Back to Journals » International Journal of Women's Health » Volume 17
Prevalence and Diagnostic Strategies for Sarcopenia in Menopausal and Non-Menopausal Women: A Cross-Sectional Comparative Study
Authors Li M, Yan X, Wu R, Liao Y, Zhang J, Ye Y, Xu C ![]()
Received 11 March 2025
Accepted for publication 14 June 2025
Published 28 June 2025 Volume 2025:17 Pages 1887—1895
DOI https://doi.org/10.2147/IJWH.S527620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Miaoyuan Li,1,2,* Xuewen Yan,3,* Rongshun Wu,4 Yanting Liao,5 Jing Zhang,3 Yufang Ye,3 Chenxia Xu6
1The First Clinical Medical College of Jinan University, Guangzhou, 510280, People’s Republic of China; 2Department of Urology, Zhongshan People’s Hospital, Zhongshan, 528400, People’s Republic of China; 3Women’s Health Department, Boai Hospital of Zhongshan, Zhongshan, 528400, People’s Republic of China; 4Department of Critical Care, Zhongshan People’s Hospital, Zhongshan, 528400, People’s Republic of China; 5Gynecology Department, Boai Hospital of Zhongshan, Zhongshan, 528400, People’s Republic of China; 6Prenatal Diagnosis Center, Boai Hospital of Zhongshan, Zhongshan, 528400, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chenxia Xu, Prenatal Diagnosis Center, Boai Hospital of Zhongshan, No. 6 Chenggui Road, East District, Zhongshan, Guangdong, 528400, People’s Republic of China, Email [email protected]
Objective: This study aimed to compare the prevalence of sarcopenia between postmenopausal and premenopausal women and evaluate the diagnostic performance of various screening methods combining anthropometric measurements and functional assessments.
Methods: A total of 1630 women (794 postmenopausal, 836 premenopausal) were included. Data on upper arm circumference (AC), calf circumference (CC), and SARC-F questionnaire scores were collected. ROC curve analysis was performed to assess the sensitivity, specificity, and accuracy of individual and combined diagnostic models.
Results: The overall prevalence of sarcopenia was 6.44%, with a higher prevalence in postmenopausal women (7.43%) than in premenopausal women (5.50%). Sarcopenic individuals had lower BMI and poorer functional performance. Among postmenopausal women, the SARC-F + CC combination demonstrated the highest diagnostic accuracy (AUC = 91.2), while in premenopausal women, the SARC-F + AC model was most effective (AUC = 85.53). The SARC-F + CC combination showed the best sensitivity (89.0%) and specificity (75.0%) across all participants.
Conclusion: Sarcopenia is more prevalent in postmenopausal women, with menopause identified as a key risk factor. Combining SARC-F with calf circumference enhances diagnostic accuracy and is recommended for early screening in primary healthcare settings to facilitate timely interventions and improve patient outcomes.
Keywords: sarcopenia, menopause, non-menopausal, prevalence, diagnostic methods, upper arm circumference, calf circumference, SARC-F questionnaire
Background
Sarcopenia is a prevalent and increasingly severe geriatric syndrome characterized by the progressive loss of skeletal muscle mass, strength, and function, which exacerbates with age.1 This condition not only significantly impacts physical function and quality of life in older adults, but is also closely associated with a higher risk of falls, fractures, frailty, urological cancers (e.g., bladder and kidney cancers), stress urinary incontinence, and mortality, placing a substantial burden on individuals and healthcare systems.2
Postmenopausal women are at particularly high risk for developing sarcopenia, primarily due to the significant decline in estrogen levels that occurs after menopause. Estrogen plays a crucial role in maintaining muscle mass and function by regulating protein synthesis and degradation, enhancing antioxidant defenses, and supporting mitochondrial function.3,4 Research has shown that the decrease in estrogen after menopause accelerates muscle mass loss and promotes fat infiltration into muscle, which significantly increases the risk of sarcopenia.5 In addition, postmenopausal women often experience a decline in physical activity and inadequate nutrition, which further exacerbates the process of muscle degeneration.6
Despite the higher risk of sarcopenia in postmenopausal women, it is often underrecognized and underdiagnosed in clinical practice. This is mainly due to the subtle signs of sarcopenia and the lack of clear diagnostic criteria and simple screening tools. Current standards, like those from the Asian and European Working Groups for Sarcopenia, often rely on complex techniques such as dual-energy X-ray absorptiometry (DXA) and bioelectrical impedance analysis (BIA), which are not practical for use in primary healthcare settings.7,8 As a result, there is an urgent need for simple, cost-effective, and reliable screening methods for early detection.
