Back to Journals » International Journal of Women's Health » Volume 17
Prevalence and Factors Associated With Antepartum Depression Among Pregnant Women in Latent Labor: A Multi-Facility Cross-Sectional Study in Rural Southwestern Uganda
Authors Atuhaire C ![]() , Taseera K, Atwine D, Maling S, Patel V
, Taseera K, Atwine D, Maling S, Patel V
Received 24 November 2024
Accepted for publication 18 March 2025
Published 25 March 2025 Volume 2025:17 Pages 903—912
DOI https://doi.org/10.2147/IJWH.S508301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Catherine Atuhaire,1 Kabanda Taseera,1 Daniel Atwine,2 Samuel Maling,1 Vikram Patel3
1Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2Department of Clinical Research, Soar Research Foundation, Mbarara, Uganda; 3Department of Global Health and Social Medicine, Harvard Medical School, Boston, MA, USA
Correspondence: Catherine Atuhaire, Email [email protected]
Background: Despite limited studies on antepartum depression (APD) in Sub-Saharan Africa (SSA), it is suggested that the prevalence on the continent may be higher than the global average. This study aimed at determining the prevalence of APD and identifying its associated factors among pregnant women in latent labor in rural south western Uganda.
Methods: The findings in this manuscript were part of a prospective cohort that aimed at investigating Social Support and Perinatal Depression among women in latent labor through six weeks postpartum. We conducted a multi-facility study enrolling women in latent labor to assess for APD and its associated factors from November 2023 to March 2024. The study was carried out in three health facilities in Mbarara District, rural southwestern Uganda. The prevalence of APD based on the Mini International Psychiatric Interview (M.I.N.I 7.0.2) using the depression module. Factors associated with APD were analyzed using bivariate and multivariate logistic regression. Variables with a p-value < 0.2 in bivariate analysis were included in the multivariable model, with statistical significance set at p< 0.05. Odds ratios (OR) and 95% confidence intervals (CI) were reported. Data were analyzed using STATA software version 14.0.
Results: Of the 448 enrolled participants, 37 had APD giving a prevalence of 8.2% (95% CI: 6.0– 11.2%). Factors that were significantly associated with APD were Maternal age 30– 49 years, bad health status before pregnancy, not happy about being pregnant, having had complications during pregnancy and having a history of stressful life events during pregnancy.
Conclusion: This study reveals a very significant yet comparatively lower prevalence of antepartum depression among pregnant women in latent labor in rural southwestern Uganda. These insights highlight the persistent need for comprehensive mental health strategies especially the non-pharmacological approaches within antenatal care to enhance maternal and child health outcomes.
Keywords: antepartum depression, pregnant women, latent labor
Background
The World Health Organization (WHO) defines Antepartum Depression (APD) as a non-psychotic mood disorder occurring during pregnancy, characterized by diminished interest or pleasure in most activities, significant weight loss, disrupted sleep, fatigue, reduced appetite, feelings of hopelessness, lowered self-esteem, and impaired concentration.1 APD is usually overlooked as the symptoms are often similar to the somatic experiences associated with pregnancy.2
Globally, over 10% of pregnant women experience APD.3 In sub-Saharan Africa, the prevalence of APD is 26.3%4 while it ranges from 19% to 27% in Uganda.5,6 APD disrupts women’s daily activities, their bio-social adaptation to pregnancy, and overall functioning, while also affecting their relationships with spouses, family, and the wider community.7 Over 75% of people in low- and middle-income countries (LMICs) lack access to pharmacological and non-pharmacological treatment of depression8 despite APD in LMIC ranging from 12 to 42%.9 Pregnancy, as a major life event, involves considerable hormonal changes and increased emotional vulnerability, making it a critical period for the development of APD.
APD is associated with a variety of factors categorized into sociodemographic, obstetric, lifestyle, and psychosocial domains. Sociodemographic factors include advancing age, low socioeconomic status, low educational level, and unemployment.10 Obstetric factors encompass miscarriages, unintended pregnancies, preeclampsia, preterm deliveries, male gender preference for the unborn child, and a history of abortion.7,11,12 Lifestyle factors such as poor nutrition, partner alcohol use, and unhealthy habits like substance abuse and smoking also contribute to APD.7 Psychosocial factors include marital discord, intimate partner violence (IPV), lack of emotional support, and life stress.13,14
The economic and health impacts of APD are substantial. In the United Kingdom, APD contributes to an estimated 8.1 billion pounds in healthcare costs.4 Additionally, APD is linked to poor compliance with antenatal care, insomnia, and an increased risk of suicide.15,16 Women with APD are also at higher risk of developing postpartum depression (PPD), with rates ranging from 21% to 37% among those followed from the antenatal period to postpartum.17–19
Untreated APD can lead to adverse maternal and neonatal outcomes, including premature birth, low birth weight, respiratory conditions, and impaired mother-infant interactions.20 Despite the growing recognition of mental health issues during pregnancy, there remains a paucity of data in SSA and specifically in Uganda. Studying APD in the latent phase of labor is essential for improving maternal mental health care and optimizing labor outcomes, as it may be a strong predictor of PPD. WHO highlights the need to integrate mental health care into existing maternal health programs to improve overall health outcomes.20 This study determined the prevalence and associated factors of antepartum depression among pregnant women in latent labor in rural southwestern Uganda, to address this critical gap in knowledge.
