Back to Journals » International Journal of Women's Health » Volume 17
Prevalence of, and Factors Associated with Hemodynamic Instability Among Women Presenting with Incomplete Abortion at a Tertiary Hospital in Southwestern Uganda
Authors Kakama C ![]() , Agaba DC, Byamukama O
, Agaba DC, Byamukama O ![]() , Kajabwangu R
, Kajabwangu R ![]() , Kengonzi E, Akol MA, Muhumuza A, Businge J, Turanzomwe S
, Kengonzi E, Akol MA, Muhumuza A, Businge J, Turanzomwe S ![]() , Ainomugisha B, Kalyebara KP, Kayondo M, Ngonzi J, Muganwa WG, Lugobe HM
, Ainomugisha B, Kalyebara KP, Kayondo M, Ngonzi J, Muganwa WG, Lugobe HM ![]()
Received 28 January 2025
Accepted for publication 27 May 2025
Published 30 May 2025 Volume 2025:17 Pages 1547—1556
DOI https://doi.org/10.2147/IJWH.S515760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Caxton Kakama,1 David Collins Agaba,2 Onesmus Byamukama,3 Rogers Kajabwangu,1,3 Elizabeth Kengonzi,1 Mathiang Agany Akol,1 Amos Muhumuza,1 Julius Businge,1 Stuart Turanzomwe,1 Brenda Ainomugisha,1 Kato Paul Kalyebara,1 Musa Kayondo,1 Joseph Ngonzi,1 Wasswa George Muganwa,3 Henry Mark Lugobe1
1Department of Obstetrics and Gynecology, Mbarara University of Science and Technology, Faculty of Medicine, Mbarara, Uganda; 2Department of Physiology, Mbarara University of Science and Technology, Faculty of Medicine, Mbarara, Uganda; 3Department of Obstetrics and Gynecology, Mbarara Regional Referral Hospital, Mbarara, Uganda
Correspondence: Caxton Kakama, Department of Obstetrics and Gynaecology, Mbarara University of Science and Technology, Faculty of Medicine, Mbarara, 1410, Uganda, Tel +256 777465000, Email [email protected]
Background: Sub-Saharan Africa has a high abortion case-fatality rate, and most of these maternal deaths are due to hemodynamic instability which results from hemorrhage, especially in cases of incomplete abortion. Timely identification and management of hemodynamic instability is an important strategy for addressing the morbidity and mortality associated with incomplete abortion. This study, therefore, aimed at determining the prevalence and factors associated with hemodynamic instability among women presenting with incomplete abortion at Mbarara Regional Referral Hospital (MRRH).
Methods: We conducted a cross-sectional study at the gynaecology ward of MRRH from January 2024 to April 2024. We consecutively enrolled women with incomplete abortion and collected data on socio-demographic, abortion- and medical-related factors, and measured their blood pressure and heart rate at admission. Obstetric shock index (OSI), the ratio of the heart rate to systolic blood pressure, was used as a measure of haemodynamic stability. A participant whose OSI was ≥ 0.9 was considered haemodynamically unstable. We performed a modified Poisson regression analysis to determine the factors associated with hemodynamic instability.
Results: A total of 137 women with incomplete abortion were enrolled in this study with a mean age of 26.3 (± 5.93) years. The majority of the participants had first-trimester abortions (65.7%), were married (70.8%), and were from rural areas (60.0%). The prevalence of hemodynamic instability was 41.6% (95% CI: 33.6– 50.1). At multivariable regression analysis, gestation age ≥ 13 weeks (aPR 1.67, 95% CI: 1.12– 2.49) and post-abortion infection (aPR 1.75, 95% CI: 1.18– 2.60) were significantly associated with hemodynamic instability.
Conclusion: Approximately two in every five women with incomplete abortion at MRRH were hemodynamically unstable at admission during the study period. Women with second trimester abortion and those with post-abortion infection are more likely to present with hemodynamic instability. We recommend strengthening routine assessment and management of hemodynamic instability among women with incomplete abortion.
