Back to Journals » Clinical Interventions in Aging » Volume 16
Prevalence of Severe Neurocognitive Impairment and Its Association with Socio-Demographics and Functionality Among Ugandan Older Persons: A Hospital-Based Study
Authors Atim LM, Kaggwa MM ![]() , Mamun MA
, Mamun MA ![]() , Ashaba S
, Ashaba S ![]() , Maling S
, Maling S
Received 12 May 2021
Accepted for publication 30 June 2021
Published 22 July 2021 Volume 2021:16 Pages 1415—1425
DOI https://doi.org/10.2147/CIA.S319891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Letizia Maria Atim,1,* Mark Mohan Kaggwa,1,2,* Mohammed A Mamun,3,4 Scholastic Ashaba,1 Samuel Maling1
1Department of Psychiatry, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2African Centre for Suicide Prevention and Research, Mbarara, Uganda; 3CHINTA Research Bangladesh (Centre for Health Innovation, Networking, Training, Action and Research – Bangladesh), Savar, Dhaka, 1342, Bangladesh; 4Department of Public Health and Informatics, Jahangirnagar University, Savar, Dhaka, 1342, Bangladesh
*These authors contributed equally to this work
Correspondence: Mark Mohan Kaggwa; Mohammed A Mamun Tel +88-1738592653
Email [email protected]; [email protected]
Background: The prevalence of neurocognitive disorders, especially dementia, is rising due to an increase in longevity. Early detection and diagnosis of neurocognitive impairments are important for early interventions and appropriate management of reversible causes, especially by the primary health workers. However, this study aimed to determine the prevalence and associated factors of severe neurocognitive impairment among elderly persons attending a tertiary hospital in Uganda.
Methods: This cross-sectional survey was conducted in a Ugandan hospital setting, where older adults go for treatment for their chronic health problems. Following the inclusion criteria, interviews were conducted, where information about socio-demographics was collected, whereas neurocognitive impairment and functionality were assessed by Mini-Mental State Examination and Barthel Index, respectively. Chi-square test, Pearson correlation test, and logistic regression were performed to determine the factors associated with severe neurocognitive impairment.
Results: A total of 507 elderly persons aged 60 years and above were enrolled in this study (mean age 68.62 ± 7.95 years), and the prevalence of severe neurocognitive impairment was 28.01%. Advanced age, female gender, lower education level, and functional dependency were significantly associated with severe neurocognitive impairment.
Conclusion: Severe neurocognitive impairment is prevalent among Ugandan hospital attending elderlies with functional dependency. This suggests a need to routinely screen cognitive disorders among older persons who visit the healthcare facilities with other physical complaints to enable early detection and treatment of reversible causes of neurocognitive impairment, such as depression and delirium to enable better functionality.
Keywords: dementia, neurocognitive disorder, functionality, prevalence and associated factors, early diagnosis, Barthel Index, Mini-Mental Status Examination, Ugandan elderly
Introduction
Neurocognitive disorder such as dementia involves the impairment of one or more cognitive domains and interference with the level of functionality. Neurocognitive impairment is one of the major global health problems in the ever-growing ageing societies.1 Worldwide about 50 million people have dementia, 60% from low-income countries like Uganda, where the present study was carried out.2 The number is estimated to reach 82 million in the year of 2030 and 152 million in 2050, considering the rapid growth rate of the older persons.2,3 Despite the increase in the prevalence of neurocognitive impairment globally, the burden varies across regions. This disparity is attributed to different factors, such as age, gender, education levels, area of residence, ethnic groups, cultural differences, diet habits, and tradition of living.4,5 In addition, physical conditions, like HIV/AIDS, hypertension, diabetes, and stroke, are also found as risk factors for the increment of neurocognitive disorders.6 Major neurocognitive disorders are characterized by significant functional decline and dependence,7 which impacts neurological symptoms of dementia, such as incontinence, tremors, ataxia, etc.8 Patients are taken to the hospital, especially when their functionality starts to decline, other than a fall in cognition which is considered a normal aging process by many caretakers.9,10 In extreme cases, functional dependence leads to early mortality in older adults with neurocognitive disorders.11
Nowadays, the number of older persons (aged 60 years and above) is increasing globally due to the improvement in medical care and services;12 and Uganda is not an exception to the scenario.13 However, many older persons who visit healthcare facilities for medical conditions (well-established neurocognitive disorder risk factors), such as diabetes, hypertension, HIV care, stroke, etc., are not usually assessed for neurocognitive impairment.10,14 Early diagnosis and detection of neurocognitive impairment are important because early interventions delay functional dependence, and reversible causes like depression can be detected and managed appropriately.15 With early detection, the primary healthcare workers can anticipate potential problems associated with the neurocognitive impairment progression and influence his decision regarding further management such as either referral for further management or management of the treatable causes, such as depression, delirium, etc.15,16 Early detection might also help older persons and their caretakers in making further diagnostic and treatment decisions.15–17 In addition, early diagnosis of neurocognitive impairment improves the quality of life of the patient, reduces economic burden related to the medical care of delayed diagnosis, delays the progress of neurocognitive decline by appropriate treatment, manages the treatable causes, and helps caretakers prepare for the long caring journey.18 Despite the growing knowledge of neurocognitive impairment, early diagnosis is rare until individuals have severe functional decline and are at late stages of the dysfunction.19
In Uganda, studies investigating severe neurocognitive impairment were conducted mainly among people below 60 years living with HIV.20–24 The neurocognitive disorder explored commonly was HIV-acquired neurocognitive disorder, whose prevalence ranged from 41 to 58%.20–24 However, a recent community-based study involving the general population; in Uganda aged 60 years about neurocognitive disorders, particularly Alzheimer’s disease, found the prevalence to be at 20%, but its relationship with functional decline was not explored.25 Therefore, the present study aimed to investigate the prevalence and sociodemographic factors and functional dependence associated with severe neurocognitive impairment within the older persons attending a tertiary hospital in southwestern Uganda.
