Back to Journals » Clinical Ophthalmology » Volume 13
Prevalence of increased intraocular pressure in patients with Graves’ ophthalmopathy and association with ophthalmic signs and symptoms in the north-west of Iran
Authors Eslami F ![]() , Borzouei S
, Borzouei S ![]() , Khanlarzadeh E, Seif S
, Khanlarzadeh E, Seif S
Received 13 February 2019
Accepted for publication 17 June 2019
Published 25 July 2019 Volume 2019:13 Pages 1353—1359
DOI https://doi.org/10.2147/OPTH.S205112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fatemeh Eslami,1 Shiva Borzouei,2 Elham Khanlarzadeh,3 Shiva Seif3
1Department of Ophthalmology, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran; 2Clinical Research Development Unit of Shahid Beheshti Hospital, Hamadan University of Medical Sciences, Hamadan, Iran; 3School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
Introduction: Graves’ ophthalmopathy (GO) is the most common extra-thyroidal manifestation of Graves’ disease and is characterized by multiple ocular symptoms such as eyelid retraction, lid lag, proptosis, elevated intraocular pressure (IOP) and ultimately loss of vision. We aimed to investigate the prevalence of increased IOP in Graves’ patients and association with ophthalmic signs and symptoms in north-west of Iran.
Materials and methods: This descriptive cross-sectional study recruited 93 patients with GO who were diagnosed based on clinical and laboratory examinations. A complete ocular examination and IOP measurements on forward gaze were performed using Goldman applanation tonometer.
Results: In this study, 93 patients with GO were evaluated from 2016 to 2017. Among these patients, 67 (72.05%) were female and 27 (27.95%) were male. The most common complaints of patients were lid retraction (62.36%), puffy eyelids (58.06%) and proptosis (46.23%), respectively. The duration of disease was 0–24 months in most patients. Most subjects were at grade 3 according to NOSPECS classification. Nine patients (9.6%) had an IOP greater than or equal to 21 mmHg. The mean IOP in subjects was 16.61±3.42 mmHg. The mean IOP in males and smokers was significantly higher than that of females and nonsmokers. The mean IOP increased significantly with a higher grade of disease, duration of disease, age and smoking.
Conclusions: According to the results, females comprised the majority of the study population, while ocular complications were more prevalent among males. The highest IOP was seen in old cases of GO. The most prevalent ocular signs in patients were eyelid retraction and periorbital edema. The least prevalent sign was glaucomatous optic neuropathy. In this study, the prevalence of intra-ocular hypertension was higher than that of the general population, especially in males, old cases with a drug history of antithyroid medication and smokers.
Keywords: Graves’ ophthalmopathy, intra ocular pressure
Introduction
Thyroid eye diseases (TED) form a part of the Graves' disease triad, which includes hyperthyroidism, periorbital myxedema or dermopathy with manifestations such as eyelid retraction, lid lag, proptosis, extraocular muscle restriction, compressive optic neuropathy, exposure keratopathy, conjunctival erythema and chemosis.1
In the pathogenesis of Graves' disease, interactions between T lymphocytes and fibroblasts result in tissue activation that is mediated by several cytokines. Activated fibroblasts leading to synthesize of hyaluronan and other glycosaminoglycans, which expand orbital tissue. Moreover, fibrocytes can differentiate into adipocytes or myofibroblasts and thus can contribute to the orbital tissue remodeling.2 Extraocular muscle fibers become widely separated by the accumulation of hyaluronidase-digestible material and orbital fat increase secondary to adipogenesis, which these events lead to proptosis and optic-nerve compression. Also, extraocular muscles can become fibrotic in a later stage of the disease, resulting in restricted motility.3
Female susceptibility to autoimmune diseases such as Graves' is higher than male, and female to male ratio of systemic hyperthyroidism is 4 to 1. Ophthalmopathy is the key signs of Graves' disease. The female to male ratio in thyroid ophthalmopathy is 2.5 to 1.4 The effects of risk factors such as age, sex, radioactive iodine intake and smoking on this disease have been investigated5 A direct relationship has been observed between the development of hyperthyroidism and TED, but the severity of TED is usually not parallel to the serum T3 and T4 levels.1 More than half of the people with hyperthyroidism develop eye symptoms during their disease, which might be unilateral or bilateral, mild or severe.6
Elevation of IOP on up-gaze is observed in most patients with exophthalmos. There is an abnormal IOP in 68% of patients without proptosis.7 The cause of elevated IOP in thyroid ophthalmopathy is an increase in the episcleral venous pressure.8 Patients with ocular hypertension (OHT) should be more accurately followed up compared to the normal population in terms of glaucoma incidence. OHT is not preventable, but regular ophthalmic examinations and follow-up can prevent its progression to glaucoma.9 The clinical features of Graves' ophthalmopathy (GO) may be one of the most common manifestations of Graves' disease. There are few studies to evaluate the prevalence and severity of GO in Iranian population. In our study, we aimed to investigate the frequency of increased IOP and severity of ophthalmopathy in Graves' patients in Hamadan city (west of Iran).