Keywords: incomplete abortion, hemodynamic instability, obstetric shock index, post-abortion infection
Introduction
Globally, 8% of all maternal deaths are attributed to abortion-related complications, according to the 2025 WHO systematic analysis on global and regional causes of maternal deaths.1 Sub-Saharan Africa has the highest abortion case-fatality rate of 185 deaths per 100,000 abortions compared to other global regions.1,2 Most of these maternal deaths are due to the excessive hemorrhage that complicates incomplete abortion.3 In Uganda, abortion-related complications account for 7% of all maternal deaths in the country,4,5 and the proportion is even as higher (12%) at Mbarara Regional Referral Hospital.6
Hemodynamic instability is a complication that may indicate the severity of incomplete abortion and refers to a condition where the body is unable to maintain adequate blood pressure and blood supply to the vital organs.7,8 Hemodynamic instability can result into the need for blood transfusion, multi-organ failure, or even death if left uncorrected.9 Hemodynamic instability occurs as a result of hemorrhage which causes a decrease in the preload, cardiac output and blood pressure, resulting in an instantaneous compensatory rise in the maternal heart rate due to sympathetic tone activation mediated by the baroreceptor reflex.7,8 Hemodynamic instability can also occur following septic abortion, which results in hypotension due to generalized vasodilatation as well as fluid extravasation into the extracellular space due to endothelial injury mediated by bacterial endotoxins.10,11 Assessment of the hemodynamic status of women with incomplete abortion at admission is thus important for timely identification and management before the occurrence of severe complications like multi-organ failure.12 The obstetric shock index, the ratio of heart rate to systolic blood pressure, is a simple cost-effective and better predictor and indicator of hemodynamic impairment compared to other parameters like mean arterial blood pressure, pulse rate, systolic blood pressure and diastolic blood pressure used independently13,14 This is because it utilizes the early rise in heart rate following hemorrhage before the blood pressure falls. There is a dearth of data on the prevalence of hemodynamic instability in women who have had an incomplete abortion, however, a study done in Ethiopia reported a prevalence of 14.4%. Some factors have been found to be associated with hemodynamic instability and these include: age, occupation, marital status, residence, level of education, referral status, duration of bleeding, mode of termination, gestation age, delayed presentation, history of uterine evacuation, post-abortion infection and HIV status.15–18
This study aimed at determining the prevalence of, and factors associated with hemodynamic instability among women presenting with incomplete abortion at MRRH, in southwestern Uganda, to help formulate evidence-based interventions aimed at reducing abortion-related morbidity and mortality.
Methods
Study Setting, Study Design and Study Population
This was a hospital-based cross-sectional study conducted from January 2024 to April 2024 at the gynecological ward of Mbarara Regional Referral Hospital, a public tertiary hospital that serves about 3,000,000 people in southwestern Uganda. The hospital is a referral center and a teaching hospital for Mbarara University of Science and Technology. The gynecological ward is composed of three sections; the admission area where vital signs measurement and stabilization are routinely done for women with incomplete abortion, the procedure room where women with incomplete abortion are done manual uterine evacuation from and the ward area where patients are admitted after stabilization. Other post-abortion care services like counseling and family planning are also provided in a side room on the ward. The gynecological unit also has a gynecological outpatient clinic where these women are reviewed as well as linking them to other reproductive health services. The hospital also has an operating theatre where women with abortion complications like a perforated uterus can be operated from and in addition, there is also an intensive care unit where those who are critically ill and require mechanical ventilation are admitted. The obstetrics and gynecology department has obstetricians and gynecologists, resident doctors and a nursing team who can diagnose and manage women with incomplete abortion and other gynecological conditions. On average 30 women with incomplete abortion are managed every month. The restrictive abortion law in Uganda is one of the factors that increases the prevalence of illegal abortion, which escalates its adverse effects on maternal health.
Our study population was all women with incomplete abortion admitted at the gynecological ward of MRRH. All women with a diagnosis of incomplete abortion were enrolled in this study. A woman with incomplete abortion was one with; pre-vaginal bleeding, open cervical os and a history of partial expulsion of products of conception confirmed clinically or radiologically, at a gestation age less than 26 weeks as determined from the last normal menstrual period or first-trimester ultrasound scan.9 We excluded all women who were known to have hypertensive disease from the study as hypertension alters the autonomic regulation and therefore affects the pulse rate and thus affects the obstetric shock index.
