Back to Journals » Clinical Interventions in Aging » Volume 15
Prevalence of Falls, Physical Performance, and Dual-Task Cost While Walking in Older Adults at High Risk of Falling with and Without Cognitive Impairment
Received 20 March 2020
Accepted for publication 29 May 2020
Published 22 June 2020 Volume 2020:15 Pages 945—952
DOI https://doi.org/10.2147/CIA.S254764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Fuzhong Li,1 Peter Harmer2
1Oregon Research Institute, Eugene, OR 97403, USA; 2Department of Exercise and Health Science, Willamette University, Salem, OR, 97301, USA
Correspondence: Fuzhong Li
Oregon Research Institute, 1776 Millrace Dr., Eugene, OR 97403, USA
Email [email protected]
Purpose: To compare the prevalence of falls, physical performance, and dual-task cost during walking between cognitively healthy and impaired older adults at high risk of falling.
Methods: A cross-sectional analysis of 670 community-dwelling older adults who were considered at high risk of falling, operationalized as 1) having fallen at least once in the preceding 12 months and having a health-care practitioner’s referral indicating that the participant was at risk of falls or 2) having impaired mobility as evidenced by a Timed Up and Go (TUG) result ≥ 13.5 s. Participants (mean age = 77.7 years, SD = 5.6) were divided into cognitively healthy (n = 461) or cognitively impaired (n = 209) groups using a cutoff score of < 23 on the Montreal Cognitive Assessment test. Assessment included self-reported number of falls over the previous 12 months, functional reach, TUG, Short Physical Performance Battery (SPPB), and single- and dual-task walk performance. Data were analyzed using Poisson regression to estimate the prevalence ratios of falls and analysis of variance to examine between-group differences on physical performance and dual-task cost during walking performance.
Results: In the analysis, 82.3% of older adults with cognitive impairment and 69.4% of unimpaired older adults reported 1 or more falls in the previous 12 months. Compared with cognitively healthy participants, those with cognitive impairment were 2.57 (95% confidence interval [CI] = 2.17 to 3.05) times more likely to have any fall and 2.33 (95% CI = 1.95 to 2.78) times more likely to have multiple falls. Older adults with cognitive impairment performed worse on functional reach (mean difference [MD] = − 2.33 cm, 95% CI = − 3.21 to − 1.46), TUG (MD = 3.05 s, 95% CI = 2.22 to 3.88), and SPPB (MD = − 1.24 points, 95% CI = − 1.55 to − 0.92) and showed increase in dual-task costs (MD = 6.59%, 95% CI = 4.19 to 9.03) compared to those without cognitive impairment.
Conclusion: Older adults at high risk for falls and who have cognitive impairment are associated with a greater risk for falls and decrements in physical and dual-task performance.
Keywords: cognitive impairment, dual-task, falls, elderly, physical performance
Introduction
As the proportion of older adults in the population increases, concerns about falls and impaired cognitive and functional abilities and their impact on older adult fallers, their caregivers, and the health-care system raise significant public health issues.1–3 While falls and injurious falls in older adults have unequivocally been recognized as a major public health problem globally,1,4,5 increasing evidence suggests that those who experience cognitive impairment may be at greater risk.3,6 Studies have shown that between 30% and 50% of older adults with cognitive impairment have reported falls7,8 and that they may have 5 times higher risk of falling compared to those who are cognitively unimpaired.9 In addition, older adults with cognitive impairment perform poorly on balance, gait, and dual-task activities.8,10,11
While evidence points to the increased risk for falls and fall-related injury and functional deficits among community-dwelling older adults with cognitive impairment,3,6,12,13 what remains unclear is whether cognitive impairment elevates fall risks for those who are already at high risk of falling, a subpopulation of older adults who may be further disadvantaged by compromised attentional resources, executive function, control of posture, and gait.3,14 With the demonstrated increase in morbidity and mortality among individuals with cognitive impairment, including those with Alzheimer’s disease and related disorders,15,16 the lack of knowledge linking cognitive impairment to increased fall risks among high-risk fallers may impede our efforts to develop effective interventions specifically targeting this growing population of older adults. Additionally, clarifying these relationships can help inform clinical guidelines and evidence-based recommendations for improving treatment of motor deficits and fall prevention strategies for individuals at increased risk of cognitive impairment and falls.