Methods
Study Setting
A hospital-based survey was conducted at Mbarara Regional Referral Hospital (MRRH), a tertiary hospital located in Mbarara city, southwestern Uganda. MRRH is currently the biggest referral hospital in southwestern Uganda, attending approximately 600 elderly people every month as inpatient and outpatient.
Participants and Sample Size
Older persons of both gender (aged 60 years and above) attending the outpatient department of MRRH in February, 2021, were enrolled in this study. The participants with sensory impairment such as being deaf or dumb were excluded from this study. However, the minimum sample size of 246 older persons was arrived at based on the Leslie26 formula for the prevalence studies at 95% confidence interval and power of 80% and substituting a prevalence of dementia of 20% determined in a previous study in southwestern Uganda.25
Data Collection
The participants were recruited consecutively as they came to the hospital for their outpatient appointments. All the tools were compiled in a single questionnaire that was also translated into the local language and back-translated into English. Trained research assistants collected data, and each interview took about 20 minutes to complete. However, the sociodemographic characteristics, such as age, gender, area of residence, marital status, occupational status (ie, previously formally vs informally employed and currently active vs inactive, or retired), level of education, type of housing, and presence of chronic illness such as hypertension, diabetes, stroke, etc., were asked in the survey. Besides, neurocognitive impairment was based on the MiniMental State Examination (MMSE), whereas the Barthel Index (BI) was used to assess the level of functionality.
Study Measures
Mini–Mental State Examination
The MMSE, also called the Folstein test, was used to screen for cognitive impairment.27,28 The MMSE is used for examining different cognitive functions including registration (repeating named prompts), attention and calculation, recall, language, ability to follow simple commands and orientation. It is mainly verbal except for one section that requires a patient to draw a simple diagram. Its advantage is that it does not require specialized equipment or training for administration. A cut-off of 17 and below signifies severe neurocognitive impairment, 18 to 23 represents mild neurocognitive impairment, and above 24 signifies no neurocognitive impairment.27,28 The language in the MMSE was modified to fit the local context and was administered by the research assistant fluent in the local language. A cutoff of 17 indicates severe neurocognitive disorder irrespective of the education status or age of the participants. However, in this study, the Cronbach’s alpha was 0.78.
Barthel Index
The level of functionality was tested using the BI. The BI is composed of 10 items with varying weights.29 Two items regarding personal care (wash face, comb hair, shave, and clean teeth) and bathing are evaluated with a 2-score scale (0 and 5 points); 6 items regarding feeding, getting onto and off the toilet, ascending and descending stairs, dressing, controlling bowels, and controlling bladder are evaluated with a 3-score scale (0, 5, and 10 points); and 2 items regarding moving from wheelchair to bed and returning, and walking on a level surface are evaluated with a 4-score scale (0, 5, 10, and 15 points). The BI is a cumulative score calculated by summing each item score. The BI scores are multiples of 5 with a range of 0 (completely dependent) to 100 (independent of basic ADL). Higher scores represent a higher degree of independence.29 The score was categorized into 5 groups 0–20 = total dependency, 21–60 = severe dependency, 61–90 = moderate dependency, 91–99 = slight dependency, and 100 = complete independence. The Cronbach’s alpha of this study was 0.88.
Ethical Consideration
This study’s formal ethical approval was obtained from the Mbarara University of Science and Technology research ethics committee (MUSTREC#05/11-20). Besides, administrative clearance to conduct the study was obtained from the director of Mbarara regional referral hospital. Participants who agreed to participate in this study would either append their signature or thumbprint on the consent form. Participants received 5000 Ugandan Shilling to compensate for their time, and in addition they received a bar of soap as a token of appreciation. Participants diagnosed with severe neurocognitive impairment were referred to the psychiatry department for further management and investigation.
Statistical Analysis
Data were initially entered in an Excel sheet, which was exported to STATA 16.0 for the final analysis. The means and standard deviations for normally distributed continuous variables and percentages for categorical variables were used as the descriptive statistics. The Gaussian assumption was used to assess for normality based on the Shapiro–Wilks test and histograms. Chi-square test for categorical variables or Student’s t-tests for continuous variables were performed to determine significant differences between individuals with severe neurocognitive impairment and those without. Pearson correlation coefficient was used to ascertain the relationship between severe neurocognitive impairment, functional dependency, other study variables. Considering the severe neurocognitive impairment as the dependent variable, its associations with socio-demographics were presented by logistic regression tests. Factors significant at bivariate logistic analysis were tested for collinearity using variance inflation factor (VIF). Those with a VIF below three were included in the final model at multiple logistic regression. The significant level was at less than 5% for a 95% confidence interval.
