Back to Journals » Substance Abuse and Rehabilitation » Volume 16
Prevalence and Factors Associated with Probable Alcohol Use Disorder Among Men at Higher Risk of HIV Enrolled in the HIV Pre-Exposure Prophylaxis Program in Tanga, Tanzania. A Call for Integrated Care
Authors Kitomary NR ![]() , Metta E
, Metta E ![]() , Leshabari MT, Moen K, Mmbaga EJ
, Leshabari MT, Moen K, Mmbaga EJ
Received 11 July 2025
Accepted for publication 24 October 2025
Published 6 December 2025 Volume 2025:16 Pages 293—307
DOI https://doi.org/10.2147/SAR.S553175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra Badgaiyan
Nuruel Robert Kitomary,1,2 Emmy Metta,1 Melkizedeck Thomas Leshabari,1 Kåre Moen,2 Elia J Mmbaga2,3
1Department of Behavioural Sciences, Muhimbili University of Health and Allied Sciences, Dar Es Salaam, Tanzania; 2Department of Community Medicine and Global Health, University of Oslo, Oslo, Norway; 3Department of Epidemiology and Biostatistics, Muhimbili University of Health and Allied Sciences, Dar Es Salaam, Tanzania
Correspondence: Nuruel Robert Kitomary, Department of Behavioural Sciences, Muhimbili University of Health and Allied Sciences, 9-United Nations Road, Upanga, Dar-Es-Salaam, 11103, Tanzania, Tel +255 625928998, Email [email protected]
Background: Probable alcohol use disorder is rarely on the minds of people who use alcohol, probably due to technicality related to making that diagnosis. Men who have sex with men are more vulnerable to alcohol use, usually as a coping strategy to manage minority distress, stigma, violence and validation. This study determined the prevalence and factors associated with probable alcohol use disorder among men who have sex with men enrolled in the HIV pre-exposure prophylaxis program in Tanga, Tanzania.
Methodology: This study included 364 men who have sex with men recruited through respondent driven sampling. Structured questionnaire was used for socio-demographic and sexual characteristics data collection. Probable alcohol use disorder was assessed using the Alcohol Use Disorder Identification Test (AUDIT). A modified Poisson regression model was used to determine the factors associated with probable alcohol use disorder among men who have sex with men.
Results: Our study found that about 45% of participants had probable alcohol use disorder. The prevalence was high among participants with a history of having group sex (aPR=1.29; 95% CI: 1.00– 1.65, P=0.051), who had ever paid for oral or anal sex (aPR=1.65; 95% CI: 1.21– 2.25, p=0.002), who reported facing financial difficulties (aPR=1.40; 95% CI: 1.10– 1.79, p=0.007), those who experienced moderate stigma (aPR=1.44;95% CI: 1.13– 1.84, p=0.003) and higher stigma (aPR=1.39;95% CI: 1.02– 1.91, p=0.040).
Conclusion: The prevalence of probable alcohol use disorder was found to be relatively high among men who have sex with men, especially those with a history of group sex, paying for sex, facing financial difficulties and those who reported experiencing a moderate-to-high level of stigma. This highlights the need to intensify health, reproductive and safe sex practices programs while escalating anti-stigma campaigns. We recommend the integration of substance screening and harm reduction services in HIV treatments and prevention programming.
Keywords: alcohol use disorder, men who have sex with men, HIV pre-exposure prophylaxis, PrEP, Tanzania
Introduction
Alcohol use is a culturally accepted practice in many communities worldwide.1 With that acceptability, it can affect human life both biologically, psychologically, and socially, particularly when in problematic patterns of use, which develop gradually along the course of use. At this level, it represents a significant medical and mental health concern known as “alcohol use disorder.” This condition encompasses a cluster of cognitive, behavioural, and physiological symptoms, indicating that an individual continues to use alcohol despite facing substantial alcohol-related problems.2 Alcohol use disorder is a risk factor for numerous health conditions, such as diabetes, accidents, violence, and various social risks, including unprotected sexual intercourse, contributing up to approximately 5.1% of all disability-adjusted life years and 5.3% of global mortality.3 The disorder negatively impacts human life,4 resulting in poor health-seeking behaviours, which might lead to underutilization of health services, for example, inadequate use of HIV pre-exposure prophylaxis, neglect of self-care practices like unprotected sexual intercourse, and poor nutrition, thereby affecting both individuals and society as a whole.5
Men who have sex with men (MSM) as members of marginalized populations are at higher risk of using alcohol, exemplifying many other substances to cope with imposed distress for different reasons. In this study, alcohol use is identified as a behavioural response among the men who have sex with men compared to heterosexual men, which might affect their retention of PrEP, attracting attention for further exploration in the Tanzanian context.6 Their elevated risk of alcohol use is attributed to the need to alleviate stress stemming from community marginalization, discrimination, and stigma.7 Alcohol is seen as a means to raise confidence for engaging in sex, particularly in environments where sex is commodified8 among men who have sex with men. However, while alcohol initially serves the intended purpose, it may result in alterations in brain neurochemistry, resulting in both physical and behavioural changes, such as addiction, impaired health-seeking behaviours, and poor adherence to health guidelines.9
In western countries, reports shows that, 33.2% and 87.9% of men who have sex with men use alcohol, which can render them at a chance of impaired health-seeking behaviours such as HIV PrEP use and retention.10,11 In this scenario, they can be at higher susceptibility to HIV acquisition, mainly driven by impulsiveness and engagement in unprotected sexual intercourse; for example, the systematic reviews indicate that 13% to 15% of substance use, including alcohol, among men who have sex with men is specifically geared towards facilitating sexual activities, often leading to pathological use.12,13 Alcohol use is commonly initiated for social and recreational purposes, but later it ends up as alcohol use disorder, exemplified by findings in Peru where a study reported that approximately 62.8% of men who have sex with men met the criteria for alcohol use disorder, which is nearly two-thirds of them.14
In sub-Saharan Africa, studies demonstrate a wide range of alcohol use prevalence, from 1.4% to 100% among MSM, with notable rates of alcohol use disorder, particularly in Egypt and Kenya, respectively.15 In South Africa, alcohol use among men who have sex with men is among the recreational and communal influences, with some individuals using it to enhance sexual performance,16 but fewer studies have reported the specific prevalence of alcohol use disorder.