Therefore, we examined a sample of community-dwelling older adults who were identified as being at high risk of falling to compare the prevalence of falls and physical and dual-task performance between those who were cognitively healthy and those demonstrating cognitive impairment. On the basis of prior research,8–11 we hypothesized that, in this high-risk population, older adults with cognitive impairment would have a higher prevalence of falls and an increased risk for multiple falls and worse physical and dual-task performance compared to cognitively healthy older adults.
Methods
Study Design and Population
We employed a cross-sectional design using data ascertained from the baseline of a previously completed randomized controlled trial that examined the effectiveness of a Tai Ji Quan exercise intervention to prevent falls.17 The sample was drawn from community-dwelling older adult residents aged ≥70 years who lived in three counties (Multnomah, Clackamas, Lane) in the state of Oregon, where there was a high density of older adult populations and high rates of fall-related deaths. Participants were recruited through promotional efforts conducted at local senior or community centers, senior meal sites (ie, Meals on Wheels), medical clinics, and statewide senior falls prevention networks, supplemented by targeted mass mailings and local newspaper advertisements. Of 1147 individuals who responded to the study promotion and screened per study eligibility criteria (see below), 670 were enrolled into the study, representing a 58% response rate.
Main study eligibility criteria included 1) being 70 years of age and older and 2) being at high risk of falling, defined as having a history of falls in the preceding year and having a health-care practitioner's referral indicating that the participant was at risk of falls or having demonstrated impaired mobility (a score of 13.5 s or greater on the Timed Up and Go [TUG] test18). Individuals with severe cognitive impairment (a score ≤20 on the Mini-Mental State Examination (MMSE))19 or with major limiting physical conditions (as determined by their providers) were excluded. Data used from this study were collected between February 2015 and August 2017. The study was approved by the institutional review board of the Oregon Research Institute, Eugene, Oregon, and written informed consent was obtained from all participants.
Classification of Cognitive Impairment
For the purpose of this study, participants were divided into cognitively healthy (n = 461) or impaired (n = 209) on the basis of a cutoff score of <23 on the Montreal Cognitive Assessment (MoCA) test.20 MoCA is a clinically valid and reliable measure of cognitive function that involves multiple domains, including attention, executive functions, memory, language, conceptual thinking, calculations, visuospatial abilities, and orientation, with scores ranging from 0 to 30, where higher scores indicate better cognitive functioning. The raw MoCA scores were corrected for level of education, that is, 1 point was added to the participant’s score if he or she has 12 years or less of formal education. The decision to use a cutoff score of <23 was based on a meta-analysis indicating that this cutoff score provided the best diagnostic accuracy for differentiating those with healthy cognitive function from those with cognitive impairment.21
Outcome Measures
Outcome measures included number of falls in the past 12 months and performance-based measures of functional reach,22 TUG,18 Short Physical Performance Battery (SPPB),23 and walk performance under single- and dual-task conditions.24 Participant falls data over the previous 12 months were obtained via their recall of fall events, which were defined as “when you land on the floor or the ground, or fall and hit objects like stairs or pieces of furniture, by accident.”17 At an in-person interview, participants were asked, “Have you fallen in the last three (six, nine) months?” and “Have you fallen in the last year?” At each question, we also asked how many falls they had. We sought to determine as accurate an estimate of the timing of any fall(s) and the number of falls as possible. To overcome the limitations related to recall,25 we also sought corroboration of participant self-reports with a proxy informant (78%).
Functional reach assessed the maximal distance (in cm) participants could reach forward, beyond arm’s length, while maintaining a fixed based of support in the standing position, with higher scores indicating better balance. The TUG measure assessed the time (in sec) taken to stand up from a standard armchair (approximate seat height, 46 cm; arm height, 65 cm), walk a distance of 3 m, turn, walk back to the chair, and sit down, with higher scores indicating more difficulty with the task. The SPPB included measures of 1) increasingly challenging standing balance tasks, 2) a 4-m walk (walk velocity), and 3) chair stands (leg strength). A single summary measure of SPPB was used, with the score ranging from 0 points (worst physical function) to 12 points (best physical function).