Results
Characteristics of the Participants
A total of 507 participants were recruited to this study, whose mean age was 68.62 (±7.95) years. Participants were predominantly female (60.52%), living in rural areas (75.40%), and married (54.96%) (Table 1). However, the prevalence of severe neurocognitive impairment was 28.01% (n=142) considering 17 and below as cut-off point.
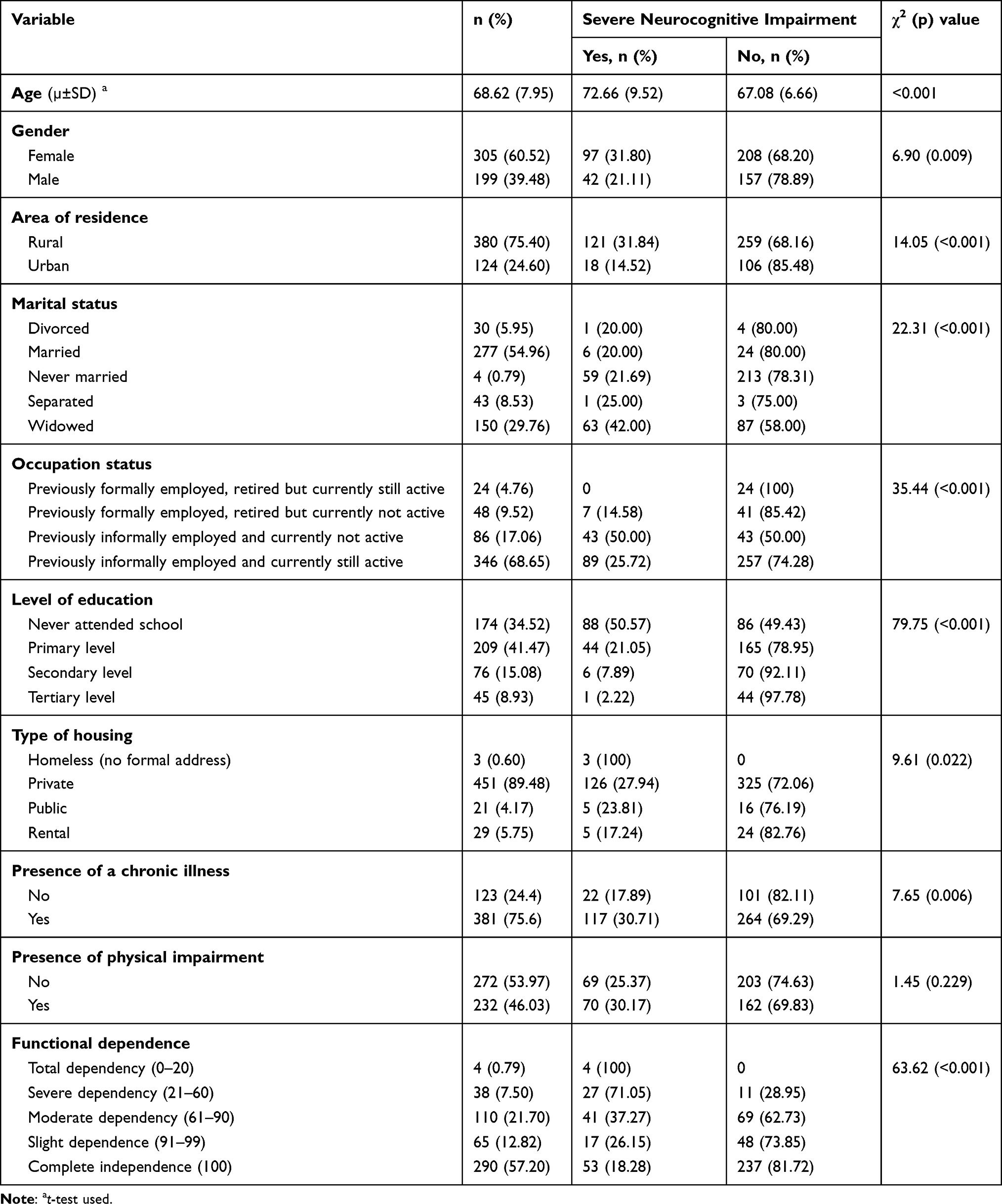 |
Table 1 The Associations Between the Studied Variables with Severe Neurocognitive Impairment |
Relationship Between Severe Neurocognitive Impairment and Studied Variables
There was a statistically significant difference between individuals with severe neurocognitive impairment and those without, among all of the studied variables except the presence of physical impairment (χ2=1.45, p=0.229). About 31.80% of females had a severe neurocognitive impairment, whereas it was 21.11% for male participants (χ2=6.90, p=0.009). Severe neurocognitive impairment was lower among participants with a higher level of education (χ2=79.75, p<0.001), and rural dwellers (31.84% vs 14.52% urban dweller participants; χ2=14.05, p<0.001). Similarly, there were significant relationships between marital status and occupational status with severe neurocognitive impairment (χ2=22.31, p<0.001, and χ2=35.44, p<0.001, respectively). About 30.17% of elderlies with chronic disease had a severe neurocognitive impairment, but it was 17.89% for those who had no chronic disease (χ2=7.65, p=0.006). For details about the association of the socio-demographic characteristics with severe neurocognitive impairment, please see Table 1.
