Back to Journals » Risk Management and Healthcare Policy » Volume 16
Prevalence and Influencing Factors of Physical Restraints in Intensive Care Units: A Retrospective Cohort Study
Authors Cui N ![]() , Zhang H, Gan S, Zhang Y, Chen D, Guo P, Wu J, Li Z, Jin J
, Zhang H, Gan S, Zhang Y, Chen D, Guo P, Wu J, Li Z, Jin J
Received 2 March 2023
Accepted for publication 13 May 2023
Published 19 May 2023 Volume 2023:16 Pages 945—956
DOI https://doi.org/10.2147/RMHP.S408919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Nianqi Cui,1,2,* Hui Zhang,3,* Sijie Gan,4 Yuping Zhang,1 Dandan Chen,5 Pingping Guo,5 Jingjie Wu,5 Zhuang Li,6 Jingfen Jin1,7,8
1Nursing Department, The Second Affiliated Hospital of Zhejiang University School of Medicine (SAHZU), Hangzhou, Zhejiang, People’s Republic of China; 2School of Nursing, Kunming Medical University, Kunming, Yunnan, People’s Republic of China; 3Department of Cardiology, Guizhou Provincial People’s Hospital, Guiyang, Guizhou, People’s Republic of China; 4Product Development Center, Zhejiang Xinhua Mobile Media Co. Ltd, Hangzhou, Zhejiang, People’s Republic of China; 5Faculty of Nursing, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 6Medical Faculty, Yunnan College of Business Management, Kunming, Yunnan, People’s Republic of China; 7Key Laboratory of The Diagnosis and Treatment of Severe Trauma and Burn of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China; 8Dean’s Office, Changxing Branch Hospital of SAHZU, Huzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhuang Li, Medical Faculty, Yunnan College of Business Management, No. 296 Haitun Road, Wuhua District, Kunming, Yunnan, 650106, People’s Republic of China, Tel + 86 15198859387, Fax +86 0871-68314770, Email [email protected] Jingfen Jin, Nursing Department, The Second Affiliated Hospital of Zhejiang University School of Medicine (SAHZU), No. 88 Jiefang road, Shangcheng District, Hangzhou, Zhejiang, 310009, People’s Republic of China, Tel + 86 137 5711 8239, Fax +86 0571-87783887, Email [email protected]
Purpose: Physical restraints are used routinely in intensive care units (ICUs) and have negative effects. It is critical to identify the impact factors of physical restraints on critically ill patients. The present study investigated the prevalence of physical restraints and impact factors associated with their use in a large cohort of critically ill patients over one year.
Patients and Methods: A retrospective cohort study was performed in multiple ICUs at a tertiary hospital in China in 2019 using observational data from electronic medical records. The data consisted of demographics and clinical variables. Logistic regression was used to assess the independent impact factors for the use of physical restraint.
Results: The analysis consisted of 3776 critically ill patients with a prevalence of physical restraint use of 48.8%. The logistic regression analysis indicated that physical restraint use was associated with independent risk factors, including surgical ICU admission, pain, tracheal tube placement, and abdominal drainage tube placement. Physical restraint use was associated with independent protective factors, including male sex, light sedation, muscle strength, and ICU length of stay.
Conclusion: The prevalence of physical restraint use in critically ill patients was high. Tracheal tubes, surgical ICU, pain, abdominal drainage tubes, light sedation, and muscle strength were independent variables associated with the use of physical restraint. These results will assist health professionals in identifying high-risk physical restraint patients based on their impact factors. Early removal of the tracheal tube and abdominal drainage tube, pain relief, light sedation, and improvements in muscle strength may help reduce the use of physical restraints.
Keywords: critical care, restraints, physical, epidemiology, nursing
Introduction
A physical restraint (PR) is defined as any action or procedure that prevents aperson’s free body movement to aposition of choice and/or normal access to his/her body by the use of any method, attached or adjacent to aperson’s body that he/she cannot control or remove easily. 1 There are wide variations in estimates of PR prevalence in intensive care units (ICUs) between countries. PR is prevalent in the United States and Canada at a rate of 16.6 to 56%.2–4 PR is widely used in Europe and ranges from 0% in the United Kingdom and Portugal to 100% in Italy according to the units surveyed.5 Data from 44 ICUs in Australia and New Zealand showed that the utilization rate of PR was 8%.6 The prevalence of PR use is 32.9% and 35.8% in ICUs in Japan and Jordan, respectively.7,8 Two cross-sectional surveys in China showed that 59.07% and 61.2% of critically ill patients were physically restrained.9,10 Because PR restricts patient’ free movement, increase pressure on the restrained limbs and restricts blood circulation, multiple clinical complications are associated with PR in ICUs, including neurovascular complications (eg, redness, limb movement, edema, and color complications),11 pressure injuries,12 unplanned extubation,13 agitation,14 delirium,15,16 posttraumatic stress disorder,17 depression, anxiety, anger, social isolation, and reduction of personal autonomy.18,19
PR may increase the risk of cardiac arrest in a certain instances (eg, if a patient used cocaine prior to being restrained).20 A retrospective analysis found that vest and strap restraints caused 122 deaths.21 Due to the negative effects of PR, multiple associations published guidelines that advocate for reduced use of PR.22–24 For example, the PR guideline published by the Registered Nurses’ Association of Ontario recommended that a nurse should perform a risk assessment of the patient upon admission and on an ongoing basis to identify any risk factors that may lead to PR.24 Therefore, identifying the impact factors for PR in critically ill patients is paramount because it allows early detection of patients who may be negatively affected by PR, and it promotes alternative approaches to PR.
