Back to Journals » Clinical Ophthalmology » Volume 16
Preventing Retinal Detachment: Where are We? Implications from Stickler Syndrome
Authors Morris RE ![]() , Kuhn F, Sipos T
, Kuhn F, Sipos T
Received 7 September 2022
Accepted for publication 12 December 2022
Published 23 December 2022 Volume 2022:16 Pages 4315—4321
DOI https://doi.org/10.2147/OPTH.S388631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Robert Morris.
Views: 825
Robert E Morris,1– 3 Ferenc Kuhn,2,4 Timothy Sipos1– 3
1Retina Specialists of Alabama, LLC, Birmingham, AL, USA; 2Helen Keller Foundation for Research and Education, Birmingham, AL, USA; 3Department of Ophthalmology, University of Alabama at Birmingham (UAB), Birmingham, AL, USA; 4Department of Ophthalmology, University of Pécs Medical School, Pécs, Hungary
Correspondence: Robert E Morris, Helen Keller Foundation for Research and Education, 2208 University Boulevard, Suite 101, Birmingham, AL, USA, 35233, Tel +1 205 936-0704, Email [email protected]
Abstract: Stickler syndrome, a rare inherited disease, carries a lifetime risk of rhegmatogenous retinal detachment (RRD) of up to 65%, higher than any other predisposing condition known. Both syndromic and non-syndromic eyes suffer RRD predominately from the same pathogenesis, vitreous tractional tears in the peripheral retina. Consequently, extraordinary publications in 2021– 2022, each reporting successful prevention of RRD in Stickler syndrome, using 360-degree (encircling) laser retinopexy, provide the first strong evidence upon which similar prophylaxis in non-syndromic eyes at high risk of RRD from peripheral retinal tears can confidently go forward.
Keywords: retinal tear, retinal detachment, retinal detachment prevention, 360-degree laser retinopexy, stickler syndrome, encircling laser prophylaxis
Plain Language Summary
In a rare, inherited disease called Stickler syndrome, the vitreous gel is only partially formed within the eye. The vitreous can then move about with body movements from birth onward, tearing the peripheral retina and causing retinal detachment, even in childhood and adolescence. Blindness in multiple generations of Stickler syndrome families at a young age spurred efforts to find a retinal detachment prevention. Doctors in Cambridge, England, first found an effective prevention with cryotherapy. In 2021 and 2022, doctors in the United States and England announced that noninvasive encircling laser treatment of the peripheral retina can also prevent retinal detachment in most Stickler eyes.
Because most detachments are caused by peripheral retinal tears, this is strong evidence that similar encircling laser treatment could likely prevent many retinal detachments commonly seen in high-risk aging eyes. This would thus prevent the most frequent cause of acute blindness in otherwise healthy eyes of the elderly population.
Introduction
Stickler syndrome (SS) is a rare, inherited disease that is the highest risk condition known to predispose eyes to rhegmatogenous retinal detachment (RRD), with a lifetime risk of approximately 65%.1,2 This report briefly reviews the etiology of RRD and the current state of RRD preventive efforts. It then discusses the implications of recent successful prevention treatments in Stickler syndrome for high-risk eyes with other, non-syndromic conditions.3–5
Without treatment, spontaneous detachment of the (neurosensory) retina from the eye wall is the leading cause of acute blindness in the aging eye. Treatment became possible only during the 20th century, after Jules Gonin proved that a full thickness defect in the retina allowed vitreous cavity fluid to enter the potential subretinal space (Figure 1).6 Countless millions undoubtedly went blind in one or both eyes from even microscopic retinal defects during prior centuries.