Relationship Between Severe Neurocognitive Impairment, Functional Dependence and Other Study Variables
All of the participants who reported being totally functionally dependent had severe neurocognitive impairment, and the trend increased with the severity of dependency (χ2=63.62, p<0.001) (Figure 1). From the correlation test, a similar finding was also reported; that is, a low positive correlation between neurocognitive impairment and functional independence was found (r = 0.46, p <0.001), meaning that the individuals with neurocognitive impairment have a higher dependency.
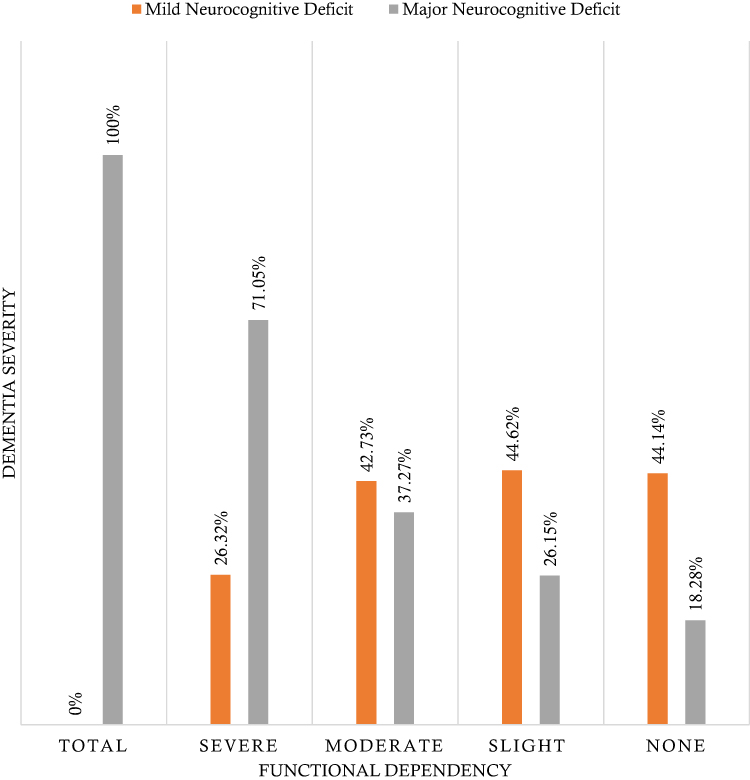 |
Figure 1 Relationship between functional dependency and neurocognitive impairment. |
Highest level of significant correlation at less than 0.001 was between neurocognitive impairment and level of education (r2 = 0.50). Other statistically significant correlations between variables had lower correlation coefficients, ie, 0.31 for both (age and functional dependence) and (age and neurocognitive impairment). The rest of the significant correlations were negligible (Table 2).
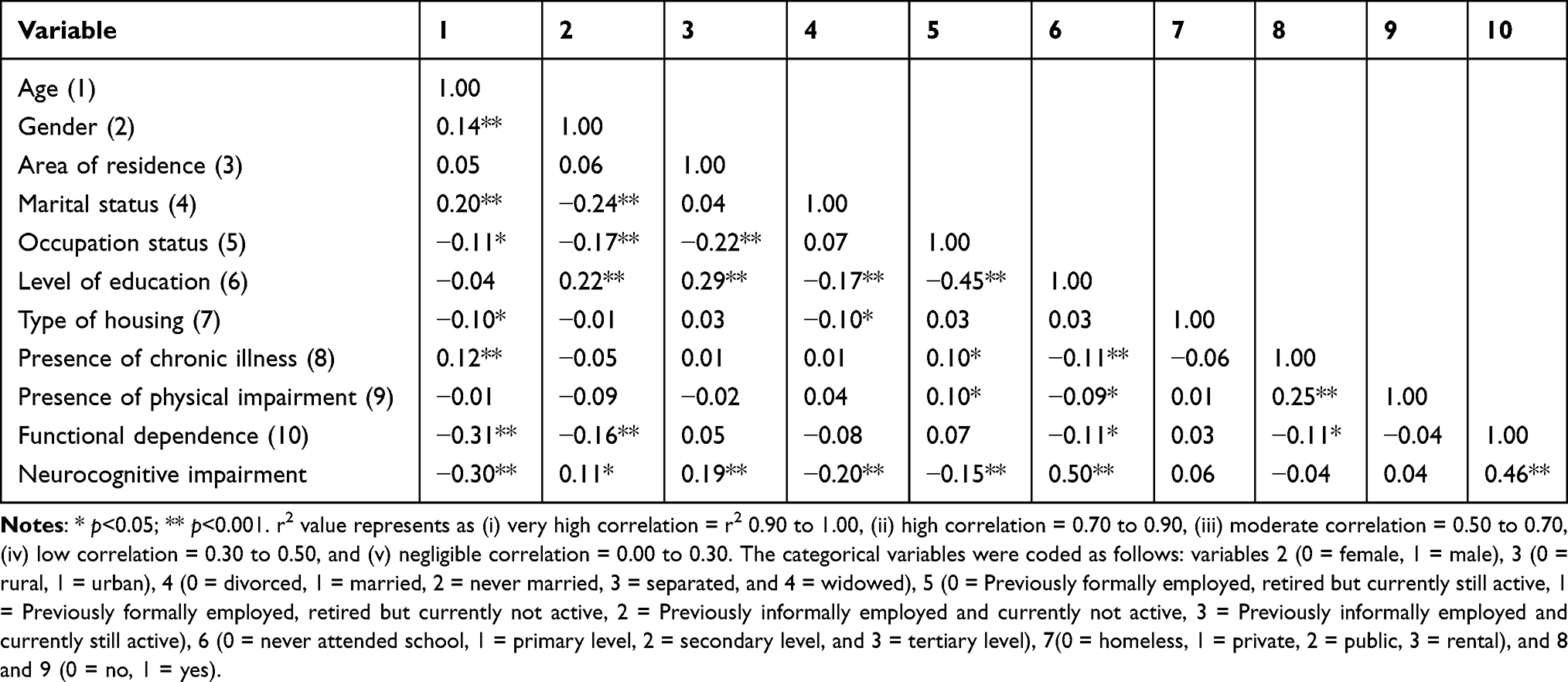 |
Table 2 Correlation Between Study Variables |
Factors Associated with Severe Neurocognitive Impairment
On bivariate analysis, statistically significant association of severe neurocognitive impairment was with age, female gender, rural residence, being widowed, being previously informally employed and currently not active, having attained any level of education, presence of chronic illness, and functional dependence. After testing for multicollinearity among the significant variables in bivariable logistic regression, the final model had a sensitivity of 92.60, specificity 50.00, goodness-of-fit p-value 0.186, and all the included variables had a mean VIF of 1.20, non-above 3. These covariates were entered simultaneously into a multivariable logistic regression model. After backward stepwise logistic regression, the following factors significantly increased the likelihood of having dementia: age [adjusted odds ratio (aOR) = 1.08, 95% confidence interval (CI) (1.04–1.12)], female gender [aOR = 2.29, CI (1.29–4.09)], and functional dependence – severe [aOR = 7.63, CI = (2.91–20.04)] and moderate [aOR = 1.98, CI = (1.11–3.55)]. The likelihood of having severe neurocognitive impairment significantly reduced with increase of education level, [ie, 0.34 (0.20–058), 0.10 (0.03–0.27), and 0.04 (0.04–0.37), for primary, secondary and tertiary level of education, respectively] (Table 3).
 |
Table 3 Logistic Regression Analysis for Factors Associated with Severe Neurocognitive Impairment |
Discussion
In this survey of elderly persons attending a Ugandan tertiary hospital, 28% severe neurocognitive impairment prevalence was reported; which was higher than a recent community-based study conducted among the same age group in the country’s southwestern part (20%).25 The high prevalence is attributed to the study being conducted in a hospital sitting; hence, more elderly individuals with neurocognitive impairment might have suffered from chronic conditions. Also, our study used MMSE for screening for severe