significance was declared at p < 0.05 and 95% confidence intervals.
Result
Socio-Demographic Variables of Solid Waste Collectors Working at BHU, 2020
One hundred ninty one waste handlers participated in the study with 94.8% response rate. The majority of respondents were female which accounted for 95.78% and the median age of respondents was 29 years ranging from 17 to 45 years minimum and maximum respectively. 48.93% were married followed by 29.78% who were single and 6.38%, 4.25%, 6.38% were divorced, separated, and widowed respectively. Most of the study subjects had education between 09–12 Grade (45.21%) followed by Grade 5–8 (22.34%) and (14.36%) and (13.82%) below Grade 1–4 and being illiterate respectively (Figure 1).
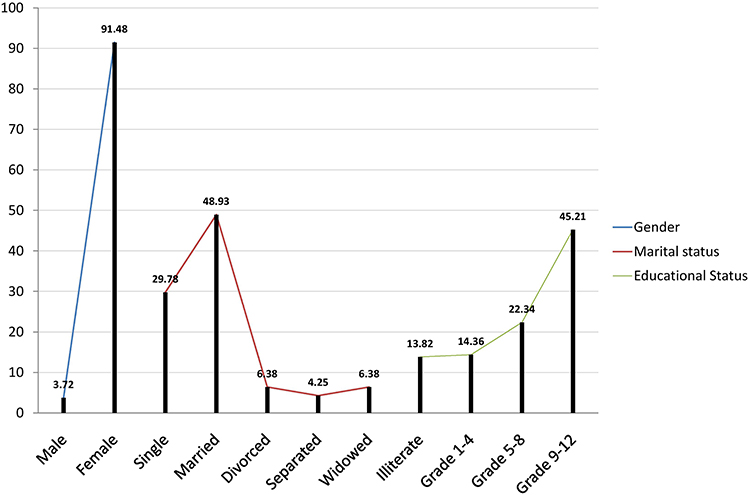 |
Figure 1 Socio-demographic variables of solid waste collectors working at BHU, 2020. Among all the waste handlers who participated in the study with above 90% response rate. Nearly three quarters of respondents were aged below 45 years. Nearly 50% were married, followed by around one third being single and the remaining were divorced, separated, and widowed respectively. Maximum number of participants of study had education below higher secondary. |
Solid waste handlers were asked about training before engaging in the present work and only 77 (42.6%) of respondents were trained before engaging in this work. Regarding the training organization, 09 (4.7%) were trained by their association, 53 (29.3%) by government, and 35 (8.6%) by different Non-Governmental Organizations (NGOs), the rest did not receive any form of training. Concerning on-the-job training, 137 (76.4%) were trained by the government and the rest (43 (23.7%)) were trained by NGOs. 109 (60.8%) of the respondents did know about work-related health risks and also, 114 (63.1%) knew how to prevent work-related health risks and about the method of preventing health-related risks; the majority of the respondents answered: wearing gloves, masks, apron, and boots while working as a means of preventing occupational health hazards. About 133 (73.9%) of the waste handlers knew about PPE and the rest (47 (26.1%)) did not know much about PPE. Generally, about 144 (63.3%) solid waste handlers had good knowledge of preventing occupational health risks and about PPE (Table 1).