Recently, clinical tools such as the SARC-F questionnaire, arm circumference (AC), and calf circumference (CC) have been suggested for screening. However, research shows these methods have limited accuracy on their own.9–11 Therefore, combining multiple screening methods holds promise in improving the accuracy and clinical practicality of sarcopenia screening.
This study aims to compare the prevalence of sarcopenia in postmenopausal versus premenopausal women and evaluate the effectiveness of various diagnostic tools and their combinations. By conducting receiver operating characteristic (ROC) curve analysis, we will identify the optimal combination of arm circumference, calf circumference, and the SARC-F scale, as well as the most suitable diagnostic thresholds. The findings will contribute to the development of early intervention strategies and improve the management of sarcopenia, particularly in postmenopausal women, a high-risk group. As the global population ages, sarcopenia will become an increasingly significant public health issue. Therefore, understanding its prevalence and developing effective screening and intervention strategies is crucial for enhancing the health and quality of life of aging women.
Materials and Methods
Study Population
This study included a total of 1630 women aged 20 to 90 years, recruited from Boai Hospital in Zhongshan, Guangdong Province. Participants were categorized into two groups based on their menopausal status: 794 postmenopausal women (defined as having no menstruation for more than 12 consecutive months without other medical or surgical causes) and 836 premenopausal women.
Diagnostic Criteria and Screening Tools
Sarcopenia diagnosis was based on the 2019 Asian Working Group for Sarcopenia (AWGS) guidelines,7 which include the following assessment criteria (Figure 1).
 |
Figure 1 Sarcopenia Diagnostic Flowchart based on the 2019 Asian Working Group for Sarcopenia (AWGS) criteria. |
Demographic and Clinical Characteristics
Baseline demographic and clinical data were collected, including age, height, weight, body mass index (BMI), upper arm circumference (AC), calf circumference (CC), left and right handgrip strength, and SARC-F questionnaire scores. The SARC-F questionnaire served as a preliminary screening tool to assess the risk of sarcopenia. All participants underwent bioelectrical impedance analysis (BIA) to assess muscle mass, ensuring compliance with the 2019 Asian Working Group for Sarcopenia (AWGS) diagnostic criteria for sarcopenia.
Stratification Variable
Participants were stratified into postmenopausal and premenopausal groups based on menopausal status. Menopause is a key factor affecting muscle mass and function, primarily due to the decline in estrogen, which accelerates muscle loss and increases the risk of sarcopenia.3,12 Estrogen plays a crucial role in maintaining muscle metabolism, and its reduction after menopause contributes to decreased muscle strength and physical performance.5 Given these differences, stratification allows for a clearer comparison of sarcopenia prevalence and diagnostic accuracy between the two groups. Additionally, analyses were conducted for the total cohort to evaluate overall trends and the effectiveness of different screening models across all participants.
Diagnostic Models
Seven diagnostic models were developed using combinations of AC, CC, and the SARC-F questionnaire to identify the most effective screening strategy:
- Model A: Upper arm circumference (AC)
- Model B: Calf circumference (CC)
- Model C: SARC-F questionnaire
- Model D: AC + CC
- Model E: AC + SARC-F
- Model F: CC + SARC-F
- Model G: AC + CC + SARC-F
Statistical Analysis
Data analysis was performed using SPSS version 25.0.
- Continuous variables were expressed as mean ± standard deviation (Mean ± SD) and compared using an independent sample t-test.
- Categorical variables were presented as frequencies (n, %) and compared using the chi-square test.
- Logistic regression models were constructed to assess the diagnostic performance of various screening combinations. Predictors such as upper arm circumference (AC), calf circumference (CC), and SARC-F questionnaire scores were analyzed as continuous variables in both the regression analyses and receiver operating characteristic (ROC) analyses. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated, and the area under the curve (AUC) was used to assess overall diagnostic accuracy.
- A significance level of P < 0.05 was considered statistically significant.