Methods
Study Design
The findings in this manuscript were part of a prospective cohort that aimed at investigating Perceived Maternal Social Support and Perinatal Depression among women from latent labor to six weeks postpartum. We conducted a multi-facility cross-sectional study design using quantitative approach to assess antepartum depression among pregnant women in latent labor between 29th November 2023 and 20th March 2024.
Study Setting
This study was conducted in three health facilities in Mbarara district, rural southwestern Uganda: Mbarara Regional Referral Hospital (MRRH), Bwizibwera Health Center IV (BHC IV), and Mbarara Municipal Health Center IV (MMHC IV).
MRRH is a government-owned referral and teaching hospital associated with Mbarara University of Science and Technology. Founded in 1940, it has a capacity of 600 beds and handles about 1200 to 1500 patients daily. The hospital serves a catchment population of over four million across 12 districts, including Mbarara district, with an average monthly attendance of 400 pregnant women at its antenatal clinic. BHC IV, located in a suburban area, serves the rural community of Kashari county. It has eight midwives and a daily attendance of approximately 15 mothers. In the past six months, about 300 pregnant women visited BHC IV. MMHC IV is situated in Mbarara city and has three nursing staff in its antenatal clinic, with an average monthly attendance of 200 pregnant women.
Participants and Period
We enrolled 512 pregnant women in their third trimester, admitted in latent labour at the selected health facilities. Participants were recruited consecutively as they visited the facilities.
Sample Size Calculation
We estimated a sample size of 512 pregnant women using the formula for estimation of single population proportion, n = Zα/2 2 *P (1 - P)/r221 to estimate a prevalence of APD as high as 50%, which is an arbitrary value given the lack of a comparable study in our context with assumptions of Zα/2 of 1.96, margin error (r) of estimation of 5% (0.05) and a predicted 25% non- response rate and missing data.
Sampling Procedure
We used proportionate stratified sampling method, to determine the sample size for each of the three sites. Pregnant women within each site were selected consecutively based on eligibility criteria until the sample size of 512 was attained. This was based on the number of women that had given birth in each health facility the previous 6 months (hospital records).
Variable Definitions
The primary outcome was antepartum depression, diagnosed using the Mini International Psychiatric Interview (M.I.N.I 7.0.2) based on DSM-5 criteria using the depression module. This is a structured diagnostic interview used to assess Major Depressive Disorder during pregnancy (APD). The MINI 7.0.2 is a reliable and valid tool for diagnosing antepartum depression, with strong inter-rater and test-retest reliability in diverse populations.22 APD was recorded as a binary variable (0 for absent, 1 for present). Independent variables included socio-demographic characteristics, maternal obstetric and medical factors, baby factors, and social support factors.
Social support is support respondents receive from spouses, family members, and friends. This was measured by the Maternal Social Support Scale (MSSS).23 This validated tool measures perceived social support. Participants are asked the extent of support from their significant others’ on a 5-point Likert scale, where 1 is never and 5 always. Scoring for two items is reversed. Scores range from 0 to 30, categorized as low (0–18), medium (19–24) and adequate (>24) (23). Cronbach’s alpha value for this tool was documented as between 0.71 and 0.90 when applied to Syrian women in Jordan.24
Occupation was referred to as how people earned a living, ranging from being unemployed to being employed as a professional or laborer according to Uganda Bureau of Statistics.25
Education was classified as Primary or no education which means basic literacy and numeracy knowledge typically for children less than 12 years, secondary means acquisition of advanced literacy, science, social studies, and vocational skills typically for teenagers below 19 years and tertiary encompasses both academic and vocational level of education in adults.26
Stressful life events were measured using the Perceived Stress Scale-10 (PSS-10). This is a 10 item valid and reliable widely used psychological tool for measuring an individual’s perception of stress over the past month, with responses on a 5-point Likert scale.27
Data Collection Procedure
After consent and enrollment of eligible pregnant women in each site, they were first subjected to the questionnaire by the study graduate nurses and midwives. All the participants were then moved to another private room where they were clinically examined by a psychiatrist or an experienced registered mental health clinician using a MINI to establish presence or absence of APD. Latent labor in this study was defined as a stage when a pregnant woman had mild, irregular and shorter in duration contractions with the cervix effacing up to 4 centimeters before progressing to active labor.28 Data were collected in a private setting within the facility.