Materials and methods
This descriptive cross-sectional study enrolled 93 patients with GOy. All patients with confirmed diagnosis of Graves' disease in the endocrine clinics of the Hamadan University of Medical Sciences who have any signs or symptoms of GO were recruited to the study.
The diagnosis of Graves' disease was based on clinical and laboratory findings of diffuse enlargement of thyroid gland, triiodothyronine (T3), thyroxin (T4), T3 resin uptake, raised free T4 or T3 levels and suppressed thyroid stimulating hormone levels. Patients with Graves' disease were referred to the Ophthalmology clinic of Farshchian Hospital affiliated by Hamadan University of Medical Sciences. A comprehensive ophthalmic assessment including best corrected visual acuity (BCVA), external eye examination, ocular motility examination, exophthalmometry, tear status evaluation, intraocular pressure (IOP) measurement, slit lamp examination and fundoscopy was performed. Patients with history of corticosteroids and beta-blockers consumption were excluded from the study.
In this study, glaucoma status defined as repeated elevated IOPs ≥22 mm Hg measured by Goldmann applanation tonometry in the primary position, visual field defects and/or glaucomatous optic neuropathy that is a generalized or localized thinning of the optic disc neuroretinal rim in stereoscopic fundoscopy. Measured IOP was corrected for central corneal thickness (CCT) using Doughty and Zaman formulae with correction of 2.5 mm Hg for each 50-µm change in CCT assuming a baseline of 500 µm.10
An increase in IOP was expected in up-gaze in patients with restrictive TED,11 but IOP was measured in primary position in all of the patients and neither of the participatants had restriction in primary position.
Tear status was evaluated with Schirmer’s test and tear breakup time (TBUT). We considered Schirmer’s test less than 10 mm and TBUT less than 10 s as tear film dysfunction. Degree of proptosis was measured by the Hertel exophthalmometer.
Proptosis was defined as the measurement of protrusion of the globe >20 mm from the lateral orbital rim in either eye or any discrepancy in the degree of protrusion of the two eyes by >2 mm. The classification of GO was based on the classification by the American Thyroid Association from Werner’s (NOSPECS classification) (Table 1).
 |
Table 1 Modified Werner’s NOSPECS classification score |
The current study was conducted with the coordination of Hamadan University of Medical Sciences (research code: IR.UMSHA.REC.1394.93.). Data were collected anonymously and the results were released in general. Written informed consent was obtained from all individuals involved. Also, a parent provided written informed consent for any participant under the age of 18 years.
The quantitative variables were reported as mean and SD, and categorical variables were reported as frequency and percent. The normality of the variables was tested using the Kolmogorov–Smirnov test. Independent sample T-test and in the cases of non-normal distribution Mann–Whitney test was used for comparing the means between the two groups. Analysis of variance and in the cases of non-normal distribution Kruskal–Wallis were used to compare the quantitative variables among more than two groups. The Chi-square test was used to compare the categorical variables among the groups. The level of statistical significance was set at p<0.05. The SPSS software (version 20.0) was used for data analysis.
Results
This study enrolled 93 patients (26 men and 67 women) with Graves' disease. The mean age of patients was 34.98±12 years, ranging from 11 to 80 years. The majority of the cases (61.3%, n=57) were in their 3th to 5th decade. The mean duration of Graves' disease was 2.56±2.16 years (ranging from 6 months to 18 years). The most common apparent sign was lid retraction, which was noticed in 62.36% of patients, that was followed by peri-orbital edema and proptosis. (Table 2)
 |
Table 2 Baseline characteristics of patients |
Mean (SD) of visual acuity was 0.87 (±0.20). The patients had a mean modified Werner’s NOSPECS classification score of 3.15 (±1.46). The score was significantly associated with sex and was higher in males (3.80 vs 2.89 in females; P<0.001). The score was positively correlated with the age of the patients (P<0.001).