Results
Prevalence of Sarcopenia
A total of 1630 women were included in this study, comprising 794 postmenopausal and 836 premenopausal women. The overall prevalence of sarcopenia was 6.44% (105/1630), with a higher prevalence observed in postmenopausal women (7.43%, 59/794) compared to premenopausal women (5.50%, 46/836). As shown in Table 1, postmenopausal women had a higher prevalence of sarcopenia, indicating a greater risk in this population.
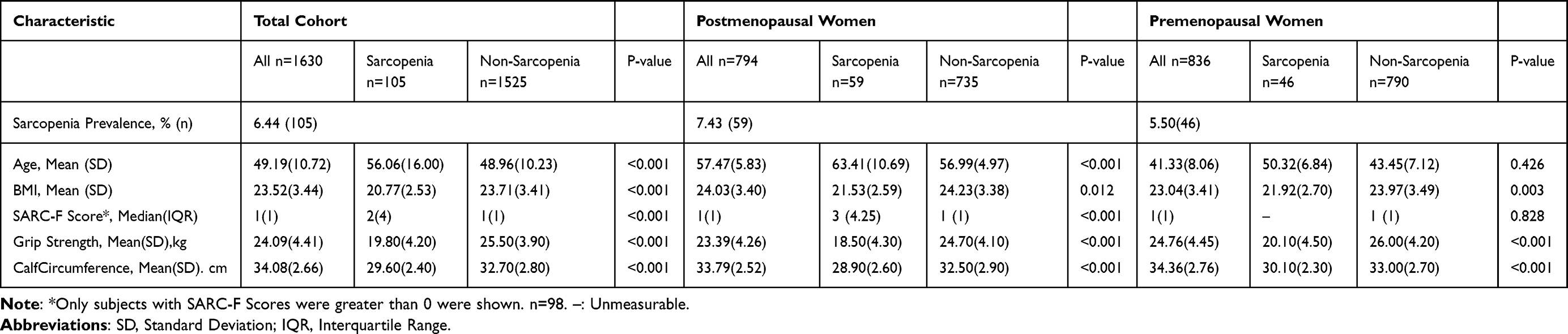 |
Table 1 Characteristics of the Study Participants |
Differences in Demographic and Clinical Characteristics
As presented in Table 1, sarcopenic individuals were significantly older than non-sarcopenic individuals. Among postmenopausal women, the mean age of the sarcopenic group was 63.41±10.69 years, compared to 56.99±4.97 years in the non-sarcopenic group. Similarly, in premenopausal women, sarcopenic individuals were older (50.32±6.84 years) compared to non-sarcopenic individuals (43.45±7.12 years).
BMI was notably lower in the sarcopenic group across all populations. In the total cohort, sarcopenic individuals had a BMI of 20.77±2.53, whereas non-sarcopenic individuals had a higher BMI of 23.71±3.41. Similar trends were observed in both postmenopausal and premenopausal groups.
Functional performance, as assessed by the SARC-F questionnaire, was poorer in sarcopenic individuals. As seen in Table 1, postmenopausal women with sarcopenia had a median SARC-F score of 8 (IQR: 7–10), higher than non-sarcopenic individuals (5 (IQR: 4–7)). Sarcopenic individuals also exhibited significantly lower handgrip strength and calf circumference measurements compared to non-sarcopenic individuals, indicating reduced muscle strength and mass.
Diagnostic Performance of Different Models
As shown in Table 2 and Figure 2, the diagnostic performance of various models for sarcopenia screening was evaluated across postmenopausal, premenopausal, and total populations.
- Postmenopausal Women: The highest diagnostic accuracy was observed with the SARC-F + CC combination, achieving an AUC of 91.2, with a sensitivity of 89.8% and specificity of 77.8%. The AC + CC combination also demonstrated good performance with an AUC of 91.0%.
- Premenopausal Women: In premenopausal women, the SARC-F + AC + CC combination had the highest AUC of 89.5, with sensitivity and specificity values of 89.0% and 74.2%, respectively.
- Total Cohort: Across the entire cohort, the highest AUC was achieved by the SARC-F + AC + CC combination (89.09), with a sensitivity of 89.0% and specificity of 75.0%.