In Tanzania, approximately 14% of men who have sex with men have reported using any form of substances regardless of the severity, including alcohol, which is associated with risky sexual behaviours; a study which was done more than 17 years ago, when the interventions were limited than today.17 The prevalence of probable alcohol use disorder among men who have sex with men in Tanzania is unknown. Studies elsewhere report alcohol use among men who have sex with men to be related to positive HIV status, unstable housing, unemployment, and frequent diagnosis of sexually transmitted diseases;18 increased libido, sexual adventures, coping mechanisms for rejection and discrimination, anxiety, and low self-esteem as drivers of drug use in communities of men who have sex with men.19 In this understanding, alcohol use is an important health concern which deserves a special attention. However, the prevalence of probable alcohol use disorder and possible determinants are not known in the Tanzanian context among men who have sex with men. Therefore, this study aimed to determine the prevalence and factors associated with probable alcohol use disorder among men who have sex with men enrolled in the pre-exposure prophylaxis program in Tanga, Tanzania.
Methodology
Study Design and Setting
This was the cross-sectional analytical study design, presenting an analysis of data from a pragmatic quasi-experimental trial evaluating the rollout of HIV pre-exposure prophylaxis (PrEP) in Tanzania, known as the PREPTA study. The trial focused on both men who have sex with men and female sex workers across two regions Dar Es Salaam (intervention group) from March 2021 to July 2022 and Tanga (control group) from February 2022 to June 2023, respectively.20–22 This study explicitly analyses data from men who have sex with men for whom data regarding alcohol use were available and complete. The Tanga region (control arm) was chosen for this study as it represents real-world (without m health intervention) PrEP implementation in Tanzania.
Study Population and Eligibility
The study involved men who had sex with men who were enrolled in a pre-exposure prophylaxis program in Tanga, Tanzania. Eligibility criteria included being aged at least 18 years, having had sex with a man in the last 3 months, and having lived in the city of Tanga for the past 6 months, and other inclusion criteria such as creatinine clearance exceeding 60 mL/min and consented to initiate PrEP according to the national HIV guideline.23
Sample Size
The study used a convenient sample of 364 men who have sex with men, using data from the pre-exposure prophylaxis rollout in Tanzania (PREPTA) project. The original sample size for the PREPTA study was estimated at 369 men, based on a formula for calculating sample sizes in cohort studies that accounted for the RDS (Respondent-Driven Sampling) recruitment method.24,25
Data Collection Procedure
The PREPTA project data were collected through face-to-face interviews conducted by trained research assistants, who were well-prepared to ensure accurate and ethical data collection. The assistants received training that covered data safety, the research process, and ethical considerations. To protect participants’ sensitive information, responses were recorded on handheld tablets connected to the Services for Sensitive Data (TSD) platform, a secure server with strict access and data transfer controls.21,22 The tools for data collection were, standardized and tested with 10 participants to check for clarity, ease of understanding, and cultural relevance before data collection. The AUDIT tool was used for assessing alcohol use disorder, standardized questionnaire contained questions focusing on sexual behaviors, HIV knowledge, PrEP-related stigma, self-efficacy, and social support, depressive symptoms and anxiety symptoms.
Measurements
Dependent Variable
The primary outcome was probable alcohol use disorder. To determine the prevalence of alcohol use disorder, all participants who scored ≥16 in the alcohol use disorder identification test tool (AUDIT) were considered positive (probable alcohol use disorder).26 Alcohol use was evaluated using the Alcohol Use Disorders Identification Test; a 10-item screening tool developed by the World Health Organization to help healthcare providers identify individuals who may benefit from interventions aimed at reducing alcohol use.26 We employed a Swahili version of the instrument, which has been validated in a Tanzanian population of patients with traumatic brain injury, with only minor adjustments in wording to enhance clarity.27 The AUDIT is designed to detect hazardous and harmful drinking patterns as well as potential alcohol dependence. The first three questions focus on hazardous drinking, defined as alcohol consumption that increases the risk of adverse outcomes without necessarily indicating a disorder.26 These questions assess drinking frequency, the typical quantity of alcohol consumed, and the frequency of heavy drinking episodes.
Four additional items specifically target harmful alcohol use and address issues such as blackouts, feelings of guilt, alcohol-related injuries, and concern from others about the individual’s drinking. The remaining items assess classic signs of dependence, including prioritization of drinking, difficulty in controlling alcohol use, and drinking in the morning. The total score ranges from 0 to 40. According to WHO guidelines; scores of 8–15 indicate hazardous use, scores of 16–19 reflect harmful use, and scores of 20 or above suggest probable dependence. Individuals in these categories require psychotherapies, pharmacological treatment and monitoring in line with WHO recommendations.26 Participants who reported no alcohol consumption in the past twelve months were not asked to complete the AUDIT tool because their maximum possible score would not exceed 6, and they were automatically categorized as low-risk.