neurocognitive impairment that gives higher prevalence estimates considering participants' age and education level and not considering functionality as part of the confirmation of the diagnosis. In the neighboring country, Tanzania, an 8.9% severe neurocognitive impairment (ie, dementia) rate was detected among individuals aged 70 years and above, an increase from 6.4% in 2010.30 In addition, 6.0% (95% CI = 5.0–8.0) of dementia was estimated in a systematic review of East African studies.31 Evidently, higher portion of the participants reported suffering from severe neurocognitive impairment in this study; which may be because of sample characteristics being hospital-based who came to get treatment for chronic diseases. Chronic diseases are associated with major causes of neurocognitive decline, such as delirium, depression, and the effect of the chronic diseases such as HIV – HIV-associated neurocognitive disorders.10,12,22 While assessing for severe neurocognitive impairment in community settings, the prevalence seems relatively lower (usually ranges between 2.3% and 21.6%),6,25,32–34 as reported herein. Supporting the prevalence of the present study, it can be noted that prior hospital-based studies, where the subjects usually have underlying medical conditions, were found reporting higher severe neurocognitive impairment rate due to the confounding effect of chronic health problems, such as diabetes, hypertension, depression, delirium, among others.10,12
To the best of authors’ knowledge, this is the first study in sub-Saharan Africa investigating the role of functional dependence in severe neurocognitive impairment, where severe functional dependency was prevalent among elderly people with severe neurocognitive impairment. These findings are similar to the recent studies reported from other parts of the world, such as Asia (China, South Korea, Thailand, and Japan),35,36 Europe (Czech Republic),37 and South America (Brazil).38 This relationship may be because of severe neurocognitive impairment, such as Alzheimer’s dementia causing loss of significant areas in the brain, which is responsible for operating daily life activities.39 Hence, the increasing odds for neurocognitive impairment as the functional dependence increases. This makes decreasing functional independence a sensitive marker for early detection of neurocognitive impairment, similar to other studies.15,16,40 However, with a low correlation between neurocognitive impairment and functionality and most of the participants in this study remaining functionally independent (slightly and completely no dependence) despite having a severe neurocognitive impairment, it makes functionality a poorer predictor of neurocognitive impairment. Therefore, additional methods for early diagnosis of neurocognitive impairment are highly suggested, which may include (i) facilitating routine screening for dementia with simple diagnostic tools for cognitive decline, (ii) making it routine to report neurocognitive scores for every elderly person attending a healthcare facility, or (iii) having a high index of suspicion in the presences of commonly identified risk factors.