Among the individual diagnostic tools, calf circumference (CC) alone showed strong discriminatory ability, with an AUC of 91.0 in postmenopausal women and 88.34 in premenopausal women. However, its statistical significance was not observed in all subgroups.
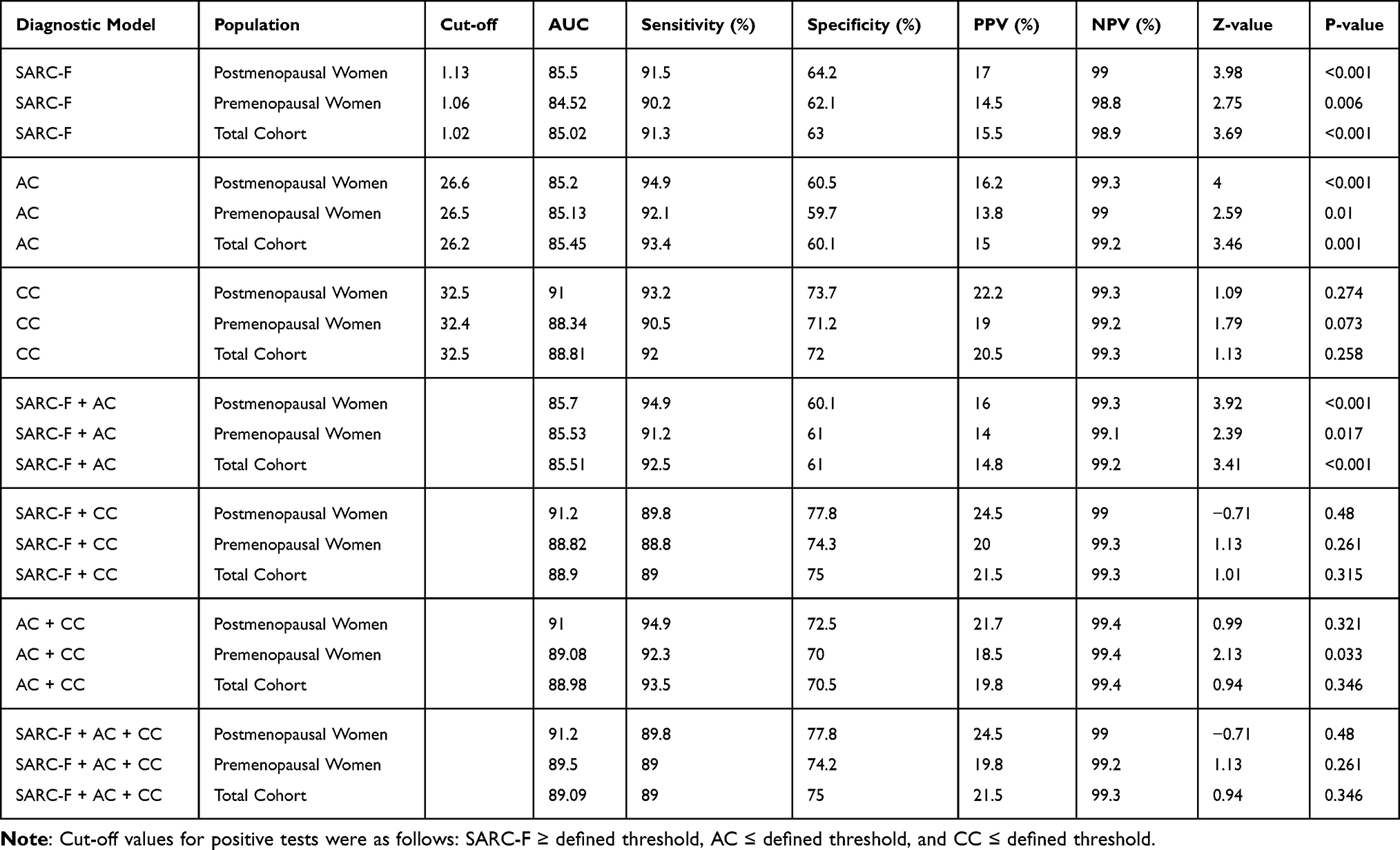 |
Table 2 Performance of Different Diagnostic Models in Various Populations |
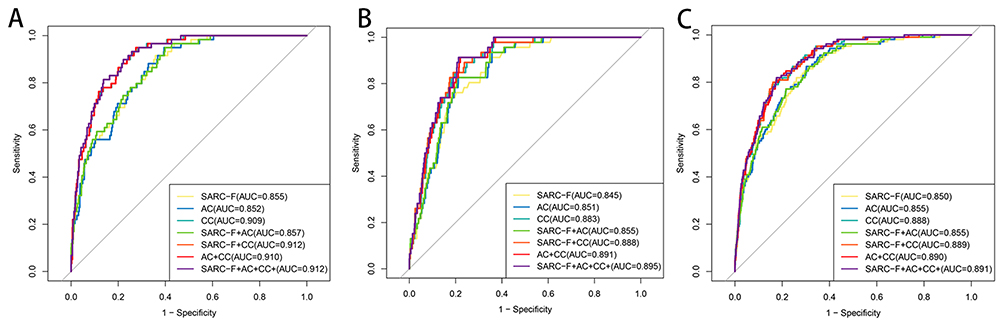 |
Figure 2 ROC Curve Results for the Seven Methods of Sarcopenia Prediction: (A) Postmenopausal Women; (B) Premenopausal Women; (C) Total Cohort. |
Key Findings and Implications
Based on the results in Tables 1 and 2, several important observations can be made:
- Postmenopausal women exhibited a higher prevalence of sarcopenia, highlighting the need for targeted screening in this population.
- Lower BMI and reduced muscle strength were closely associated with sarcopenia across all groups.
- Combining simple, non-invasive measures such as SARC-F and calf circumference significantly improved diagnostic accuracy, making them practical tools for clinical screening.
- The SARC-F + CC combination emerged as the most effective model for postmenopausal women, while the SARC-F + AC + CC model provided the highest diagnostic accuracy for the total population.
Discussion
This study underscores the significant impact of menopause on the prevalence of sarcopenia and provides valuable insights into the effectiveness of various diagnostic models. The findings highlight the need for early screening and targeted interventions, particularly in postmenopausal women, to mitigate the adverse effects associated with sarcopenia.
Higher Prevalence of Sarcopenia in Postmenopausal Women
Our study revealed a higher prevalence of sarcopenia in postmenopausal women (7.43%) compared to premenopausal women (5.50%), consistent with previous research suggesting that hormonal changes, especially the decline in estrogen, contribute to muscle loss and functional impairment. Estrogen plays a crucial role in maintaining muscle mass by modulating protein synthesis and mitochondrial function. Its decline after menopause accelerates muscle deterioration, leading to increased frailty and a higher risk of falls and fractures.4
Impact of Age and BMI on Sarcopenia
As shown in Table 1, individuals with sarcopenia were significantly older than those without, consistent with international findings that aging is a key risk factor for sarcopenia due to changes in muscle metabolism, neuromuscular function, and hormonal levels.13,14 Additionally, sarcopenic women had significantly lower BMI, suggesting that lower body mass may indicate higher sarcopenia risk. Reduced BMI is often associated with inadequate protein intake, decreased physical activity, and metabolic changes that contribute to muscle wasting.15 Huang et al further highlighted the importance of dietary quality for muscle strength in multi-ethnic Asian populations, emphasizing nutrition as a crucial factor in sarcopenia prevention.16