Previous studies investigated the impact factors for PR use in ICUs. One prospective cohort study found that an endotracheal tube (odds ratio (OR), 7.38; 95% confidence interval (CI), 3.43–15.87), exposure to benzodiazepines (OR, 6.27; 95% CI, 3.05–12.90) or propofol (OR, 3.78; 95% CI, 1.52–9.40), delirium (OR, 2.94; 95% CI, 1.27–6.80), and enteral tube (OR, 2.53; 95% CI, 1.28–4.99) were associated with PR use in ICUs in the United States.2 PR use was associated with several independent impact factors, including delirium (OR, 11.235; 95% CI, 4.695–26.886), mechanical ventilation (OR, 6.345; 95% CI, 3.057–13.168), and age ≥ 75 years (OR, 13.355; 95% CI, 4.540–39.293), according to a cross-sectional study. The use of analgesics (OR, 0.296; 95% CI, 0.146–0.601) was an independent protective factor against PR use.10 Another prospective, cross-sectional study showed that male sex (OR, 1.832; 95% CI, 1.062–3.158), mechanical ventilation (OR, 2.158; 95% CI, 1.358–23.430), life-threatening treatment interruption (OR, 1.581; 95% CI, 1.031–2.425) and irritability (OR, 1.694; 95% CI, 1.074–2.670) were independent risk factors for PR use. However, there may be issues with these existing studies. First, healthcare professionals’ decision-making for PR has marked cultural heterogeneity.25 There may be differences in the factors that affect the decision-making for PR use by healthcare professionals in different cultural contexts, which means that different factors may influence PR use in critically ill patients. Therefore, the impact factors of PR may vary in different countries. Second, most studies on the impact factors of PR in China were cross-sectional studies and may only reflect the impact factors of PR at the investigation time point. These studies did not identify the impact factors of ICU patients during their ICU stay. Knowing the prevalence of PR use days/days in ICU is preferred over the prevalence of the number of patients with PR use/number of patients in the ICU because it provides a more accurate representation of how long patients are subjected to PR during their ICU stay. Reducing the duration of PR may have more clinical implications than shortening the frequency of PR. Practitioners who understand the factors that affect patients with a longer duration of PR can provide more targeted clinical treatment and nursing care. The sample size for existing studies was relatively small, which may explain the wide 95% CIs of the ORs.
Therefore, the present study investigated the prevalence of PR and impact factors associated with PR use in a large cohort of critically ill patient in China over one year.
Materials and Methods
Study Design
This study was an observational electronic medical record (EMR) based retrospective cohort study. The clinical research ethics committee of The Second Affiliated Hospital Zhejiang University School of Medicine independently approved the study protocol (No. 2020131). Due to the retrospective design, the ethics committee approved a waiver of informed consent. To protect the privacy of study participants, study data were kept confidential. The Declaration of Helsinki was followed in the performance of this study.
Inclusion and Exclusion Criteria
We included consecutive patients (≥18 years) who were admitted to one of the following ICUs at a tertiary hospital in Hangzhou, China from January 1, 2019 to December 31, 2019: two mixed medical-surgical ICUs (62 beds in total), the emergency ICU (16 beds), and the surgical ICU (12 beds). Patients with previous psychiatric disorders and incomplete information were excluded.
Study Definitions
PR was defined as any action or procedure that prevents a person’s free body movement to a position of choice and/or normal access to his/her body by the use of any method, attached or adjacent to a person’s body that he/she cannot control or remove easily.1 Based on this definition, PR included wrist or ankle ties, belts, hand mitts that were attached or tied to the bed or other surface, and sheet ties. Side rails were not within the definition scope of PR. Critical care nurses were the main decision-maker for PR at the study site, and the method to identify PR was based on their clinical experience. The intensivist prescribed orders to implement PR in the physician order entry system. The nurse immediately implemented PR on the patient and recorded the time in nursing record systems. When they believed that the patient no longer required PR (eg, when the patient was conscious and without endotracheal tube), they communicated with the intensivist and the intensivist prescribed orders to relieve PR. The nurse removed the PR and recorded the time in nursing record systems. The number of PR use days refers to the time between the patient’s use of PR and the release of PR in the nursing record system.
Selection of Variables
The selection of variables were derived from a literature review and our previous qualitative descriptive studies.26,27 Based on the literature, age, sex, comorbidities, mechanical ventilation (MV), irritability, exposure to benzodiazepines or propofol, delirium, life-threatening treatment interruption, endotracheal tube, enteral tube, and nurse-to-patient ratio may be impact factors associated with PR use. According to our previous qualitative descriptive studies,26,27 patients with high-risk catheters (eg, endotracheal tube), ability to self-extube (eg, normal muscle strength), no recognition of catheters (eg, delirium) and intolerance to the tracheal tube (eg, pain) were more likely to be physically restrained.