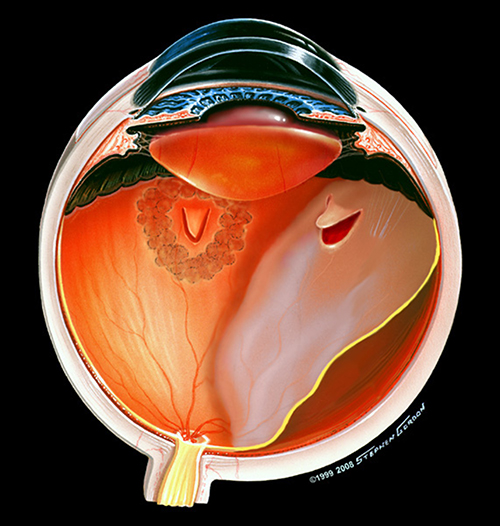 |
Figure 1 Illustration of retinal detachment caused by a new tear in normal appearing retina, in an eye that had previously received successful focal laser for a retinal tear in attached retina elsewhere. Used with permission of artist Stephen Gordon ©1999. |
The majority of retinal defects that produce RRD are tractional tears resulting from the forces generated by vitreous gel movements, coincident with or subsequent to posterior vitreous detachment (PVD).7 These forces are transmitted to the retina predominately at the vitreous base, extending from 2 mm anterior to the ora serrata to 3 mm posterior to it.8 Over 90% of such causative tears, atrophic holes, and lattice degeneration occur anteriorly, in retina that provides only far peripheral vision (Figure 1).9 Therefore, treatments to the peripheral retina typically do not produce substantial visual disability, even if they result in retinal scarring.3
This critically important point provides the basis for prophylactic treatments to either reduce vitreous traction forces on the peripheral retina by indenting (buckling) the eye wall; or to strengthen peripheral retinal adherence to the eye wall (retinopexy), or both.10 Vitrectomy removal of vitreous gel could theoretically reduce traction forces without changing the peripheral retina, but it has only recently been described in a form that could likely achieve a net reduction in long-term RRD risk vs the non-vitrectomized eye.11
As an intraocular procedure, vitrectomy involves an additional risk of endophthalmitis, albeit small.12 Both buckling and vitrectomy are invasive, leaving retinopexy as the only noninvasive treatment for RRD prophylaxis.
Retinopexy Prophylaxis
Cryotherapy was the primary form of retinopexy prophylaxis from its introduction in 1964,13 until the advent of laser retinopexy in 1970.14 Although laser retinopexy can be more precisely placed, with better intensity control, it predominated only gradually until its application to the peripheral retina was substantially improved by the introduction of indirect ophthalmoscope (IDO) delivery during the 1990s.15
Nevertheless, over 50 years after the introduction of laser retinopexy, no randomized clinical trial of its use for prophylaxis has been forthcoming.16,17 RRD prophylaxis thus remains mostly a matter of judgement by the physician and the informed patient, aided by retrospective studies and literature analysis.16
It is commonly accepted that symptomatic tears should be treated, but focal prophylactic treatment of asymptomatic, non-traumatic, predisposing lesions (defects and lattice degeneration*) is still not supported by “strong” evidence and is usually not recommended.16 Given an option, however, many patients prefer focal treatment (Figure 2) over lifetime observation of potentially causative lesions, since it involves minimal risk and morbidity.18
 |
Figure 2 Image of pigmented lattice degeneration at the equator of the left eye, treated one month previously at the patient’s request with focal IDO laser prophylaxis, concurrent with repair of a retinal detachment in the right eye, under laryngeal mask anesthesia. Used with permission of Retina Specialists of Alabama LLC. |
Physicians are duty bound to search for such visible predisposing lesions in the course of routine eye examinations, but it is understood that the majority of causative tears occur in normal appearing (peripheral) retina.19 This led Byer to conclude that, “If we cannot predict the danger sites, we cannot prevent detachment.”20 After also citing the above,19 Wilkinson further stated that
A demonstration that vitreoretinal lesions increase risk does not justify the treatment of these disorders in the absence of scientific evidence that the therapy genuinely lowers the rate of subsequent retinal detachment.21
*Foos found that eyes with lattice degeneration harbored tears in 17% of autopsy eyes vs only 2% of all eyes.9
But for high-risk eyes, especially in partially sighted individuals for whom RRD could be catastrophic, there is another path than abandoning such focal retinopexy. It is a path that has often been utilized, but without “strong” evidence heretofore16,17 - treat visible predisposing lesions in the peripheral retina and add encircling (360 degrees) grid laser retinopexy to the normal-appearing, but at-risk peripheral retina elsewhere.
The frustration of seeing RRD occurring from new defects elsewhere (Figure 1) in fact led some early retinologists to supplement rather than abandon focal treatment of visible lesions by adding such encircling laser grid prophylaxis to the peripheral retina. Using only a slit lamp and a mirrored contact lens,22,23 they achieved some notable successes,24,25 but their technique was difficult, typically left untreated retina anteriorly, and was not widely adopted.26
Recognizing that IDO laser delivery enabled more effective peripheral retinopexy,15 we pursued encircling prophylaxis for certain high-risk eyes during the 1990s. We presented our work to the first meeting of the (newly named) American Society of Retina Specialists (ASRS) in 2002. Subsequent ASRS surveys indicate that approximately half of members have since performed encircling laser prophylaxis.