Participant walk performance was assessed via an Instrumental Timed Up and Go (ITUG) test (APDM, Inc.). Following an explanation of the walking procedures, participants were asked to stand up from an armless chair, walk for a distance of 14 m with no cognitive task (single-task walking), and then walk 14 m with a concurrent cognitive (arithmetic) assignment (dual-task walking) (ie, walking while performing a serial subtraction of 5 from a prior-determined number).24 The verbal instructions for these tasks included the following: “Walk at normal pace” (during both single- and double-task walking) and “perform as many subtractions as accurately as you can” (during dual-task walking).
The total walking duration (in seconds) during each walk trial was recorded. Two trials were administered under both the single-task condition and the dual-task condition (starting with the number 95 in trial 1 and 65 on trial 2). For the dual-task walk trials, the serial subtractions of 5 were not performed at random and no specific instructions were given regarding task prioritization. The order of the walking conditions was counterbalanced across participants. Scores (in seconds) from each of the walk conditions were averaged to represent single-task walk and dual-task walk. Using the average score ascertained from each walk, a dual-task cost measure was estimated as dual-task cost = ((dual-task – single-task)/single-task) x 100, with positive values (in percentage) indicating deteriorated walking performance in the dual-task condition (ie, dual-task cost) with respect to the single-task condition.
Covariates
As part of the study assessment, each participant completed a health survey that contained demographic and clinical information regarding age, race/ethnicity, gender (1 = men; 2 = women), level of education (elementary/middle/high school, community college, university degree or higher), health status (1 = very poor, 2 = poor, 3 = fair, 4 = good, 5 = very good, 6 = excellent), level of depression (with higher scores indicative of higher levels of depression),26 number of chronic diseases diagnosed (eg, arthritis, heart disease, high blood pressure, diabetes, etc.), and number of medication used (prescriptions). These measures were included as covariates in the data analysis.
Data Analyses
We conducted descriptive analyses, using analysis of variance for continuous variables and the chi-square (or Fisher’s Exact) test for categorical variables, to examine the demographic characteristics of the study population by cognitive status, with outcomes presented as means or percentages. Using the GENLIN procedure in SPSS, we performed Poisson regression analyses on falls count data to estimate falls prevalence and its 95% confidence interval (CI) between the impaired and unimpaired groups and univariate logistic regression to assess the association between cognitive impairment and the odds of having multiple falls (defined as having 2 or more falls). Given that there were multiple dependent variables, we performed MANOVA to examine whether there was a between-group difference (main effect) on any of the three physical performance measures (functional reach, TUG, SPPB) and dual-task cost during walking performance. In the presence of a main effect, follow-up univariate ANOVAs were performed. Between-group differences in means and their 95% CIs are presented. We performed all analyses with and without adjusting for age, gender, health status, chronic conditions, and medication use. For all statistical tests, two-sided P values of <0.05 were considered significant. There were no missing data in the study, and all analyses were conducted using SPSS version 26 (IBM Corp).
Results
A total of 670 older adults participated in the study. Descriptive information on participant demographic and clinical characteristics is shown in Table 1. Participants (mean age = 77.7 years, SD = ±5.6) were primarily white (92.1%) and female (65.1%). There were statistical differences between groups in the variables of age, gender, health status, and fall counts.