Functional and Muscle Strength Decline in Sarcopenic Women
Functional limitations, as assessed by the SARC-F questionnaire, were more pronounced in sarcopenic women, with higher median SARC-F scores indicating greater difficulties in daily activities. The significant reduction in grip strength and calf circumference further confirmed the loss of muscle strength and mass in sarcopenic individuals. Consistent with our findings, Lu et al reported that SARC-F has high specificity but only moderate sensitivity, highlighting the need to combine it with objective anthropometric measures to improve screening accuracy.17 These results support the utility of combining functional assessments with objective muscle measurements to improve the accuracy of sarcopenia screening and facilitate early intervention.18
Diagnostic Performance of Different Models
The evaluation of diagnostic models (Table 2) demonstrated that the combination of SARC-F and calf circumference (SARC-F + CC) achieved the highest diagnostic accuracy in postmenopausal women (AUC = 91.2). This combination provided a good balance between sensitivity (89.8%) and specificity (77.8%), making it a practical and effective screening tool. These findings are consistent with Bahat et al, who reported enhanced diagnostic accuracy when combining SARC-F with calf circumference (SARC-CalF), especially among Asian populations.19
For the total cohort, the combination of SARC-F, AC, and CC yielded the highest AUC (89.09), with balanced sensitivity (89.0%) and specificity (75.0%). This finding indicates that a multi-parameter approach improves diagnostic accuracy and may be more suitable for broader population-based screening programs.20 Notably, the individual performance of calf circumference alone (AUC = 91.0 in postmenopausal women) suggests its strong potential as a single, easy-to-use screening measure, although its performance in premenopausal women was less robust.21,22
Clinical Implications
Our findings suggest that integrating functional and anthropometric assessments into routine clinical practice can enhance sarcopenia detection, particularly in postmenopausal women who are at greater risk. Given the high sensitivity of the SARC-F + CC combination, it may be especially useful for initial screening in primary care settings, allowing for early identification and intervention before severe functional decline occurs.
