Back to Archived Journals » Open Access Surgery » Volume 15
Prevalence and Predictors of Preoperative Functional Disability Among Patients Scheduled for Elective Surgery in Northwest Ethiopia: A Multi-Center Cross-Sectional Study
Authors Zeleke ME ![]() , Chekol WB
, Chekol WB ![]() , Kassahun HG
, Kassahun HG ![]() , Mekonnen ZA
, Mekonnen ZA
Received 17 January 2022
Accepted for publication 13 April 2022
Published 26 April 2022 Volume 2022:15 Pages 45—56
DOI https://doi.org/10.2147/OAS.S358809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Mulualem Endeshaw Zeleke, Wubie Birlie Chekol, Habtamu Getinet Kassahun, Zemenay Ayinie Mekonnen
Department of Anesthesia, University of Gondar, Gondar, Northwest, Ethiopia
Correspondence: Wubie Birlie Chekol, Email [email protected]
Background: Assessment of preoperative functional disability is vital for health status information. It is associated with an increase in perioperative risk of morbidity and mortality. Preoperative period is a critical time to enhance patient’s functional recovery. So, this study aimed to assess the prevalence and associated factors of preoperative functional disability among patients scheduled for elective surgery.
Methods: Institution-based, multi-center, cross-sectional study was conducted in three Northwest Ethiopia referral hospitals from April 2021 to June 2021. Patients who scheduled for elective surgery in surgical, orthopedic, gynecology and ophthalmology wards were interviewed with semi-structured questionnaires. Functional disability was assessed by using a 12-item World Health Organization Disability Assessment schedule. Data were analyzed by SPSS version26.0. Binary logistic regression analysis was used to determine the associated variables.
Results: A total of 403 patients who scheduled for elective surgery with mean age of (43.21 ± 16.18) years were included. The prevalence of preoperative functional disability was 34.5% (95% CI: 29.8, 39). Alcohol consumption (AOR: 2.05, 95% CI; 1.11, 3.77), malnutrition (AOR: 6.85, 95% CI; 3.06, 15.33), pain (AOR: 2.26, 95% CI; 1.28, 3.99) and depression (AOR: 7.90, 95% CI; 4.16, 15.01) were significantly associated with functional disability.
Conclusion: The prevalence of preoperative functional disability was high. Alcohol consumption, nutritional deficiency, pain and depression were among the modifiable risk factors. So, added vigilance is needed in patients with these modifiable risk factors before surgery.
Keywords: preoperative assessment, activity limitation, patient health questionnaire
Introduction
Functional disability is defined as limitations or difficulties in any area of functioning or performing activities that relates to environmental, personal as well as health-related factors. It is a broad term used to describe the limitations and restrictions of performing activities, which can be defined as the need for help or difficulty in performing basic daily functions that are essential for an autonomous life in society.1–4
According to the International Classification of Functioning, Disability and Health (ICF) disability is an umbrella term, encompassing impairment, activity limitations and participation restrictions. Based on World Health Organization’s report, developed countries comprise about 10% of the population who have some kind of functional disability and this percentage rising to about 15% in developing countries.4–6 In preoperative patients, the problem was profound and its burden was nearly double (29.2%) compared to the population.7
Surgical patients may have multiple problems in the preoperative period that impose functional disability due to the disease that surgery was being needed or other else, then those surgical patients need vigorous attention and preoperative advanced assessment including investigation, however, the rapid increment of a number of surgeries performed does not allow the professionals to give multifaceted intervention to all patients in this period.8
It has been associated with multidimensional factors including sex, age, low education level, alcohol consumption, history of cerebrovascular diseases, cognitive impairment and hospitalization.9–11 It associated with a number of non-communicable diseases,12 musculoskeletal problems,13 obesity14 and it increases the number of hospitalization, increased risk of morbidity and mortality.15,16
In hospitalized patients decreased functional status is the strongest predictor of 6-month mortality, prolonged length of stay and readmissions to the hospital.17 Preoperative risk factors for postoperative morbidity and mortality are well established.18 A study by Carli et al provided a reasonable evidence that low preoperative physical fitness was associated with postoperative adverse events.19
Current evidence advocates that the preoperative period might be a better time to employ rehabilitative strategies and engage patients in activities to prepare for upcoming surgery than therapy after surgery that might not be the best, as patients are fatigued, in pain, and anxious about the final prognosis and potential future impairments. Preoperative optimization does not only improve pre-existing comorbidities pharmacologically but also to enhances physical fitness by rehabilitation before surgery within a relatively short period of time.7,8,19,20 Clinical studies on the causes and preventive measures of functional disability are therefore requisite for appropriate health policy and planning. To give optimal care, to formulate plans, policies, programs, and strategies a number of reliable data on disability and its association with other comorbidities are required.10
Therefore, due to limited study on its type in Ethiopia, major health problems of preoperative functional disability, increased numbers of surgical cases, and difficulty in providing multifaceted preoperative interventions to all elective patients scheduled for surgery, this study aimed to assess the prevalence and predictors of preoperative functional disability among patients scheduled for elective surgery in Northwest Ethiopia.
Methods
Study Design, Settings, Study Area and Period
A multicenter, cross-sectional study was conducted at University of Gondar Comprehensive Specialized Hospital (UOGCSH), Tibebegion Comprehensive Specialized Hospital (TGCSH) and Felegehiwot Specialized Hospital (FHSH) from April 2021 to June 2021. UOGCSH is located in Gondar town, Northwest Ethiopia. TGCSH and FHSH are located in Bahir Dar Town, Northwest Ethiopia.The study was done in surgical, orthopedic, gynecology and ophthalmology wards on patients scheduled for elective surgery.
Study Participants
This study included a total of 403 patients, with the age of ≥18 years, scheduled for elective surgery and signed informed consent for the study; where as, patients who previously participated in the study (re-operation), known psychiatric patients and unable to complete the questionnaire without assistance were our exclusion criteria.
Study Variables
The outcome variables of this study was preoperative functional disability which was measured by World Health Organization Disability Assessment Scale (WHODAS-2.0), as dichotomous variables (Yes/No). The independent variables of the study were, socio-demographic variables (age, sex, place of residency, marital status, educational level, occupation, monthly income), body mass index (BMI), behavioral characteristics (physical exercise, cigarette smoking, alcohol consumption, and chewing khat), disease conditions (diabetes mellitus, cardiovascular disease, respiratory disease, depression, and others include cerebrovascular disease, infectious diseases), number and type of current medications, preoperative pain, history of hospitalization in past one year and nutritional status.