Independent Variables
The independent variables in the study were grouped into socio-demographic and sexual characteristics which included the following: age which was grouped into two groups (18–24years and ≥25years), education level grouped as either primary education and low including informal educations, marital status categorized as never married versus any history of marriage either currently of previously, having own children as either father to a child or never had a child, easy access to condoms (one can get a condom timely when he wants to have sex either dispensable in hotels, in health facilities or can buy), financial dependents (having people who directly depend on him to get money either yes or no), monthly personal income in Tanzanian shillings (all income he collected via formal or informal employment in a month categorized as ≤100,000/= or 100,001–299,999/= and ≥300,000/=), financial barriers to accessing healthcare (inability to accessing healthcare services due to lack of money to pay for that service as yes or no), history of sexually transmitted diseases (asked for any history of sexually transmitted disease based of different symptoms like urethral discharge as yes or no), HIV knowledge as yes or no, twelve-month history of forced sex (being engaged in anal sex without his willingness as yes or no), self-perceived HIV status as low, moderate of high, PrEP self-efficacy (extent of his believe that PrEP can offer protection against HIV transmission as low or high), prior arrests by police as yes or no. Social support was measured using an 8-item, 5-point Likert scale adapted from the Duke-UNC Functional Social Support Questionnaire (FSSQ), which demonstrated high reliability with a Cronbach’s alpha of 0.88. A total score below 32 indicated inadequate social support and above that was adequate social support.21,22 Perceived stigma against men who have sex with men was evaluated using 13 items a Swahili translated and pre-tested questionnaire, each question with five response options (1 = Strongly Disagree to 5 = Strongly Agree), yielding a high reliability with a Cronbach’s alpha of 0.84. Moreover, stigma was categorized into low (scores ≤26), moderate (scores 27–38), and high (scores ≥39). Furthermore, perceived PrEP stigma was measured using a 10-item scale a Swahili translated and pre-tested questionnaire, a five point Likert scale, checked for internal consistency with a Cronbach’s alpha of 0.88. Lastly, the PrEP stigma was classified as low (scores ≤30) or high (scores >30); all these were composed in the baseline questionnaire.28 Lastly, the mental distress (depressive or anxiety symptoms or both), which was assessed using both the patient health questionnaire (PHQ-2) and the generalized anxiety questionnaire (GAD-2), was determined by the presence of either depressive symptoms or anxiety symptoms or both. The PHQ-2 assesses anhedonia, ie, how often the patient has had “little interest or pleasure in doing things” in the past two weeks, and depressed mood, ie, feeling down, depressed, or hopeless. Items are responded to on a Likert-type scale from 0-Not at all to 3-Nearly every day for a total score of 0 to 6.29,30 Similarly, the GAD-2 assesses “Feeling nervous, anxious, or on edge” and “Not being able to stop or control worrying” for the past two weeks. Items are responded to on a Likert-type scale from 0-Not at all to 3-Nearly every day for a total score of 0 to 6.29,30 Both of these tools are short versions for quick community-based population screening and validated in Tanzania with good internal consistency at a Cronbach alpha of 0.81 by Materu et al in Tanzania.31,32 Both tools were translated to Swahili language, a national language and were pre-tested before data collection started.
Data Analysis
Descriptive statistics for continuous variables were summarized using the mean and standard deviation, while categorical variables, such as education level, were presented as proportions. In bivariate analysis, the chi-square test was used to screen for the factors associated with probable alcohol use disorder, which will be selected for the final regression analysis. Few factors were selected to be included in the modified Poisson regression analysis, especially those with a p-value <0.2 in the bivariate analysis, and those identified in previous literature to be related to probable alcohol use disorder. Given that the prevalence of alcohol used disorder (45%) exceeds 10%, the modified Poisson logistic regression with robust standard errors was used to determine independent factors associated with probable alcohol use disorder with the measure of association a prevalence ratio. This method was chosen because it minimizes the risk of overestimating effects, which can occur when using a conventional logistic regression model.33 Variables with a p-value <0.05 in the multivariable modified Poisson regression model were considered statistically significant. All analyses were conducted using STATA, version 18.
Ethical Consideration
The study was conducted in accordance with Declaration of Helsinki. It received ethical clearance registration number MUHAS-REC-12-2024-2542 from the Muhimbili University of Health and Allied Sciences Ethical Review Committee in Tanzania. The study project from which data for this study received ethical approval from the Regional Committee for Medical and Health Research Ethics (REK) in Norway (protocol ref no: 33675). All the study participants provided their written informed consent to participate in this study.
Results
Sociodemographic Characteristics of Men Who Have Sex with Men Who Enrolled in HIV Pre-Exposure Prophylaxis
A total of 364 participants were included in the data analysis. The mean (±SD) age of the study participants was 24.7±5.5 years, whereby more than half (59.0%) were between 18 and 24 years old, and most (87.91%) had never been married.
Regarding the total monthly income, slightly more than one-third (31.86%) of participants reported a monthly income between 100,000 and less than 300,000, while nearly one-third (31.86%) earned 100,000 or less. The remaining participants had a monthly income of 300,000 or more.
Additionally, two-thirds (66.1%) of the participants had no children, while 65.66% of them had financial dependents. Furthermore, almost half (49.45%) reported facing financial difficulties when accessing healthcare services.
In univariable analysis, the age group of the participants (p=0.000), having their own children (p=0.000), having financial dependents (p=0.000) and facing financial difficulties in accessing health care (p=0.000) were associated with probable alcohol use disorder. At the same time, other sociodemographic characteristics were not (Table 1).
