Back to Journals » Clinical Optometry » Volume 14
Prevalence and Factors Associated with Myopia Among High School Students in Hawassa City, South Ethiopia, 2019
Authors Gebru EA ![]() , Mekonnen KA
, Mekonnen KA
Received 27 March 2021
Accepted for publication 9 August 2021
Published 10 March 2022 Volume 2022:14 Pages 35—43
DOI https://doi.org/10.2147/OPTO.S308617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Mr Simon Berry
Elias Abera Gebru, Kidus Ayichluhem Mekonnen
Department of Optometry, College of Medicine and Health Sciences, Hawassa University, Hawassa, South Ethiopia
Correspondence: Elias Abera Gebru Department of Optometry, College of Medicine and Health Sciences, Hawassa University, PO Box 1560, Hawassa, Ethiopia Tel +251 918190360 Email [email protected]
Purpose: Myopia is one of the avoidable causes of visual impairment. Twenty-seven percent of the world population were myopic in 2010 and after 30 years it is expected half of the peoples in the planet will become myopic. The aim of this study was to determine the prevalence and factors associated with myopia among high school students.
Materials and Methods: A cross-sectional school-based study design using stratified simple random sampling technique was used to select 349 high school students from 21 high schools in Hawassa city. The study was conducted from April 24 to May 7, 2019. Structured questionnaire, six meter Snellen visual acuity chart, trial frame, trial set, retinoscope and cyclopentolate 1% eye drops were used to collect data. Data were analyzed using Statistical Package for Social Science (SPSS) version 20 computer software. Variables having p-value < 0.05 in multivariate logistic regression were considered as statistically significant.
Results: A total of 349 participants having a response rate of 97% were involved with the mean age of 16.90± 1.32 years. Prevalence of myopia was 16.05% (95%CI: 12.6, 20.1). Early age of schooling (adjusted odds ratio, AOR=3.14; 95%CI: 1.16, 10.06), parents being myopic (AOR=8.46; 95%CI: 7.11, 12.08), prolonged near work (AOR=11.65; 95%CI: 2.11, 64.5), short working distance (AOR=10.90; 95%CI: 0.57, 20.55), lack of outdoor sport activities (AOR=7.37; 95%CI: 2.71, 20.03) and visual display unit (VDU) usage (AOR=8.36; 95%CI: 2.39, 29.33) were variables significantly associated with myopia.
Conclusion and Recommendations: The prevalence of myopia was high in the study area. Early age of schooling, parents being myopic, prolonged near work, short working distance, lack of outdoor sport activities, and visual display unit usage were variables significantly associated with myopia. There should be strategies to prevent visual impairments secondary to myopia with affordable optical corrections and appropriate use of visual display units.
Keywords: myopia, prevalence, high school students, Hawassa, Ethiopia
Introduction
Myopia is a refractive error which occurs when parallel light rays from an object at infinity are focused in front of the retina, when accommodation is relaxed. Its main symptom is blurred distance vision.1 In most studies done on adults having spherical equivalent power of ≥ −0.50 diopter (DS) in both eyes or in one eye considered as myopia. Most of the time unaided near visual acuity of the myopic eye is normal or better than unaided distance acuity, hence, its popular term is “nearsightedness”.2 According to American optometric clinical practice guidelines myopia leveled as mild from −0.50 to −3.00 DS, moderate from −3.25 to −6.00 DS, and high > −6.00 DS in at least one eye.1,3 During vision screening or clinical examination myopia can be detected by major symptom (blurred distance vision), sign (reduced unaided distance visual acuity), and/or using clinical instruments like retinoscopy, autorefraction, or photorefraction.1,4 The power of the cornea, crystalline lens, and the axial length will determine the refractive status of the eye. An eye in myopic condition have an axial length too long for its optical power, or too optically powerful for its axial length.1,5
Myopia cannot be prevented totally, but it can be corrected with proper minus power eye glasses, contact lenses, or refractive surgery. The goals of correcting or managing myopia are for clear vision, comfortable and efficient binocular vision, and for good ocular health. Almost all patients with myopia can have good vision if early and appropriate correction has been given.1,4,6
The burdens of uncorrected myopia are serious especially in students. Poor vision and an inability to read material on the chalkboard due to myopia can greatly affect a student’s participation in education, different activities, and other social participations. Furthermore, when they become adults they are excluded from productive working lives, which results in severe economic and social consequences.7
Myopia is a highly significant problem, not only because of its high prevalence, but also because of it medical burden including pathologic complications such as myopic macular degeneration, choroidal neovascularization, retinal breaks and detachment, cataract, and glaucoma that contribute to visual morbidity in all ages, gender, and ethnicity.8