Operational Definitions
Nutritional status was assessed by MNA-SF, which ranges from a score of 0–14 points: where 0–7= malnourished, 8–11 = at risk, 12–14= normal.21 We assessed functional disability using a 12-item WHODAS-2.0 with six domains and numerical values assigned to each item on a 5-point Likert scale: none = 0; mild = 1; moderate = 2; severe = 3; and extreme = 4. The total score, between 0 and 48, higher scores indicating higher functional disability and, then it divided by 48 and multiplied by 100 to convert it to a percentage of the maximum disability score. The severity of the preoperative disability is based on the total score of 0–4= none, 5–24= mild, 25–49= moderate, 50–95= severe, and 96–100= complete. The range from 0–100 points, where: 0= no disability and 100= complete disability. Clinically significant disability was defined as a score of ≥25%.This version was chosen because it is brief and can be administered in a short period of time, making it appropriate for use in clinical settings for assessing functional disability.22,23 We used patient health questionnaire (PHQ-9) to screen for depression which is a widely used depression screening tool by asking about depressive symptoms present in the preceding 2 weeks. The scores were expressed, Not at all = 0; several days = 1; More than half the days = 2; nearly every day = 3. A score of ≥ 10 was used for detecting depression.24–26
Study Size Determination and Sampling Techniques
The sample size was calculated using single population proportion formula. Since there was no previous study that found to estimate the prevalence of preoperative functional disability in similar population distribution so, assuming that the prevalence will be 50% with margin of error (d) 5% and confidence interval of 95%. n=  , n=
, n=  , n= 384 Where: n = number of sample size, Z = 95% confidence level= 1.96, P= 0.5 maximum population proportion and q= 1-p= 0.5 (50%), since no previous proportion assumption of 10% non response rate was added to the total sample size and determined to be 422.
, n= 384 Where: n = number of sample size, Z = 95% confidence level= 1.96, P= 0.5 maximum population proportion and q= 1-p= 0.5 (50%), since no previous proportion assumption of 10% non response rate was added to the total sample size and determined to be 422.
After proportional allocation done on these three Northwest Ethiopia Referral Hospitals, patients were selected with simple random sampling (Figure 1).
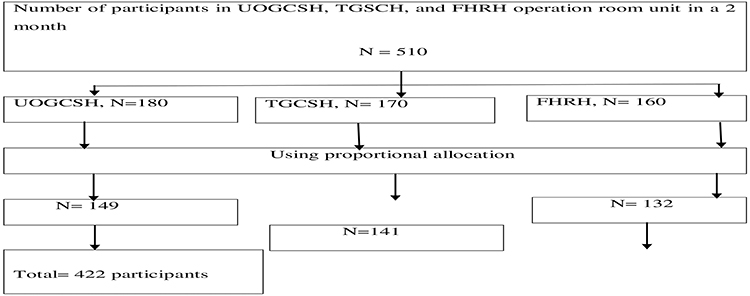 |
Figure 1 Method of the sampling procedure for prevalence and associated factors of preoperative functional disability among elective surgical patients, attending at UOGCSH, TGCSH, and FHRH from April 15 to June 15, 2021. |
Data Collection Procedure and Quality Control
Training was given for data collectors and supervisors on objectives and relevance of the study and data collection techniques. In order to assess the reliability of the tool and clarity of the variables, pretest was done on 22 (5%) of the sample size prior to the actual data collection. Considering this, data collection procedures were performed with informed consent, chart review and patient interview with semi-structured interviewer-administered questionnaire. The questionnaires were written primarily in English language and then translated into the local language using previously translated questionnaires. We preferred the interview-based method because our participants were both literate and illiterate. Finally, data were cleaned and coded carefully before the analysis.
Data Analysis and Interpretation
Data was entered into Epi Data version 4.6.0 and analysis was done by using SPSS version 26. The frequency distribution and overall prevalence were determined and recorded using the descriptive and inferential methods of data analysis. Normality of distribution was checked with the Shapiro–Wilk test. The Chi-Square test was used for categorical comparisons and assumptions. Binary logistic regression analysis was used to assess the association between explanatory variables and the outcome variables. Factors associated with preoperative functional disability were selected during the bivariate analysis with a p-value <0.2, and a crude odds ratio was done to show the strength of association. Further analysis was made by multivariable logistic regression analysis, to see the independent effects of each variable on the preoperative functional disability, and variables with p-value <0.05 at 95% CI were considered as statistically significant. The magnitude of the association was measured using the adjusted odds ratio at 95% CI. Hosmer-Lemeshow test was also used for checking the goodness of fit. Descriptive statistics were carried out and the results were presented by using texts, tables and graphs, mean and standard deviation.
Results
Socio-Demographic Characteristics of Study Participants
In total, 422 patients were eligible for participation during the study period, and the data of 403 patients were analyzed in the study with a response rate of 95.4%. The mean age of patients with a standard deviation was 43.21 ± 16.18 years, 280 (69.5%) of the subjects were in the age group of below 55 years, and the minimum and maximum ages were 18 and 90 years, respectively. Out of the total 219 (54.3%) were male, and 157 (39%) of participants were illiterate. Patient characteristics are shown in (Table 1).