The mean IOP was 16.61±3.42 mmHg in all participants. The mean (SD) IOP of male and female was 18.23 (±3.8) mmHg and 15.98 (±3.07) mmHg, respectively. This figure among smokers and nonsmokers was 20.50 (±3.61) mmHg and15.92 (±2.91) mmHg, respectively. The mean of IOP increased significantly with the increase of the disease grade, duration of disease and age (Table 2).
The cup to disc ratio (CDR) and loss of visual acuity in males was significantly more than females (Table 3).
 |
Table 3 Comparison of IOP and cup to disc ratio based on gender, smoking, grade of disease, duration of disease and age groups |
The frequency of proptosis, chemosis, restriction of eye movement and dry eyes in male patients was significantly higher than that of females. The frequency of these complications in smokers was significantly higher than that of nonsmokers. In addition, these manifestations increased significantly with duration and grade of disease (Table 3).
The frequency of periorbital edema significantly increased with duration and grade of disease as well as smoking, but it was not significantly different between males and females. It was also observed that the prevalence of periorbital edema significantly decreased up to the age of 40 and significantly increased in patients older than 40 years (Table 4).
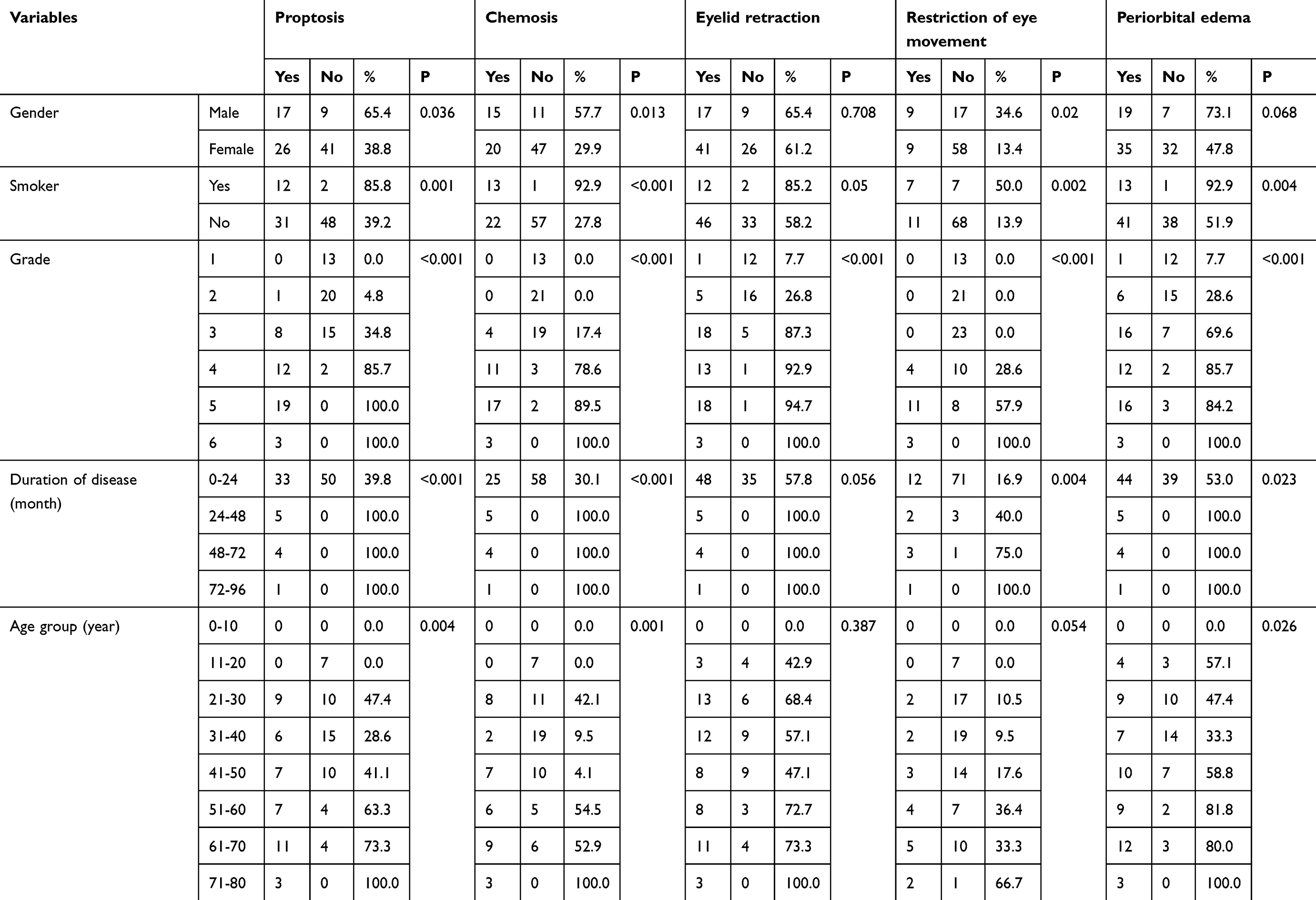 |
Table 4 Frequency of manifestations based on gender, smoking, grade of disease, duration of diseases, and age |
Discussion
GO is an autoimmune inflammatory orbital disease linked to autoimmune hyperthyroidism and rarely be seen in patients with Hashimoto’s thyroiditis or in euthyroid patients.4 GO is the most common form of extrathyroidal manifestation in patients with Graves' disease. These manifestations include exophthalmos, soft tissue involvement, extraocular muscle restriction, corneal ulcer, elevated IOP, optic neuropathy and blindness.12 More than half of the people with hyperthyroidism develop eye symptoms during their disease which might be unilateral or bilateral, mild or severe.13 Several studies have investigated the effects of risk factors such as age, sex, radioactive iodine intake and smoking on this disease.5 In our patient sample, GO affected females only 2–3 times more frequently than males (72.05% versus 27.95% of cases, respectively), whereas in other studies female to male ratio was between 4–6:1.4,9
Nine patients (9.6%) had an IOP greater than or equal to 21 mmHg. The participants’ mean IOP was 16.61 mmHg. The mean IOP in males and smokers was significantly higher than that in females and nonsmokers. The mean IOP increased significantly with grade of disease, duration of disease and age. Elevated IOP in the Graves' disease has been reported in many studies,1,6,7,9,14 which indicates the relationship between IOP and the Graves' disease. In studies by Timothy and Lee, IOP was significantly higher in smokers than that in nonsmokers.15,16 Elevated IOP is due to the effect of nicotine as an effective substance in cigarettes. Nicotine causes immediate adrenaline secretion, and the adrenaline effects include increased heart rate, increased blood pressure and, consequently, elevated IOP.16,17