A person who becomes blind due to myopia at a young age suffers more years of blindness than a person becoming blind from cataract. This situation tends to place a greater socioeconomic burden on society.9
The incidence and prevalence of myopia in the world is widely vary. It is more common in Asian countries, with prevalence up to 40% in the general population.10 But relatively less common in Europe and North American countries.11,12 Its prevalence and distribution in Africa is lower than Asian and European countries.6,13 The prevalence of myopia reaches 20–25% in school age and 25–35% among the mid-to-late teenage population in the world.13 Eighty percent (80%) of mild to moderate myopia and 10% of high myopia prevalent in students aged from 16 to 18 years that attended of grade 10 and 114 classes and prevalence of myopia in university students is also high.14 The prevalence of myopia significantly declines somewhat in the population aged between 40 and 79 years old but increases in people older than 80 years old.15
Myopia has a complex trait including both genetic and environmental factors.2–4 Different studies show that doing a substantial amount of close work on a regular basis, greater academic ability, higher educational level, less time spent on outdoor activity and parental history of myopia can increase the risk for myopia.4,16 Data from many studies have also documented females and males showed similar prevalence rates of myopia. Furthermore, It was determined that with age the average refractive error among schoolchildren becomes more myopic.14,17 Studies on populations with very similar genetic backgrounds, but growing up in different environments in China, India, and Nepal have shown a clear urban–rural difference in the prevalence of myopia.7,15,18 It has been suggested that myopia occurs less frequently among students of rural than urban schools.7,19 Socioeconomic status, level and length of education, parental myopia, exposure to close work and level of intelligence are associated with myopia. Even though they are not main factors, level of lighting, stress, pharmacological agents, and amount of time spent at indoor activity has an effect on the development of myopia.1,3,19 It remains unclear if educational level is an independent risk factor or a surrogate for closeup work or some other socioeconomic characteristic.5,20–22
Ethiopia is one of the African countries with a relatively poor eye health-care service and is believed to have one of the world’s highest rates of blindness. Refractive error, remarkably myopia is the second leading cause of blindness accounting for 7.8%. Lack of awareness and recognition of the problem, nonavailability of and/or inability to afford refractive services, insufficient provision of affordable corrective lenses and cultural disincentives to compliance are factors for poor coverage for myopia correction. Hence, to overcome this problem research concerning myopia is crucial.20,23,24
Little is known about the prevalence and associated factors as well as public health importance of myopia in students in developing countries, particularly in Ethiopia. This study aims to determine the actual burden of myopia and its associated factors on high school students.
Methods and Materials
A school-based cross-sectional study design was conducted from April 24 to May 7, 2019. The study was conducted in Hawassa city, Southern Ethiopia. Hawassa city is located 273 km south of Addis Ababa (the capital city of Ethiopia). Hawassa is the capital city of both Sidama regional state and Southern nations, nationalities and peoples region having eight sub-cities and 32 kebeles. In the city there were 11 governmental and 10 private high schools which serve 18,761 and 8662 students, respectively. The total the number of students were 27,423. One governmental tertiary eye care and training center and two private higher ophthalmic clinics have been found in the study area. All high school students in Hawassa city were a source population and data were collected from selected high school students who were available during the data collection period. Students who had ocular conditions preventing refraction, recent ocular trauma, and active ocular infection were excluded from the study.
Sample size was determined using single proportion formula by taking into consideration 11.9% prevalence rate of myopia among high school students in Gondar town, North West Ethiopia.25
Where; n=sample size
Z=value of z statistic at 95% confidence interval=1.96
P=proportion of myopia taken from similar study conducted in North West Ethiopia, Gondar town is 11.9%
1-P=0.88
d=margin of error 5%=0.05, Hence

In addition, by taking a similar study conducted in Gondar town, North West Ethiopia, parental/familial myopia, ocular abnormality, school type, working distance and use of visual display units were considered as the main consistent factors for myopia and used for sample size determination.