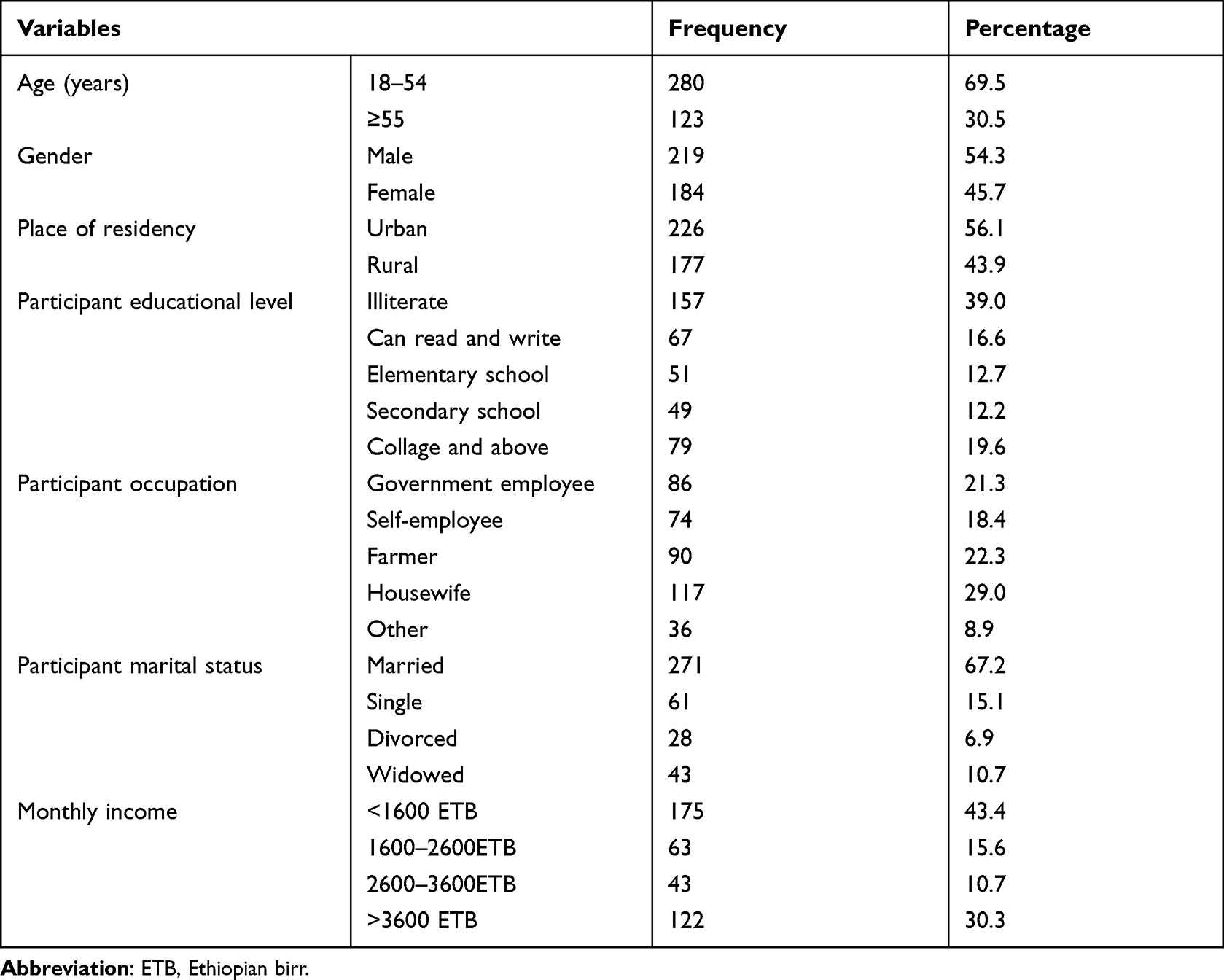 |
Table 1 The Socio-Demographic Characteristics of Patients Scheduled for Elective Surgery at UOGCSH, TGCSH, and FHRH from April 15 to June 15, 2021 (N=403). |
Preoperative and Behavioral Characteristics of the Study Participant
Regarding the previous history of hospitalization less than half of the participants 156 (38.7%), were admitted one or more times. Only 23 (5.7%) patients were ASA physical status III, scheduled to undergo different types of surgery.The BMI of the majority of the study participants were normal 290 (72%), however, 86 (21.3%) of participants had malnutrition (Table 2).
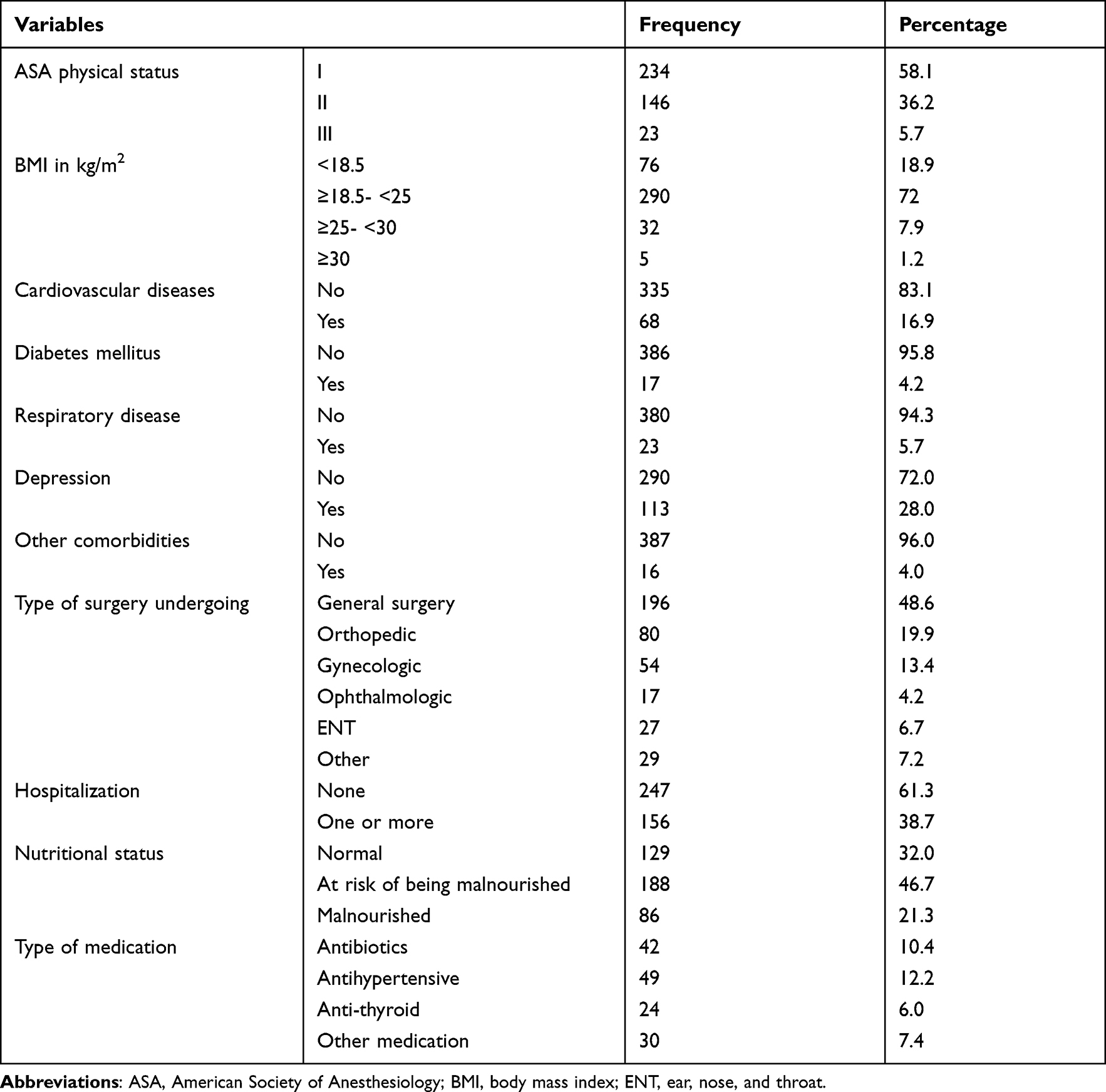 |
Table 2 Preoperative Characteristics of Patients Scheduled for Elective Surgery at UOGCSH, TGCSH, and FHRH from April 15 to June 15, 2021 (N=403). |
Participants had different types of comorbidities, out of those depression accounts for 113 (28%) (Figure 2).