Study Limitations and Future Directions
Despite the valuable insights gained from this study, several limitations should be considered. First, the study was conducted in a single center and focused exclusively on an Asian population, which may limit the generalizability of the findings to other ethnic or geographic groups. Anthropometric measures such as calf circumference (CC) and arm circumference (AC) are population-dependent, and prior studies have demonstrated significant differences in these measures between Asian and European populations, likely due to variations in body composition and nutritional patterns.21,23 Future multi-center studies with larger and more ethnically diverse samples are necessary to validate the diagnostic models and confirm their applicability in diverse settings. Additionally, the cross-sectional nature of the study prevents the establishment of causal relationships between sarcopenia and its associated risk factors. Longitudinal studies are required to better understand the progression of sarcopenia over time and the long-term effects of different interventions.
Future research should also explore the integration of advanced imaging techniques, such as dual-energy X-ray absorptiometry (DXA), to further enhance the precision of sarcopenia diagnosis. Furthermore, incorporating biochemical markers of muscle metabolism could provide additional insights into the underlying mechanisms of sarcopenia in postmenopausal women.
Conclusion
This study highlights the higher prevalence of sarcopenia in postmenopausal women and the utility of combining functional and anthropometric measures for improved screening accuracy. The SARC-F + CC combination emerged as a highly effective screening tool, offering a balance of sensitivity and specificity. Evidence suggests that dietary quality plays a key role in maintaining muscle strength, particularly among Asian populations, highlighting the importance of nutrition in preventing sarcopenia. Given that anthropometric indicators such as CC and AC are population-dependent, further validation in diverse cohorts is warranted. Early detection and tailored interventions, including lifestyle modifications and nutritional support, are crucial for preventing the progression of sarcopenia and improving health outcomes in aging women.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Boai Hospital of Zhongshan (protocol code KY-2024-001-04).
Acknowledgments
Miaoyuan Li and Xuewen Yan are co-first authors for this study. We thank the staff and technicians of the Prenatal Diagnosis Center and Women’s Health Department at Boai Hospital for their invaluable support and assistance in data collection. We also gratefully acknowledge Dr. Yan Pan from the School of Public Health, Sun Yat-sen University, for his contribution to the statistical analysis of this study.
Funding
This research was funded by the Zhongshan Science and Technology Bureau, grant numbers 2021B3005 and 2023B1042. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Disclosure
The authors declare no competing interests in this work.