This study identified a wide range of severe neurocognitive impairment associated factors, such as advanced age, female gender, and lower levels of education, which are also reported in the prior studies.1,6,25,34,41–44 As age increases, the rate of neuronal degeneration and vascular changes increases, weakness in the immune system and body repair systems; hence, a higher likelihood of severe neurocognitive impairment is seen with increasing age.45,46 In addition, female participants are at a higher likelihood of severe neurocognitive impairment, which may be due to various factors, such as (i) longevity of females – increasing age, (ii) lack of estrogen after menopause – a hormone considered protective against Alzheimer’s dementia, (iii) being prone to adverse effects of head injury that increase their likelihood to severe neurocognitive impairment despite men having higher rates of head trauma, (iv) being at higher risk of psychiatric problems like depression, which increases the risk of severe neurocognitive impairment, (v) being culturally less privileged for educational attainment, especially in resource-limited settings, and (vi) being less privileged of protective factors of dementia, such as smoking of nicotine.47,48 In addition, participants with a higher level of education are reported of lower prevalence of neurocognitive impairment as per this study because it favors a cognitive reserve – the ability to keep up a good cognitive performance despite brain pathology.49,50 Although all the identified associated factors in this study are easy to recognize and can be used to screen out individuals to undergo further tests for neurocognitive disorders, diagnosing neurocognitive disorders among elders still poses a challenge in Uganda. Many patients have sought alternative modes of treatment before they reach the hospitals and at the healthcare facilities; the health workers have limited knowledge about neurocognitive disorders due to various myths and lack of skills by the healthcare providers.50,51 Majority of the care for elders with neurocognitive disorders is by the caregivers, community, and village health teams whose perception do not promote adequate management.9,52–54 Thus, patients reaching the health facility late and mortality become inevitable during admission.55
This study had limitations that should be taken into account while interpreting our findings. First, many of the participants had no formal education and could not read and write; therefore, some sections of the MMSE may not have been responded to appropriately (although such errors in responding to the MMSE, were reduced by having trained local research assistant fluent in the local language, to ensuring a better communication with the participants). Also, we did not adjust the score for the MMSE in terms of age and level of education of the participants, which may affect the findings. We did not also use all the MMSE items for all participants, especially the ones with low levels of education who could not read and write. Despite the fact that the tools used were pretested prior to the study, they have not been validated in our settings, limiting the findings. We, therefore, recommend further studies to test the reliability of these screening tools, especially for conditions such as dementia. The study also did not include some of the important variables that are common risk factors for neurocognitive impairment, such as diabetes, hypertension, depression, blood biochemical parameters. Lastly, it was a cross-sectional study, and causality cannot easily be determined.
Conclusions
Severe neurocognitive impairment prevalence is increasing over the years, reflecting the need for adequate studies for the early diagnosis of vulnerable individuals. Considering that information about neurocognitive impairment among Ugandan older persons is sparse, the findings of this study contribute to understanding the prevalence of severe neurocognitive impairments and its sociodemographic and functionality associations in the country. The identified associations are recommended as a marker that can be used for early detection and intervention of neurocognitive impairment. Therefore, it is urged that functionality assessments for the elderly should be routinely done in healthcare facilities when the elderly people seek care for other ailments.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author MMK on reasonable request.
Ethical Approval and Consent of Participants
The study was conducted in accordance with the Declaration of Helsinki. The study received ethics approval from research ethics committee of Mbarara University of Science and Technology (approval number: MUSTREC#05/11-20). Permission to collect data from participants was granted by the director of MRRH. All participants provided voluntary written informed consent at study enrollment.
Consent for Publication
All participants consented for publication of their information.
Acknowledgments
The research assistants Franklin Kakuru, Brenda Nabatanza, Moses Kule, Badru Kayongo, Innocent Arinaitwe, and Sarah Maria Najjuka. Mbarara regional referral hospital that provided a conducive environment for data collection, and the participants without them, these important data would not have been obtained.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The study was funded by the Kayanja Fellowship Program, Mbarara, Uganda.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Ruitenberg A, Ott A, van Swieten JC, Hofman A, Breteler MMB. Incidence of dementia: does gender make a difference? Neurobiol Aging. 2001;22(4):575–580. doi:10.1016/S0197-4580(01)00231-7
2. World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; 2019.
3. Fratiglioni L, De Ronchi D, Agüero-Torres H. Worldwide prevalence and incidence of dementia. Drugs Aging. 1999;15(5):365–375.