Because the main purpose of benzodiazepines or propofol is sedation and analgesia, we extracted sedation and pain scores of patients instead of exposure to benzodiazepines or propofol. Pain was assessed at the study sites using a numerical rating scale (NRS) every two hours. NRS scores equal to or less than two were considered “no pain” or “no effect of pain”, and scores greater than two are considered “with pain”. Depth of sedation was assessed every four hours using the Richmond Agitation Sedation Scale (RASS) when the patients received sedative drugs. RASS scores equal to or less than negative three were considered “deep sedation”, negative two to zero was considered “light sedation”, and greater than one was considered “agitation”. Muscle strength was evaluated every 12 years using the Medical Research Council (MRC) scale.28 MRC scores equal to or less than one were considered “no muscle strength”, and MRC scores greater than one were considered “with muscle strength”.
The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) was used to assess delirium every morning (8:00) and evening (20:00). The CAM-ICU was not used when the patient was receiving sedative drugs. In addition to routine assessment, patients were reassessed based on changes in status. Our previous qualitative descriptive studies indicated that nurses did not accurately identify or assess critically ill patients with delirium.26,27 Therefore, the data related to delirium in the EMR may be inaccurate. To test our idea and determine whether the NRS, RASS, and MRC assessments were accurate, we included 30 patients to validate the EMR variables (NRS, RASS, MRC, and CAM-ICU) with the researcher assessments. The kappa coefficients for the NRS, RASS, and MRC outcomes were 0.634, 0.874, and 0.867, respectively, and all p values were less than 0.001. However, the kappa coefficient for the CAM-ICU outcome was 0.194 (p = 0.073). Therefore, the results of delirium in the EMR database were inaccurate, and we did not extract these data.
Although the Glasgow Coma Scale (GCS) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) and nurse-to-patient ratio may impact PR use, we were unable to extract these data due to the lack of these data in the EMR. Due to the lack of definition of high-risk catheters, we extracted all data related to catheters or tubes in the EMR database. The final variables that we extracted included demographics (sex and age) and clinical variables (ward, history of hypertension, history of diabetes, history of alcohol consumption, history of smoking, pain, depth of sedation, muscle strength, ICU length of stay, duration of MV, intraventricular drainage tubes, tracheal tubes, nasogastric tubes, nasoenteric tubes, central venous catheters, peripherally inserted central catheters, peripheral venous catheters, chest drainage tubes, abdominal drainage tubes, lumbar drainage tubes, pelvic drainage tubes, hemodialysis catheters, and urethral catheters).
Data Collection and Analysis
Data were collected using a validated prospective EMR database. The prevalence of PR was calculated by dividing the number of days in which patients were physically restrained by the total length of ICU stay (days) for all patients. Patients were categorized into two groups based on the presence or absence of PR. The presence of PR indicated that the patient underwent PR at least once during the ICU stay. The absence of PR indicated that the patient did not receive PR during the ICU stay, regardless of the type. We compared the demographics and other variables between these two groups. Continuous variables are characterized by the mean (standard deviation) or median (interquartile range), and categorical variables are described as counts and percentages. The analysis of continuous variables was performed using t-tests or Mann–Whitney tests. The chi-squared test, corrected chi-squared test, and Fisher’s exact test were used to analyze categorical variables. We explored factors potentially associated with PR using multivariable logistic regression, including patient characteristics. The significant variables were entered in a stepwise manner (significance level for entering effects, 0.05; significance level for removing effects, 0.1) when the univariate analysis of the two groups was statistically significant. ORs were reported with 95% CIs in logistic regression models. Statistical analysis was performed using IBM SPSS Statistics Version 26.0 (IBM Corp., Armonk, NY, USA). STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines were followed in reporting the study.
Results
There were 5377 patients admitted to the ICUs during this 1-year study period. In our cohort, 3776 patients were included after excluding patients with incomplete or missing data (1033 patients), and patients younger than 18 years (568 patients). The total number of days when 2574 patients were physically restrained was 10,768. During the study period, 22064.77 days were spent on the ICU by all patients. Therefore, the prevalence of PR was 48.8%. The median duration of PR use was 0.68 days (IQR 0–2.51).
Among the patients with PR, the median duration of PR use was 1.43 days (IQR 0.65–4.36). There were significant differences in sex, ward, pain, sedation, muscle strength, ICU length of stay, duration of MV, tracheal tubes, nasogastric tubes, central venous catheters, abdominal drainage tubes, pelvic drainage tubes, and urethral catheters between patients without PR and patients with PR. The details of the demographics and clinical variables are presented in Table 1.