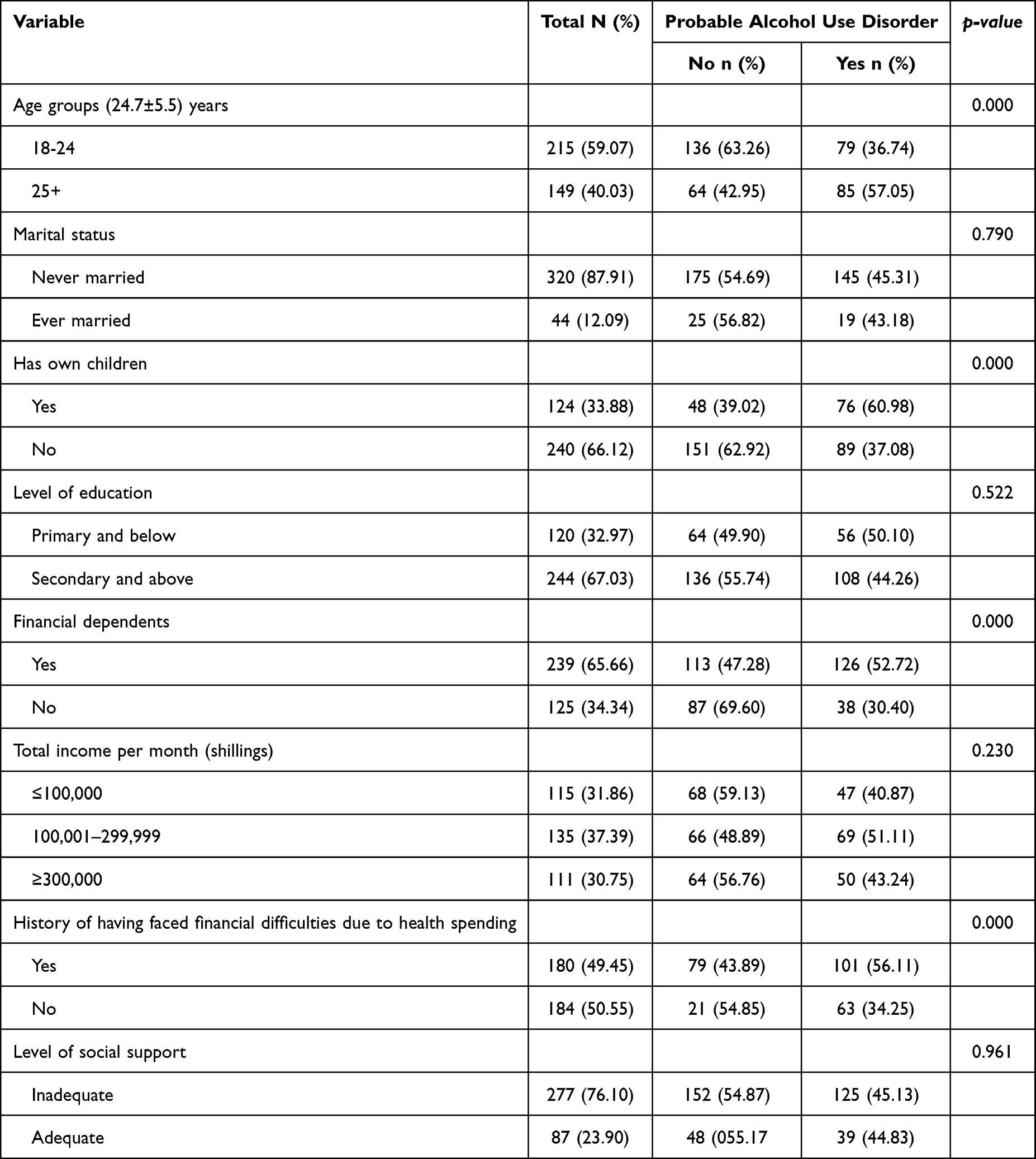 |
Table 1 Distribution of Sociodemographic Characteristics by Probable Alcohol Use Disorder Among Men Who Have Sex with Men Enrolled on HIV Pre-Exposure Prophylaxis |
Structural and Sexual Characteristics of Men Who Have Sex with Men Enrolled in HIV Pre-Exposure Prophylaxis
The mean age of sexual debut among participants was 15.9±2.7 years, where nearly three-quarters (70.88%) of them had a sexual debut below 18 years of age, and more than a third (36.26%) of them had either anal, oral or thighs sexual debut. Regarding the age of first anal sex, 40.41% of them had their first anal sex at an age less than 18 years, and nearly a third (31.04%) of participants had a man as their first sexual partners.
About a three-quarters (77.75%) had an insertive role in their last anal sex. More than two-thirds (69.33%) of the study participants reported no use of condoms in their last anal, and more than half of them had multiple sexual partners (55.49%). Nearly three-quarters (74.45%) of the participants reported ever paid for having oral or anal sex, and almost 1 in every 10 participants (11.54%) had a history of having group sex and 15.38% of them had a history of being arrested during the past twelve months. More than three-quarters (77.47%) of the participants reported easy access to male condoms, but 12.64% of them had a history of being diagnosed with sexually transmitted diseases in the previous six months. Furthermore, about 71.97% of the participants perceived themselves as at higher risk of HIV acquisition, while more than a third (35.16%) reported experiencing moderate stigma, and 14.01% reported experiencing high levels of stigma and about 16.76% participants had mental distress (having either depressive symptoms/anxiety symptoms or both).
During bivariable analysis, the last anal sex position role (p=0.031), history of ever paid for having oral or anal sex (p=0.002), history of being arrested in the past 12 months (p=0.048), having group sex (p=0.013) and experienced stigma (p=0.010) were associated with probable alcohol use disorder, while factors did not (Table 2).
 |
Table 2 Distribution of Structural and Sexual Characteristics by Probable Alcohol Use Disorder Among Men Who Have Sex with Men Enrolled on Pre-Exposure Prophylaxis |
Factors Associated with Probable Alcohol Use Disorder Among Men Who Have Sex with Men Enrolled in HIV Pre-Exposure Prophylaxis
The participants with a history of having group sex had a higher prevalence of probable alcohol use disorder compared to those who were not (aPR=1.29; 95% CI: 1.00–1.65, P=0.051). Those who had ever paid for oral or anal sex had nearly twice higher the prevalence of probable alcohol use disorder compared to their counterparts (aPR=1.65; 95% CI: 1.21–2.25, p=0.002). Also, the study participants who reported facing financial difficulties in accessing healthcare services had a higher prevalence of probable alcohol use disorder (aPR=1.40; 95% CI: 1.10–1.79, p=0.007). The prevalence of probable alcohol use disorder was also increased among participants who experienced moderate stigma (aPR=1.44;95% CI: 1.13–1.84, p=0.003) and higher stigma (aPR=1.39;95% CI: 1.02–1.91, p=0.040) compared to those with a low level of experienced stigma (Table 3).