The maximum sample size was determined by comparing results for objective one and objective two from simple proportion formula and Epi Info™ StatCalc software by considering 95%CI, 80% power, since the larger sample size was obtained from Epi Info™ StatCalc for a variable of school type which was 327. It was taken as optimum sample size that accommodates all study objectives then by considering 10% to nonresponse rate the final required sample size was 360. Stratified sampling technique was used to select study participants. The sample was taken from 30% of the total high schools in Hawassa city. There are 21 high schools, 10 private and 11 government high schools. As shown in Figure 1 six high schools were selected using simple random sampling methods among all high schools and in those selected schools there were a total of 7313 students. The number of study participants were determined by proportional allocation for each selected high schools by using: ns=n (NS/N): where ns=sample size for each selected schools, NS=number of students in each school, n=total sample size, N=the total number of students in the selected schools. Then the registration number of all students in every selected schools were merged and computer-generated simple random sampling was done to get study participants.
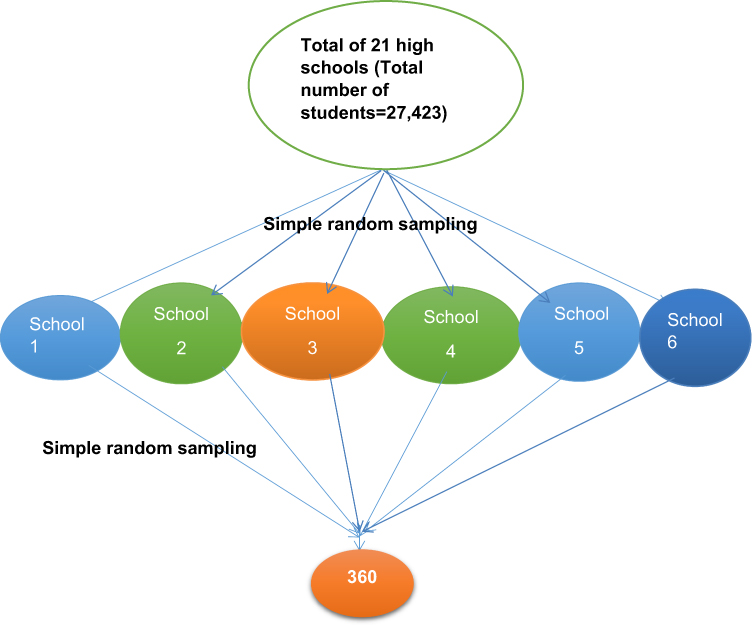 |
Figure 1 Schematic presentation of sampling procedures on prevalence and factors associated with myopia among high-school students in Hawassa city, South Ethiopia. |
Operational Definitions
Myopia
The spherical equivalent refractive error (SER) has to be ≥ −0.50 D in the poorer eye and was sub-classified as low (−0.50 to 3.00 DS), medium (−3.25 to −6.00 DS) and high (above −6.00 DS).26
Familial Myopia
First degree relatives with any degree of myopia diagnosed by eye-care professionals.
Illumination During Reading
It is considered as dim light for the reading illumination at home <60 watt lamp/fluorescent and bright light for >60 watt lamp/fluorescent.24
Working Distance
The habitual distance range at which a person adapts to do near tasks and is considered as 33–60 cm. Any working distance shorter than this is considered as close working distance.
Ocular Abnormality
Any ocular disorder (like keratoconus and other corneal ectasias, corneal degenerations and dystrophies, cataract, lens subluxation/dislocation as well as retinal disorders that can induce myopia during its course or as a consequence of the disease process determined by ocular examination.