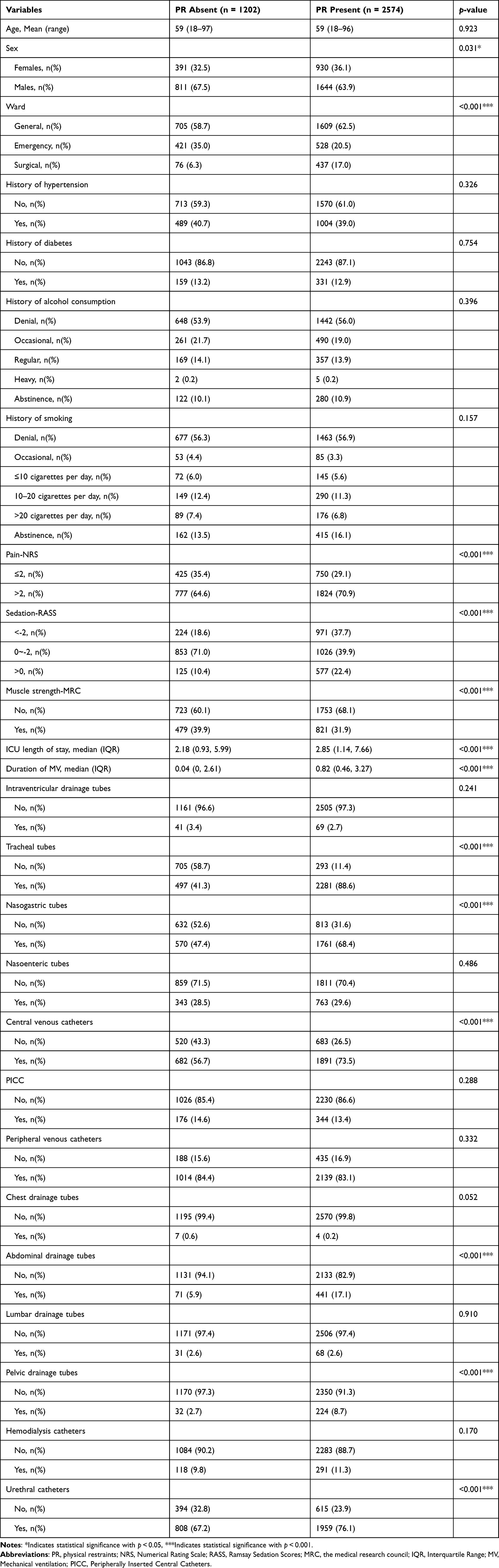 |
Table 1 Characteristics of Patients with and without Physical Restraints |
Multivariate logistic regression included these variables. Based on the results of the final stepwise logistic regression analysis, the variables associated with PR use were surgical ICU (OR, 2.082; 95% CI, 1.530–2.833), pain (OR, 1.938; 95% CI, 1.599–2.350), tracheal tubes (OR, 9.013; 95% CI, 7.417–10.953), abdominal drainage tubes (OR, 1.755; 95% CI, 1.279–2.408), male sex (OR, 0.837; 95% CI, 0.704–0.996), light sedation (OR, 0.501; 95% CI, 0.405–0.619), muscle strength (OR, 0.703; 95% CI, 0.590–0.836), and ICU length of stay (OR, 0.985; 95% CI, 0.976–0.995). The results of multivariate logistic regression are shown in Table 2 and Figure 1. A p value < 0.01 was observed in the Hosmer-Lemeshow test, which may be a result of the large sample size and made adjustment of the model more difficult. The Cox & Snell R2 was 0.257, and the Nagelkerke R2 was 0.36, which indicated that the model was well fitted.
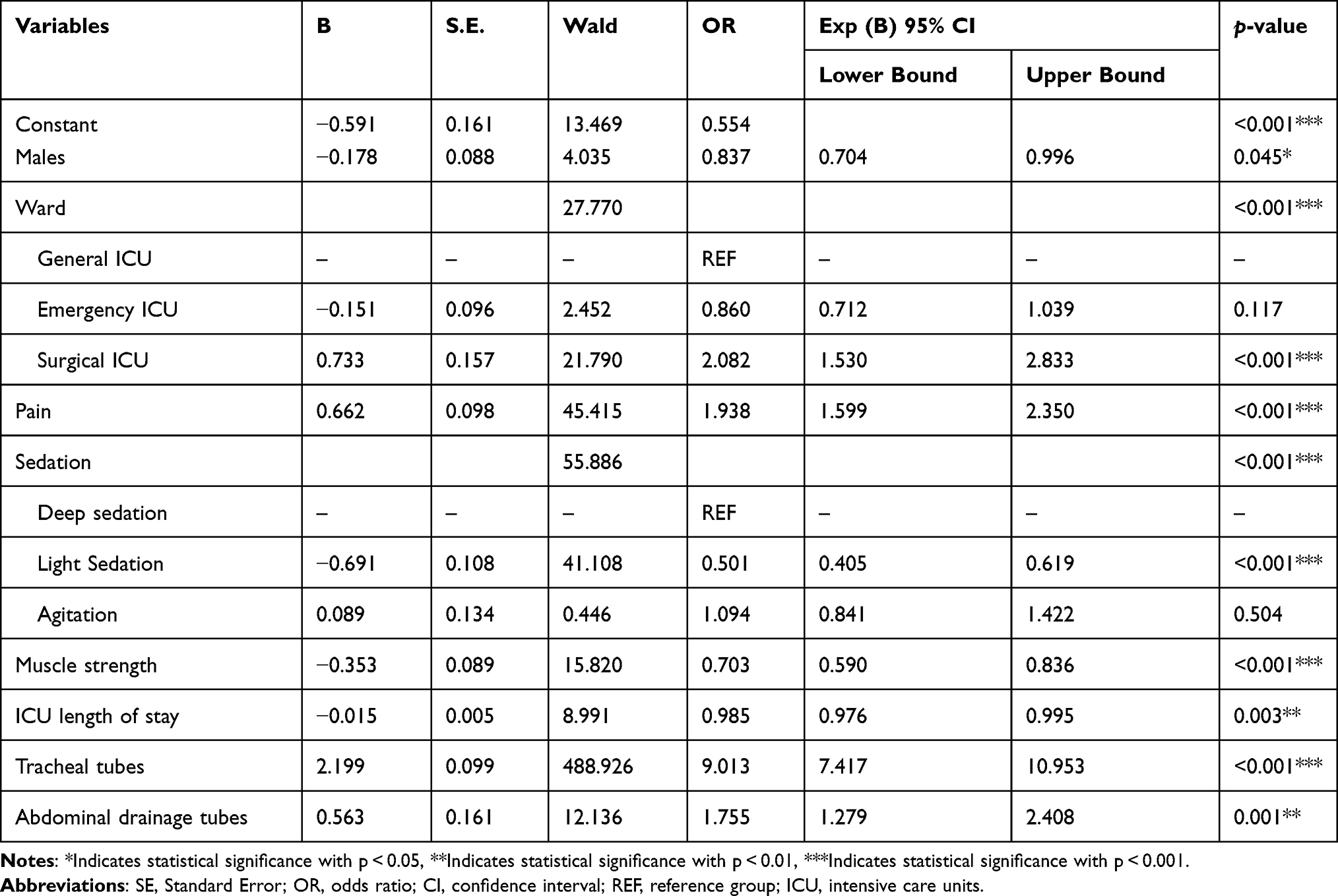 |
Table 2 Logistics Regression Model of Influencing Factors for the Use of Physical Restraints |
 |
Figure 1 Forest plot of influence factors for the use of physical restraints. |
Discussion
This large retrospective cohort study showed that the prevalence of PR was high in critically ill patients in China. The prevalence of PR was 48.8%. Among critically ill patients who underwent PR, the median duration of PR use was 1.43 days (IQR 0.65–4.36). The results of logistic regression analysis suggested that tracheal tubes, surgical ICU, pain, abdominal drainage tubes, light sedation, and muscle strength were closely related to PR use.
The reported prevalence of PR use varies in different countries. The prevalence of PR use in this study was lower than previous studies performed in China. The prevalence of PR was 53.9% in a 2007 study in Nantong, China.10 The prevalence of PR was calculated by dividing the number of shifts in which patients were restrained by the total length of ICU stay (shifts) for all patients in this study, which is different from the present study. Another study in China in 2019 demonstrated that the prevalence of PR was 59.07%. The prevalence of PR was calculated by dividing the number of patients restrained by the total number of all patients in this study, which is also different from the present study. Although there are no clear standards on the prevalence of PR, the Handbook of Nursing-Sensitive Quality Indicators published by the National Institute of Hospital Administration29 defined the calculation method of the prevalence of PR by dividing the number of days in which patients were physically restrained by the total length of ICU stay (days) for all patients, which is consistent with the calculation method of our study. In addition to the difference in the calculation method of the prevalence of PR, differences in study designs and survey locations may also be one of the reasons for the differences. A prospective observational study in Toronto, Canada found that 235 patients were admitted to the ICU, and 102 of these patients underwent PR from November 2019 to March 2020.30 PR was present in 43.4% of critically ill patients in this study, which is lower than our study. The median prevalence of PR use in a mixed-methods study performed in 17 ICUs in Spain was 19.11%.31 However, this study did not report the calculation method of the prevalence of PR. In another Japanese study, 259 of 787 critically ill patients received PR. Therefore, PR was present in 32.9% of critically ill patients in this study, which is lower than our study. In a point prevalence study in Australia and New Zealand, PR was present