Sample Size and Sampling
The sample size was calculated using OpenEpi online software, and we considered the proportion of hemodynamic instability among women with incomplete abortion as 50% since this has not been documented in our setting, and assumed a finite population of 180 women with incomplete abortion who could be accessed during the study period, a 95% confidence interval and a margin error of 5%.19,20 This gave a sample size of 123 participants and after adjusting for a 10% non-response rate, the final sample size was 137 participants. Consecutive sampling was used to enroll all eligible participants until the desired sample size was obtained.
Data Collection Procedures and Study Variables
Data were collected by two research assistants using interviewer-administered structured questionnaires. The research assistants were nurses, who were trained on the data collection tool, blood pressure measurement and on how to consent study participants.
The dependent variable was hemodynamic instability and was measured using obstetric shock index (OSI) calculated as heart rate (HR) divided by systolic blood pressure (SBP), using the vital signs measured at admission before initiation of any intervention.13,14 A woman with an OSI of ≥0.9 was considered to have hemodynamic instability. Blood pressure and pulse rate were measured using an automated calibrated patient monitor (Mindray UMEC10 Vital Sign Patient Monitor, Shenzhen Mindray Bio-Medical Electronics Co., Ltd, China). An appropriate-sized cuff that covered at least two-thirds of the length of the right upper arm and the entire circumference of the arm was attached as well as a pulse oximeter probe attached to the middle finger of the left arm. The participant was asked to remain quiet as the machine took measurements. The cuff inflated and deflated automatically after pressing the start button and then displayed the BP and pulse rate on the screen of the monitor.
The independent variables included both continuous and categorical variables. Continuous variables were age, parity, number of previous abortions and gestational age. Categorical variables included: occupation, residence, education level, referral status, marital status, induced abortion, previous history of uterine evacuation, delayed presentation, planned pregnancy, post-abortion infection and HIV status. Delayed presentation was considered to be a duration of more than 6 hours from the time of onset of vaginal bleeding to the time of admission. Married was considered as living with a partner. Post-abortion infection was considered to be present if there was foul-smelling products of conception/discharge and a fever (body temperature of ≥37.5OC).
Data Management and Analysis
We used a coded questionnaire to collect data. All data was cross-checked for completeness or discrepancies. Data from the questionnaires was entered into Research Electronic Data Capture (REDCap®) software and was exported to STATA software version 17 for cleaning and analysis. Data was analyzed using STATA software version 17 (Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC USA). Continuous variables were presented as mean ± Standard Deviation, while categorical variables were presented as frequencies and percentages. Prevalence of hemodynamic instability was computed as the number of participants with an obstetric shock index greater than or equal to 0.9 expressed as a percentage of the total participants. Factors associated with hemodynamic instability were determined using modified Poisson regression. Biologically plausible variables and those with a p-value of less than 0.2 from the bivariate model were added to the final multivariable analysis model and those variables with a p-value <0.05 were statistically significant.
Results
During the study period, 141 women with incomplete abortion were admitted on the gynaecology ward. However, we excluded 4 women as they had a known history of hypertension. We therefore enrolled 137 participants, 57 of whom were hemodynamically unstable at admission as shown in Figure 1.
 |
Figure 1 Flow chart of the participants. |
Baseline Characteristics of Study Participants
The mean age of the study participants was 26.34±5.93 years. The majority were aged 20–34 years (76.6%), staying in rural areas (60.6%), married (70.8%) and were peasant farmers (62.0%). When stratified by hemodynamic stability status, participants did not differ based on baseline characteristics, as shown in Table 1.