Data Analysis
Data was entered into a database designed with KOBO Collect software, cleaned and verified. The dataset was imported into STATA© 14.0 software (College Station, Texas, USA) for analysis. Participants’ characteristics were described using means or medians for continuous variables and proportions for categorical variables and presented in a table.
Prevalence of APD was calculated by dividing the number of diagnosed cases by the total number of participants screened. Factors associated with APD were analyzed using bivariate and multivariable logistic regression. Variables with a p-value <0.2 in bivariate analysis were considered in the multivariable model building. This aimed at ensuring that potentially significant predictors were included while avoiding the exclusion of variables that could confound the relationship or have meaningful associations with the outcome variable (APD).29 A manual back-ward stepwise selection method was used in establishing the final multivariable analysis model with factors that bore an independent significant association with APD with a significance threshold set at p<0.05. Both unadjusted and adjusted Odds ratios and 95% confidence intervals were reported.
Results
We enrolled a total of 512 women in their 3rd trimester attending three health facilities between 29th November 2023 and 20th March 2024.
Participant Characteristics
Of the 512 women enrolled, 448 women who had complete data on all selected variables were included in the analysis. Missing data arose from incompletely filled questionnaires by the interviewers in the selected health facilities. These were distributed across the 3 study sites, that is, Mbarara Regional Referral Hospital (n=226; 50.5%), Bwizibwera Health Centre IV (n= 127; 28.4%), and Mbarara Municipal Council Health Centre IV (n=95; 21.2%). The mean age of the participants was 26.6 ± 5.6 years, with the majority being between 10–29 years (71.2%), married (96.2%). More than half had at least a secondary level of education (54.7%) and were unemployed (52.2%) (Table 1).
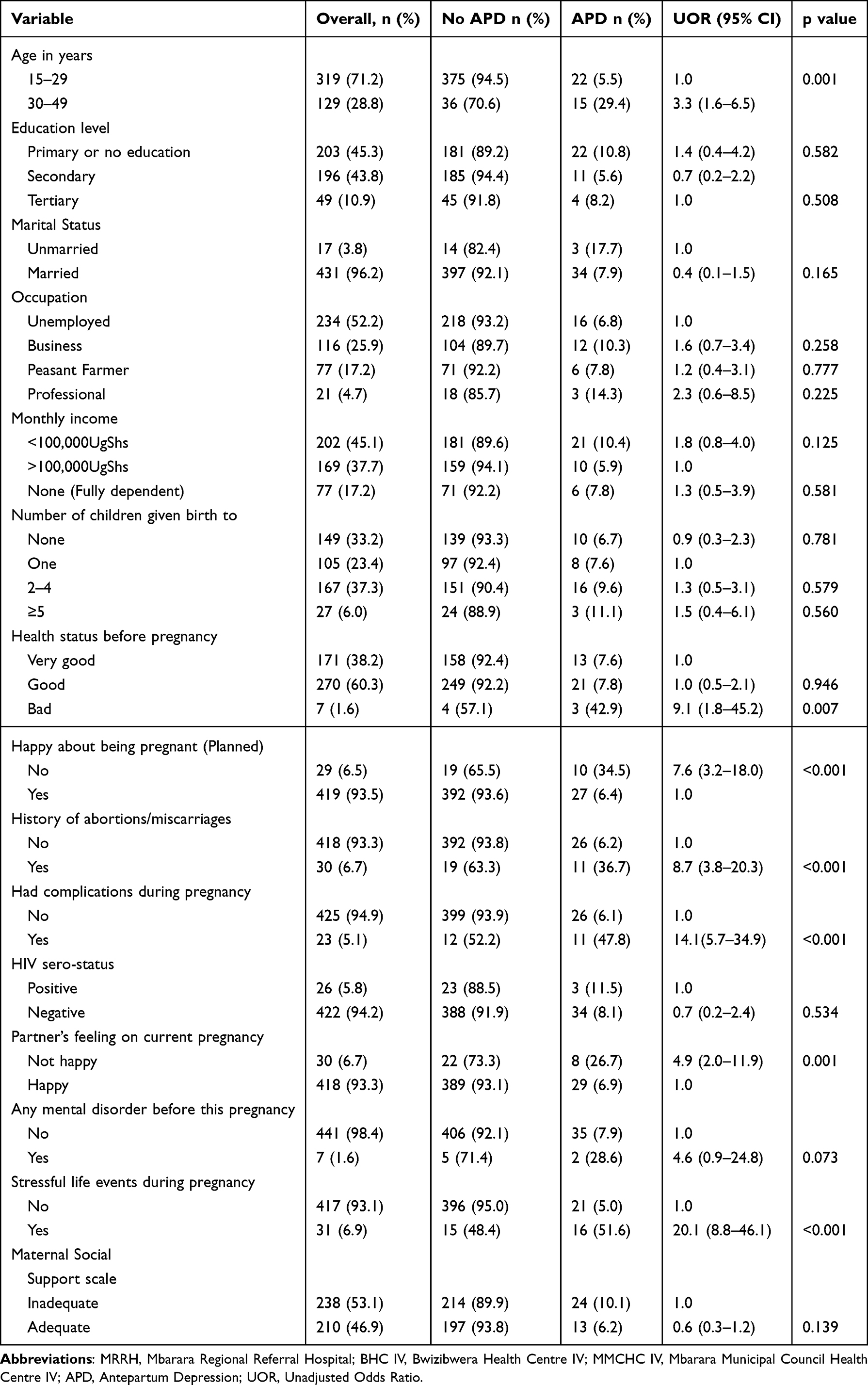 |
Table 1 Results for Bivariate Analysis for Sociodemographic and Obstetric Factors Associated With Antepartum Depression in Rural South-Western Uganda |
Two-thirds of the mothers (66.8%) had previously given birth. Nearly all participants (98.4%) reported good health status prior to the current pregnancy. Most pregnancies were planned (82.1%), with 93.5% expressing happiness about their pregnancy and 94.2% being HIV negative (Table 1).