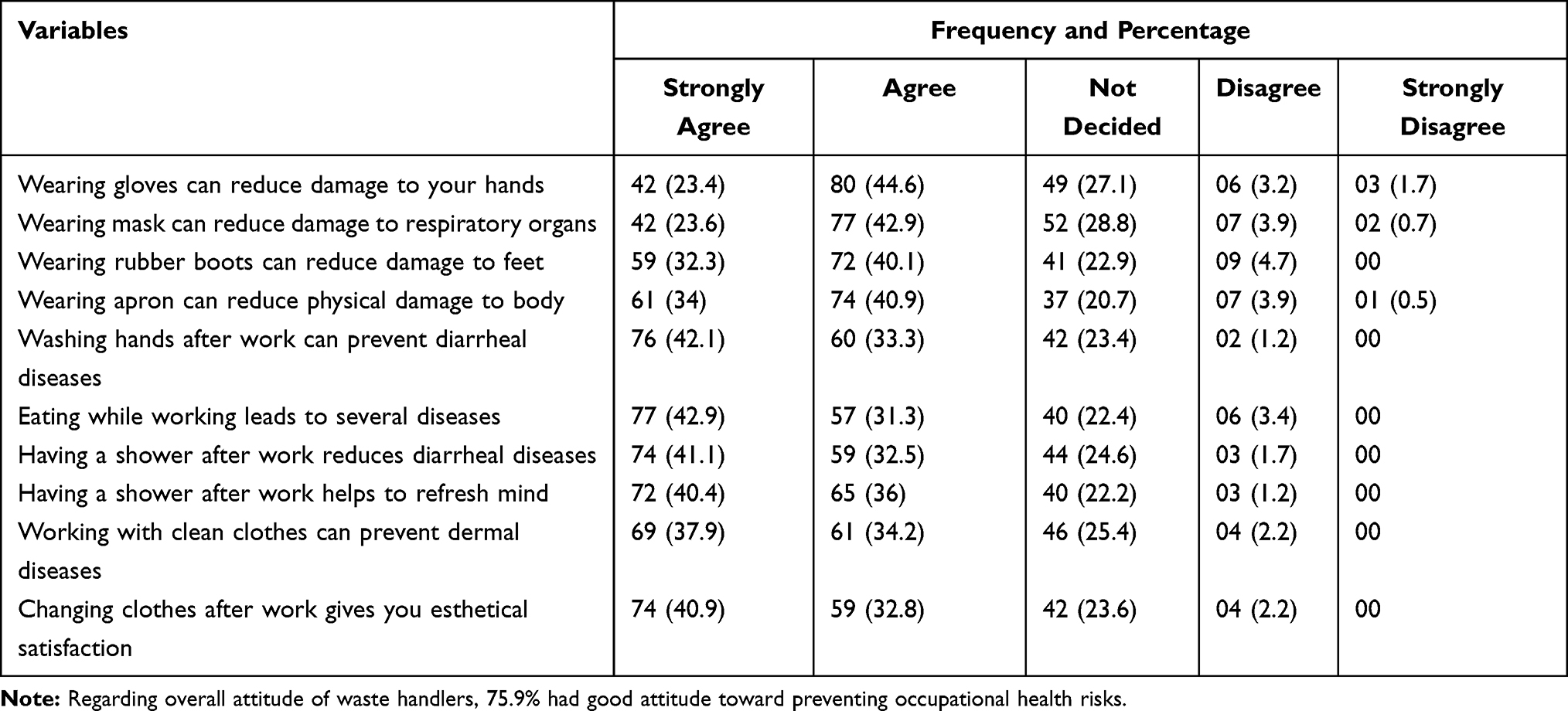 |
Table 1 Workers’ Knowledge and Attitude on Preventing Occupational Health Risks Among Bulehora University Solid Waste Collectors, Oromia Region, Ethiopia. September 2020, (n=191) |
Practice and Associated Factors Related Data in Preventing Occupational Health Risks
Results on PPE availability showed that 126 (70.4%) of the respondents had PPE like gloves, facemask, boots, and apron and only 07 (3.7%) waste collectors reported having overall PPE. 99 (55%) waste handlers reported using the materials while working. Among the non-users of PPE, 50 (61.9%) said they failed to use it because they did not have PPE, 05 (6.6%) lacked awareness, 17 (21.5%) stated discomfort, 02 (1.7%) negligence, and 07 (8.3%) “to save time”. Only 22 (12.1%) solid waste handlers had tetanus toxoid vaccine after engaging in this work. The remaining 158 (87.9%) did not get tetanus toxoid vaccine, 42 (26.5%) did not take vaccine because of lack of awareness, 112 (70.9%) had no access to vaccine, and 04 (2.5%) because of negligence.
The study participants were interviewed on some of their personal hygiene issues. Accordingly, 148 (82.5%) waste handlers were washing their hands with soap after work, 140 (78.1%) changed their wor clothes after work, 64 (36%) washed their work clothes after work every day, and 172 (95.9%) used soap on washcloths, 71 (39.4%) showered daily after work, 54 (30%) shared their work clothes and PPE with their colleagues, 64 (35.5%) of the respondents reported that they were eating at the workplace. Waste handlers’ behavioral related issues were observed stating: 17.6% faced physical abuse, 81.5% verbal abuse, and 0.8% other forms in the workplace. 27 (15.3%) were smokers, out of this 13 started smoking after starting waste collection job. 31 (17.3%) used to chew kchat (locally grown substance consumed as recreation leading to addiction) and also 16 of them started chewing after engaging this job. 41 (23%) of study participants had a sleeping problem, out of this, 35 started to face this problem after they engaged in this work. 83 (46.3%) of respondents were dissatisfied with their job. Low income (70.5%), bad working conditions and stigma (3.3%), lack of health insurance, and improper payment (2.7%) were the main reasons for job dissatisfaction (Table 2).