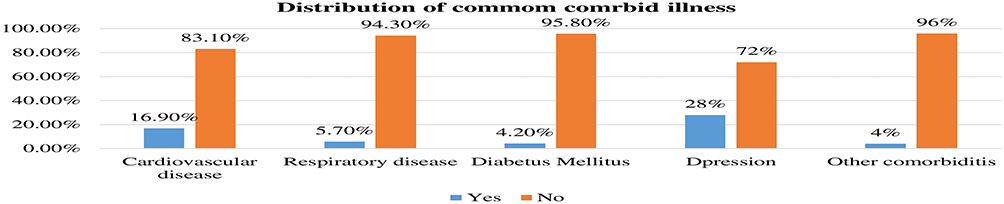 |
Figure 2 Distribution of different comorbid illnesses among elective surgical patients undergoing surgery attending UOGCSH, TGCSH, and FHRH from April 15 to June 15, 2021. (N=403). |
Prevalence of Preoperative Functional Disability
The overall prevalence of preoperative functional disability was 139 (34.5%) (95% CI: 29.8, 39), considering moderate and above disability levels. Out of all, 125 (31%) patients were without functional disability, 139 (34.5%) patients were with mild functional disability, 101 (25.1%) patients with moderate functional disability, and 38 (9.4%) patients with severe functional disability (Figure 3).
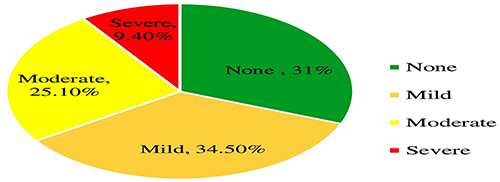 |
Figure 3 Prevalence of severity of preoperative functional disability among elective surgical patients attending UOGCSH, TGCSH, and FHRH from April 15 to June 15, 2021. (N=403). |
From the six specific domains of functional disability, the lowest percentage value was observed in the domain of (getting along) 16.9%, and the highest percentage value was observed in the domain of (participation in society) 50.4% (Figure 4).
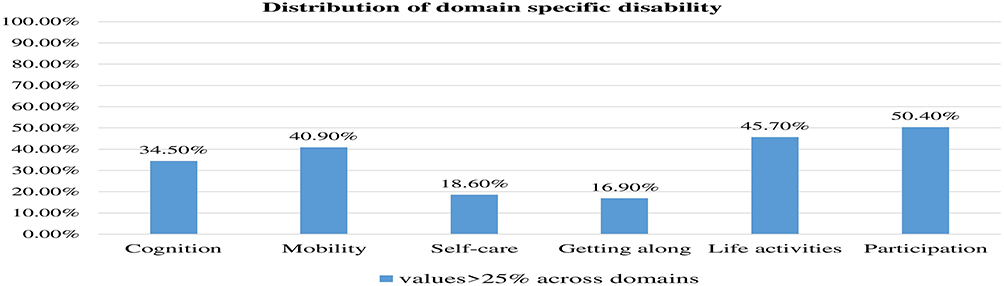 |
Figure 4 Distribution of preoperative functional disability across specific domains among patients attending UOGCSH, TGCSH, and FHRH from April 15 to June 15, 2021. (N=403). |
Factors Associated with Preoperative Functional Disability
To determine the association of independent variables with preoperative functional disability, bivariate, and multivariate binary logistic regression analysis was carried out. In bivariate analysis factors such as age, marital status, occupation, chewing chat, taking alcohol drinks, ASA physical status, number of medications, cardiovascular disease, respiratory disease, nutritional status, hospitalizations, preoperative pain, and depression were significantly associated with preoperative functional disability at a P-value <0.2.
According to multivariate analysis, age (adjusted odds ratio (AOR): 2.14, 95% CI: 1.07, 4.28), alcohol consumption (AOR: 2.05, 95% CI; 1.11, 3.77), nutritional status of malnutrition (AOR: 6.85, 95% CI; 3.06, 15.33), at risk of malnutrition (AOR: 2.72, 95% CI: 1.34, 5.52), hospitalization (AOR: 1.91, 95% CI; 1.06, 3.42), pain (AOR: 2.26, 95% CI; 1.28, 3.99), and depression (AOR: 7.90, 95% CI; 4.16, 15.01), were independently associated with preoperative functional disability. The Hosmer–Lemeshow test results were, reflecting that the model is correctly specified, and the percentage of correct classifications was 82.1% (Table 3).