Partner satisfaction with the pregnancy was high, with 93.3% of the partners reported as happy. Most participants felt well-supported by their partners regarding the health of the fetus and continuation of the pregnancy (91.5%), were happy with their marriage (88.6%), and satisfied about the social support received from friends and family (85.3%). (Table 1).
Prevalence of Antepartum Depression (APD)
Of the 448 enrolled participants, 37 had APD giving a prevalence of 8.2% (95% CI: 6.0–11.2%). On stratification across maternal age groups, the prevalence of APD was significantly higher among those aged 30–49 years (15.5%; 95% CI: 10.2–22.9) as compared to those aged 10–29 years (5.3%; 95% CI: 3.3–8.4), p<0.001.
Factors Associated With Antepartum Depression
In bivariate analysis, the following factors showed a statistically significant association with APD: age of mother, reporting bad health status before pregnancy, being happy about being pregnant, having a history of abortions or miscarriages, reporting having suffered complications during pregnancy, Partner feeling unhappy about the current pregnancy, poor Partner’s support to the health of the fetus and continuation of the pregnancy, not being escorted to hospital by Spouse, being unhappy with their marriage, low satisfaction towards social support received from friends/family during pregnancy, Gender based abuse/violence by partner, and having history of stressful life events during pregnancy, p<0.05.
These were considered in the establishing of a multiple logistic model using a manual backward stepwise elimination method (Table 1).
Multivariable Regression Analysis
In the final model, five variables demonstrated statistically significant predictive values for APD. These were maternal age of 30–49 years (AOR= 4.2; 95% CI: 1.8–10.0, p=0.001), bad health status before pregnancy (AOR=10.0; 95% CI: 1.3–74.8, p=0.025), not happy about being pregnant (AOR=4.9; 95% CI: 1.5–16.2, p=0.010), having had complications during pregnancy (AOR=9.0; 95% CI: 2.7–30.4, p<0.001) and having a history of stressful life events during pregnancy (AOR= 17.4; 95% CI: 6.4–47.3, p<0.001) (Table 2).
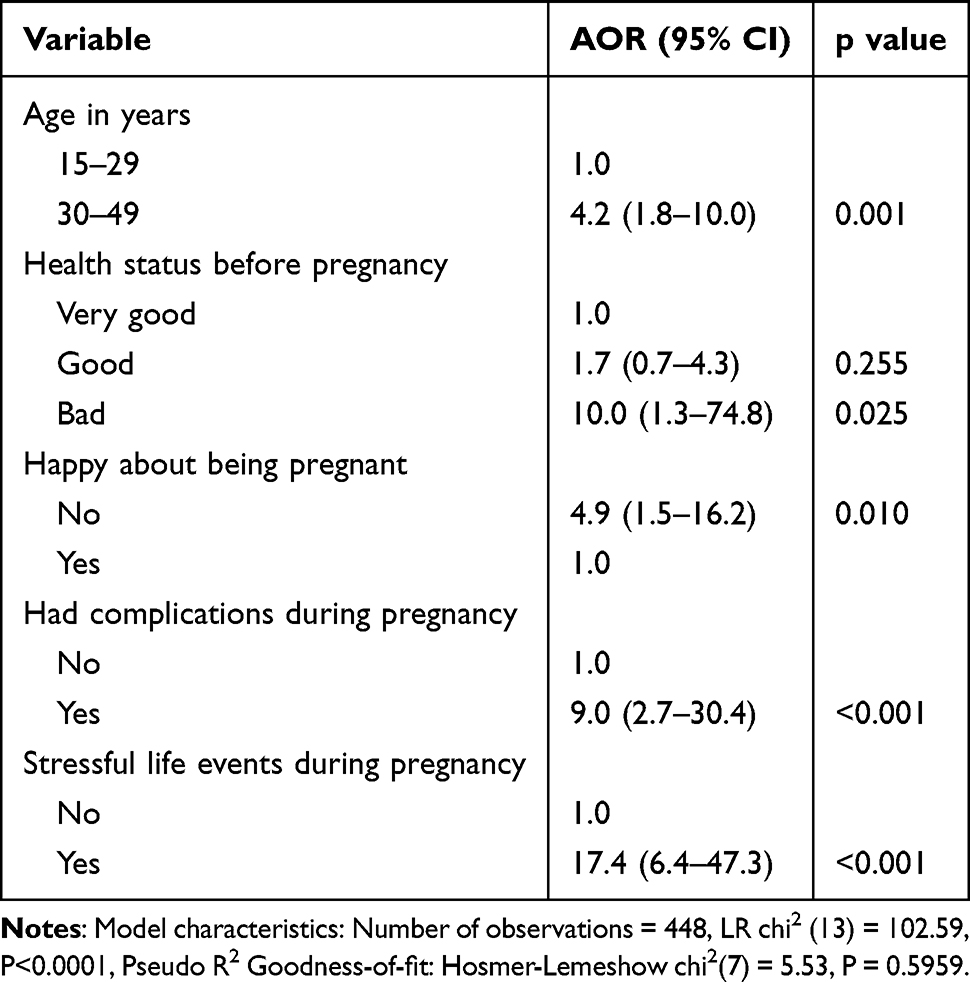 |
Table 2 Results for Multivariable Analysis for Factors Associated With Antepartum Depression in Rural South Western Uganda |
Discussion
This study aimed at determining the prevalence of antepartum depression among pregnant women in latent labor in rural southwestern Uganda and identifying factors influencing its occurrence. Our study found a prevalence of APD at 8.2% (95% CI: 6.0–11.2%) and further highlighted five variables that significantly contributed to APD among mothers in latent labor and these included, maternal age, bad health status before pregnancy, not being happy about being pregnant, having had complications during pregnancy, and having a history of stressful life events during pregnancy. This is within the range of APD for LMICs30 as well as other African countries like Nigeria,7 Tanzania,31 rural central32 and southwestern Uganda.33 It is, however, significantly lower than the prevalence rate reported in a systematic