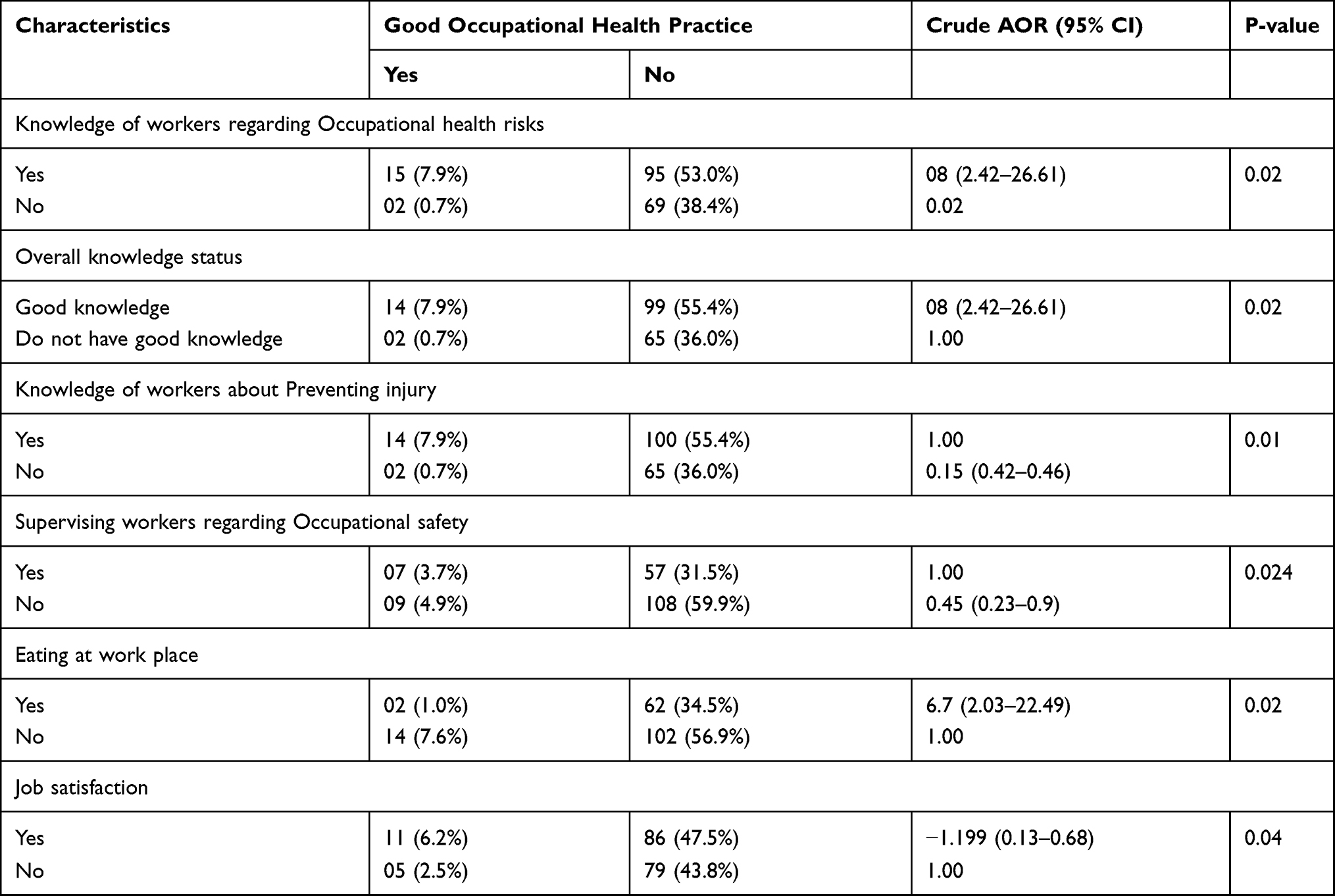 |
Table 2 Selected Occupational Health Risk Prevention Determinants, Bulehora University Solid Waste Collectors, Oromia Region, Ethiopia. September 2020, (n=191) |
Multivariate Analysis
The multivariate analysis was done by considering the conceptual framework to assess the relative effect of the explanatory factors on the outcome variable (prevention practice).