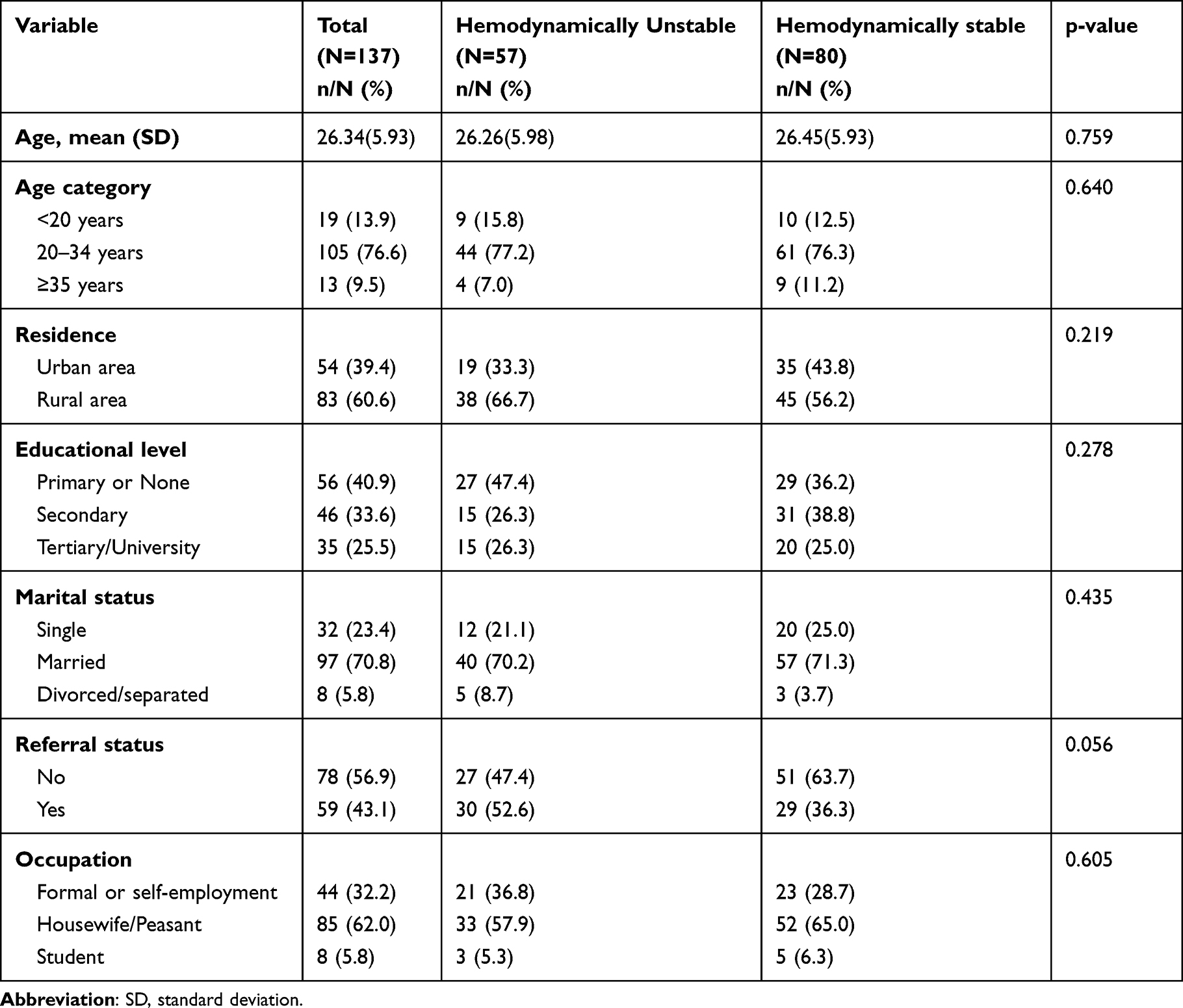 |
Table 1 Baseline Characteristics of the Participants |
Medical and Abortion Related Characteristics of the Participants
The majority of the participants presented in first trimester (65.7%) and had no prior history of abortion (55.5%). The proportion of participants with post-abortion infection was higher among women who were hemodynamically unstable than those who were stable (43.9% vs 12.5%, p-value <0.001), and the proportion of women in second trimester who were hemodynamically unstable was higher than those who were hemodynamically stable (47.4% vs 25%, p-value 0.007), as shown in Table 2.
 |
Table 2 Medical and Abortion Related Factors |
Prevalence of Hemodynamic Instability
Out of the 137 patients with incomplete abortion enrolled in the study, 57 participants had an OSI ≥ 0.9 and thus were hemodynamically unstable, giving a prevalence of hemodynamic instability among women presenting with incomplete abortion at MRRH of 41.6% (95% CI: 33.6–50.1).