 |
Table 3 The Factors Associated with Probable Alcohol Use Disorder Among Men Who Have Sex with Men Enrolled in HIV Pre-Exposure Prophylaxis |
Discussion
Our study identified less integrated care by detecting the probable alcohol use disorder among men who have sex with men at a prevalence of 45% during the pre-exposure prophylaxis rollout programme in Tanga, Tanzania. The study found that probable alcohol use disorder to be common among men who have sex with men enrolled in the programme, presenting an inadequately integrated HIV prevention and treatment service. The history of group sex, history of paying for anal or oral sex, facing financial difficulties and those experiencing stigma were associated with higher prevalence of probable alcohol use disorder.
Our study has replicated the findings from a study in Lima by Harrera et al,34 which reported a similar prevalence (45%) among MSM and transgender women. The similarity could be due to the use of similar measurements and a slightly larger sample size, which can affect the ratio even if they had more cases than in our case. However, the different findings have been reported in Colombia at the prevalence of 18.8%, lower than the findings of our study.35 Although, it should be noted that this prevalence was reported in age-specific groups, mainly those aged eighteen to twenty-three years of age. Furthermore, in the comparison study,36 they used the Diagnostic and Statistical Manual version IV (DSM-IV) in screening for alcohol use disorder, which introduces subjectivity and under- or overestimation compared to the AUDIT tool, which was used in our study, a standardized tool.
Unlike our study, the Peruvian studies have reported a higher prevalence of alcohol use disorder at 55.2%37 and 62.8%38 in a similar population, however, in different periods. Some reasons for the higher prevalence could be due to fact that the comparison study used low cut-off points (≥8) (increasing number of cases) compared to our study where we used higher cut-off points (≥15) in scoring alcohol use disorder identification test. The comparison studies also used the large sample size which increases the chances of picking the cases compared to our research, which involved only one city.
The reported probable alcohol use disorder in this study is almost double the prevalence reported in the general population of men in northern Tanzania,39 but less than what was reported from studies from other African countries, such as South Africa.40,41 In line with that, the prevalence of probable alcohol use disorder among MSM was relatively higher compared to female sex workers in Tanzania.42 Although the occasional alcohol use is common among MSM, the escalated level of psychosocial distress can prompt a use as copying strategy and later on long term use some of them can end up with alcohol use disorder as a mental health concern,43 hence elevating the prevalence of alcohol use disorder in this community. The available evidence shows that, integrating substance use such as alcohol screening into HIV programming, and addressing substance use can improve the success of other interventions, such as PrEP uptake and adherence,44 which can be a good step to take in line with findings of this study.
Concerning the possible determinants, this study found that the history of group sex, history of paying for anal or oral sex, facing financial difficulties and those experiencing stigma were associated with higher prevalence of probable alcohol use disorder. Our study found a higher prevalence of probable alcohol use disorder among MSMs with a history of engaging in group sex. Engaging in group sex, exemplifies the different risky sexual behaviours which have been consistently reported in various studies across the world among people who use substances such as alcohol, with particular attention in key and vulnerable populations, such as men who have sex with men.45,46 The behaviours could stem from different factors, including a need for sexual adventure, disinhibition and impaired judgment due to intoxication, desire for social acceptance, validation and confidence within their sexual networks.43,45 The interaction of these psychosocial reasons can explain the possible association found by this study. This finding is particularly important for public health interventions and prevention programs, as group sex under the influence of alcohol often leads to neglected or improper condom use,43,45 thereby increasing the risk of HIV transmission and other health consequences.
In line with similar behavioural patterns, our study has found that participants who had a history of paying for sex had a higher prevalence of probable alcohol use disorder compared to their counterparts.47 The findings of our study are consistent with a study by Diane et al in the Dominican Republic, which found that exchanging sex for anything or paying for sex was common among their study participants.48 Paying for sex and transactional sex are among the findings which have been reported from the previous studies, such as a study by Sheri et al in Botswana,49 which found a strong association between paying for sex and problematic alcohol use. This is among the risky sexual behaviours which have been discussed with particular attention in key and vulnerable populations such as men who have sex with men, as it can play a mediating role in HIV transmission,50 due to autonomy and decision-making compromise as buyers of sex can be decision makers for condoms use.
MSM who reported facing financial difficulties showed a higher prevalence of alcohol use disorder compared to their counterparts. These findings align with those of a 2018 study by Su Hyun et al in Paris,49 which reported an increased prevalence of substance use, including alcohol, among men who have sex with men experiencing financial hardship. On top of this, our findings are also consistent with reports from China48 and Ireland,50 where the studies found an association of low-income level, unemployment (indicating possible financial difficulties) and alcohol use disorder among men who have sex with men. The relationship between financial difficulties and alcohol use disorder can be understood from multiple perspectives. The social causation hypothesis51 suggests that financial hardship makes MSM more vulnerable to alcohol use disorder due to psychological distress, leading to drinking as a coping mechanism, and limited access to healthcare services, including medical and psychological support. Conversely, the social drift hypothesis posits that alcohol use disorder can contribute to financial difficulties.51 It argues that the disorder disrupts normal brain reward circuitry, impairing behaviours and reducing the ability to engage in income-generating activities, thereby perpetuating financial hardship. However, unlike our study findings, Wenhua and colleagues11 in New York found no association between alcohol use and income level among men who have sex with men; this could be due to population (have relatively stable economy to meet basic needs compared to MSM in Tanga, Tanzania) and methodological differences, (their study was matched case control study attracting effect of similarity).