From all variables entered in all steps of analysis, only educational status and job satisfaction remained significant in multivariate analysis. Knowledge of workers regarding occupational health risks, knowledge of workers about preventing injury, overall knowledge, and supervision by the concerned body and job satisfaction were statistically significant to good occupational health practice at the bivariate level (Table 3).
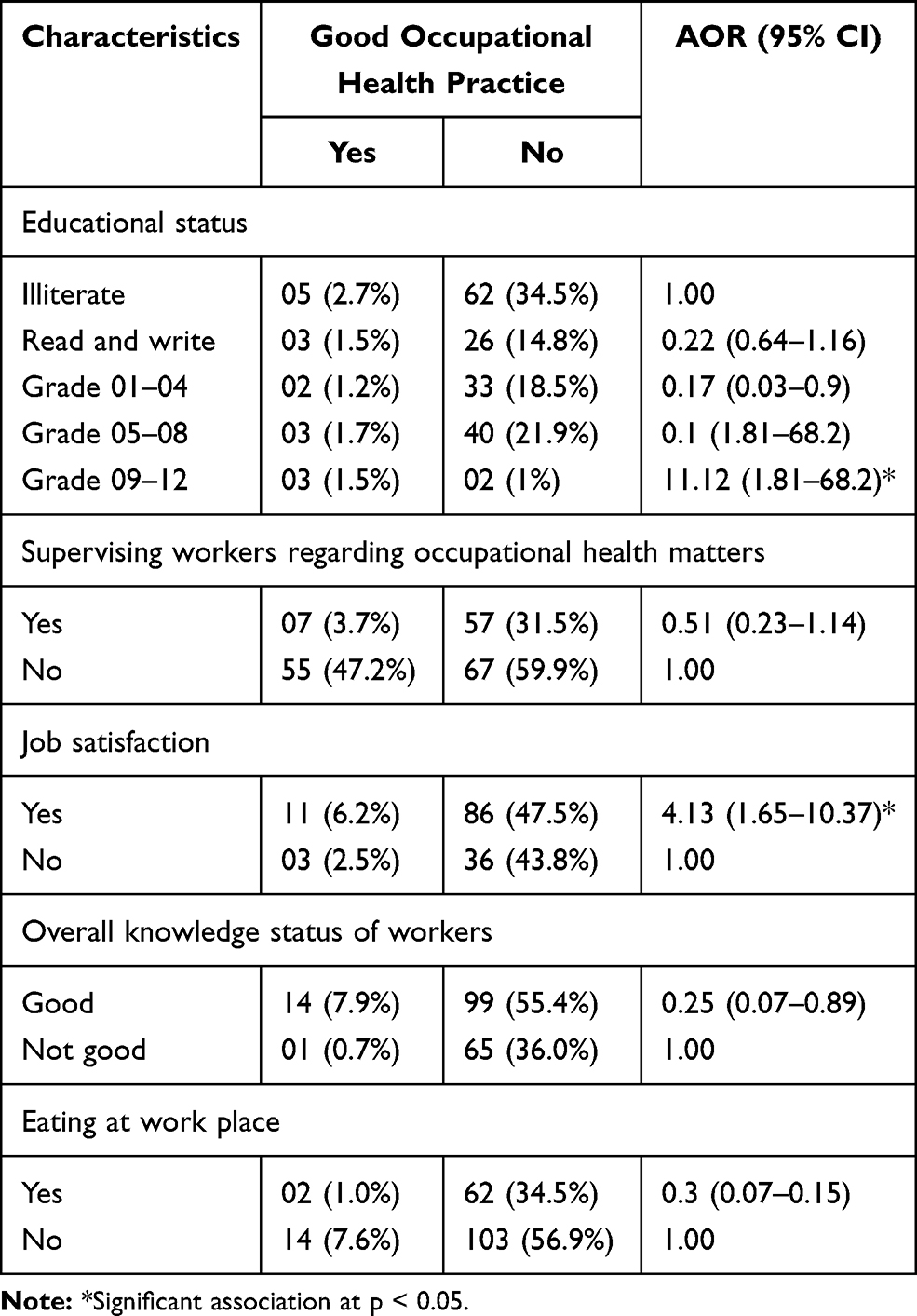 |
Table 3 Socio-Demographic, Knowledge, Attitude and Behavioral Factors regarding Good Occupational Health Practice Among Bulehora University Solid Waste Collectors, Oromia Region, Ethiopia. September 2020, (n=191) |
Discussion
The response rate of this study was 94.8%, which was comparable with previous studies, eg, 97.9%,7 92%,10 and 95%.11 Number of female solid waste collectors was higher as compared to some other studies which had either no or a small number of female workers in this sector.9,10,12 The main reason for a large number of females in this study might be due to the fact that this sector is one of the professions which needs less skills and females are actively involved due to the lack of education and inadequate access to skillful training available for females due to gender inequalities in this part of the world. The monthly income of waste collectors in this study was higher than in a previous study, 150 birr13 and 400 birr.7 This might be due to increasing government concern regarding this sector.