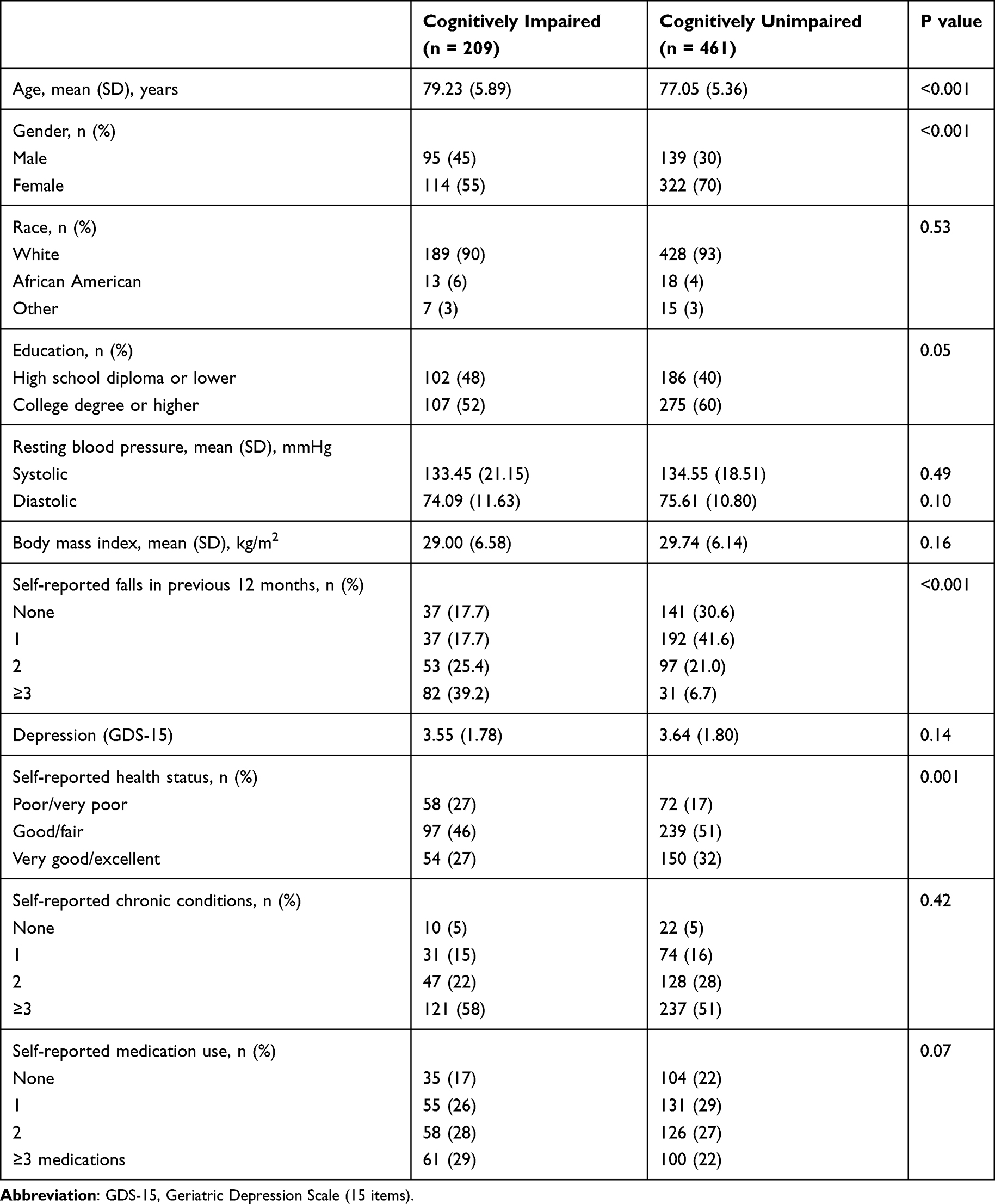 |
Table 1 Demographic and Clinical Characteristics of the Study Population by Cognitive Status |
Prevalence of Falls
The overall prevalence of falls during the previous year in the study population was 73.4% (95% CI, 70.08% to 76.78%; n = 492). There was a statistical difference in any falls and multiple falls between the two groups (Table 2), with a higher number of falls observed among those in the cognitively impaired group. Comparing participants with cognitive impairment to cognitively healthy participants, the prevalence of any fall was 82.3% (172/209 = 0.823) and 69.4% (320/461 = 0.694), respectively (p = 0.001). The fall prevalence ratio, derived from the unadjusted Poisson regression model, was 2.57 (unadjusted odds ratio [uOR]; 95% CI: 2.17 to 3.05), indicating a statistically significant difference in prevalence between the two groups, with those having a cognitive impairment being 2.6 times more likely to have fallen in the previous 12 months. The prevalence ratio remained unchanged after controlling for the a priori specified set of covariates, with the adjusted OR (aOR) = 2.51 (95% CI: 2.09 to 3.01).