As the third most common sign found in this study, proptosis was observed in 43 (46.24%) patients. Mean IOP in the group with proptosis (18.39 mmHg) was significantly higher than that of the group without proptosis (15.8 mmHg). In a study by Ohtsuka et al, the mean IOP in patients with proptosis was significantly higher than that of those without proptosis.18
Thirty-five (37.63%) subjects had chemosis. Mean IOP was significantly different between patients with chemosis (18.88 mmHg) and those without chemosis (15.24 mmHg). In a study by Razavi et al, the incidence rate of chemosis in patients with GO was 4.4%.14 Rastegar et al reported the incidence rate of chemosis or conjunctivitis as 27%, and that conjunctivitis had a significant relationship with age and sex, as it was higher in males than in females. They observed that the incidence of chemosis increased with the duration of the disease.6
In the present study, the most common ocular sign was eyelid retraction that was observed in 58 patients (62.36%). The mean IOP in patients with eyelid retraction was significantly higher than those without eyelid retraction. Eyelid retraction has been reported as the most common finding in several studies.4,19–23 Rastegar et al reported eyelid retraction as the second most common finding after proptosis, which increased with age. Similar to the present study, there was no significant difference between the incidence of lid retraction between male and female in their study.6
The frequency of eye movement restriction in this study was 19.35%. The difference in mean IOP was significant between individuals with and without eye movement restriction. In a study by Razavi et al, eye movement restriction was reported in 19.1% of patients. In their study, elevated IOP on up-gaze in individuals with eye movement restriction was higher than those without eye movement restriction.14
Among the subjects in this study, 35.48% had dry eyes. The mean IOP in subjects with dry eyes (18.73 mmHg) was significantly higher than those without dry eyes (15.91 mmHg). Another study reports the frequency of dry eyes in patients with Graves’ disease up to 45–85%.24 Numerous studies indicate an increase in the frequency of dry eyes at an older age.25–27 In some studies, female gender is considered a risk factor for dry eyes,28 while others have found no relationship between sex and dry eyes.25
Visual acuity was also examined in this study. Normal visual acuity is 20/20 or 6/6 and a visual acuity less than 5 (out of 10) is considered as impaired vision.29,30 BCVA decreased in our study population. Furthermore, visual acuity decreased significantly with increasing age, disease duration and higher grade of disease. In addition, there was a negative relationship between visual acuity and IOP. Several studies have shown that visual acuity decreases with age, which confirms the result of our study.31–33 Considering that only 31.18% of the subjects were over 50 years and decreased visual acuity was also observed in younger people, the decreased mean visual acuity in this study cannot be only due to aging.