After coalescent treatment of visible defects and lattice degeneration, we treated the peripheral retina to the ora 360 degrees (sparing the long ciliary nerves at 3 o’clock and 9 o’clock) with a grid of laser burns of moderate intensity, spaced one to two spot widths apart. In effect, we were producing a “second ora” posterior to the vitreous base27,28 (to be protective during possible PVD) and posterior to treatment applied to all high-risk peripheral retina (Ora Secunda Cerclage, OSC, Figure 3).29,30
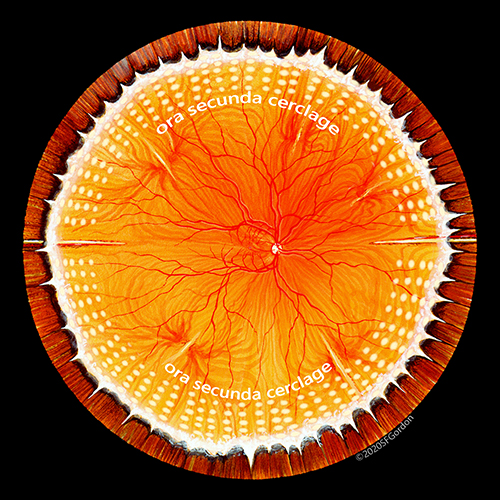 |
Figure 3 Illustration of “standard” ora secunda cerclage (OSC) that in our experience has proven successful in non-syndromic eyes for more than two decades. Used with permission of artist Stephen F Gordon ©2020. |
The vortex vein ampullae (VVA) are key IDO landmarks approximating the anatomical equator.31 Laser burns should approach the ora from a posterior starting position at least halfway back from the ora to the VVA, or even as far posteriorly as the actual VVA, according to the treating ophthalmologist’s judgment. The VVA themselves are avoided. In our experience, this pattern has been safe and effective, however we learned that OSC against giant retinal tear (GRT) required tighter grid placement (one spot width spacing), with slightly higher intensity burns, crossing the ora to include the anterior vitreous base.3
The goal of OSC is to bond the entire at-risk peripheral retina to the eye wall with sufficient strength to withstand vitreous traction forces that could otherwise cause tears and detachment. Properly controlled laser retinopexy achieves a bond three to five times as strong as unprotected retina,32 with maximum strength developing over approximately one month.
Strong Evidence from Stickler Syndrome
The extremely high risk of RRD at a young age in Stickler syndrome (30%, or half, occurring before age 20)1,2 caused the Cambridge group to begin encircling retinopexy using cryopexy at the ora to prevent GRT, more than 40 years ago. In 2014, they reported at least a five-fold decrease in Stickler RRD with such encircling cryopexy at the ora (an eight-fold decrease in fellow eyes), using individually matched, untreated eyes as controls.2 There were no clinically significant complications after these noninvasive procedures, including no development of epimacular membranes.
In January 2021, we reported in detail an effective encircling laser retinopexy technique for prophylaxis of Stickler RRD, in five eyes of a single family (Supplementary Video) genetically and clinically proven to be at high risk for RRD, emulating the Cambridge cryopexy,3 Moreover, our technique (Ora Secunda Cerclage/Stickler Syndrome, OSC/SS) extended more posteriorly, between the VVA, preventing even the small, posterior tears frequently seen in Stickler detachments, without symptomatic loss of peripheral vision. With a mean follow-up now of 10.5 years in the five treated eyes (including three fellow eyes), none have developed RRD. Twenty-four additional (genetically confirmed type 1 or type 2) SS eyes have since been treated with OSC/SS with none suffering subsequent RRD. We are currently designing a prospective, non-randomized clinical trial of the OSC/SS technique to facilitate cohort comparison studies.3,33
Naravane et al and Khanna et al subsequently reported similarly large reductions in RRD rates in (predominately clinically diagnosed) SS, in larger series, using a form of encircling laser retinopexy extending to approximately the equator (26.7% vs 4.6%, p = 0.034; 73% vs 3%, p = 0.001, respectively).4,5 Linton et al recently reported a fourth encircling laser prophylaxis study for (predominately genetically confirmed) SS, confining treatment to the ora region as a GRT prophylaxis.34 RRD was reduced from 23% to 9% (p = 0.057), with no GRT lesions seen in the eyes that detached despite prophylaxis (vs 42.9% GRT in control eyes detaching). Along with the Cambridge study it emulated, this conclusively illustrates the ability of encircling prophylaxis to prevent GRT as the ultimate PVD injury to the retina;34 and also explains its demonstrated effectiveness in preventing lesser tears during PVD when treatment is extended posteriorly to encompass the entire vitreous base.3–5 None of these studies noted significant treatment complications. Importantly, a trend in all SS encircling prophylaxis studies was a lower rate of RRD failure as prophylaxis was extended posteriorly.