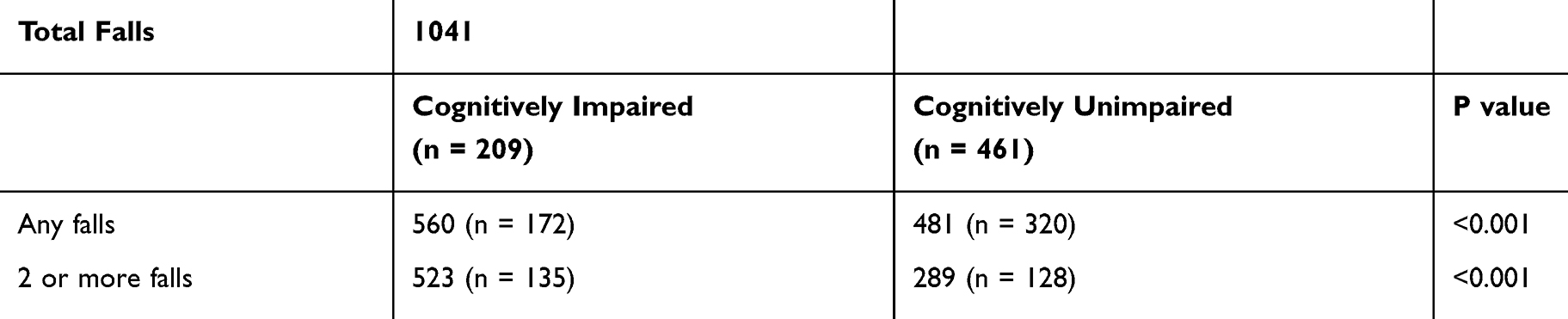 |
Table 2 Prevalence of Falls by Cognitive Status |
When the odds of falling and multiple falls were examined, the uOR from the unadjusted logistic regression model showed that those with impairment were 1.19 (95% CI, 1.09 to 1.29) times more likely to experience falling compared to the cognitively healthy older adults, and the estimate was relatively unchanged after adjustment with the covariates (aOR = 1.61, 95% CI, 1.06 to 1.28). For multiple falls, the uOR estimate showed that those with impairment were 2.33 (95% CI, 1.95 to 2.78) times more likely to experience multiple falls compared to the cognitively healthy older adults. The adjusted model estimate (aOR) was 2.23 (95% CI, 1.83 to 2.70).
Physical Performance and Dual-Task Cost During Walking
There was a statistically significant difference in physical and dual-task performance scores from MANOVA, F (4, 655) = 23.76, p <.0001; Wilk’s Λ = 0.88. Descriptive statistics for the outcome measures for each group are presented in Table 3. Compared with cognitively healthy participants, those with impairment showed worse performance on functional reach (mean difference [MD] = −2.33 cm, 95% CI: −3.21 to −1.46) (the negative value indicates shorter distance reached), TUG (MD = 3.05 s, 95% CI: 2.22 to 3.88) (the positive value indicates slower time), SPPB (MD = −1.24 points, 95% CI: −1.55 to −0.92) (the negative value indicates worse performance), and increase in dual-task cost (MD = 6.59%, 95% CI: 4.19 to 9.03) (the positive value indicates slower time).
 |
Table 3 Descriptive Statistics on the Study Outcome Measures by Cognitive Status |
Discussion
Findings from this cross-sectional study showed that community-dwelling older adults at high risk of falling with cognitive impairment were 2.6 times more likely to report a fall and more than twice as likely to experience multiple falls in the previous 12 months compared to their cognitively healthy peers. In addition, older adults with cognitive impairment also showed poorer physical performance and exhibited lower dual-task ability (as evidenced by high dual-task cost) during walking performance compared to cognitively unimpaired older adults.
The finding on falls is congruent with past studies. Cross-sectional studies have shown that older adults with mild cognitive impairment (MCI) were associated with a higher rate of falls.10,11 In a prospective study, Gleason et al27 showed that community-living older adults who scored worse incrementally on the global MMSE scale (ranging from 22 to 30 points, with higher scores indicating better cognitive function) significantly increased risk for falling over 12 months by about 20%, while a prospective study by Ansai et al7 found that more than 50% of older adults with MCI and mild Alzheimer’s disease reported falls over 6 months. A meta-analysis of cognitive impairment in fall risk showed that older adults with impairment on global cognitive measures were at greater risk for falls and serious fall-related injuries.13 The current study, however, is the first showing that among community-dwelling older adults at high risk of falls, those with cognitive impairment have an elevated rate of falls, suggesting that even among high-risk fallers, having a concomitant impairment in cognition elevates the fall risk.