Furthermore, our study found an increased prevalence of probable alcohol use disorder among the participants who reported experiencing a moderate to high level of stigma. The experienced stigma among MSM has been reported in the different literature52,53 such that some will cope by excessive alcohol intake, leading to probable or clinical alcohol use disorder. Studies have reported similar findings to our study, regardless of the population studied,54,55 which justifies the science behind “stigma is stigma, no matter what type and where, or to whom”, and so addressing is a crosscutting issue. Stigma has an intrinsic role in determining the quality of life of men who have sex with men in communities where this type of sex orientation is criminalized and it can led to different ameliorative coping strategies, such as alcohol use.54 This presents an opportunity for researchers and healthcare stakeholders to strengthen anti-stigma campaigns, promote health for all, and improve the coverage and utilization of healthcare services, particularly in reproductive health, HIV treatments and prevention programming.
The Study Limitation
The study had several limitations. Participants were recruited based on their eligibility for PrEP; hence, they may not represent the actual population of men who have sex with men. Participants identified with alcohol use disorder by the screening tool AUD did not receive further assessments for diagnosis or interventions. The use of respondent-driven sampling methods, a non-probabilistic method in the recruitment of respondent-driven sampling methods, and a non-probabilistic method in the recruitment may have introduced selection bias. However, the regression analysis of respondent driven sampling data has been indicated to be accurate in estimating predictors of outcome, similar to estimates from probabilistic sampling. Furthermore, the use of standardized measures and efforts to ensure confidentiality and anonymity might have addressed these potential biasses.
Conclusions and Recommendations
The prevalence of probable alcohol use disorder was found to be relatively high. This is especially true among those who reported a history of group sex, paying for sex, facing financial difficulties and those who reported experiencing a moderate-to-high level of stigma. This highlights the need for health stakeholders, researchers and scientists to intensify health, reproductive and safe sex practices while escalating anti-stigma campaigns. We recommend the integration of substance screening and harm reduction services in HIV treatments and prevention programming to improve the outcomes.
Data Sharing Statement
Access to the data used in this analysis is available upon reasonable request to the principal investigator (PI) of the PREPTA project.
Contact details: Prof. Elia J. Mmbaga Email: [email protected].
Acknowledgment
This study utilized data collected during the PREPTA project funded by the Research Council of Norway through the Global Health and Vaccination Programme (GLOBVAC) [project number 285361]. We sincerely thank the project team for their dedication in fulfilling the project and supporting us throughout. We are also deeply grateful to the participants, as their involvement made this study possible.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. Global status report on alcohol and health_2018. [cited May 14, 2025]; Available from: https://iris.who.int/bitstream/handle/10665/274603/9789241565639-eng.pdf.
2. Mushi D, Francis JM, Moshiro C, Hanlon C, Teferra S. Integration of alcohol use disorder interventions in general health care settings in Sub-Saharan Africa: a scoping review. Front Psychiatry. 2022;13. doi:10.3389/fpsyt.2022.822791
3. Newbury-Birch D, Ferguson J, Connor N, Divers A, Waller G. A rapid systematic review of worldwide alcohol use disorders and brief alcohol interventions in the criminal justice system. Front Psychiatry. 2022;Vol. 13. doi:10.3389/fpsyt.2022.900186
4. Klingemann H. Alcohol and its social consequences-the forgotten dimension. 2001 [cited May 26, 2025]. Available from: https://iris.who.int/bitstream/handle/10665/108554/WHO-EURO-2001-3851-43610-61278-eng.pdf?sequence=1&isAllowed=y.
5. Nagpal J, Divya M, Prasad S, et al. “ALCOHOL CONTROL” SERIES, No. 4 reducing harm from use of alcohol-community responses “Expressions”-The life-skills education and school mental health programme child and adolescent centre.
6. Delphin-Rittmon ME, Secretary for Mental Health A, Use S, Abuse S. Health services administration M. lesbian, gay, or bisexual adultsslides for the 2020 national survey on drug use and health. 2022.
7. Harper GW, Crawford J, Lewis K, et al. Mental health challenges and needs among sexual and gender minority people in western Kenya. Int J Environ Res Public Health. 2021;18(3):1–22. doi:10.3390/ijerph18031311
8. Compton WM, Jones CM. Substance use among men who have sex with men. N Engl J Med. 2021;385(4):352–356. doi:10.1056/NEJMra2033007
9. Mackesy-Amiti ME, Fendrich M, Johnson TP. Substance-related problems and treatment among men who have sex with men in comparison to other men in Chicago. J Subst Abuse Treat. 2009;36(2):227–233. doi:10.1016/j.jsat.2008.06.004
10. Htut KM, Areesantichai C, Mon MM. Alcohol consumption patterns among men who have sex with men in major cities of Myanmar: a cross-sectional study. F1000Res. 2020;9:1149. doi:10.12688/f1000research.25707.1
11. Lu W, Vu TT, Wilton L, et al. Patterns and factors associated with alcohol misuse among young black men who have sex with men in New York City. Am J Mens Health. 2024;18(3). doi:10.1177/15579883231218580
12. Tomkins A, George R, Kliner M. Sexualised drug taking among men who have sex with men: a systematic review. In: Perspectives in Public Health. Vol. 139. SAGE Publications Ltd; 2019:23–33.