Active Rest During Reading
Considered as “yes” when the student takes rest commonly during reading and “no” when the student takes rest occasionally or never.24
Data Collection Procedures (Instrument, Personnel)
The data were collected by trained optometrists and ophthalmic nurses with good experience of regional surveys and working on refraction service. The data regarding sociodemograpic and family related information were collected using a pretested structured questionnaire by trained ophthalmic nurses. Parental myopia was identified by asking the students about eye glasses wearing history of parents but in rare situations students, who were not sure about presence of myopia among their family member, tries to contact the family leader by cell phone directly to refine. The questionnaire was translated into Amharic version (local language) from English version and then back to English by language translator for consistency of the tool. Physical examinations data recording format was prepared for refraction and ocular examination were conducted using six-meter Snellen visual acuity test chart, pinhole, retinoscope, trial case lenses, trial frame, Jackson cross-cylinder lens and direct ophthalmoscope. Students who had visual acuity of worse than 6/9 in either eye were taken as the cutoff point and pinhole was performed to check if there is any visual acuity improvement then cycloplegic retinoscopy was done using cyclopentolate hydrochloride 1% eye drops by senior optometrists. Students who did not have pinhole visual acuity improvement and who had any other ocular abnormalities were referred to Hawassa University Referral Hospital, Ophthalmology and Optometry Department for further ophthalmic evaluation.
Data Quality Control
Pretest was done by taking 5% of the sample size, after selecting one school which was not included in the study. After the pretest necessary modifications were made accordingly. Data was collected by senior ophthalmic nurses and optometrists experienced in the study measurements and interview techniques. Training for data collectors was given. On the field work, the principal investigator closely followed the day-to-day data collection process and ensured completeness and consistency of the collected data.
Data Processing and Analysis
After coding, the data was entered into Epi Info™ version 7 and then exported and analyzed by using SPSS version 20. Frequencies, proportions and summary statistics were calculated for selected variables. Hosmer–Lemeshow test was done to check model fitness (p>0.05 taken as adequate). Bivariable and multivariate binary logistic regression was used to determine the associated factors. The variables that were found with p<0.2 in Bivariate analysis were entered to multivariate analysis. Adjusted odds ratio (AOR) with 95% confidence interval (CI) was used to show the strength of association. Those variables with p-value <0.05 were considered as statistically significant.
Ethical Consideration
Ethical clearance was obtained from Hawassa University College of Medicine and Health Sciences Institutional Review board in accordance with the Declaration of Helsinki.27 Officials at different levels, Hawassa city administrative education office and selected schools were informed through formal letters. Each participating school was visited a week before the data collection day, and permission to conduct the study was obtained. Written informed consent form was given to each of the student below 18 years to be taken to their parents or guardians the day before data collection. Only students who were duly give assent and provided signed consent forms from their parents who were willing for the students to take part in the study were recruited. Parents who required further explanation before consenting for their children to participate in the study were invited to the particular school on the data collection day. For participants who were 18 years and above, written informed consent was obtained. Participants were informed about the objective of the study and they also had the right to refuse to participate in the study. Confidentiality of the information obtained was assured through not writing their name, interviewing participants privately, and by keeping the collected information locked. Participants who were found to have myopia and any other ocular disorder, were referred and underwent full ocular examination at Hawassa University Referral Hospital.
Results
Sociodemographic Characteristics
A total of 349 students were participated in the study. The response rate was 97%. The mean age (standard deviation) of participants was 16.90 (±1.32) year. More than half of the study participants were female 190 (54.4%) and from private schools 180 (51.6%). Most of the study participant parents were accomplish secondary school 117 (33.5%) and more than one third of them were government workers 149 (42.7%) (see Table 1).
 |
Table 1 Sociodemographic Characteristics of Study Participants Among High-school Students in Hawassa City, South Ethiopia, 2019 (n=349) |
Prevalence of Myopia
Myopia was diagnosed in 56 students (16.05%) (95%CI: 12.6, 20.1). Regarding the degree of myopia, 36 (10.3%) had low degree myopia. Most participants were visual display unit users 50 (23.3%) and not using active rest during close work (see Table 2).
 |
Table 2 Proportion of Degree of Myopia, Familial Myopia, Family Member with Myopia and Ocular Abnormalities Among High-school Students in Hawassa City, South Ethiopia 2019 (n=349) |
Factors Associated with Myopia
Bivariate Analysis
According to bivariable analysis female sex, early age of schooling, positive parental history, lack of outdoor sport activities, short working distance, longer time spent for close work, not taking active rest during studying, dim illumination, use of visual display units, and abnormal ocular findings were significantly associated with myopia (see Table 3).