In addition to increased risk of falling, current evidence indicates that older adults with cognitive impairment, including MCI, also exhibit functional deficits in the domains of balance and dual-task walking performance.3,13,28,29 Corroborating existing evidence, we showed that among those with high fall risk, those with cognitive impairment performed more poorly on mobility-related daily tasks involving upper and lower extremity functioning (eg, reaching, sit-to-stand, balance, and gait). These participants also showed higher dual-task costs in their performance of simultaneous motor and cognitive interference tasks during walking, suggesting greater cognitive deficits among high-risk fallers that may be attributed to impairment in attention allocation and executive function.30,31
Although the mechanisms precipitating falls among older adults with cognitive impairment, especially in those with high risk of falling, have not been clearly delineated, the literature on older adults with neurological deficits generally suggests that factors such as impaired attentional resource allocation and deficiencies in executive function and working memory may contribute to the increased propensity for falling.3 Other studies have indicated that gait abnormalities among older adults with cognitive impairment may also contribute to multiple falls and poorer performance of dual-task activities.29
Results of this study indicate the need for allocation of intervention resources directed toward this vulnerable population at high risk of falling. Currently, relatively few evidence-based interventions exist for community-dwelling older adults at high risk of falling and with cognitive impairment. Exercise prevents falls in older adults,32–34 and some emerging findings, albeit from a limited number of unpowered and small sample studies, suggest the potential of exercise to prevent falls in older adults with cognitive impairment.33,35 However, compelling evidence is lacking, and more targeted trials are needed to clarify this relationship. In addition, interventions may need to be specifically tailored to the functional cognition level of those older adults with cognitive impairment to achieve the desired results. Similarly, given the diminished multitask ability among this population, exercise interventions such as Tai Ji Quan,36,37 dance,38 or dual-tasking training39,40 may be well suited to providing appropriate training challenges for enhancing these abilities in this group.
Our study has some limitations. First, the data analyzed were cross-sectional, which precludes causal inferences about the direction of effects studied. Second, under our dual-task test condition, we used a serial subtraction of the number 5 rather than considering varying the number so that the level of task difficulty could be increased.30,41 Also, the lack of dual-task prioritization during walking represents another weakness in our assessment approach. Third, because participants were drawn from an exercise intervention trial there is a possibility of self-selection bias inherent in our study sample. Fourth, in quantifying risk, we used a global cognitive screening measure to define cognitive impairment. Other dimensions of cognition, for example, executive function may also be associated with increased risk of falling.42,43 Finally, our fall ascertainment relied primarily on self-reported retrospective data, which is known to be subject to recall bias.25 When possible, future studies should attempt to involve proxy informants to corroborate the recalls provided by the participants.
In conclusion, findings from this study add new knowledge to the literature showing that older adults at high risk for falls and who have cognitive impairment are associated with a greater risk for falls and impaired physical and dual-task performance. Our results highlight the clinical need for allocating intervention resources specifically targeting this high-risk older adult population to reduce falls and improve physical performance and dual-task abilities.
Acknowledgments
The study reported in this manuscript was supported by the National Institute on Aging (AG045094). The opinions expressed are those of the authors and do not necessarily represent the official views of the National Institute on Aging.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors of this paper reported no financial conflicts of interest.
References
1. United States Senate, Special Committee on Aging. Falls prevention: national, state, and local solutions to better seniors. Available from: https://www.aging.senate.gov/imo/media/doc/SCA_Falls_Report_2019.pdf.
2. Centers for Disease Control and Prevention. Subjective cognitive decline – a public health issue. Available from: https://www.cdc.gov/aging/aginginfo/docs/subjective-cognitive-decline-508.pdf.
3. Montero-Odasso M, Speechley M. Falls in cognitively impaired older adults: implications for risk assessment and prevention. J Am Geriatr Soc. 2018;66(2):367–375. doi:10.1111/jgs.15219
4. Centers for Disease Control and Prevention. Older Adults Falls. Available from: https://www.cdc.gov/homeandrecreationalsafety/falls/index.html.