in only 7.6% (48/627) of critically ill patients. “The prevalence of PR” reported by these studies was the prevalence at a certain time point, rather than the prevalence of PR of the patients during ICU stay. However, this method reflects the current status of PR use in critically ill patients to some extent. According to the aforementioned related studies, it is recommended to upgrade the original institutions, update the details of the process for implementing PR, clarify the use of PR indicators, and release indicators. More effort must be made to educate nurses about the harmful effects of PR and suggest alternatives.10
Our study found that many factors influenced the use of PR, such as tracheal tubes, surgical ICU, pain, abdominal drainage tubes, light sedation, and muscle strength. The possibility of PR use was 9.013 times higher in patients with a tracheal tube than patients without a tracheal tube. Previous studies demonstrated that factors associated with PR use included endotracheal and mechanical ventilation.2,10,32 A point prevalence study performed across Europe found that PR was predominantly used to protect patients from pulling/removing the endotracheal tube and lines.5 This study did not demonstrate that intravascular lines, such as central venous and arterial access, were associated with PR use.33,34 We found that the abdominal drainage tube was also an independent risk factor for PR use (OR, 1.755; p = 0.001). Patients with pain in our study indicated that the NRS score was greater than two, which meant that pain markedly influenced sleep. Patients with pain were more likely receive PR than patients without pain. This finding somewhat corroborates Gu et al,10 who found that the use of analgesics was an independent protective factor against PR use. Compared to deep sedation, the present study found that patients with light sedation were less likely to be physically restrained, and agitation did not influence PR use. This finding contrasts to previous studies that suggested that the predominant reason for PR use was agitation and “dangerous behaviors”.34 The most likely reason that light sedation was an independent protective factor against PR use was that it was associated with a shorter time to extubation (mean difference (MD), –0.77 d; 95% CI, –2.04 to –0.50)35,36 and a reduced tracheostomy rate (RR, 0.57; 95% CI, 0.41–0.80).37,38 The present study found that muscle strength (vs muscle weakness) was an independent protective factor against PR use. According to previous studies, muscle weakness was associated with a variety of factors, including sepsis, multi-organ failure, mechanical ventilation, and pre-admission status.39,40 One plausible explanation is that patients with muscle strength are more stable. Another finding is that the possibility of PR use was 2.082 times higher in patients admitted to the surgical ICU than patients admitted to the general ICU (medical-surgical mixed ICU). Because all patients admitted to the surgical ICU were postoperative patients in our study, postoperative patients may be more likely to receive PR. Previous studies demonstrated that PR use was more common in the chest ICU than in other ICUs.41 We also found that male sex was an independent protective factor against PR use (OR, 0.837; p = 0.045). This finding contrasts previous studies that suggested that PR was more commonly used in male patients.32,42 However, the p value was borderline and close to 0.05 in the present study. Another protective factor that may be questioned is ICU length of stay because the 95% CI was very close to 1 (OR, 0.985; 95% CI, 0.976–0.995). Therefore, whether these two influencing factors truly influence PR use should be further verified.