13. Nevendorff L, Schroeder SE, Pedrana A, Bourne A, Stoové M. Prevalence of sexualized drug use and risk of HIV among sexually active MSM in East and South Asian countries: systematic review and meta-analysis. J Int AIDS Soc. 2023;26(1):26054. doi:10.1002/jia2.26054
14. Galea JT, Kinsler JJ, Salazar X, et al. Acceptability of pre-exposure prophylaxis as an HIV prevention strategy: barriers and facilitators to pre-exposure prophylaxis uptake among at-risk peruvian populations. Int J STD AIDS. 2011;22(5):256–262. doi:10.1258/ijsa.2009.009255
15. Sandfort MTG, Knox JR, Alcala C, El-Bassel N, Kuo I, Smith LR. Substance use and HIV risk among men who have sex with men in Africa: a systematic review. 2017. Available from: http://links.lww.com/QAI/B46.
16. Williams PP, Carney T, Plüddemann A, Parry CDH. Intervening to identify and reduce drug use and sexual HIV risk patterns among men who have sex with men in three provinces in South Africa. J Subst Use. 2014;19(1–2):141–146. doi:10.3109/14659891.2012.760009
17. Johnston LG, Holman A, Dahoma M, et al. HIV risk and the overlap of injecting drug use and high-risk sexual behaviours among men who have sex with men in Zanzibar (Unguja), Tanzania. Int J Drug Policy. 2010;21(6):485–492. doi:10.1016/j.drugpo.2010.06.001
18. Mrisho A, Rutatinisibwa H, Msalale G, et al. Reasons influencing PrEP continuity among key and priority populations in Tabora region, Tanzania. A cross-sectional study [Internet]. 2022 [cited March 27, 2025]. Available from: https://sjhresearchafrica.org/index.php/public-html/article/view/285/185.
19. Ahaneku H, Ross MW, Nyoni JE, et al. Depression and HIV risk among men who have sex with men in Tanzania. AIDS Care. 2016;28:140–147.
20. Lichtwarck HO, Mbotwa CH, Kazaura MR, Moen K, Mmbaga EJ. Early disengagement from HIV pre-exposure prophylaxis services and associated factors among female sex workers in Dar es Salaam, Tanzania: a socioecological approach. BMJ Glob Health. 2023;8(12):e013662. doi:10.1136/bmjgh-2023-013662
21. Mbotwa C, Kazaura M, Moen K, et al. Predictors of mHealth use in promoting adherence to pre-exposure prophylaxis among female sex workers: an evaluation of the Jichunge intervention in Dar es Salaam, Tanzania. BMC Health Serv Res. 2022;22(1). doi:10.1186/s12913-022-08245-2
22. Mbotwa CH, Kazaura MR, Moen K, et al. Effect of an mHealth intervention on retention in HIV pre-exposure prophylaxis services among female sex workers: preliminary evidence of the use of the Jichunge app in Dar es Salaam, Tanzania. Digit Health. 2023;9. doi:10.1177/20552076231170507
23. National Center for HIV C, Hepatitis V, Prevention T. Prescribing pre-exposure prophylaxis (PrEP) A guide for health care providers 2023 1. 2023 [cited March 27, 2025]. Available from: https://www.hiv.gov/hiv-basics/hiv-prevention/using-hiv-medication-to-reduce-risk/pre-exposure-prophylaxis.
24. Gile KJ, Handcock MS. Respondent driven sampling an assessment of current methodology. Nat Library Med. 2012;40(1):285–327.
25. World Health Organization(WHO). Introduction to hiv/aids and sexually transmitted infection surveillance MODULE 4 Introduction to respondent-driven sampling. [cited March 27, 2025];11–392. Available from: https://applications.emro.who.int/dsaf/emrpub_2013_en_1539.pdf.
26. Babor TF, Robaina K. The Alcohol Use Disorders Identification Test (AUDIT): a review of graded severity algorithms and national adaptations. Int J Alcohol Drug Res. 2016;5(2):17–24. doi:10.7895/ijadr.v5i2.222
27. Vissoci JRN, hertz J, El-Gabri D, et al. Cross-cultural adaptation and psychometric properties of the AUDIT and CAGE questionnaires in Tanzanian Swahili for a traumatic brain injury population. Alcohol Alcohol. 2018;53(1):112–120. doi:10.1093/alcalc/agx058
28. Mikomangwa WP, Moen K, Mmbaga EJ, et al. HIV pre-exposure prophylaxis use during periods of unprotected sex among female sex workers in Tanga city, Tanzania: a control arm analysis of the pragmatic quasi-experimental trial. Front Public Health. 2024;12.
29. Kroenke K, Spitzer RL, Williams JBW. The patient health questionnaire-2 validity of a two-item depression screener. 2009 [cited March 27, 2025]. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(09)60009-X/abstract.
30. Löwe B, Wahl I, Rose M, et al. A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. 2010;122(1–2):86–95. doi:10.1016/j.jad.2009.06.019
31. Hlynsson JI, Carlbring P. Diagnostic accuracy and clinical utility of the PHQ-2 and GAD-2: a comparison with long-format measures for depression and anxiety. Front Psychol. 2024;15.