5. World Health Organization. Falls. Available at: https://www.who.int/news-room/fact-sheets/detail/falls.
6. Bridenbaugh SA, Kressig RW. Epidemiology and falls risk factors in cognitively impaired older adults. In: Montero-Odasso M, Camicioli R, editors. Falls and Cognition in Older Persons. Cham: Springer; 2019:34–48.
7. Ansai JH, de Andrade LP, Masse FA, Gonçalves J, de Medeiros TAC, Vale FAC, Rebelatto RJ. Risk factors for falls in older adults with mild cognitive impairment and mild Alzheimer Disease. J Geriatric Phys Ther. 2019;42(3):E116–E121. doi:10.1519/JPT.0000000000000135
8. Gllali G, Launay CP, Blumen HM, et al. Falls, cognitive impairment, and gait performance: results from the GOOD Initiative. J Am Med Dir Assoc. 2017;18(4):335–340. doi:10.1016/j.jamda.2016.10.008
9. Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319(26):1701–1707. doi:10.1056/NEJM198812293192604
10. Tyrovolas S, Koyanagi A, Lara E, Santini ZI, Haro JM. Mild cognitive impairment is associated with falls among older adults: findings from the Irish longitudinal study on ageing (TILDA). Exp Gerontol. 2016;75:42–47.
11. Verghese J, Robbins M, Holtzer R, et al. Gait dysfunction in mild cognitive impairment syndromes. J Am Geriatr Soc. 2008;56(7):1244–1251. doi:10.1111/j.1532-5415.2008.01758.x
12. Delbaere K, Kochan NA, Close JC, et al. Mild cognitive impairment as a predictor of falls in community-dwelling older people. Am J Geriatr Psychiatry. 2012;20(10):845–853. doi:10.1097/JGP.0b013e31824afbc4
13. Muir SW, Gopaul K, Montero-Odasso M. The role of cognitive impairment in fall risk among older adults: a systematic review and meta-analysis. Age Ageing. 2012;41(3):299–308. doi:10.1093/ageing/afs012
14. Wollacott M, Sumway-Cook A. Attention and the control of posture and gait: a review of an emerging area of research. Gait Posture. 2002;16(1):1–14. doi:10.1016/S0966-6362(01)00156-4
15. Alzheimer’s Association. Alzheimer’s Association Report: 2019 Alzheimer’s disease and facts and figures. Alzheimer’s Dem. 2019;321–387(6):1641–1648. doi:10.1152/ajplegacy.1975.229.6.1641
16. Mayeux R, Stern Y. Epidemiology of Alzheimer disease. Cold Spring Harb Perspect Med. 2012;2(8):a006239. doi:10.1101/cshperspect.a006239
17. Li F, Harmer P, Fitzgerald K, et al. Effectiveness of a therapeutic Tai Ji Quan intervention versus a multimodal exercise intervention to prevent falls among older adults at high risk of falling: A randomized clinical trial. JAMA Intern Med. 2018;178(10):1301–1310. doi:10.1001/jamainternmed.2018.3915
18. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
19. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
20. Bernstein IH, Lacritz L, Barlow CE, Weiner MF, DeFina LF. Psychometric evaluation of the Montreal Cognitive Assessment (MoCA) in three diverse samples. Clin Neuropsychol. 2011;25(1):119–126. doi:10.1080/13854046.2010.533196
21. Carson N, Leach L, Murphy KJ. A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int J Geriatr Psychiatry. 2018;33:379–388. doi:10.1002/gps.4756
22. Duncan PW, Weiner DK, Chandler J, Studenski S. Functional reach: a new clinical measure of balance. J Gerontol. 1990;45(6):M192–M197. doi:10.1093/geronj/45.6.M192
23. Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–M94. doi:10.1093/geronj/49.2.M85
24. Li F, Harmer P, Chou LS. Dual-task walking capacity mediates Tai Ji Quan impact on physical and cognitive function. Med Sci Sports Exerc. 2019;51(11):2318–2324. doi:10.1249/MSS.0000000000002051
25. Garcia PA, Dias JM, Silva SL, Dias RC. Prospective monitoring and self-report of previous falls among older women at high risk of falls and fractures: a study of comparison of agreement. Braz J Phys Ther. 2015;19(3):218–226. doi:10.1590/bjpt-rbf.2014.0095
26. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontol. 1986;5(1/2):165–173. doi:10.1300/J018v05n01_09
27. Gleason CE, Gangnon RE, Fischer BI, Mahoney JE. Increased risk for falling associated with subtle cognitive impairment: secondary analysis of a randomized clinical trial. Dement Geriatr Cogn Disord. 2009;27:557–563. doi:10.1159/000228257
28. Bahureska L, Najafi B, Saleh A, et al. The impact of mild cognitive impairment on gait and balance: a systematic review and meta-analysis of studies using instrumented assessment. Gerontol. 2017;63:67–83. doi:10.1159/000445831
29. Taylor ME, Delbaere K, Milkolarizak AS, Stephen RL, Close J. Gait parameter risk factors for falls under simple and dual task conditions in cognitively impaired older people. Gait Pos. 2013;37(1):126–130. doi:10.1016/j.gaitpost.2012.06.024
30. Hall CD, Echt KV, Wolf SL, Rogers WA. Cognitive and motor mechanisms underlying older adults’ ability to divide attention while walking. Phys Ther. 2011;91(7):1039–1050. doi:10.2522/ptj.20100114
31. Srygley JM, Mirelman A, Herman T, Giladi N, Hausdorff JM. When does walking alter thinking? Age and task associated findings. Brain Res. 2009;1253:92–99. doi:10.1016/j.brainres.2008.11.067
32. Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012;9(9):CD007146.
33. Sherrington C, Michaleff ZA, Fairhall N, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. 2017;51(24):1750–1758. doi:10.1136/bjsports-2016-096547
34. Tricco AC, Thomas SM, Veroniki AA, et al. Comparisons of interventions for preventing falls in older adults: a systematic review and meta-analysis. JAMA. 2017;318(17):1687–1699. doi:10.1001/jama.2017.15006
35. Chan WC, Yeung JW, Wong CS, et al. Efficacy of physical exercise in preventing falls in older adults with cognitive impairment: a systematic review and meta-analysis. J Am Med Dir Assoc. 2015;16(2):149–154. doi:10.1016/j.jamda.2014.08.007
36. Li F, Harmer P, Liu Y, Chou LS, Tai J. Quan and global function in older adults with cognitive impairment: a pilot study. Arch Gerontol Geriatr. 2014;58(3):434–439. doi:10.1016/j.archger.2013.12.003
37. Wayne PM, Walsh JN, Taylor-Piliae RE, et al. Effect of Tai Chi on cognitive performance in older adults: systematic review and meta-analysis. J Am Geriatr Soc. 2014;62:25–39. doi:10.1111/jgs.12611
38. Meng X, Li G, Jia Y, et al. Effects of dance intervention on global cognition, executive function and memory of older adults: a meta-analysis and systematic review. Aging Clin Exp Res. 2020;32(1):7–19. doi:10.1007/s40520-019-01159-w
39. Ghai S, Ghai I, Effenberg AO. Effects of dual tasks and dual-task training on postural stability: a systematic review and meta-analysis. Clin Interv Aging. 2017;12:557–577. doi:10.2147/CIA.S125201
40. Wollesen B, Schulz S, Seydell L, Delbaere K. Does dual task training improve walking performance of older adults with concern of falling? BMC Geriatr. 2017;17:213. doi:10.1186/s12877-017-0610-5
41. Chu YH, Tang PF, Peng YC, Chen HY. Meta-analysis of type and complexity of a secondary task during walking on the prediction of elderly falls. Geriatr Geroontol Int. 2013;13(2):289–297. doi:10.1111/j.1447-0594.2012.00893.x
42. Muir SW, Speechley M, Wells J, Borrie M, Gopaul K, Montero-Odasso M. Gait assessment in mild cognitive impairment and Alzheimer’s disease: the effect of dual-task challenges across the cognitive spectrum. Gait Pos. 2012;31(1):96–100. doi:10.1016/j.gaitpost.2011.08.014
43. Montero-Odasso M, Muir SW, Speechley M. Dual-task complexity affects gait in people with mild cognitive impairment: the interplay between gait variability, dual tasking, and risk of falls. Arch Phys Med Rehab. 2012;93(2):293–299. doi:10.1016/j.apmr.2011.08.026
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.