review that was carried out in Sub-Saharan Africa4 and Uganda’s other rural regions (37.7%).34 The variance between our study and the other studies can be attributed to the variations in sample sizes, tools used to measure APD, using a screening tool as a diagnostic tool without validation, timing of the postpartum period, regional and socio-cultural differences. For example, studies employing screening tools like Patient Health Questionnaire 9 (PHQ-9) to assess depression often yield higher prevalence rates, as it may capture a wider range of depressive symptoms without stringent diagnostic criteria,35 as seen in a cross-sectional study carried out in Mubende, Uganda, where women were assessed and the prevalence of APD was determined using a PHQ-9 and DSM-IV to confirm depression.34 In contrast, the M.I.N.I, which relies on DSM-5 criteria provides a more rigorous APD diagnosis likely contributing to the lower prevalence observed here.
The regional differences may also arise from varied social support levels, healthcare access, and awareness. Rural areas often lack mental health resources, which could mean that women experiencing milder symptoms may not identify or report them. In comparison, urban areas with more robust healthcare and mental health programs may yield higher APD rates, as awareness and screening are more prevalent.6 Preferred non-pharmacological treatments for APD focus on psychotherapy, lifestyle changes, social support, complementary therapies, vagus nerve stimulation among others. Pharmacological treatments use requires a careful risk-benefit analysis to ensure maternal well-being while minimizing fetal risks.36
The study further highlighted five variables that significantly contributed to APD among mothers in latent labor and these included, maternal age, bad health status before pregnancy, not being happy about being pregnant, having had complications during pregnancy, and having a history of stressful life events during pregnancy. Women aged 30 to 49 years are significantly more likely to experience APD. This finding is consistent with global studies that suggest that older mothers face unique stressors, such as increased caregiving responsibilities, economic pressures, and potential comorbid health conditions.19 These challenges can amplify emotional vulnerability, especially when healthcare resources are limited. Moreover, women in this age group regularly juggle family responsibilities alongside their pregnancies, which can further increase the risk of depression. This pattern is reflected in various LMICs studies.4
Additionally, the study highlights a significant connection between poor pre-pregnancy health and postpartum depression. This finding aligns with existing literature that suggests physical health issues like hypertension, diabetes, mental illness and many more can worsen psychological distress during pregnancy, particularly in rural LMICs where women have limited access to healthcare interventions.10 Pre-existing health issues may also affect women’s perception of pregnancy as a risky endeavor increasing their vulnerability to depressive symptoms in pregnancy.