4. Nichols E, Szoeke CE, Vollset SE, et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(1):88–106.
5. Connell CM, Gibson GD. Racial, ethnic, and cultural differences in dementia caregiving: review and analysis. The Gerontologist. 1997;37(3):355–364.
6. Olayinka OO, Mbuyi NN. Epidemiology of dementia among the elderly in sub-Saharan Africa. Int J Alzheimer’s Dis. 2014;2014.
7. Abreu W, Tolson D, Jackson GA, Staines H, Costa N. The relationship between frailty, functional dependence, and healthcare needs among community‐dwelling people with moderate to severe dementia. Health Soc Care Community. 2019;27(3):642–653.
8. Pasquini L, Guerra JL, Prince M, Chua KC, Prina AM. Neurological signs as early determinants of dementia and predictors of mortality among older adults in Latin America: a 10/66 study using the NEUROEX assessment. BMC Neurol. 2018;18(1):1–11.
9. Owokuhaisa J, Rukundo GZ, Wakida E, Obua C, Buss SS. Community perceptions about dementia in southwestern Uganda. BMC Geriatr. 2020;20:1–12.
10. Kloppenborg RP, van den Berg E, Kappelle LJ, Biessels GJ. Diabetes and other vascular risk factors for dementia: which factor matters most? A systematic review. Eur J Pharmacol. 2008;585(1):97–108.
11. Connors MH, Ames D, Boundy K, et al. Predictors of mortality in dementia: the PRIME study. J Alzheimer’s Dis. 2016;52(3):967–974.
12. Sleeman KE, de Brito M, Etkind S, et al. The escalating global burden of serious health-related suffering: projections to 2060 by world regions, age groups, and health conditions. Lancet Global Health. 2019;7(7):e883–e892.
13. Wandera SO, Kwagala B, Ntozi J. Determinants of access to healthcare by older persons in Uganda: a cross-sectional study. Int J Equity Health. 2015;14(1):1–10.
14. Rukundo ZG, Musisi S, Nakasujja N. Psychiatric morbidity among physically ill patients in a Ugandan Regional Referral Hospital. Afr Health Sci. 2013;13(1):87–93.
15. Balbim GM, Maldonado AM, Early A, Steinman L, Harkins K, Marquez DX. Evaluation of public health messages promoting early detection of dementia among adult latinos with a living older adult parental figure. Hispanic Health Care Int. 2020;18(3):163–173.
16. Moyer VA. Screening for cognitive impairment in older adults: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(11):791–797.
17. Lohmeyer JL, Alpinar-Sencan Z, Schicktanz S. Attitudes towards prediction and early diagnosis of late-onset dementia: a comparison of tested persons and family caregivers. Aging Ment Health. 2020;1–12:832–43.
18. So A, Hooshyar D, Park KW, Lim HS. Early diagnosis of dementia from clinical data by machine learning techniques. Appl Sci. 2017;7(7):651.
19. Rasmussen J, Langerman H. Alzheimer’s disease–why we need early diagnosis. Degener Neurol Neuromuscul Dis. 2019;9:123.
20. Sacktor N, Saylor D, Nakigozi G, et al. Effect of HIV Subtype and Antiretroviral therapy on HIV-associated neurocognitive disorder (HAND) stage in Rakai, Uganda. J Acq Immune Def Syndr. 2019;81(2):216.
21. Saylor D, Nakigozi G, Pardo CA, et al. Vitamin D is not associated with HIV-associated neurocognitive disorder in Rakai, Uganda. J Neurovirol. 2019;25(3):410–414.
22. Namagga JK, Rukundo GZ, Voss JG. Prevalence and risk factors of HIV-associated neurocognitive disorders in rural Southwestern Uganda. J Assoc Nurses AIDS Care. 2019;30(5):531.
23. Rubin LH, Saylor D, Nakigozi G, et al. Heterogeneity in neurocognitive change trajectories among people with HIV starting antiretroviral therapy in Rakai, Uganda. J Neurovirol. 2019;25(6):800–813.
24. Sacktor N, Nakasujja N, Redd AD, et al. HIV subtype is not associated with dementia among individuals with moderate and advanced immunosuppression in Kampala, Uganda. Metab Brain Dis. 2014;29(2):261–268.
25. Mubangizi V, Maling S, Obua C, Tsai AC. Prevalence and correlates of Alzheimer’s disease and related dementias in rural Uganda: cross-sectional, population-based study. BMC Geriatr. 2020;20(1):48.
26. Kish L. Statistical Design for Research. Vol. 83. John Wiley & Sons; 2004.
27. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198.
28. Tombaugh TN, McIntyre NJ. The mini‐mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–935.
29. Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index: a simple index of independence useful in scoring improvement in the rehabilitation of the chronically ill. Md State Med J. 1965.
30. Yoseph M, Paddick SM, Gray WK, et al. Prevalence estimates of dementia in older adults in rural Kilimanjaro 2009–2010 and 2018–2019: is there evidence of changing prevalence? Int J Geriatr Psychiatry. 2021;36(6):950–959.