 |
Table 3 Associated Factors in Bivariate Analysis of Myopia Among High-school Students, Hawassa City, South Ethiopia 2019 (n=349) |
Multivariate Analysis
All independent variables who were associated with myopia in the bivariate analysis were selected for multivariate analysis. In the multivariate analysis early age of schooling (AOR=3.14; 95%CI: 1.16, 10.06), positive family history for myopia (AOR=8.46; 95%CI: 7.11, 12.08), prolonged near work (AOR=11.65; 95%CI: 2.11, 64.5), short working distance (AOR=10.90; 95%CI: 0.57, 20.55), lack of outdoor sport activities (AOR=7.37; 95%CI: 2.71, 20.03) and use of visual display units (AOR=8.36; 95%CI: 2.39, 29.33) were found to be independently associated with myopia (see Table 4).
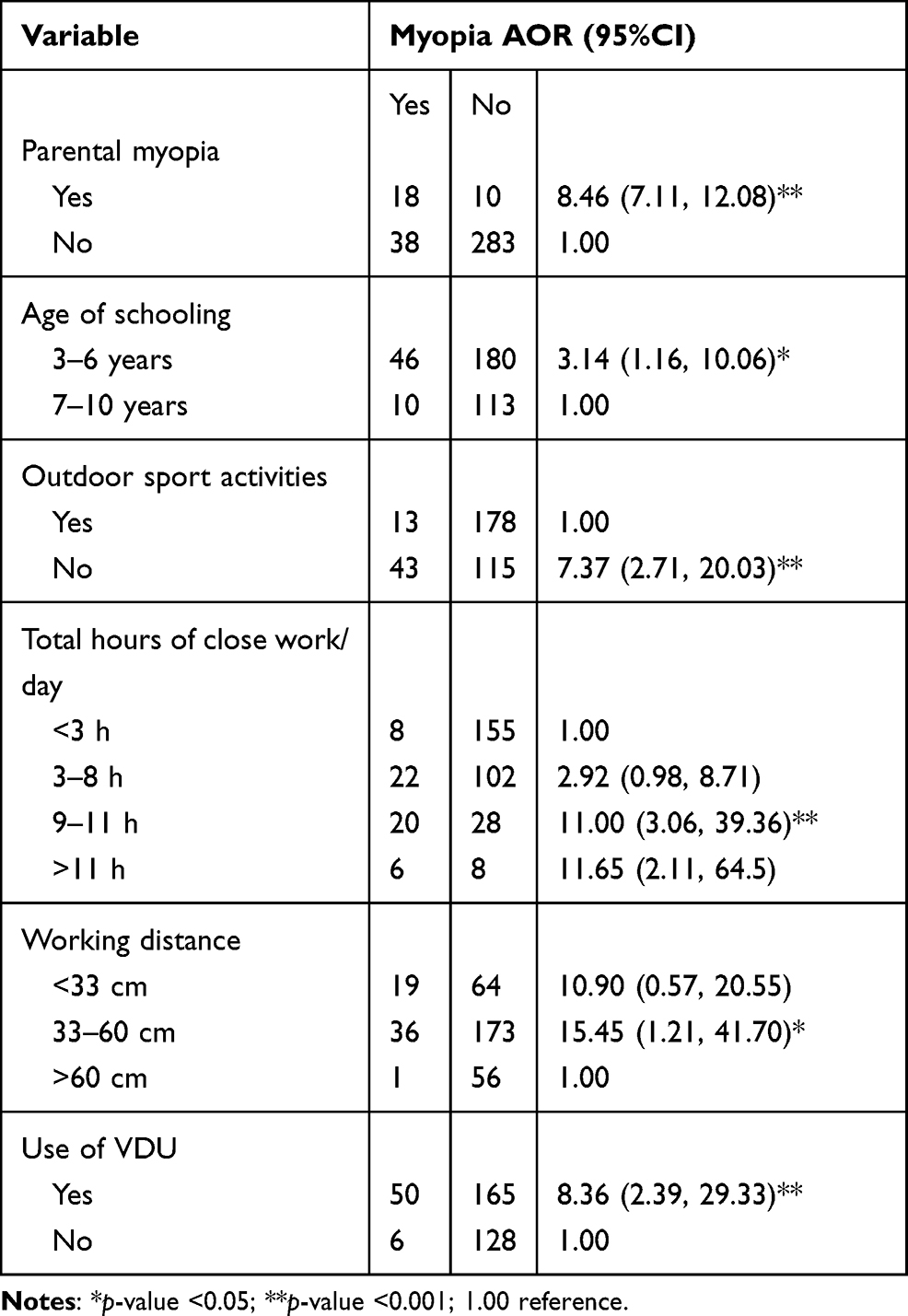 |
Table 4 Factors Associated with Myopia Among High-school Students, Hawassa City, South Ethiopia 2019 (n=349) |
Discussion
In this study the prevalence of myopia was 56(16.05%) (95%CI: 12.6, 20.1). This finding is similar to other studies conducted in Australia (17%),2 Poland (13.3%),18 and Amman city (17.6%).28 Whereas, compared to studies done in Ethiopia (11.9%), Tanzania (5.59%), and Nigeria (2.9%)23,25,29 this study finding is larger. This discrepancy might be due to there being an increment of using visual display units among students relating with technological advancement showing increased myopia rates with surrogated environmental factors. In contrast, the prevalence of myopia in this study is relatively lower than other studies done in America (53.4%), South Korea (96.54%), Hong Kong (87%), China (80.7%), Shanghai (95.5%), Taiwan (86.1%), India (19.1%), Israel (20.3%), and Ghana 28.9%.2,12–15,21,30 This difference might be due to the variation in race between the study participants and Asian descent. Most Asian nations were more myopic as a result of a complex genetic trait responsible for myopia.1,5 In addition, due to different environmental factors that may influence the occurrence and development of myopia relating to fast advancement of technology in developed nations, students were subjected for excessive near tasks.
In this study students who had positive family history of myopia were 8.46 times more likely to develop myopia compared to those who had no family history of myopia. Studies conducted in Beijing,4 Hong Kong,31 Singapore,19 Taiwan military conscript,32 and Ethiopia25 agree with this study finding. Parental myopia was considered as a marker for both genes and a shared family environmental exposure. Myopic parents are more likely to have intensive education or less time spent outdoors and it was also suggested that children with myopic parents have a longer axial length than those without myopic parents.