Factors Associated with Hemodynamic Instability
Factors associated with hemodynamic instability included gestation age ≥13 weeks (aPR 1.67, 95% CI: 1.12–2.49) and post-abortion infection (aPR 1.75, 95% CI: 1.18–2.60). Women with second trimester abortion were 1.67 times more likely to be hemodynamically unstable at admission compared to those admitted with first-trimester abortion. Also, women with post-abortion infection at admission were about 1.75 times more likely to present with hemodynamic instability compared to those who had no post-abortion infection, as shown in Table 3.
 |
Table 3 Bivariable and Multivariable Modified Poisson Regression Analysis for Factors Associated with Hemodynamic Instability |
Discussion
In this study, the prevalence of hemodynamic instability among women presenting with incomplete abortion at MRRH is 41.6%. Hemodynamic instability in patients with incomplete abortion results from vaginal bleeding that leads to decreased intravascular volume, venous return, cardiac output, and blood pressure, ultimately resulting in hemodynamic instability.21,22
This prevalence of hemodynamic instability is high possibly because we studied women with incomplete abortion, which is associated with vaginal bleeding that leads to decreased intravascular volume, venous return, cardiac output, and blood pressure, ultimately resulting in hemodynamic instability.21,22 This could also be because the majority of participants presented more than 6 hours from the onset of vaginal bleeding (76.6%) which could have increased the amount of blood loss and thus predisposing them to hemodynamic instability. The study site was also a tertiary hospital and thus receives patients referred from peripheral health facilities who may present with severe complications of incomplete abortion.
There is a paucity of literature on the prevalence of hemodynamic instability among women presenting with incomplete abortion making it difficult to compare our findings. However, this prevalence was higher than that found in a health facility-based cross-sectional study conducted at Yirgalem General Hospital, Sidama Zone, Southern Ethiopia that aimed at determining the factors associated with management outcomes among women with incomplete abortion where 14.4% had hypovolemic shock (hemodynamic instability). This prevalence was lower compared to our study because the assessment for hypovolemic shock in the Ethiopian study was at discharge after the initiation of interventions.15
In this study, women admitted with second-trimester (≥13 weeks of gestation) incomplete abortion were 1.67 times more likely to be hemodynamically unstable at admission compared to those admitted with first-trimester abortion. Similar findings have been reported in Ethiopia, Uganda, Brazil and Argentina.15,18,23,24 Similarly, another study conducted in Italy to evaluate maternal complications of first trimester and second-trimester termination of pregnancy showed that maternal complications were significantly higher in the second trimester compared to first trimester.25 This is because at the gestation age ≥13 weeks, there is firm attachment of the placenta on to the endometrium and this predisposes to retained placenta following an abortion, thus increasing the blood loss which can lead to hemodynamic instability. In addition, gestation age ≥13 weeks is associated with more retained products of conception compared to first trimester abortion, which could predispose to excessive vaginal bleeding thus hemodynamic instability.23,26,27
In this study, women who had post-abortion infection were 1.75 times more likely to present with hemodynamic instability compared to those who had no post-abortion infection. This is similar to studies done in India and Kenya.26,28 This is because infection/sepsis causes a dysregulated immune response leading to the excessive release of pro-inflammatory cytokines that trigger systemic inflammation, causing vasodilation and increased vascular permeability. As the dysfunction of the immune response, endothelium, and microcirculation progresses, the body’s ability to maintain blood pressure and tissue perfusion becomes compromised, leading to hypotension and a compensatory increase in heart rate, hence hemodynamic instability.29–31
Our study is important because it highlights the need for continuous assessment of women with incomplete abortion, a major cause of maternal morbidity and mortality. It is novel because it utilizes obstetric shock index, an objective way to assess the haemodynamic status of patients with abortion-related hemorrhage using simple equipment to guide resuscitative interventions.