The odds of having APD were 5 times higher among women who expressed unhappiness with their pregnancy as compared to those who expressed happiness with their pregnancy and this was consistent with findings from other studies.7 The unexpected or unwanted nature of a pregnancy can heighten mental distress, specifically in situations where social support may depend on the pregnancy being accepted by partners or family members,37 this is very common among young or teenage mothers. The social expectations placed on women in these circumstances often add a layer of pressure, compounding feelings of helplessness hence increasing the likelihood of suffering from APD.
Pregnancy complications were a substantial predictor of APD, reflecting the heightened emotional and physical strain these conditions impose on the women diagnosed with the condition during the antenatal period. Complications such as gestational hypertension, diabetes, or pre-eclampsia not only increase medical risks but also contribute to increased anxiety and worry, creating fertile grounds for depressive symptoms in the pregnant mothers.38 These results highlight the obligation for focused mental health support for women having high-risk pregnancies.
The most pronounced factor was the history of stressful life events during pregnancy, aligns with extensive evidence from studies worldwide.39 In rural Ugandan contexts, such events may include financial instability, intimate partner violence,40 or familial conflicts. This extreme vulnerability suggests a recurring relationship where external stressors aggravate APD symptoms, further complicating the pregnancy experience even when they are in labor. It also points to a critical area where interventions could allay APD risk by addressing external stressors, through counseling, financial aid, or social support programs.
In a nutshell, the study’s findings resonate with broader SSA and global research indicating that APD associated factors are often intertwined with sociodemographic and psychosocial dynamics, especially in LMICs.7,15 Differences in prevalence rates between this and other studies are most likely due to factors like methodological variations, cultural differences in mental health stigma, and the depth of mental health resources available to pregnant women.
Most research on APD focuses on early pregnancy or postpartum outcomes, while mental health research during labor remains limited.41 Studying APD in the latent phase of labor helps bridge this knowledge gap, as depression during this phase may be a strong predictor of PPD. Early identification and support for women experiencing APD could play a crucial role in preventing or managing PPD, ultimately improving maternal mental health outcomes.
Recommendations
To address antepartum depression effectively, mental health services should be integrated into the antenatal care package with regular screenings and training for healthcare providers, especially midwives, and nurses, to recognize it in high-risk groups as a health promotion measure. Community awareness initiatives involving both men and women can reduce stigma, intimate partner violence, and unplanned pregnancies and build supportive networks, while engaging male partners may lessen stress-related depressive symptoms.
Establishing psychosocial support systems in pregnancy, like peer counseling and financial aid programs, would alleviate stressors coupled with social and economic challenges, particularly for women facing unplanned pregnancies or complications. At the policy level, there’s a need to advocate for mandatory APD screenings, availing validated tools for screening and inclusion in national guidelines can ensure consistent, quality mental health support across all maternal healthcare settings.
Finally, Community-based interventions play a critical role in addressing APD by providing social support, emotional care, economic empowerment and culturally appropriate care at the community level. Strengthening these initiatives enhances maternal mental health outcomes and overall pregnancy well-being.
Conclusion
This study reveals a very significant yet comparatively lower prevalence of antepartum depression among pregnant women in latent labor in rural southwestern Uganda. The findings identify key factors associated with APD, such as advanced maternal age, poor health before pregnancy, unintended pregnancies, complications during pregnancy, and the experience of stress while pregnant. These insights highlight the persistent need for comprehensive mental health strategies within antenatal care to enhance maternal and child health outcomes. To reduce the impact of antepartum depression on mothers and their newborn babies, it is essential to integrate mental health screenings into antenatal visits through resource allocation and continuous training of midwives, strengthen community support systems, and provide targeted interventions for high-risk pregnant mothers. This study complements the growing body of evidence on APD in low-resource settings and emphasizes the importance of culturally relevant and accessible maternal mental health services especially the non-pharmacological approaches to address the unique needs of women in rural Uganda.
Future research should investigate urban-rural differences of APD, the long term impact of APD interventions and the impact of IPV and societal stigma on development of APD.
Abbreviations
APD, Antepartum Depression; BHC IV, Bwizibwera Health Centre IV; HICs, High-Income Countries; IPV, Intimate Partner Violence; LMICs, Low- and Middle-Income Countries; MMCHC IV, Mbarara Municipal Council Health Centre IV; MRRH, Mbarara Regional Referral Hospital; PPD, Postpartum Depression; SSA, Sub-Saharan Africa; UgShs, Uganda Shillings; WHO, World Health Organization.