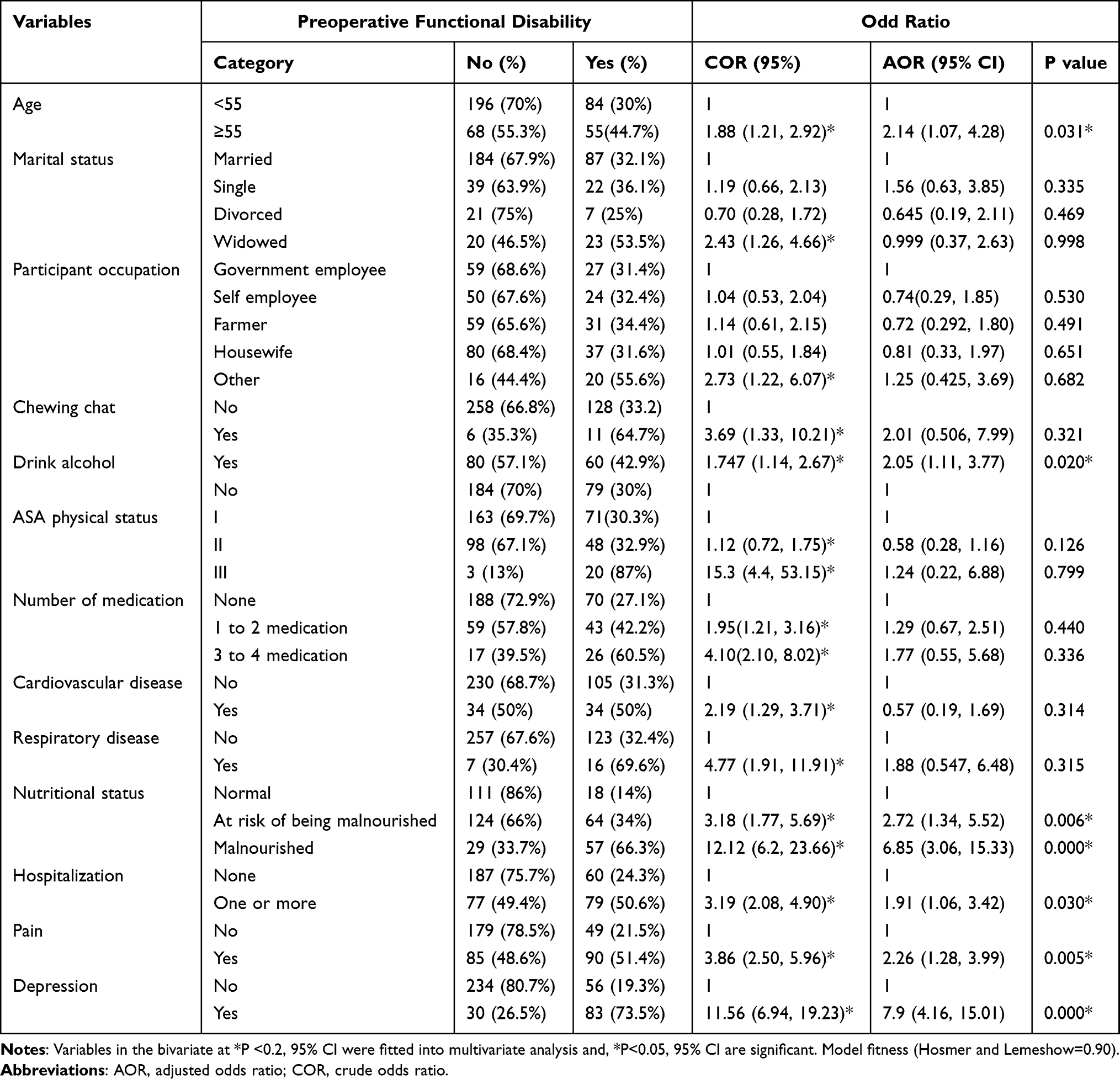 |
Table 3 Analysis of Factors Associated with Preoperative Functional Disability Among Patients Scheduled for Elective Surgery at UOGCSH, TGCSH and, FHRH Northwest, Ethiopia, 2021 (N=403). |
Discussion
This study provided general information about functional disability with WHODAS-2.0 on elective surgical patients at surgical, orthopedic, gynecology, and ophthalmology wards during the preoperative period. This study revealed that 34.5% of patients who scheduled for elective surgery had a preoperative functional disability. This may be because of surgical patients may seek surgical interventions that is caused by varied reasons with the association of multiple comorbidities that may cause disability.
This finding was higher than that of the study conducted in Japan, 29.2%.7 Other multicenter study conducted in Australia, 27%,3 and in Madagascar 17%.27 This might be due to sample size and population differences, due to the inclusion of various types of patients who were scheduled for surgery by different causes. Both of the studies, done in Japan was included ≥55-years participants only, and in the case of Madagascar, it was a comparative study of pre and postoperative patients with selected cases.
On the other hand, although the study was not comparable in population, our finding was in agreement with the study done in the community-based level in India 37.4% (95% CI: 34.2, 40.7), and on the contrary, our result was less than the study done in Germany 45.4%28 and in Spain 49.8%.29 The assessment tool type, population differences, and cut-off points used to measure the functional disability made it difficult to compare the prevalence rates. In this study, the population was surgical patients age 18–90 years and the sample size was 403, but both were population-based studies including aged participants only.
Our data also demonstrated that from WHODAS-2.0 six domains, the highest percentage value was observed in participation in society domain (50.4), and the lowest percentage value was observed in getting along with people domain (16.9%). This finding could be because of surgical patients are more prone to physical limitations and restrictions in societal activities due to either the disease-causing frustration of stigma or other comorbidities than getting along with people.
On the independent predictors of functional disability increased age, alcohol consumption, nutritional deficiency, history of hospitalization in the last one year, untreated pain, and depression were more significantly associated with preoperative functional disability.