The study, however, had some limitations; It was a hospital-based study which may limit its generalizability to women in other facilities and the community. Hemodynamic instability was assessed based solely on OSI, however, OSI does not account for confounding conditions such as dehydration or pre-existing cardiac conditions, which could also affect the index. We also did not assess variables like nutritional status, anemia, and prior blood loss before admission, which also have an impact on the OSI. The diagnosis of post-abortion infection was based only on the presence of a raised temperature and foul-smelling products of conception/discharge. Although this is the routine practice in this setting due to the unavailability of the necessary investigations, it could have led to an overestimation of the rate of post-abortion infection.
Conclusion
The prevalence of hemodynamic instability among women presenting with incomplete abortion at MRRH is high. Women with incomplete abortion who are in the second trimester (≥13 weeks of gestation) and those with post-abortion infection are more likely to present with hemodynamic instability. We recommend strengthening of routine assessment and management of hemodynamic instability using obstetric shock index for all women with incomplete abortion at admission, and a study to determine the outcomes of women incomplete abortion who present with hemodynamic instability at MRRH. We also recommend the use of family planning services to prevent unplanned/unwanted pregnancies.
List of Abbreviations
Arr, adjusted risk ratios; CI, confidence interval; OSI, obstetric shock index; MRRH, Mbarara Regional Referral Hospital.
Data Sharing Statement
The datasets generated and analysed for this study are available from the corresponding author, upon reasonable request.
Ethics Approval and Consent to Participate
This study was performed in accordance with the principles stated in the Declaration of Helsinki. We obtained approval from the Mbarara University of Science and Technology Research Ethics Committee under reference number- MUST 2023-1225 and obtained administrative permission from Mbarara Regional Referral Hospital. All the study participants gave written informed consent.
Acknowledgment
We are grateful for the support from all the Obstetrics and Gynecology Department members of Mbarara University of Science and Technology and the administration of Mbarara Regional Referral Hospital during the study period. We also thank the research assistants and the study participants for agreeing to participate in the study.
This manuscript is available as a preprint on Research Square under the following link; https://www.researchsquare.com/article/rs-5529525/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
The authors declare that they have no competing interests with regard to the publication of this work.
References
1. Cresswell JA, Alexander M, Chong MYC, et al. Global and regional causes of maternal deaths 2009–20: a WHO systematic analysis. Lancet Glob Health. 2025;13(4):e626–e634. doi:10.1016/S2214-109X(24)00560-6
2. Say L, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–33. doi:10.1016/S2214-109X(14)70227-X
3. Bankole A, et al. From unsafe to safe abortion in Sub-Saharan Africa: slow but steady progress. 2020.
4. MOH, Uganda ministry of health annual health sector performance report 2020/2021. 2021.
5. UBOS I. UBOS. Uganda demographic and health survey. 2016.
6. Lugobe HM, et al. 490 Maternal mortality at a referral hospital in south western Uganda: a 5 year descriptive analysis. Am J Clin Exp Obstet Gynecol. 2021;224(2):S311–S312. doi:10.1016/j.ajog.2020.12.511
7. Bose EL, Hravnak M, Pinsky MR. The interface between monitoring and physiology at the bedside. Crit Care Clin. 2015;31(1):1–24. doi:10.1016/j.ccc.2014.08.001