Data Sharing Statement
The data that support the findings of this study are available from the first and corresponding author, Catherine Atuhaire but restrictions apply under license for the current study.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Mbarara University of Science and Technology Research Ethics Committee (MUST-REC) (MUST-2023-921). Permissions were also secured from the hospital director of MRRH, the District Health Officer of BHC IV, and the District City Officer of MMHC IV. Approval was further obtained from the Uganda National Council of Science and Technology (UNCST) (HS3525ES). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent for data collection and publication of the study findings was obtained from all the participants before they were enrolled into the study. Participants below 18 years are emancipated minors and therefore they provided written informed consent. Participants diagnosed with APD were referred to the Mental Health Clinic for further assessment and management.
Acknowledgments
We are grateful to all mothers who participated in this research.
Author Contributions
All authors made substantial contributions to conception and design, implementation of the study, analysis and interpretation of data; Catherine Atuhaire wrote the first draft of the manuscript and all the other authors took part in reviewing and revising the draft article; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the Fogarty International Center and [National Institute of Mental Health], of the National Institutes of Health under Award Number D43 TW011632. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This funding was for data collection and not publishing.
Disclosure
Authors declare the study was conducted in absence of any conflict of interest.
References
1. Organization WH. The WHO special initiative for mental health (2019–2023): universal health coverage for mental health. JSTOR. 2019.
2. Guo J, Zheng A, He J, et al. The prevalence of and factors associated with antenatal depression among all pregnant women first attending antenatal care: a cross-sectional study in a comprehensive teaching hospital. BMC Pregnancy Childbirth. 2021;21:1–9.
3. Woody C, Ferrari A, Siskind D, Whiteford H, Harris M. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disorders. 2017;219:86–92. doi:10.1016/j.jad.2017.05.003
4. Dadi AF, Wolde HF, Baraki AG, Akalu TY. Epidemiology of antenatal depression in Africa: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020;20:1–13.
5. Nabwire M, Nakimuli A, Nakasujja N, Migisha R, Kiggundu C. Prevalence and factors associated with anxiety disorders among pregnant women at Mulago National Referral Hospital, Uganda. Int J Women Health. 2024;16:237–247. doi:10.2147/IJWH.S440361
6. Kaggwa MM, Najjuka SM, Bongomin F, Mamun MA, Griffiths MD. Prevalence of depression in Uganda: a systematic review and meta-analysis. PLoS One. 2022;17(10):e0276552. doi:10.1371/journal.pone.0276552
7. Adeoye IA, Sogbesan A, Esan O. Prevalence, associated factors and perinatal outcomes of antepartum depression in Ibadan Nigeria. BMC Pregnancy Childbirth. 2022;22(1):219. doi:10.1186/s12884-022-04549-7
8. Evans-Lacko S, Aguilar-Gaxiola S, Al-Hamzawi A, et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO World Mental Health (WMH) surveys. Psychol Med. 2018;48(9):1560–1571. doi:10.1017/S0033291717003336
9. World Health Organization. Other common mental disorders:Global Health Estimates. 2017.
10. Babu GR, Murthy GVS, Singh N, et al. Sociodemographic and medical risk factors associated with antepartum depression. Front Public Health. 2018;6:127. doi:10.3389/fpubh.2018.00127
11. Lee KW, Ching SM, Devaraj NK, et al. Diabetes in pregnancy and risk of antepartum depression: a systematic review and meta-analysis of cohort studies. Int J Environ Res Public Health. 2020;17(11):3767. doi:10.3390/ijerph17113767
12. Joshi D, Shrestha S, Shrestha NJPO. Understanding the antepartum depressive symptoms and its risk factors among the pregnant women visiting public health facilities of Nepal. PLoS One. 2019;14(4):e0214992. doi:10.1371/journal.pone.0214992
13. Otieno F. Antepartum Depression and Intimate Partner Violence Experience Among Women in a Low-Income Urban Settlement in. Nairobi, Kenya: University of Nairobi; 2017.
14. Islam MJ, Broidy L, Baird K, Mazerolle P. Intimate partner violence around the time of pregnancy and postpartum depression: the experience of women of Bangladesh. PLoS One. 2017;12(5):e0176211. doi:10.1371/journal.pone.0176211
15. Gelaye B, Addae G, Neway B, et al. Poor sleep quality, antepartum depression and suicidal ideation among pregnant women. J Affect Disorders. 2017;209:195–200. doi:10.1016/j.jad.2016.11.020
16. Wang Y, Liu H, Zhang C, et al. Antepartum sleep quality, mental status, and postpartum depressive symptoms: a mediation analysis. BMC Psychiatry. 2022;22(1):521. doi:10.1186/s12888-022-04164-y
17. Al Rawahi A, Al kiyumi MH, Al Kimyani R, et al. The effect of antepartum depression on the outcomes of pregnancy and development of postpartum depression: a prospective cohort study of Omani women. Sultan Qaboos Univ Med J. 2020;20(2):e179. doi:10.18295/squmj.2020.20.02.008
18. Yu J, Zhang Z, Deng Y, et al. Risk factors for the development of postpartum depression in individuals who screened positive for antenatal depression. BMC Psychiatry. 2023;23(1):557. doi:10.1186/s12888-023-05030-1
19. Atuhaire C, Rukundo GZ, Nambozi G, et al. Prevalence of postpartum depression and associated factors among women in Mbarara and Rwampara districts of south-western Uganda. BMC Pregnancy Childbirth. 2021;21:1–12.