The high rate of RRD in SS, beginning at a young age,1,2 and occurring in a genetically defined and identifiable condition, provides a unique opportunity to document a large preventive affect versus the natural course.2–5,33,34 Moreover, the prophylaxis experience in SS is directly applicable to non-syndromic, aging eyes since SS detachments typically result from the same pathogenesis - vitreous traction tears in the peripheral retina. Encircling laser retinopexy usually succeeds by preventing these tears, as the treated neurosensory retina becomes in effect a part of the eye wall, withstanding vitreous traction.
At least eleven earlier reports of encircling laser prophylaxis effectiveness in non-syndromic eyes have gone largely unremarked for decades. Although they have individually not been regarded as strong proof, in their totality they now add to the credibility of the recent SS successes, and they will be reviewed in a sequel to this article.
Conclusion
Despite numerous calls for randomized clinical trials of RRD prophylaxis, none have materialized during a half century since the advent of laser retinopexy.16,17,21 However, the large, long duration, case-controlled Cambridge SS study now clearly provides strong evidence of encircling retinopexy safety and effectiveness for any asymptomatic eyes that are deemed to be at high risk for RRD from giant retinal tear.2 Moreover, four subsequent laser retinopexy studies of SS prophylaxis together demonstrate both equivalency to the Cambridge cryopexy procedure,3–5,34 and the ability to protect the entire peripheral retina against more posterior tears, regardless of PVD status.3–5 Thus, randomizing high-risk eyes to no treatment in continued pursuit of stronger evidence has become ethically questionable.3,35
Focal retinopexy prophylaxis minimizes a predisposing lesion’s ability to thereafter cause RRD, but it affords no protection of untreated retina elsewhere. This is accomplished for eyes at high risk for peripheral tears by encircling grid laser retinopexy that is finally a proven effective prophylaxis in the highest risk condition of all, Stickler syndrome.
It is obviously more difficult to define “high risk” in non-syndromic eyes, and we do not purport to do so here. But with strong SS prophylaxis evidence in hand, increased efforts to define “high risk” non-syndromic eyes by their natural course will ensue, along with increased recognition of partially sighted individuals to whom (another) RRD poses an avoidable threat of legal blindness, and who thus have less risk tolerance.
As data are collected and analyzed for future cohort comparison studies of prophylaxis in non-syndromic eyes, it will remain the responsibility of each physician and each informed patient to assess risk and risk tolerance with the data then available – but hence forward, in an environment in which safe and effective encircling prophylaxis is appropriately recognized.
Many reports of encircling laser prophylaxis give little description of technique.4,5,36,37 But its safety and effectiveness can be quite technique dependent. We plan to publish a comprehensive description of optimal technique in a sequel to this article.
While espousing a more interventional approach to RRD prevention, we also recognize treatment risks. Laser treatment permanently changes the retina, and it should be applied with skill and great care – as much as necessary, but as little as possible. It is not a minor procedure. It is the surgeon’s permanent laser signature.
Acknowledgments
Christina Sullivan, Laura Beckwith, Dewayne Conn, and Jessica Haynes have provided substantial assistance in manuscript preparation, administration, and clinical care, for which we are grateful.
Funding
Support for this article was provided by the Helen Keller Foundation for Research and Education, through grants from the Hanna Charitable Trust and the Kent Companies of Midland, Texas.
Disclosure
The authors report no conflicting interests with respect to this study. Dr. Robert Morris is President of the Helen Keller Foundation for Research and Education, Birmingham, Alabama, USA. Dr. Ferenc Kuhn is the Foundation’s Director of Clinical Research and Chairman of the International Society of Ocular Trauma. Drs. Morris and Kuhn are vitreoretinal surgeons and longtime research collaborators in ocular trauma, macular surgery, endophthalmitis, and retinal detachment. Dr. Timothy Sipos is a senior fellow at Retina Specialists of Alabama, Birmingham, Alabama, USA.
References
1. Parma ES, Körkkö J, Hagler WS, Ala-Kokko L. Radial perivascular retinal degeneration: a key to clinical diagnosis of an ocular variant of stickler syndrome with minimal or no systemic manifestations. Am J Ophthalmol. 2002;134(5):728–734.