References
1. Papadopoulou SK. Sarcopenia: a contemporary health problem among older adult populations. Nutrients. 2020;12(5):1293. doi:10.3390/nu12051293
2. Yeung SSY, Reijnierse EM, Pham VK, et al. Sarcopenia and its association with falls and fractures in older adults: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2019;10(3):485–500. doi:10.1002/jcsm.12411
3. Buckinx F, Aubertin-Leheudre M. Sarcopenia in menopausal women: current perspectives. Int J Womens Health. 2022;14:805–819. doi:10.2147/ijwh.S340537
4. Warzecha M, Amarowicz J, Berwecka M, et al. Relation between risk of falls, sarcopenia and parameters assessing quality of skeletal muscles in a group of postmenopausal women. Menop Rev/Przeglad Menopauzalny. 2020;19(3):123–129. doi:10.5114/pm.2020.99617
5. Geraci A, Calvani R, Ferri E, et al. Sarcopenia and menopause: the role of estradiol. Front Endocrinol. 2021:12. doi:10.3389/fendo.2021.682012
6. Willoughby DS, Florez C, Davis J, et al. Decreased neuromuscular function and muscle quality along with increased systemic inflammation and muscle proteolysis occurring in the presence of decreased estradiol and protein intake in early to intermediate post-menopausal women. Nutrients. 2024;16(2):197. doi:10.3390/nu16020197
7. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e302. doi:10.1016/j.jamda.2019.12.012
8. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
9. Woo J, Leung J, Morley JE. Defining sarcopenia in terms of incident adverse outcomes. J Am Med Dir Assoc. 2015;16(3):247–252. doi:10.1016/j.jamda.2014.11.013
10. Ida S, Kaneko R, Murata K. SARC-F for screening of sarcopenia among older adults: a meta-analysis of screening test accuracy. J Am Med Dir Assoc. 2018;19(8):685–689. doi:10.1016/j.jamda.2018.04.001
11. Barbosa-Silva TG, Menezes AM, Bielemann RM, et al. Enhancing SARC-F: improving sarcopenia screening in the clinical practice. J Am Med Dir Assoc. 2016;17(12):1136–1141. doi:10.1016/j.jamda.2016.08.004
12. Ko J, Park YM. Menopause and the loss of skeletal muscle mass in women. Iran J Public Health. 2021;50(2):413–414. doi:10.18502/ijph.v50i2.5362
13. Rodrigues F, Domingos C, Monteiro D, et al. A review on aging, sarcopenia, falls, and resistance training in community-dwelling older adults. Int J Environ Res Public Health. 2022;19(2):874. doi:10.3390/ijerph19020874
14. Sato PHR, Ferreira AA, Rosado EL. The prevalence and risk factors for sarcopenia in older adults and long-living older adults. Arch Gerontol Geriatrics. 2020;89:104089. doi:10.1016/j.archger.2020.104089
15. Martinez JA, Wertheim BC, Thomson CA, et al. Physical activity modifies the association between dietary protein and lean mass of postmenopausal women. J Acad Nutr Diet. 2017;117(2):192–203.e191. doi:10.1016/j.jand.2016.10.009
16. Huang J, Shanmugam A, Huang X, et al. Association of diet quality with hand grip strength weakness and asymmetry in a multi-ethnic Asian cohort. Br J Nutr. 2024;131(7):1236–1243. doi:10.1017/s0007114523002647
17. Lu JL, Ding LY, Xu Q, et al. Screening accuracy of SARC-F for sarcopenia in the elderly: a diagnostic meta-analysis. J Nutr Health Aging. 2021;25(2):172–182. doi:10.1007/s12603-020-1471-8
18. Ackermans LLGC, Rabou J, Basrai M, et al. Screening, diagnosis and monitoring of sarcopenia: when to use which tool? Clin Nutr ESPEN. 2022;48:36–44. doi:10.1016/j.clnesp.2022.01.027
19. Bahat G, Erdoğan T, Ilhan B. SARC-F and other screening tests for sarcopenia. Curr Opin Clin Nutr Metab Care. 2022;25(1):37–42. doi:10.1097/mco.0000000000000801
20. Krzymińska-Siemaszko R, Deskur-śmielecka E, Kaluźniak-Szymanowska A, et al. Comparison of diagnostic value of the SARC-F and its four modified versions in polish community-dwelling older adults. Clin Interv Aging. 2023;18:783–797. doi:10.2147/cia.S408616
21. Champaiboon J, Petchlorlian A, Manasvanich B-A, et al. Calf circumference as a screening tool for low skeletal muscle mass: cut-off values in independent Thai older adults. BMC Geriatr. 2023;23(1):826. doi:10.1186/s12877-023-04543-4
22. Kiss CM, Bertschi D, Beerli N, et al. Calf circumference as a surrogate indicator for detecting low muscle mass in hospitalized geriatric patients. Aging Clin Experiment Res. 2024;36(1):25. doi:10.1007/s40520-024-02694-x
23. Wulan SN, Westerterp KR, Plasqui G. Ethnic differences in body composition and the associated metabolic profile: a comparative study between Asians and Caucasians. Maturitas. 2010;65(4):315–319. doi:10.1016/j.maturitas.2009.12.012
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.