This study is part of a guideline adaptation project.43 According to the guideline adaptation methodology CAN-Implement,44 the guideline adaptation group must outline the practice problem and define the scope of the topic and specific health questions at the beginning of the project. The present study clarified the prevalence and influencing factors of PR in critically ill patients. Combined with previous qualitative descriptive studies by our research team,26,27 PR and unplanned extubation, mechanical ventilation, pain, agitation/sedation, and family involvement were linked inextricably. These results provide important guidance for subsequent studies, including the discovery of relevant guidelines and systematic reviews, appraising evidence, and formulation of the direction and strength of recommendations for adapted guidelines.45–48 The findings of the present study should arouse the attention of nursing managers because PR is frequently implemented in critically ill patients and prompt intervention may be necessary. Clinical practitioners can identify high-risk patients with PR by assessing risk factors for PR use, and closer monitoring in the high-risk population is possible. Healthcare professionals can tailor their care plans to the unique needs of each patient. This personalized approach has the potential to improve overall patient outcomes.
Limitations
First, we could not collect clinical variables that may be associated with PR use in critically ill patients, such as the admission diagnosis, non-invasive ventilation, GCS score, APACHE II score and nurse-to-patient ratio, because of limitations in the EMR database. We also did not include delirium data for analysis due to inaccurate delirium assessment. Second, because our study was performed at a single center, the results may not be applicable to other clinical settings. However, we emphasize that this study was a cohort study performed over a one-year period in multiple ICUs in a tertiary hospital with a large number of cases. These findings could not be generalized to pediatric ICUs because we excluded these patients.
Conclusion
Our study revealed a high prevalence of PR use (48.8%) in this cohort of critically ill patients. This study also demonstrated that tracheal tubes, surgical ICU, pain, and abdominal drainage tubes were identified as independent risk factors for PR use, whereas light sedation and muscle strength were independent protective factors for PR use. These findings help health professionals identify high-risk patients with PR by assessing risk factors. Early removal of the tracheal tube and abdominal drainage tube, relief of pain, light sedation, and improvement of muscle strength may contribute to reducing PR use. Health professionals should regularly assess risk factors and develop targeted interventions based on these risk factors to minimize the duration of PR use. Policy-makers should provide education and training to all healthcare professionals on early extubation, sedation, pain, mobilization, and other PR management in critically ill patients.
Acknowledgments
Grateful acknowledgement is given to anonymous reviewers for their indispensable assistance.
Funding
This work was supported by The Science Research Foundation of Chinese Nursing Association [Grant No: ZHKY201913], Zhejiang University Academic Award for Outstanding Doctoral Candidates [grant numbers: 202059], Guizhou Provincial People’s Hospital Yuan Ren Cai Xiang Mu [2022]-18, and the Science Technology Platform and Talent Team Plan Projects in Guizhou Province [Grant 2017(5405)].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bleijlevens MH, Wagner LM, Capezuti E, Hamers JP. Physical restraints: consensus of a research definition using a modified delphi technique. J Am Geriatr Soc. 2016;64(11):2307–2310. doi:10.1111/jgs.14435
2. Lawson TN, Tan A, Thrane SE, et al. Predictors of new-onset physical restraint use in critically ill adults. Am J Crit Care. 2020;29(2):92–102. doi:10.4037/ajcc2020361
3. Boley SP, Stellpflug SJ. A comparison of resource utilization in the management of anticholinergic delirium between physostigmine and nonantidote therapy. Ann Pharmacother. 2019;53(10):1026–1032. doi:10.1177/1060028019846654
4. Nason R, Anderst P. Fit to be tied: restraint usage in adult intensive care unit (ICU). Can J Crit Care Nurs. 2018;29:58–59.