2. Fincham GS, Pasea L, Carroll C, et al. Prevention of retinal detachment in stickler syndrome. The Cambridge prophylactic cryotherapy protocol. Ophthalmology. 2014;121(8):1588–1597. doi:10.1016/j.ophtha.2014.02.022
3. Morris RE, Parma ES, Robin NH, et al. Stickler Syndrome (SS): laser prophylaxis for retinal detachment (modified Ora Secunda Cerclage, OSC/SS). Clin Ophthalmol. 2021;15:19–29. PMID: 33447008; PMCID: PMC7802593. doi:10.2147/OPTH.S284441
4. Naravane AV, Belin PJ, Pierce B, Quiram PA. Risk and prevention of retinal detachments in patients with stickler syndrome. Ophthalmic Surg Lasers Imaging Retina. 2022;53(1):7–11. PMID: 34982001. doi:10.3928/23258160-20211213-02
5. khanna S, Rodriguez SH, Blair MA, Wroblewski K, Shapiro MJ, Blair MP. Laser prophylaxis in patients with stickler syndrome. Ophthalmol Retina. 2022;6(4):263–267. PMID: 34774838. doi:10.1016/j.oret.2021.11.001
6. Gonin J. Detachment of the retina and its treatment. Trans Ophthalmol Soc U K. 1931;50:531.
7. Wilkinson CP. Phakic retinal detachments in the elderly. Retina. 1995;15(3):220–223. PMID: 7569349. doi:10.1097/00006982-199515030-00006
8. Sebag J. Anatomy of the Eye, vitreous base. In: Dartt D, editor. Encyclopedia of the Eye. Academic Press; 2010.
9. Foos RY. Tears of the peripheral retina; pathogenesis, incidence and classification in autopsy eyes. Mod Probl Ophthalmol. 1975;15:68–81. PMID: 1160919.
10. Ripandelli G, Rossi T, Pesci FR, Cecere M, Stirpe M. The prophylaxis of fellow-eye retinal detachment in stickler syndrome: a retrospective series. Retina. 2022;42(2):250–255. PMID: 34534992. doi:10.1097/IAE.0000000000003304
11. Morris RE. Vitreous Opacity Vitrectomy (VOV): safest possible removal of “floaters”. Clin Ophthalmol. 2022;16:1653–1663. PMID: 35673347; PMCID: PMC9167598. doi:10.2147/OPTH.S361557
12. Oshima Y, Kadonosono K, Yamaji H, et al. Japan microincision vitrectomy surgery study group: multicenter survey with a systematic overview of acute-onset endophthalmitis after transconjunctival microincision vitrectomy surgery. Am J Ophthalmol. 2010;150(5):716–725.e1. doi:10.1016/j.ajo.2010.06.002
13. Lincoff HA, McLean JM, Nano H. Cryosurgical treatment of retinal detachment. Trans Am Acad Ophthalmol Otolaryngol. 1964;68:41.
14. Little HL, Zweng HC, Peabody RR. Argon laser slit lamp retinal photocoagulation. Trans Amer Acad Ophthal Otolaryngol. 1970;74:85–97.
15. Friberg TR. Clinical experience with a binocular indirect ophthalmoscope laser delivery system. Retina. 1987;7(1):28–31. doi:10.1097/00006982-198707010-00006
16. American Academy of Ophthalmology Preferred Practice Pattern. Preferred Practice Guidelines. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration. San Francisco, CA: American Academy of Ophthalmology; 2019. Available from: www.aao.org/ppp.
17. Ang GS, Townend J, Lois N. Interventions for prevention of giant retinal tear in the fellow eye. Cochrane Database Syst Rev. 2009;2:CD006909. PMID: 19370659. doi:10.1002/14651858.CD006909
18. Mester U, Volker B, Kroll P, Berg P. Complications of prophylactic argon laser treatment of retinal breaks and degenerations in 2000 eyes. Ophthalmic Surg. 1988;19(7):482–484. PMID: 3412760.