32. Materu J, Kuringe E, Nyato D, et al. The psychometric properties of PHQ-4 anxiety and depression screening scale among out of school adolescent girls and young women in Tanzania: a cross-sectional study. BMC Psychiatry. 2020;20(1). doi:10.1186/s12888-020-02735-5
33. Gnardellis C, Notara V, Papadakaki M, Gialamas V, Chliaoutakis J. Overestimation of relative risk and prevalence ratio: misuse of logistic modeling. Diagnostics. 2022;12(11):2851. doi:10.3390/diagnostics12112851
34. Herrera MC, Konda KA, Leon SR, et al. Impact of alcohol use on sexual behavior among men who have sex with men and transgender women in Lima, Peru. Drug Alcohol Depend. 2016;161:147–154. doi:10.1016/j.drugalcdep.2016.01.030
35. Peralta RL, Victory E, Thompson CL. Alcohol use disorder in sexual minority adults: age- and sex- specific prevalence estimates from a national survey, 2015-2017. Drug Alcohol Depend. 2019;205:107673. doi:10.1016/j.drugalcdep.2019.107673
36. McCabe SE, Hughes TL, West BT, Veliz P, Boyd CJ. DSM-5 alcohol use disorder severity as a function of sexual orientation discrimination: a national study. Alcohol Clin Exp Res. 2019;43(3):497–508. doi:10.1111/acer.13960
37. Vagenas P, Ludford KT, Gonzales P, et al. Being unaware of being HIV-Infected is associated with alcohol use disorders and high-risk sexual behaviors among men who have sex with men in Peru. AIDS Behav. 2014;18(1):120–127. doi:10.1007/s10461-013-0504-2
38. Ludford KT, Vagenas P, Lama JR, et al. Screening for drug and alcohol use disorders and their association with HIV-related sexual risk behaviors among men who have sex with men in Peru. PLoS One. 2013;8(8):e69966. doi:10.1371/journal.pone.0069966
39. McNee M, Badrinarayanan N, Strand E, et al. Sex differences in alcohol use patterns and related harms: a mixed-methods, cross-sectional study of men and women in northern Tanzania. PLOS Global Public Health. 2024;4(11):e0003942. doi:10.1371/journal.pgph.0003942
40. Kalichman SC, Simbayi LC, Cain D, Jooste S. Alcohol expectancies and risky drinking among men and women at high-risk for HIV infection in Cape Town South Africa. Addict Behav. 2007;32(10):2304–2310. doi:10.1016/j.addbeh.2007.01.026
41. Simbayi LC, Phil D, Kalichman SC, et al. Alcohol use and sexual risks for HIV infection among men and women receiving sexually transmitted infection clinic services in Cape Town, South Africa*. J Studies Alcohol. 2004;65(4):434–442. doi:10.15288/jsa.2004.65.434
42. Lichtwarck HO, Kazaura MR, Moen K, Mmbaga EJ. Harmful alcohol use and associated socio-structural factors among female sex workers initiating hiv pre-exposure prophylaxis in Dar es Salaam, Tanzania. Int J Environ Res Public Health. 2023;20(1).
43. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. 2003;129:674–697. doi:10.1037/0033-2909.129.5.674
44. Taibo L, Matsushima M, Timpson W, et al. Behavioral interventions targeting alcohol use among people living with HIV/AIDS: a systematic review and meta-analysis. AIDS Behav. 2017;21(Suppl 2):126–143. doi:10.1007/s10461-017-1886-3
45. Heath J, Lanoye A, Maisto SA. The Role of Alcohol and Substance Use in Risky Sexual Behavior Among Older Men Who Have Sex with Men: A Review and Critique of the Current Literature. Vol. 16. Media, LLC: AIDS and Behavior. Springer Science and Business; 2012:578–589.
46. Deiss RG, Clark JL, Konda KA, et al. Problem drinking is associated with increased prevalence of sexual risk behaviors among men who have sex with men (MSM) in Lima, Peru. Drug Alcohol Depend. 2013;132(1–2):134–139. doi:10.1016/j.drugalcdep.2013.01.011
47. Berg RC, Weatherburn P, Marcus U, Schmidt AJ. Links between transactional sex and HIV/STI-risk and substance use among a large sample of European men who have sex with men. BMC Infect Dis. 2019;19(1). doi:10.1186/s12879-019-4326-3
48. Yu L, Jiang C, Na J, et al. Elevated 12-month and lifetime prevalence and comorbidity rates of mood, anxiety, and alcohol use disorders in Chinese men who have sex with men. PLoS One. 2013;8(4).
49. Park SH, Al-Ajlouni Y, Palamar JJ, et al. Financial hardship and drug use among men who have sex with men. Subst Abuse Treat Prev Policy. 2018;13(1). doi:10.1186/s13011-018-0159-0
50. Daly FP, O’Donnell K, Davoren MP, et al. Potential alcohol use disorder among MSM in Ireland - Findings from the European MSM internet survey (EMIS 2017). Drug Alcohol Depend. 2021;223:108698. doi:10.1016/j.drugalcdep.2021.108698
51. Jones L, Sumnall H. Understanding the relationship between poverty and alcohol misuse. 2016 [cited May 26, 2025]. 1–41 p. Available from: https://www.drugsandalcohol.ie/25676/1/Understanding-the-relationship-between-poverty-and-alcohol-abuse-2.pdf.
52. Shangani S, Naanyu V, Operario D, Genberg B. Stigma and healthcare-seeking practices of men who have sex with men in Western Kenya: a mixed-methods approach for scale validation. AIDS Patient Care STDS. 2018;32(11):477–486. doi:10.1089/apc.2018.0101
53. Saalim K, Amu-Adu P, Amoh-Otu RP, et al. Multi-level manifestations of sexual stigma among men with same-gender sexual experience in Ghana. BMC Public Health. 2023;23(1). doi:10.1186/s12889-023-15087-y
54. Crozier ME, Farokhnia M, Persky S, Leggio L, Curtis B. Relationship between self-stigma about alcohol dependence and severity of alcohol drinking and craving. BMJ Mental Health. 2023;26(1):e300852. doi:10.1136/bmjment-2023-300852
55. Earnshaw VA, Jin H, Wickersham JA, et al. Stigma toward men who have sex with men among future healthcare providers in Malaysia: would more interpersonal contact reduce prejudice? AIDS Behav. 2016;20(1):98–106. doi:10.1007/s10461-015-1168-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Retention in HIV Pre-Exposure Prophylaxis Among Men Who Have Sex with Men in Tanga, Tanzania
Kiondo F, Metta E, Mmbaga EJ, Leshabari MT, Swai C, Mbotwa CH, Moen K
HIV/AIDS - Research and Palliative Care 2025, 17:185-194
Published Date: 11 July 2025