Those study participants who use short working distance during close work were more likely to be myopic than those using working distance greater than 60cm. This result is in line with other studies done in Norway,33 China,3 Vietnam,9 and Ethiopia.25 This may point to the fact that persistent short working distance leads to peripheral blurred retinal image occurring during ciliary spasm that comes after prolonged near focus then a biochemical process is initiated within the retina, sclera and choroid that lead to axial elongation.30
Students who spent a total of 9–11 hours/day in close work become myopic 11 times more than students who spent less than three hours/day. This study result goes in line with results found in Beijing, Singapore, and Taiwan military conscripts, Amman city and also Ethiopia.3,8,24,25,32 Close-up work, such as reading, writing, computer work, and close television viewing encompasses tasks of high accommodative demand that increase pressure in the posterior part of the eye and increase ocular length.
Those study participants who were not doing outdoor sport activities had seven times increased odds of becoming myopic. This agrees with studies done in Taiwan,17 Ohio State University, USA,22 and Jordan.34 It may be explained in a way that, by nature most outdoor sport activities do not need any near focusing and accommodation and are performed under natural illumination in contrast to those who did not do outdoor sport activities.8 In addition, inhibitor effects on ocular growth found that outdoor sports activities seemed to cause little change in choroidal blood flow.32
Students who used visually display units increase the odds of becoming myopic by 8.36 times when compared to nonusers. Studies conducted in Victoria, Australia,2 Beijing24 and Ethiopia25 also confirmed the effect of VDUs on myopia. The most likely reason for this association is connected with near work.24
This study indicated schooling below six years old increased myopia occurrence three times than students schooling seven-to-ten years old. This result is confirmed by studies done in Greece6 and Norway.33 Exposure to a more intensive schooling system at an early age may be an independent risk factor for myopia which could disturb the optical integrity of the eye, either the curvature or the axial length, because daily growth patterns in normal eyes especially in children, whose ocular development has not ceased seem to be regulated by an endogenous circadian oscillator. During early schooling age this process could not control the growth pattern and results in increasing of axial length.19
Limitations
Some students may have mild myopia even if their visual acuity is 6/9, this may cause slight underestimation of the prevalence of myopia. Conversely, 95%CI may be large for some variables like prolonged close work and VDU usage.