5. Benbenbishty J, Adam S, Endacott R. Physical restraint use in intensive care units across Europe: the PRICE study. Intensive Crit Care Nurs. 2010;26(5):241–245. doi:10.1016/j.iccn.2010.08.003
6. Maiden MJ, Bone A, Fitzpatrick M. Physical restraint of patients in Australia and New Zealand intensive care units. Intensive Care Med. 2021;47(2):234–236. doi:10.1007/s00134-020-06287-w
7. Kawai Y, Hamamoto M, Miura A, et al. Prevalence of and factors associated with physical restraint use in the intensive care unit: a multicenter prospective observational study in Japan. Intern Emerg Med. 2021;17(1):37–42. doi:10.1007/s11739-021-02737-5
8. Suliman M. Prevalence of physical restraint among ventilated intensive care unit patients. J Clin Nurs. 2018;27(19–20):3490–3496. doi:10.1111/jocn.14588
9. Zhang C, Liu D, He Q. The characteristics of ICU physical restraint use and related influencing factors in China: a multi-center study. Ann Palliat Med. 2021;10(2):1198–1206. doi:10.21037/apm-20-563
10. Gu T, Wang X, Deng N, Weng W. Investigating influencing factors of physical restraint use in China intensive care units: a prospective, cross-sectional, observational study. Aust Crit Care. 2019;32(3):193–198. doi:10.1016/j.aucc.2018.05.002
11. Ertuğrul B, Özden D. The effect of physical restraint on neurovascular complications in intensive care units. Aust Crit Care. 2020;33(1):30–38. doi:10.1016/j.aucc.2019.03.002
12. Liu Y, Wu X, Ma Y, et al. The prevalence, incidence, and associated factors of pressure injuries among immobile inpatients: a multicentre, cross-sectional, exploratory descriptive study in China. Int Wound J. 2019;16(2):459–466. doi:10.1111/iwj.13054
13. Ai ZP, Gao XL, Zhao XL. Factors associated with unplanned extubation in the Intensive Care Unit for adult patients: a systematic review and meta-analysis. Intensive Crit Care Nurs. 2018;47:62–68. doi:10.1016/j.iccn.2018.03.008
14. Mion LC. Physical restraint in critical care settings: will they go away? Geriatr Nurs. 2008;29(6):421–423. doi:10.1016/j.gerinurse.2008.09.006
15. Mehta S, Cook D, Devlin JW, et al. Prevalence, risk factors, and outcomes of delirium in mechanically ventilated adults. Crit Care Med. 2015;43(3):557. doi:10.1097/CCM.0000000000000727
16. Pan Y, Jiang Z, Yuan C, et al. Influence of physical restraint on delirium of adult patients in ICU: a nested case-control study. J Clin Nurs. 2018;27(9–10):1950–1957. doi:10.1111/jocn.14334
17. Jones C, Bäckman C, Capuzzo M, et al. Precipitants of post-traumatic stress disorder following intensive care: a hypothesis generating study of diversity in care. Intensive Care Med. 2007;33(6):978–985. doi:10.1007/s00134-007-0600-8
18. Perez D, Peters K, Wilkes L, Murphy G. Physical restraints in intensive care: experiences of patients, families and nurses. Aust Nurs Midwifery J. 2017;24(10):45.
19. Jacob JD, Holmes D, Rioux D, Corneau P, MacPhee C. Convergence and divergence: an analysis of mechanical restraints. Nurs Ethics. 2019;26(4):1009–1026. doi:10.1177/0969733017736923
20. Tolson D, Morley JE. Physical restraints: abusive and harmful. J Am Med Dir Assoc. 2012;13(4):311–313. doi:10.1016/j.jamda.2012.02.004
21. Miles SH, Irvine P. Deaths caused by physical restraints. Gerontologist. 1992;32(6):762–766. doi:10.1093/geront/32.6.762
22. Bray K, Hill K, Robson W, et al. British Association of Critical Care Nurses position statement on the use of restraint in adult critical care units. Nurs Crit Care. 2004;9(5):199–212. doi:10.1111/j.1362-1017.2004.00074.x
23. Maccioli GA, Dorman T, Brown BR, et al. Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit: use of restraining therapies--American College of Critical Care Medicine Task Force 2001–2002. Crit Care Med. 2003;31(11):2665–2676. doi:10.1097/01.CCM.0000095463.72353.AD
24. Registered nurses’ association of Ontario. promoting safety: alternative approaches to the use of restraints; 2012. Available from: http://rnao.ca/bpg/guidelines/promoting-safety-alternative-approaches-use-restraints.
25. Goethals S, Dierckx DCB, Gastmans C. Nurses’ decision-making in cases of physical restraint: a synthesis of qualitative evidence. J Adv Nurs. 2012;68(6):1198–1210. doi:10.1111/j.1365-2648.2011.05909.x
26. Cui N, Qiu R, Zhang Y, et al. Why are physical restraints still in use? A qualitative descriptive study from Chinese critical care clinicians’ perspectives. BMJ Open. 2021;11(11):e055073. doi:10.1136/bmjopen-2021-055073
27. Cui N, Qiu R, Zhang Y, Jin J. “patient comfort can be sacrificed for patient safety”-perception and practice reported by critical care nurses toward physical restraints: a qualitative descriptive study. Front Med. 2021;8:573601. doi:10.3389/fmed.2021.573601
28. Medical Research Council. Aids to Examination of the Peripheral Nervous System. Her Majesty’s Stationary Office; 1976.