In our study among factors of preoperative functional disability, age was independently associated with a greater likelihood of disability among those who were aged participants as compared with those respondents who were young age, which was consistent and has been described many times in different international studies. This may be because that aging is associated with increased vulnerability to chronic health problems, decreases in physiological activity, and other health problems progressively and irreversibly.30 In addition, aging has a relation to many anatomical and functional changes such as decreasing muscle strength, decreased radius of activity, and reduced cardiopulmonary fitness that can contribute to disability.31
Participants had a greater likelihood of disability among those who consume alcohol as compared with those participants who did not consume alcohol. Our findings corresponds to existing literature that says alcohol consumption is at an increased risk of functional disability.32,33 Although some studies said in some situations and quantities alcohol consumption offered protective effects for the presence of disabilities to perform a basic daily activity, due to allowing greater participation in social activities and better functional conditions.34
In this study, the cause might be related to the fact that alcohol consumption is harmful to people’s health by disrupting behavior, residential instability, and medication noncompliance that can decrease functional status.35 In addition, alcohol consumption has a direct impact on the increased risk of cardiovascular events, hepatotoxicity, and can interact with a depressed mood that leading to disability.32,33 Chronic alcoholics have more airway colonization with pathologic bacteria, increasing the risk for pneumonia, and also at risk of liver and other organ damage because of impaired cellular mechanisms and a decrease in antioxidants that contribute to functional disability.36
Long-term khat chewing was highly associated with cardiovascular (increased pulse rate, increased arterial pressure, and increased risk for acute myocardial infarction), respiratory, gastrointestinal, metabolic, endocrine, and nervous system dysfunction,37–39 however in our study it only fitted with bivariate analysis other than multi-variate analysis.
Malnutrition is a common finding in surgical patients on admission to the hospital, and it is associated with greater postoperative morbidity, prolonged length of stay, and higher cost of treatment.40 In our study, the prevalence of malnutrition was 21.3% (95% CI: 17.4, 25.3), and 46.7% (95% CI: 41.4, 51.6) of patients were at risk of malnutrition, which is in agreement with the results reported in a study in Latin America ranged from 2.6% to 73.2%.41
In this study finding, the odds of developing functional disability were 6.85 times higher among respondents who had malnutrition and 2.72 times higher among participants who were at risk of malnutrition, as compared with those respondents who were well-nourished. This might be because of the decreased muscle mass and muscle strength resulting from preoperative anorexia, as well as digestion and absorption disorders.42 Malnutrition also one of the main comorbidities of surgical patients specifically were, observed in patients who underwent gastrointestinal surgery on admission that can cause functional limitation.43 Deficiency of nutrients is a risk factor for numerous complications and adverse long-term sequelae including cerebral palsy and cognitive, visual, and hearing impairments.44 In addition, malnutrition can cause or contribute to an individual’s physical, sensory, intellectual, or mental health disability.45
In this study, there was a significant association between preoperative functional disability and history of hospitalization. This is supported by a study done by Junior et al.34 This is due to the fact that hospitalization depends on the number and type of morbidity occurrence and severity of morbidities that lead to the great need for hospital care, which in turn lead to functional incapacity.46 In addition history of hospitalization represents the presence of some clinical condition, as well as behavioral and nutritional status related conditions.34
According to this study, the odds of developing disability were 2.2 times higher among respondents who had preoperative pain as compared with those respondents who were not had pain. This is similar to the results of other studies that demonstrated significant associations among pain and functional disability. The possible reason for this relationship could be that pain can interfere with daily life activities.47 In addition, pain is related to adverse health outcomes such as physiological disturbance, psychological deficits, physical inactivity, falls, depression, and dementia.48
The presence of comorbid illness was significantly associated with functional disability as compared with those individuals who had not comorbidity which was supported by the other studies done internationally. In our finding, the prevalence of depression was (28%), which was less with other studies that have shown depression rates of 51% in Ecuador,47 38% in Ethiopia,49 and 34.9% in Iran.50 Differences in the prevalence rates occur because of the different tool cut point scales and the population difference of participants.
Our cross-sectional analysis highlighted that individuals specifically with symptoms of depression were 7.9 times more likely to be functionally disabled than individuals without symptoms of depression. This result may be because of heterogeneity of the development of depression that results in the association between cognitive impairment and decline in physical function. Even though the mechanism cycle remains unknown for this, some behavioral and biological conditions can negatively influence functional ability.51
Even in one study, it was found that patients with depression despite being in clinical remission, had scores of quality of life and disability similar to patients with high disease activity. This association could be because depression affects the threshold and the way of coping that also a determinant of disability.47 In addition, depressive symptoms may harm the quality of life and social relations.52
Although, this study was multi-center study, first for its type in Ethiopia and used an easy and internationally validated assessment tools like WHODAS 2.0, MNA-SF as well as PHQ-9; it’s limitations were the inability to show cause and effect relations, since the study design was cross-sectional. Plus variation of patient’s psychology with different disease and surgical entity will affect the results of this study.
Conclusion
The prevalence of preoperative functional disability was high. Alcohol consumption, nutritional deficiency, pain and depression were among the modifiable risk factors. So, added vigilance is needed in patients with these modifiable risk factors before surgery. Functional disability-focused preoperative screening of patients scheduled for elective surgery should be regularly performed. Emphasize individuals who use alcohol, having untreated pain, were malnourished, and have depressive symptoms for timely linkage to better rehabilitation and other optimization services. Promote health education about preoperative rehabilitative strategies such as physiotherapy and occupational therapy to engage patients in activities, prepare for an upcoming surgery, and to reduce potential complications as well as future impairments. Education on improving physical health variables like nutritional status by a healthy diet and controlling mechanism of coexisting diseases to inhibit the development and progression of poor functional status as well as to reduce surgical and anesthetic complications.
Abbreviations
ASA, American Society of Anesthesiologists; AOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; COR, crude odd ratio; FHRH, Felege Hiwot Referral Hospital; MNA-SF, mini nutritional assessment-short form; PHQ, patient health questionnaire; SPSS, Statistical Package of Social Science; STROBE, strengthening the reporting of observational studies in epidemiology; TGCSH, Tibebe Ghion Comprehensive Specialized Hospital; UOGCSH, University of Gondar Comprehensive Specialized Hospital; WHO, World Health Organization; WHODAS-2.0, World Health Organization Disability Assessment Schedule-2.0.
Data Sharing Statement
Data and materials used in this study are available and can be presented by the corresponding author upon reasonable requests.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Ethical Review Board of University of Gondar with Ref.No 189/ 04/2021. The study was done based on the Helsinki declaration. Written informed consent was obtained from each study participant’s. The study participants were informed on their full right to refuse, withdraw or completely reject their participation in the study.
Acknowledgment
We would like to acknowledge data collectors and University of Gondar for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas: took part in drafting, revising or critically reviewing the article: gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
College of Medicine and Health Sciences, University of Gondar.