19. Benson WE, Grand MG, Okun E. Aphakic retinal detachment. Management of the fellow eye. Arch Ophthalmol. 1975;93:245–249. doi:10.1001/archopht.1975.01010020255001
20. Byer NE. Evidence-based analysis of prophylactic treatment of asymptomatic retinal breaks and lattice degeneration; invited commentary: against treatment. Ophthalmology. 2000;107:15–16. doi:10.1016/S0161-6420(99)00066-4
21. Wilkinson CP. Evidence-based analysis of prophylactic treatment of asymptomatic retinal breaks and lattice degeneration. Ophthalmology. 2000;107(1):12–5;discussion 15–8. PMID: 10647712. doi:10.1016/s0161-6420(99)00049-4
22. Stein R, Pinchas A, Treister G. Prevention of retinal detachment by a circumferential barrage prior to lens extraction in high-myopic eyes. Ophthalmologica. 1972;165(2):125–136. PMID: 4641053. doi:10.1159/000308478
23. Pollack A, Milstein A, Oliver M, Zalish M. Circumferential argon laser photocoagulation for prevention of retinal detachment. Eye. 1994;8(4):419–422. doi:10.1038/eye.1994.99
24. Haut J, Monin C, Diner-Nedey S, Van Effenterre G. Prévention de la bilatéralisation du décollement de rétine idiopathique par un traitement au laser à l’argon [Prevention of bilateralization of idiopathic retinal detachment by treatment with argon laser]. J Fr Ophtalmol. 1987;10(11):717–722. French. PMID: 3448127.
25. Madelain J, Turut P. Résultats du traitement prophylactique systématique au laser argon après décollement de rétine idiopathique [Results of systematic preventive treatment with argon laser after idiopathic retinal detachment]. Bull Soc Ophtalmol Fr. 1990;90(2):141–147. French. PMID: 2192808.
26. Bonnet M, Aracil P, Carneau F. Rhegmatogenous retinal detachment after prophylactic argon laser photocoagulation. Graefes Arch Clin Exp Ophthalmol. 1987;225(1):5–8. doi:10.1007/BF02155795
27. Heller MD, Straatsma BR, Foos RY Tractional degenerations of the peripheral retina.
28. Wang J, McLeod D, Henson DB, Bishop PN. Age-dependent changes in the basal retinovitreous adhesion. Invest Ophthalmol Vis Sci. 2003;44(5):1793–1800. doi:10.1167/iovs.02-0802
29. Morris R, Witherspoon CD, Kuhn F, Sapp M. Retinal detachment laser prophylaxis. (By invitation). Retina Today. 2008;2008:63–66.
30. Morris RE, Shere JL, Witherspoon CD, et al. Intraoperative retinal detachment prophylaxis in vitrectomy for retained cataract fragments. J Cataract Refract Surg. 2009;35(3):491–495. PMID: 19251143. doi:10.1016/j.jcrs.2008.11.037
31. Sohn EH, Strohbehn A, Stryjewski T, et al. Posteriorly inserted vitreous base: preoperative characteristics, intraoperative findings, and outcomes after vitrectomy. Retina. 2020;40(5):943–950. PMID: 30883531; PMCID: PMC6697230. doi:10.1097/IAE.0000000000002482
32. Zauberman H, Berman ER. Measurement of adhesive forces between the sensory retina and the pigment epithelium. Exp Eye Res. 1969;8(3):276–283. PMID: 4240714. doi:10.1016/s0014-4835(69)80039-4
33. Carroll C, Papaioannou D, Rees A, Kaltenthaler E. The clinical effectiveness and safety of prophylactic retinal interventions to reduce the risk of retinal detachment and subsequent vision loss in adults and children with stickler syndrome: a systematic review. Health Technol Assess. 2011;15(16):iii–xiv, 1–62. PMID: 21466760; PMCID: PMC4781556. doi:10.3310/hta15160
34. Linton E, Jalil A, Sergouniotis P, et al. Laser prophylaxis in stickler syndrome: the Manchester protocol. Retina. 2022. PMID: 36165842. doi:10.1097/IAE.0000000000003634
35. Alexander P, Snead MP. Prevention of blindness in stickler syndrome. Genes. 2022;13(7):1150. PMID: 35885933; PMCID: PMC9318672. doi:10.3390/genes13071150
36. Koh HJ, Cheng L, Kosobucki B, Freeman WR. Prophylactic intraoperative 360° laser retinopexy for prevention of retinal detachment. Retina. 2007;27(6):744–749. doi:10.1097/IAE.0b013e318030ebd7
37. Verhoekx J, van Etten P, Wubbels R, van Meurs J, van Overdam K. Prophylactic laser treatment to decrease the incidence of retinal detachment in fellow eyes of idiopathic giant retinal tears. Retina. 2020;40(6):1094–1097. doi:10.1097/IAE.0000000000002494
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.