Conclusion
The prevalence of myopia among Hawassa City High School students was 16.5%. Early age of schooling, parents being myopic, prolonged close work, short working distance, lack of outdoor sport activities, and use of visual display units were variables positively associated with myopia.
Acknowledgment
The authors would like to thank the study participants for their active participation and cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goss DA, Grosvenor TP, Keller JT, Marsh-Tootle W, Norton TT, Zadnik K. Optometric clinical practice guideline: care of the patient with myopia. American Optometric Association; 1997. Available from: https://www.aoa.org/AOA/Documents/practice%20Management/Clinical%20Guidelines/Consensus-based%20guidelines/Care%20of%20patient%20with%20myopia.pdf. Accessed March 6, 2022.
2. Wensor M, McCarty CA, Taylor HR. Prevalence and risk factors of myopia in Victoria, Australia. Arch Ophthalmol. 1999;117(5):658–663. doi:10.1001/archopht.117.5.658
3. French AN, Morgan IG, Mitchell P, Rose KA. Risk factors for incident myopia in Australian schoolchildren: the Sydney adolescent vascular and eye study. Ophthalmology. 2013;120(10):2100–2108. doi:10.1016/j.ophtha.2013.02.035
4. Wu LJ, You QS, Duan JL, et al. Prevalence and associated factors of myopia in high-school students in Beijing. PLoS One. 2015;10(3):e0120764.
5. Konstantopoulos A, Yadegarfar G, Elgohary M. Near work, education, family history, and myopia in Greek conscripts. Eye. 2008;22(4):542–546. doi:10.1038/sj.eye.6702693
6. Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiological Optics. 2012;32(1):03–16.
7. Congdon N, Wang Y, Song Y, et al. Visual disability, visual function, and myopia among rural Chinese secondary school children: the Xichang pediatric refractive error study (X-PRES)—report 1. Invest Ophthalmol Vis Sci. 2011;49(7):2888–2894. doi:10.1167/iovs.07-1160
8. Saw SM, Gazzard G, Shih‐Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic Physiological Optics. 2013;25(5):381–391. doi:10.1111/j.1475-1313.2005.00298.x
9. Paudel P, Ramson P, Naduvilath T, et al. Prevalence of vision impairment and refractive error in school children in Ba Ria–Vung Tau province, Vietnam. Clin Experiment Ophthalmol. 2014;42(3):217–226. doi:10.1111/ceo.12273
10. Pei-Chang W, Huang H-M, Hun-Ju Y. Epidemiology of myopia. Asia-Pacific J Ophthalmol. 2016;5(6):386–393. doi:10.1097/APO.0000000000000236
11. Williams KM, Bertelsen G, Cumberland P, et al. Increasing prevalence of myopia in europe and the impact of education. Ophthalmology. 2015;122(7):1489–1497. doi:10.1016/j.ophtha.2015.03.018
12. Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32(1):3–16. doi:10.1111/j.1475-1313.2011.00884.x
13. Dayan YB, Levin A, Morad Y, et al. The changing prevalence of myopia in young adults: a 13-year series of population-based prevalence surveys. Invest Ophthalmol Vis Sci. 2015;46(8):2760–2765. doi:10.1167/iovs.04-0260
14. Sun J, Zhou J, Zhao P, et al. High prevalence of myopia and high myopia in 5060 Chinese university students in Shanghai. Investigative Opthalmol Visual Sci. 2012;53(12):7504–7509. doi:10.1167/iovs.11-8343
15. Joseph N, Nelliyanil M, Rekha T, Rai S, Kotian SM. Proportion of refractive error and its associated factors among high school students in South India. Br J Med Med Res. 2015;11(11):1–9. doi:10.9734/BJMMR/2016/20798
16. Xie Z, Long Y, Wang J, Li Q, Zhang Q. Prevalence of myopia and associated risk factors among primary students in Chongqing: multilevel modeling. BMC Ophthalmol. 2020;20(1):146. doi:10.1186/s12886-020-01410-3