Disclosure
The authors declare that they have no competing interests.
References
1. Carli F, Feldman LS. From preoperative risk assessment and prediction to risk attenuation. Br J Anaesth. 2018;122(1):11–13. doi:10.1016/j.bja.2018.10.021
2. World Health Organization. International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization; 2001.
3. Shulman MA, Myles PS, Chan MT, McIlroy DR, Wallace S, Ponsford J. Measurement of disability-free survival after surgery. Anesthesiology. 2015;122(3):524–536. doi:10.1097/ALN.0000000000000586
4. World Health Organization. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY. World Health Organization; 2007.
5. World Health Organization. International Classification of Impairments, Disabilities, and Handicaps: A Manual of Classification Relating to the Consequences of Disease, Published in Accordance with Resolution WHA29. 35 of the Twenty-Ninth World Health Assembly, May 1976. World Health Organization; 1980.
6. Din PCB. International classification of functioning, disability and health. 2001.
7. Ida M, Naito Y, Matsunari Y, Tanaka Y, Inoue S, Kawaguchi M. Prevalence and associated factors of preoperative functional disability in elective surgical patients over 55 years old: a prospective cohort study. J Anesth. 2018;32(3):381–386. doi:10.1007/s00540-018-2490-z
8. Malani PN. Functional status assessment in the preoperative evaluation of older adults. JAMA. 2009;302(14):1582–1583. doi:10.1001/jama.2009.1453
9. Millán-Calenti JC, Tubío J, Pita-Fernández S, et al. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch Gerontol Geriatr. 2010;50(3):306–310. doi:10.1016/j.archger.2009.04.017
10. Ahmad NA, Mohamad Kasim N, Mahmud NA, et al. Prevalence and determinants of disability among adults in Malaysia: results from the National Health and Morbidity Survey (NHMS) 2015. BMC Public Health. 2017;17(1):756. doi:10.1186/s12889-017-4793-7
11. Nunes JD, Saes MO, Nunes BP, et al. Functional disability indicators and associated factors in the elderly: a population-based study in Bagé, Rio Grande do Sul, Brazil. Epidemiologia e Serviços de Saúde. 2017;26:295–304. doi:10.5123/S1679-49742017000200007
12. Prynn JE, Kuper H. Perspectives on disability and non-communicable diseases in low- and middle-income countries, with a focus on stroke and dementia. Int J Environ Res Public Health. 2019;16(18):3488. doi:10.3390/ijerph16183488
13. Turner JA, Franklin G, Fulton-Kehoe D, et al. Prediction of chronic disability in work-related musculoskeletal disorders: a prospective, population-based study. BMC Musculoskelet Disord. 2004;5(1):14. doi:10.1186/1471-2474-5-14
14. Bell JA, Sabia S, Singh-Manoux A, Hamer M, Kivimäki M. Healthy obesity and risk of accelerated functional decline and disability. Int J Obes. 2017;41(6):866–872. doi:10.1038/ijo.2017.51
15. Minhas SV, Mazmudar AS, Patel AA. Pre-operative functional status as a predictor of morbidity and mortality after elective cervical spine surgery. Bone Joint J. 2017;99-B(6):824–828. doi:10.1302/0301-620X.99B6.BJJ-2016-1149.R1
16. Schmidt M, Eckardt R, Altmeppen S, Wernecke KD, Spies C. Functional impairment prior to major non-cardiac surgery is associated with mortality within one year in elderly patients with gastrointestinal, gynaecological and urogenital cancer: a prospective observational cohort study. J Geriatr Oncol. 2018;9(1):53–59. doi:10.1016/j.jgo.2017.07.011
17. MacPhedran AK, Marbey ML, Fogarty K, Vangsnes E, Vangsnes E. Is preoperative functional status associated with postoperative mortality and morbidity in elective open heart patients? Health. 2018;10:654–666. doi:10.4236/health.2018.105051
18. Kwon S, Symons R, Yukawa M, Dasher N, Legner V, Flum DR. Evaluating the association of preoperative functional status and postoperative functional decline in older patients undergoing major surgery. Am Surg. 2012;78(12):1336–1344. doi:10.1177/000313481207801225
19. Carli F, Feldman LS. From preoperative risk assessment and prediction to risk attenuation: a case for prehabilitation. Br J Anaesth. 2019;122(1):11–13.