31. Ojabemi A. The low prevalence of dementia in sub-Saharan Africa: a systematic review and meta-analysis of geographical variations and associations. Afr J Med Med Sci. 2020;49(1):9–21.
32. El Tallawy HN, Farghly WM, Shehata GA, et al. Prevalence of dementia in Al Kharga District, New Valley Governorate, Egypt. Neuroepidemiology. 2012;38(3):130–137.
33. Khedr E, Fawi G, Abbas MAA, et al. Prevalence of mild cognitive impairment and dementia among the elderly population of Qena Governorate, Upper Egypt: a community-based study. J Alzheimer’s Dis. 2015;45(1):117–126.
34. Longdon AR, Paddick SM, Kisoli A, et al. The prevalence of dementia in rural Tanzania: a cross‐sectional community‐based study. Int J Geriatr Psychiatry. 2013;28(7):728–737.
35. Yi Y, Ding L, Wen H, Wu J, Makimoto K, Liao X. Is Barthel index suitable for assessing activities of daily living in patients with dementia? Front Psychiatry. 2020;11:282.
36. Lee G. Impaired cognitive function is associated with motor function and activities of daily living in mild to moderate Alzheimer’s Dementia. Curr Alzheimer Res. 2020;17(7):680–686.
37. Kisvetrová H, Herzig R, Bretšnajdrová M, Tomanová J, Langová K, Školoudík D. Predictors of quality of life and attitude to ageing in older adults with and without dementia. Aging Ment Health. 2019;1–8.
38. Fischer A, Dourado MCN, Laks J, Landeira-Fernandez J, Morris RG, Mograbi DC. Modelling the impact of functionality, cognition, and mood state on awareness in people with Alzheimer’s disease. Int Psychogeriatrics. 2019;1–11.
39. Chabran E, Noblet V, de Sousa PL, et al. Changes in gray matter volume and functional connectivity in dementia with Lewy bodies compared to Alzheimer’s disease and normal aging: implications for fluctuations. Alzheimer’s Res Ther. 2020;12(1):1–13.
40. Wojszel ZB. Dementia diagnoses and treatment in geriatric ward patients: a cross-sectional study in Poland. Clin Interv Aging. 2020;15:2183.
41. Smith K, Flicker L, Dwyer A, et al. Factors associated with dementia in Aboriginal Australians. Austr N Zeal J Psychiatry. 2010;44(10):888–893.
42. Orrell M, Sahakian B. Education and Dementia. 1995.
43. St John PD, Seary J. Rural residence and risk of dementia. Can J Rural Med. 2016;21(3):73.
44. Jutkowitz E, MacLehose RF, Gaugler JE, Dowd B, Kuntz KM, Kane RL. Risk factors associated with cognitive, functional, and behavioral trajectories of newly diagnosed dementia patients. J Gerontol Ser A. 2017;72(2):251–258.
45. Pantoni L. Pathophysiology of age-related cerebral white matter changes. Cerebrovasc Dis. 2002;13(Suppl. 2):7–10.
46. Wahl D, Solon-Biet SM, Cogger VC, et al. Aging, lifestyle and dementia. Neurobiol Dis. 2019;130:104481.
47. Sandberg LJ. Dementia and the gender trouble?: theorising dementia, gendered subjectivity and embodiment. J Aging Stud. 2018;45:25–31.
48. Mielke MM. Sex and gender differences in Alzheimer’s disease dementia. Psychiatr Times. 2018;35(11):14.
49. Sharp ES, Gatz M. The relationship between education and dementia an updated systematic review. Alzheimer Dis Assoc Disord. 2011;25(4):289.
50. Then FS, Luck T, Angermeyer MC, Riedel-Heller SG. Education as protector against dementia, but what exactly do we mean by education? Age Ageing. 2016;45(4):523–528.
51. Kamoga R, Rukundo GZ, Wakida EK, Nakidde G, Obua C, Buss SS. Dementia assessment and diagnostic practices of healthcare workers in rural southwestern Uganda: a cross-sectional qualitative study. BMC Health Serv Res. 2019;19(1):1–7.
52. Atuhaire CD, Obua C, Rukundo GZ, Haberer JE, Wakida EK. Alzheimer’s Disease and Related Dementias: A Qualitative Assessment of Perceived Training Needs of Primary Healthcare Providers in Rural Southwestern Uganda. 2019.
53. Karungi C, Obua C, Rukundo GZ, Maling S, Haberer JE, Wakida EK. Community-Based Management and Care of People with Dementia: A Training Needs Assessment Among Village Health Teams in Uganda Based on WHO Guidelines. 2019.
54. Tumuhairwe J, Maling S, Okello ES, Gelaye B, Wakida EK, Obua C. A Qualitative Study on Caregivers and Patients Perceptions About Alzheimer’s and Related Dementias in Southwestern Uganda. 2019.
55. Kaggwa MM, Najjuka SM, Harms S, Ashaba S. Mortality among patients admitted in a psychiatric facility: a single-centre review. Clinical Audit. 2021;13:21–28.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.