17. Lin L, Shih Y, Hsiao C, Chen C. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2016;33(1):27–33.
18. Czepita D, Żejmo M, Mojsa A. Prevalence of myopia and hyperopia in a population of Polish schoolchildren. Ophthalmic Physiological Optics. 2007;27(1):60–65. doi:10.1111/j.1475-1313.2006.00419.x
19. Saw SM, Wu HM, Seet B, et al. Academic achievement, close up work parameters, and myopia in Singapore military conscripts. Br J Ophthalmol. 2001;85(7):855–860. doi:10.1136/bjo.85.7.855
20. Woldeyes A, Misganaw C. Prevalence and factors associated with refractive error among primary school children in Addis Ababa, Ethiopia. Int J Med Health Sci Res. 2014;1:92–104.
21. Jung SK, Lee JH, Kakizaki H, Jee D. Prevalence of Myopia and its association with body stature and educational level in 19-year-old male conscripts in seoul, south korea prevalence on myopia in young males in Korea. Invest Ophthalmol Vis Sci. 2012;53(9):5579–5583. doi:10.1167/iovs.12-10106
22. Sherwin JC, Reacher MH, Keogh RH, Khawaja AP, Mackey DA, Foster PJ. The association between time spent outdoors and myopia in children and adolescents: a systematic review and meta-analysis. Ophthalmology. 2012;119(10):2141–2151. doi:10.1016/j.ophtha.2012.04.020
23. Balarabe AH, Adamu I, Abubakar A. Vision screening to detect refractive errors in three selected secondary schools in Birnin Kebbi, North West, Nigeria. Sahel Med J. 2015;18(2):61. doi:10.4103/1118-8561.160799
24. You QS, Wu LJ, Duan JL, et al. Factors associated with myopia in school children in China: the Beijing childhood eye study. PLoS One. 2012;7(12):e52668. doi:10.1371/journal.pone.0052668
25. Belete GT, Anbesse DH, Tsegaye AT, Hussen MS. Prevalence and associated factors of myopia among high school students in Gondar town, northwest Ethiopia, 2016. Clinical Optometry. 2017;9:11–18. doi:10.2147/OPTO.S120485
26. Flitcroft DI, He M, Jonas JB, et al. IMI - defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20–M30. doi:10.1167/iovs.18-25957
27. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
28. Khader YS, Batayha WQ, Abdul-Aziz SM, Al-Shiekh-Khalil MI. Prevalence and risk indicators of myopia among schoolchildren in Amman, Jordan. East Mediterr Health J. 2006;12(3–4):434–439.
29. Wedner S, Ross D, Todd J, Anemona A, Balira R, Foster A. Myopia in secondary school students in Mwanza City, Tanzania: the need for a national screening programme. Br J Ophthalmol. 2012;86(11):1200–1206. doi:10.1136/bjo.86.11.1200
30. Nakua E, Otupiri E, Owusu-Dabo E, Dzomeku V, Otu-Danquah K, Anderson M. Prevalence of refractive errors among junior high school students in the Ejisu Juaben municipality of Ghana. J Sci Technol. 2015;35(1):52–62. doi:10.4314/just.v35i1.5
31. Lam CSY, Goldschmidt E, Edwards MH. Prevalence of myopia in local and international schools in Hong Kong. Optometry Vision Sci. 2004;81(5):317–322. doi:10.1097/01.opx.0000134905.98403.18
32. Lee YY, Lo CT, Sheu SJ, Lin JL. What factors are associated with myopia in young adults? A survey study in taiwan military conscriptsfactors associated with myopia in young adults. Invest Ophthalmol Vis Sci. 2013;54(2):1026–1033. doi:10.1167/iovs.12-10480
33. Kinge B, Midelfart A, Jacobsen G, Rystad J. The influence of near‐work on development of myopia among university students. A three‐year longitudinal study among engineering students in Norway. Acta Ophthalmologica Scandinavica. 2016;78(1):26–29. doi:10.1034/j.1600-0420.2000.078001026.x
34. Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci. 2017;48(8):3524–3532. doi:10.1167/iovs.06-1118
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.