20. Aguiar BM, Silva PO, Vieira MA, Costa FM, Carneiro JA. Evaluation of functional disability and associated factors in the elderly. Revista Brasileira de Geriatria e Gerontologia. 2019;22. doi:10.1590/1981-22562019022.180163
21. Cohendy R, Rubenstein L, Eledjam J. The mini nutritional assessment-short form for preoperative nutritional evaluation of elderly patients. Aging. 2001;13:293–297. doi:10.1007/BF03353425
22. Denu ZA, Yassin MO, Bisetegn TA, Biks GA, Gelaye KA. The 12 items Amharic version WHODAS-2 showed cultural adaptation and used to measure disability among road traffic trauma victims in Ethiopia. BMC Psychol. 2021;9(1):1. doi:10.1186/s40359-020-00492-4
23. Hu L, Zang YL, Li N. The applicability of WHODAS 2.0 in adolescents in China. J Clin Nurs. 2012;21(17–18):2438–2451. doi:10.1111/j.1365-2702.2012.04126.x
24. Cameron IM, Crawford JR, Lawton K, Reid IC. Psychometric comparison of PHQ-9 and HADS for measuring depression severity in primary care. Br J Gen Pract. 2008;58(546):32–36. doi:10.3399/bjgp08X263794
25. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
26. Gelaye B, Williams MA, Lemma S, et al. Validity of the Patient Health Questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210(2):653–661. doi:10.1016/j.psychres.2013.07.015
27. White MC, Randall K, Alcorn D, Greenland R, Glasgo C, Shrime MG. Measurement of patient reported disability using WHODAS 2.0 before and after surgical intervention in Madagascar. BMC Health Serv Res. 2018;18(1):305. doi:10.1186/s12913-018-3112-z
28. Strobl R, Müller M, Emeny R, Peters A, Grill E. Distribution and determinants of functioning and disability in aged adults - results from the German KORA-age study. BMC Public Health. 2013;13(1):137. doi:10.1186/1471-2458-13-137
29. Almazán-Isla J, Comín-Comín M, Damián J, et al. Analysis of disability using WHODAS 2.0 among the middle-aged and elderly in Cinco Villas, Spain. Disabil Health J. 2014;7(1):78–87. doi:10.1016/j.dhjo.2013.08.004
30. Landi F, Liperoti R, Russo A, et al. Disability, more than multimorbidity, was predictive of mortality among older persons aged 80 years and older. J Clin Epidemiol. 2010;63(7):752–759. doi:10.1016/j.jclinepi.2009.09.007
31. Intriago M, Maldonado G, Guerrero R, Moreno M, Moreno L, Rios C. Functional disability and its determinants in Ecuadorian patients with rheumatoid arthritis. Open Access Rheumatol. 2020;12:97–104. doi:10.2147/OARRR.S251725
32. Liu H, Jiao J, Zhu C, et al. Potential associated factors of functional disability in Chinese older inpatients: a multicenter cross-sectional study. BMC Geriatr. 2020;20(1):319. doi:10.1186/s12877-020-01738-x
33. Zgheib E, Ramia E, Hallit S, Boulos C, Salameh P. Factors associated with functional disability among Lebanese elderly living in rural areas: role of polypharmacy, alcohol consumption, and nutrition-based on the Aging and Malnutrition in Elderly Lebanese (AMEL) study. J Epidemiol Glob Health. 2018;8(1–2):82–90. doi:10.2991/j.jegh.2018.08.002
34. Júnior JSV, Martins C, Roza LB, Paulo TRS, Ribeiro CL, Tribess S. Prevalence of disability and associated factors in the elderly. Texto Contexto Enfermagem. 2015;24:521–529. doi:10.1590/0104-07072015001652014
35. Beyene GM, Legas G, Azale T, Abera M, Asnakew S. The magnitude of disability in patients with schizophrenia in North West Ethiopia: a multicenter hospital-based cross-sectional study. Heliyon. 2021;7(5):e07053. doi:10.1016/j.heliyon.2021.e07053
36. Moran S, Isa J, Steinemann S. Perioperative management in the patient with substance abuse. Surg Clin North Am. 2015;95(2):417–428. doi:10.1016/j.suc.2014.11.001
37. el-Shoura SM, Abdel Aziz M, Ali ME, et al. Deleterious effects of khat addiction on semen parameters and sperm ultrastructure. Human Reprod. 1995;10(9):2295–2300. doi:10.1093/oxfordjournals.humrep.a136288
38. Widler P, Mathys K, Brenneisen R, Kalix P, Fisch HU. Pharmacodynamics and pharmacokinetics of khat: a controlled study. Clin Pharmacol Ther. 1994;55(5):556–562. doi:10.1038/clpt.1994.69
39. Al-Motarreb A, Baker K, Broadley KJ. Khat: pharmacological and medical aspects and its social use in Yemen. Phytother Res. 2002;16(5):403–413. doi:10.1002/ptr.1106
40. Kahokehr AA, Sammour T, Wang K, Sahakian V, Plank LD, Hill AG. Prevalence of malnutrition on admission to hospital – acute and elective general surgical patients. Eur e-J Clin Nutr Metabol. 2010;5(1):e21–e5. doi:10.1016/j.eclnm.2009.11.001
41. Correia MI, Perman MI, Waitzberg DL. Hospital malnutrition in Latin America: a systematic review. Clin Nutr. 2017;36(4):958–967. doi:10.1016/j.clnu.2016.06.025
42. von Haehling S, Anker SD. Cachexia as a major underestimated and unmet medical need: facts and numbers. J Cachexia Sarcopenia Muscle. 2010;1(1):1–5. doi:10.1007/s13539-010-0002-6
43. Nishiyama VKG, Albertini SM, Moraes C, Godoy MF, Netinho JG. Malnutrition and clinical outcomes in surgical patients with colorectal disease. Arq Gastroenterol. 2018;55(4):397–402. doi:10.1590/s0004-2803.201800000-85
44. Weimann A, Braga M, Carli F, et al. ESPEN guideline: clinical nutrition in surgery. Clin Nutr. 2017;36(3):623–650. doi:10.1016/j.clnu.2017.02.013
45. Groce N, Challenger E, Berman-Bieler R, et al. Malnutrition and disability: unexplored opportunities for collaboration. Paediatr Int Child Health. 2014;34(4):308–314. doi:10.1179/2046905514Y.0000000156
46. Nascimento Cde M, Ribeiro AQ, Cotta RM, et al. Factors associated with functional ability in Brazilian elderly. Arch Gerontol Geriatr. 2012;54(2):e89–94. doi:10.1016/j.archger.2011.08.005
47. Intriago M, Maldonado G, Guerrero R, Moreno M, Moreno L, Rios C. Functional Disability and Its Determinants in Ecuadorian Patients with Rheumatoid Arthritis. Dove Press; 2020.
48. Makino K, Lee S, Bae S, et al. Pain characteristics and incidence of functional disability among community-dwelling older adults. PLoS One. 2019;14(4):e0215467. doi:10.1371/journal.pone.0215467
49. Duko B, Erdado M, Ebrahim J. Prevalence and factors associated with depression among hospital admitted patients in South Ethiopia: cross sectional study. BMC Res Notes. 2019;12(1):73. doi:10.1186/s13104-019-4109-3
50. Shoar S, Naderan M, Aghajani M, Sahimi-Izadian E, Hosseini-Araghi N, Khorgami Z. Prevalence and determinants of depression and anxiety symptoms in surgical patients. Oman Med J. 2016;31:176–181. doi:10.5001/omj.2016.35
51. Tavares D, Pelizaro P, Sousa Pegorari M, Paiva M, Marchiori G. Functional disability and associated factors in urban elderly: a population-based study. Revista Brasileira de Cineantropometria e Desempenho Humano. 2016;18:499–508. doi:10.5007/1980-0037.2016v18n5p499
52. Elmer T, Stadtfeld C. Depressive symptoms are associated with social isolation in face-to-face interaction networks. Sci Rep. 2020;10(1):1444. doi:10.1038/s41598-020-58297-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.