TED has been found to be usually associated with glaucoma. CDR is an index for the presence of glaucoma. A CDR above 0.6 along with other criteria is considered as glaucoma. In our study, 9 patients, which accounted for 9.6% of cases, had increased IOP and 3 patients (3.2%) of the subjects had a CDR of 0.6 or higher. CDR also increased significantly by age. Carpel reported no relationship between CDR and IOP, but a positive relationship between CDR and age.34 The presence of this severe degree of eye involvement and visual loss in our setup may be due to late presentation and due to unawareness of their disease process at presentation. It may be also due to our center being a tertiary eye center and we get the majority of complicated and referred cases.
Conclusion
We propose a detailed eye examination for all subjects who are diagnosed with Graves’ disease. Our results corresponded with numerous other studies with slight epidemiologic variations. Early diagnosis and treatment of complications such as proptosis, optic neuropathy and glaucoma lead to prevention of blindness. Furthermore, given that most of these complications became prevalent with an increase in age and higher grade of disease, eye examinations should be considered for all patients, especially in older adults, smokers and patients with higher severity score of thyroid ophthalmopathy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cockerham KP, Pal C, Jani B, Wolter A, Kennerdell JS. The prevalence and implications of ocular hypertension and glaucoma in thyroid-associated orbitopathy. Ophthalmology. 1997;104(6):914–917.
2. Smith TJ, Hegedüs L. Graves’ disease. N Engl J Med. 2016;375:1552–1565. doi:10.1056/NEJMra1510030
3. Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362:726–738. doi:10.1056/NEJMra0905750
4. Bradley EA. Graves ophthalmopathy. Curr Opin Ophthalmol. 2001;12(5):347–351.
5. Wiersinga W, Smit T, Van Der Gaag R, Mounts M, Koomneef L. Clinical presentation of Graves’ ophthalmopathy. Ophthalmic Res. 1989;21(2):73–82. doi:10.1159/000266782
6. Rastegar A, Besharati MR, Shoja MR, Manaviat MR, Ahmadieh MH. Clinical survey of ocular findings in patients with grave’s disease. J Qazvin Univ. 2006;10(9):43–51.
7. da Silva FLM, Rodrigues MDV, Akaishi PMS, Cruz AA. Graves’ orbitopathy: frequency of ocular hypertension and glaucoma. Eye. 2008;23(4):957–959. doi:10.1038/eye.2008.155
8. Burch HB, Wartofsky L. Graves’ ophthalmopathy: current concepts regarding pathogenesis and management. Endocr Rev. 1993;14(6):747–793. doi:10.1210/edrv-14-6-747
9. Behrouzi Z, Rabei HM, Azizi F, et al. Prevalence of open-angle glaucoma, glaucoma suspect, and ocular hypertension in thyroid-related immune orbitopathy. J Glaucoma. 2007;16(4):358–362. doi:10.1097/IJG.0b013e31802e644b
10. Doughty MJ, Zaman ML. Human corneal thickness and its impact on intraocular pressure measures: a review and meta-analysis approach. Surv Ophthalmol. 2000;44(5):367–408. doi:10.1016/S0039-6257(00)00110-7
11. Rahman I, Cannon PS, Sadiq SA. Tonopen versus goldmann applanation tonometry for detecting restrictive thyroid eye disease. Ophthalmic Plast Reconstr Surg. 2010;26(1):36–38. doi:10.1097/IOP.0b013e3181b80fcb
12. Kelly W, Cove-Smith R, Rashid A. Ocular manifestations of Graves’ disease. J R Soc Med. 1985;78(5):417.
13. Woo KI, Kim Y-D, Lee SY. Prevalence and risk factors for thyroid eye disease among korean dysthyroid patients. Korean J Ophthalmol. 2013;27:397–404. doi:10.3341/kjo.2013.27.6.397
14. Etezad-Razavi M, Aboutorabi R-B, Zarei-Ghanavati S, et al. Prevalence and severity of ophthalmic manifestations of Graves’ disease in mashhad university endocrine clinics. Iran J Ophthalmol. 2007;19(3):14–21.