8. Guyton JE, Hall ME. Guyton and Hall Textbook of Medical Physiology e-Book. Elsevier Health Sciences; 2020.
9. WHO. Abortion Care Guideline; 2022.
10. Prepeliță M, Lavric I. Septic abortion: clinical presentation and management. MedEspera. 2022.
11. Ahmed S, Hasnat DMA, Khair DMA, et al. Types of abortion and its consequences-a study of 100 cases in Mymensingh Medical College Hospital. Sch J App Med Sci. 2022;10:1774–1779. doi:10.36347/sjams.2022.v10i10.033
12. Birkhahn RH, et al. Shock index in diagnosing early acute hypovolemia. Am J Emerg Med. 2005;23(3):323–326. doi:10.1016/j.ajem.2005.02.029
13. El Ayadi AM, et al. Vital sign prediction of adverse maternal outcomes in women with hypovolemic shock: the role of shock index. PLoS One. 2016;11(2):e0148729. doi:10.1371/journal.pone.0148729
14. Borovac-Pinheiro A, Pacagnella RC, Morais SS, et al. Standard reference values for the shock index during pregnancy. Int J Gynecol Obstet. 2016;135(1):11–15. doi:10.1016/j.ijgo.2016.03.024
15. Gebretsadik A. Factors Associated with Management Outcome of Incomplete Abortion in Yirgalem General Hospital, Sidama Zone, Southern Ethiopia. Obstetrics and Gynecology International; 2018:2018.
16. Adanikin A, Umeora O, Nzeribe E, et al. Maternal near-miss and death associated with abortive pregnancy outcome: a secondary analysis of the Nigeria near-miss and maternal death survey. BJOG. 2019;126(S3):33–40. doi:10.1111/1471-0528.15699
17. Singh S, Hussain R, Shekhar C, et al. Incidence of treatment for postabortion complications in India, 2015. BMJ Global Health. 2020;5(7):e002372. doi:10.1136/bmjgh-2020-002372
18. Atuhairwe S, Gemzell-Danielsson K, Byamugisha J, et al. Abortion-related near-miss morbidity and mortality in 43 health facilities with differences in readiness to provide abortion care in Uganda. BMJ Global Health. 2021;6(2):e003274. doi:10.1136/bmjgh-2020-003274
19. Dean A, et al. OpenEpi. Open source epidemiologic statistics for public health, version. 2013;2(1).
20. Mbarara regional referral hospital- annual gynaecology ward report 2021/2022. 2022.
21. Hooper N, Armstrong TJ. Hemorrhagic Shock. StatPearls Publishing; 2022.
22. Cannon JW. Hemorrhagic shock. N Engl J Med. 2018;378(4):370–379. doi:10.1056/NEJMra1705649
23. Tariku M. Magnitude of severe acute maternal morbidity and associated factors related to abortion: a cross-sectional study in hawassa university comprehensive specialized hospital, Ethiopia, 2019. Biomed Res. Int. 2020;2020:1781652. doi:10.1155/2020/1781652
24. Romero M, Gomez Ponce de Leon R, Baccaro LF, et al. Abortion-related morbidity in six Latin American And Caribbean countries: findings of the WHO/HRP multi-country survey on abortion (MCS-A). BMJ Global Health. 2021;6(8):e005618. doi:10.1136/bmjgh-2021-005618
25. Garofalo G, Garofalo A, Sochirca O, et al. Maternal outcomes in first and second trimester termination of pregnancy: which are the risk factors? Journal of Perinatal Medicine. 2018;46(4):373–378. doi:10.1515/jpm-2017-0106
26. Ziraba AK, et al. Unsafe abortion in Kenya: a cross-sectional study of abortion complication severity and associated factors. BMC pregnancy childbirth. 2015;15:1–11.
27. Gutierrez G, Reines H, Wulf-Gutierrez ME, Riou B. Clinical review: hemorrhagic shock. Critical Care. 2004;8:1–9. doi:10.1186/cc2404
28. Bisht V, Rawat U, Bhaisora CP, et al. Study of septic abortion cases at a tertiary centre of Uttarakhand. J Ind Academy Forensic Med. 2012;34(4):315–317. doi:10.1177/0971097320120411
29. Litell JM, Shapiro NI, et al. Pathophysiology of septic shock. In: Webb A, editor. Oxford Textbook of Critical Care. Oxford University Press; 2016.
30. Minasyan H. Sepsis and septic shock: pathogenesis and treatment perspectives. J Crit Care. 2017;40:229–242. doi:10.1016/j.jcrc.2017.04.015
31. Lapointe V, Jocov D, Denault A. Hemodynamic instability in septic shock. Can J Anaesth. 2009;56:864–867. doi:10.1007/s12630-009-9168-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.