20. Howard LM, Khalifeh H. Perinatal mental health: a review of progress and challenges. World Psychiatry. 2020;19(3):313–327. doi:10.1002/wps.20769
21. Kelsey JL, Whittemore AS, Evans AS, Thompson WD. Methods of sampling and estimation of sample size. Monographs Epidemiol Biostatistics. 1996:311–340.
22. Karnouk C, Böge K, Lindheimer N, et al. Development of a culturally sensitive Arabic version of the Mini International Neuropsychiatric Interview (MINI-AR) and validation of the depression module. Int J Ment Health Syst 2021;15:1–10.
23. Webster J, Linnane JW, Dibley LM, Hinson JK, Starrenburg SE, Roberts JA. Measuring social support in pregnancy: can it be simple and meaningful? Birth. 2000;27(2):97–101. doi:10.1046/j.1523-536x.2000.00097.x
24. Mohammad KI, Abu Awad D, Creedy DK, Gamble J. Postpartum depression symptoms among Syrian refugee women living in Jordan. Res Nurs Health. 2018;41(6):519–524. doi:10.1002/nur.21919
25. UBoS IJK, Uganda. Uganda demographic and health survey 2016: key indicators report. 2017.
26. Lauwerys J. I. PRIMARY AND SECONDARY EDUCATION. Revue neurologique. 1965;113(5103):133–149.
27. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:385–396.
28. Vimalraj S. Mechanism of Labour. Labour and Delivery: An Updated. Guide: Springer; 2023:17–33.
29. Hosmer Jr DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. John Wiley & Sons; 2013.
30. Bennett HA, Einarson A, Taddio A, Koren G, Einarson TR. Prevalence of depression during pregnancy: systematic review. Obstetr Gynecol. 2004;103(4):698–709. doi:10.1097/01.AOG.0000116689.75396.5f
31. Ngocho JS, Minja LM, Mwamba RN, et al. Prevalence and predictors of depression among women attending antenatal care in Moshi, Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2022;22(1):594. doi:10.1186/s12884-022-04917-3
32. Sileo KM, Wanyenze RK, Crockett KS, et al. Prevalence and correlates of depressive symptoms, and points of intervention, in rural central Uganda: results from a cross-sectional population-based survey of women and men. BMJ Open. 2022;12(5):e054936. doi:10.1136/bmjopen-2021-054936
33. Nakidde G, Kumakech E, Mugisha JF. Prevalence and correlates of perinatal depression and anxiety at perinatal clinics in Southwestern Uganda: a cross-sectional study. Cureus. 2024;16(10).
34. Kasujja M, Omara S, Senkungu N, et al. Factors associated with antenatal depression among women attending antenatal care at Mubende Regional Referral Hospital: a cross-sectional study. BMC Women Health. 2024;24(1):195. doi:10.1186/s12905-024-03031-0
35. Okagbue HI, Adamu PI, Bishop SA, Oguntunde PE, Opanuga AA, Akhmetshin E. Systematic review of prevalence of antepartum depression during the trimesters of pregnancy. Open Access Macedonian J Med Sci. 2019;7(9):1555. doi:10.3889/oamjms.2019.270
36. Neumann DC. Alternative therapies for perinatal care: a holistic approach to pregnancy. 2010.
37. Muskens L, Boekhorst MG, Kop WJ, van den Heuvel MI, Pop VJ, Beerthuizen A. The association of unplanned pregnancy with perinatal depression: a longitudinal cohort study. Arch Women Mental Health. 2022;25(3):611–620. doi:10.1007/s00737-022-01225-9
38. Tsakiridis I, Bousi V, Dagklis T, et al. Epidemiology of antenatal depression among women with high-risk pregnancies due to obstetric complications: a scoping review. Arch Gynecol Obstetrics. 2019;300:849–859. doi:10.1007/s00404-019-05270-1
39. Duko B, Ayano G, Bedaso A. Depression among pregnant women and associated factors in Hawassa city, Ethiopia: an institution-based cross-sectional study. Reproductive Health. 2019;16:1–6.
40. Paulson JL. Intimate partner violence and perinatal post-traumatic stress and depression symptoms: a systematic review of findings in longitudinal studies. Trauma Violence Abuse. 2022;23(3):733–747. doi:10.1177/1524838020976098
41. Dadi AF, Miller ER, Bisetegn TA, Mwanri L. Global burden of antenatal depression and its association with adverse birth outcomes: an umbrella review. BMC Public Health. 2020;20:1–16.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.