29. National Institute of Hospital Administration. Handbook of Nursing-Sensitive Quality Indicators. People’s Medical Publishing: 2016:138–139.
30. Alostaz Z, Rose L, Mehta S, Johnston L, Dale C. Physical restraint practices in an adult intensive care unit: a prospective observational study. J Clin Nurs. 2022;32(7–8):1163–1172. doi:10.1111/jocn.16264
31. Acevedo-Nuevo M, González-Gil MT, Martin-Arribas MC. Physical restraint use in intensive care units: exploring the decision-making process and new proposals. A multimethod study. Int J Environ Res Public Health. 2021;18(22):11826. doi:10.3390/ijerph182211826
32. Souza LMDS, Santana RF, Capeletto CDSG, Menezes AK, Delvalle R. Factors associated with mechanical restraint in the hospital environment: a cross-sectional study. Rev Esc Enferm Usp. 2019;53:e03473–e03473. doi:10.1590/s1980-220x2018007303473
33. van der Kooi AW, Peelen LM, Raijmakers RJ, et al. Use of physical restraints in Dutch intensive care units: a prospective multicenter study. Am J Crit Care. 2015;24(6):488–495. doi:10.4037/ajcc2015348
34. Luk E, Burry L, Rezaie S, Mehta S, Rose L. Critical care nurses’ decisions regarding physical restraints in two Canadian ICUs: a prospective observational study. Can J Crit Care Nurs. 2015;26(4):16–22.
35. Shehabi Y, Bellomo R, Reade MC, et al. Early goal-directed sedation versus standard sedation in mechanically ventilated critically ill patients: a pilot study. Crit Care Med. 2013;41(8):1983–1991. doi:10.1097/CCM.0b013e31828a437d
36. Bugedo G, Tobar E, Aguirre M, et al. The implementation of an analgesia-based sedation protocol reduced deep sedation and proved to be safe and feasible in patients on mechanical ventilation. Rev Bras Ter Intensiva. 2013;25(3):188–196. doi:10.5935/0103-507X.20130034
37. Finkielman JD. Randomized trial of light versus deep sedation on mental health after critical illness. Crit Care Med. 2010;38(1):349–350. doi:10.1097/CCM.0b013e3181c30cbc
38. Tanaka LM, Azevedo LC, Park M, et al. Early sedation and clinical outcomes of mechanically ventilated patients: a prospective multicenter cohort study. Crit Care. 2014;18(4):R156. doi:10.1186/cc13995
39. Kress JP, Hall JB. ICU-acquired weakness and recovery from critical illness. N Engl J Med. 2014;370(17):1626–1635. doi:10.1056/NEJMra1209390
40. Dres M, Dubé BP, Mayaux J, et al. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients. Am J Respir Crit Care Med. 2017;195(1):57–66. doi:10.1164/rccm.201602-0367OC
41. Kandeel NA, Attia AK. Physical restraints practice in adult intensive care units in Egypt. Nurs Health Sci. 2013;15(1):79. doi:10.1111/nhs.12000
42. Raguan B, Wolfovitz E, Gil E. Use of physical restraints in a general hospital: a cross-sectional observational study. Isr Med Assoc J. 2015;17(10):633–638.
43. Cui N, Zhang Y, Liu Y, et al. Protocol for the adaptation of clinical practice guidelines for the management of physical restraints in critically ill patients. Ann Palliat Med. 2021;10(4):4889–4896. doi:10.21037/apm-20-2133
44. Harrison MB, van den Hoek J, Graham ID. CAN-IMPLEMENT©: Planning for Best Practice Implementation. Wolters Kluwer: Philadelphia; 2014.
45. Cui N, Zhang Y, Li Q, et al. Quality appraisal of guidelines on physical restraints in intensive care units: a systematic review. Intensive Crit Care Nurs. 2022;70:103193. doi:10.1016/j.iccn.2021.103193
46. Cui N, Yan X, Zhang Y, et al. Non-pharmacological interventions for minimizing physical restraints use in intensive care units: an umbrella review. Front Med. 2022;9:806945. doi:10.3389/fmed.2022.806945
47. Cui N, Chen D, Zhang Y, et al. The effect of non-pharmacological interventions on physical restraint reduction in intensive care units: a protocol for an umbrella review of systematic reviews and meta-analysis. Ann Palliat Med. 2021;10(6):6892–6899. doi:10.21037/apm-21-626
48. Cui N, Yang R, Zhang H, et al. Using the evidence to decision frameworks to formulate the direction and strength of recommendations for adapted guidelines of physical restraints in critical care: a Delphi study. Intensive Crit Care Nurs. 2023;76:103382. doi:10.1016/j.iccn.2022.103382
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effects of Mukbang Watching on Enteral Feeding Intolerance Among Critically Ill Patients: Study Protocol for a Randomized Controlled Trail
Yin Y, Fan CF
Patient Preference and Adherence 2023, 17:2891-2897
Published Date: 9 November 2023