The proportion of waste collectors who were trained before engaging in this line of work was 42.6%, which is greater than in other studies done in Addis Ababa, 6%13,14 and 20.8%.7 This might be due to stakeholders’ involvement like involvement of micro and small scale development office, different non-government organizations, and solid waste management office.
Regarding to supervising solid waste handlers on occupational health and safety matters which is not significantly associated with occupational health risk preventing practice in this study and proper usage of PPE by solid waste handlers it was seen to be higher than in other studies done in Addis Ababa, 0%.13,14 Even if the prevalence in this study was low by itself, the result of being better than previous studies might be due to increasing concern of different stakeholders from time to time.
35.5% of solid waste collectors who participated in this study were eating at the workplace which is comparable with other studies done in Addis Ababa, 33.7%.9,13 78.1% of participants of this study washed their hands with soap after waste collection, which is comparatively high compared to another study which only had 27.7%10,13,14 which might be due to good knowledge of preventing occupational health risks and also due to COVID-19 awareness.
Rate of wearing PPE among Bulehora University solid waste handlers was higher than in previous studies, 39%13–15 and 37.6%.7 This might be due to the involvement of different non-government organizations in supplying PPE to waste handlers. Even though the quality of the gloves was not to the mark and most of the gloves were old, perforated, and not used appropriately. While reusable gloves were being provided by the employer on demand, lack of motivation and ignorance about health hazards among sanitary health workers and their immediate supervisors were the main factors of improper utilization and disposal of the gloves.16
Conflicting at the workplace, Kchat chewing, alcohol consumption, and smoking were the main psychosocial problems identified among solid waste collectors. Most employees admitted that these habits started after starting waste collection jobs. This might be due to job dissatisfaction due to stigma and discrimination from family members and neighbors because of their waste collection job, due to the tiring nature of the work, increased availability of these substances, and influence of other workers. However, only job satisfaction and educational status were statistically significant factors related to safe occupational health practice.
The study results clearly state that organizations need to recognize the risks which result from uncertainty which is brought by failure to recognize hazards. Hazards may be seen as a result of failure to implement plans and protocols and policies fully or to a sufficient degree. Therefore, improvement of measures is necessary to address controlling of risks in the workplace by diligently reviewing the protocol and policies to eliminate the hazards by using bio-medical waste management techniques. Advocating effective risk prevention behaviors by improvements in infrastructure and work culture, to achieve this administrative and managerial system has to be remodeled and parallel influence to all the stakeholders to make appropriate decisions regarding the safety of sanitary workers. This can be achieved substantially by implementing strict enforcement of PPE policy on sanitary workers while at work throughout the institution.16
Conclusion
The result of this study revealed that the magnitude of practice regarding preventing occupational health risks among solid waste collectors is very low. This study found that job dissatisfaction is a significant factor that leads to failure in preventive practices regarding occupational health risks. The administrative and managerial system of successful PPE policy relies on human behavior and appropriate supervision and distribution, mere availability of PPE will not keep the workplace safe. There is a sincere necessity for an employer and related stakeholders to consult the employees and local health and safety representatives to incorporate control measures by working together to achieve the highest level of practicable protection for sanitary health workers.
Abbreviations
KAP, knowledge attitude and practice; PPE, personal protective equipment; OH, occupational hazards; NGO, Non Governmental Organization; WHO, World Health Organization.
Data Sharing Statement
Data utilized and assessed in the present study can be made available through the corresponding author on request.