15. Lee AJ, Rochtchina E, Wang JJ, Healey PR, Mitchell P. Does smoking affect intraocular pressure? Findings from the blue mountains eye study. J Glaucoma. 2003;12(3):209–212.
16. Timothy C, Nneli R. The effects of cigarette smoking on intraocular pressure and arterial blood pressure of normotensive young Nigerian male adults. Niger J Physiol Sci. 2007;22(1–2):33–36.
17. Dielemans I, Vingerling JR, Algra D, Hofman A, Grobbee DE, de Jong PTVM. Primary Open-angle glaucoma, intraocular pressure, and systemic blood pressure in the general elderly population. Ophthalmology. 1995;102(1):54–60.
18. Ohtsuka K. Intraocular pressure and proptosis in 95 patients with graves ophthalmopathy. Am J Ophthalmol. 1997;124(4):570–572.
19. Ardeshirei M, Daftariyan N, Mehrabi Y, Azizi F. Prevalence of ophthalmic manifestations in patients with diffuse toxic goiter in Tehran. Iran J Endocrinol Metab. 2005;7(3):217–222.
20. Bartley GB, Fatourechi V, Kadrmas EF, et al. Long-term follow-up of Graves ophthalmopathy in an incidence cohort. Ophthalmology. 1996;103(6):958–962.
21. Gaddipati RV, Meyer DR. Eyelid retraction, lid lag, lagophthalmos, and von Graefe’s sign quantifying the eyelid features of Graves’ ophthalmopathy. Ophthalmol. 2008;115:1083–1088. doi:10.1016/j.ophtha.2007.07.027
22. Teshome T, Seyoum B. Graves’ thyroid ophthalmopathy in Ethiopian patients. Ethiop Med J. 2001;39(1):1–8.
23. Jankauskiene J, Jarusaitiene D. Clinical ocular features in children and young adults with thyroid diseases. Thyroid Disorders Ther. 2017;6:221. doi:10.4172/2167-7948
24. Nowak M, Marek B, Kos-Kudła B, Kajdaniuk D, Siemińska L. Tear film profile in patients with active thyroid orbithopathy. Klinikaoczna. 2005;107(7–9):479–482.
25. Schein OD, MUÑO B, Tielsch JM, Bandeen-Roche K, West S. Prevalence of dry eye among the elderly. Am J Ophthalmol. 1997;124(6):723–728.
26. Moss SE, Klein R, Klein BEK. Long-term incidence of dry eye in an older population. Optometry Vision Sci. 2008;85(8):668–674. doi:10.1097/OPX.0b013e318181a947
27. Moss SE, Klein R, Klein BE. Incidence of dry eye in an older population. Arch Ophthalmol. 2004;122(3):369–373. doi:10.1001/archopht.122.3.369
28. Kawashima M, Yamada M, Suwaki K, et al. A clinic-based survey of clinical characteristics and practice pattern of dry eye in Japan. Adv Ther. 2017;34(3):732–743. doi:10.1007/s12325-017-0487-x
29. Ferris FL, Kassoff A, Bresnick GH, Bailey I. New visual acuity charts for clinical research. Am J Ophthalmol. 1982;94(1):91–96.
30. Klein R, Klein BE, Lee KE. Changes in visual acuity in a population. The Beaver Dam Eye Study. Ophthalmology. 1996;103(8):1169–1178.
31. Carlson SE, Werkman S, Rhodes P, Tolley E. Visual-Acuity Development in Healthy Preterm Infants: Effect of Marine-Oil Supplementation. Am J Clin Nutr. 1993;58(1):35–42.
32. Elliott DB, Yang KC, Whitaker D. Visual acuity changes throughout adulthood in normal, healthy eyes: seeing beyond 6/6. Optom Vis Sci. 1995;72:186–191.
33. Long GM, Crambert RF. The nature and basis of age-related changes in dynamic visual acuity. Psychol Aging. 1990;5(1):138. doi:10.1037/0882-7974.5.1.138
34. Carpel EF, Engstrom PF. The normal cup-disk ratio. Am J Ophthalmol. 1981;91(5):588–597.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.