Ethical Approval
The Institutional Review Boards of Bulehora University, Ethical Review Board, and Institute of Health Sciences gave their approval. Some participants (aged 17) with sufficient literacy and skills were found and were able to agree to participate in the study. Since this study was harmless and only involved the gathering of basic work-related information, the researcher, with due permission from the ethical committee, provided participants with information on written consent, clearly stating the objectives of the study and their right to refuse. Then, written informed consent was obtained from each participant. The completed questionnaires were treated with care to maintain confidentiality and held in the safe custody of the corresponding author. By avoiding possible identifiers, the confidentiality of client-related data was preserved, and the analysis was performed in compliance with the Declaration of Helsinki.
Consent
A well-informed written consent was taken from each study subject after the potential benefits and risks and also the investigational intent of the study were defined.
Acknowledgment
The researchers owe a profound sense of appreciation to all those who helped with the successful accomplishment of this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in the publishing of this research study.
References
1. Private sector participation in municipal solid waste management: guidance Pack (5 Volumes) | public private partnership (Internet). Ppp.worldbank.org; 2020. Available from: https://ppp.worldbank.org/public-private-partnership/library/private-sector-participation-municipal-solid-waste-management-guidance-pack-5-volumes.
2. Lecture Notes – ethiopia public health training initiative (Internet). Cartercenter.org; 2020. Available from: https://www.cartercenter.org/health/ephti/learning_materials/lecture_notes/index.html.
3. Occupational Medicine. Oxford Academic (Internet). Volume 70.Issue 5.Academic.oup.com; 2020. Available from: https://academic.oup.com/occmed/issue/70/5.
4. Kampen V, Hoffmeyer F, Seifert C, et al. Occupational health hazards of street cleaners - a literature review considering prevention practices at the workplace. Int J Occup Med Environ Health. 2020;33(6):701–732. doi:10.13075/ijomeh.1896.01576
5. Athanasiou M, Makrynos G, Dounias G. Respiratory health of municipal solid waste workers. Occup Med (Chic Ill). 2010;60(8):618–623. doi:10.1093/occmed/kqq127
6. Khaiwal R, Kamalpreet K, Suman M. Occupational exposure to the municipal solid waste workers in Chandigarh, India, 2016 (Internet). SAGE J. 2020.
7. Bogale D, Kumie A, Tefera W. Assessment of occupational injuries among Addis Ababa city municipal solid waste collectors: a cross-sectional study. BMC Public Health. 2014;14(1). doi:10.1186/1471-2458-14-169
8. Górny A. Assessment and management of risk in improving the OHS Management System. Syst Saf Hum - Tech Facil - Environ. 2019;1(1):105–111. doi:10.2478/czoto-2019-0013
9. Baral Y. Waste workers and occupational health risks. Int J Occup Safety Health. 2018;8(2):1–3. doi:10.3126/ijosh.v8i2.23328
10. Amabye T. Occupational risks and hazards exposure, knowledge of occupational health and safety practice and safety measures among workers of sheba leather Plc, Wukro, Tigray Ethiopia. MOJ Public Health. 2016;4(2). doi:10.15406/mojph.2016.04.00074
11. Abo T. Municipal solid waste management in Addis Ababa (Internet). Academia.edu; 2020. Available from: https://www.academia.edu/3319471/Municipal_solid_waste_management_in_Addis_Ababa.
12. Roopa S, Padmavathi R, Akolkar A, et al. Respiratory functions of conservancy workers working in solid waste management sector of Chennai, India [version 2; peer review: 1 approved, 1 approved with reservations]. F1000Research 2013, 1:67 (https://doi.org/10.12688/f1000research.1-67.v2).
13. Al-Khatib I, Sato C. Solid health care waste management status at health care centers in the West Bank – palestinian Territory. Waste Manage. 2009;29(8):2398–2403. doi:10.1016/j.wasman.2009.03.014
14. COVID 19: occupational Health (Internet). Who.int; 2020. Available from: https://www.who.int/news-room/detail/09-03-2020-covid-19-occupational-health.
15. Skyberg K. Occupational safety and health in norway revisited. Int J Occup Safety Health. 2020;9(2). doi:10.3126/ijosh.v9i2.27309
16. National Institute for Occupational Safety and Health (NIOSH). Centers for Disease Control and Prevention. CDC - Hierarchy of Controls, Workplace Safety, and Health Topic. 2015.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.