Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
Prevalence and Association of Mandibular Three-Rooted Deciduous Second and Permanent First Molars: A Retrospective CBCT Study in Iraqi Pediatric Population
Authors Talabani R ![]() , Rashid ZJ
, Rashid ZJ ![]() , Noori A
, Noori A ![]() , Amin A
, Amin A ![]() , Mohammed Saeed HM
, Mohammed Saeed HM ![]()
Received 7 March 2026
Accepted for publication 2 May 2026
Published 13 May 2026 Volume 2026:18 607617
DOI https://doi.org/10.2147/CCIDE.S607617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Renan Dal Fabbro
Ranjdar Talabani,1 Zhwan Jamal Rashid,2 Arass Noori,3 Anwar Amin,2 Hawzhen Masoud Mohammed Saeed1
1Department of Conservative Dentistry, College of Dentistry, University of Sulaimani, Sulaimani, Sulaimani, 46001, Iraq; 2Department of Orthodontics, College of Dentistry, University of Sulaimani, Sulaimani, 46001, Iraq; 3Department of Pedodontics and Community Oral Health, College of Dentistry, University of Sulaimani, Sulaimani, 46001, Iraq
Correspondence: Arass Noori, Department of Pedodontics and Community Oral Health, College of Dentistry, University of Sulaimani, Sulaimani, 46001, Iraq, Tel +964 770 144 5808, Email [email protected]
Purpose: To estimate the prevalence of three-rooted mandibular deciduous second molars (3RME) and three-rooted mandibular permanent first molars (3RM6) in Iraqi children and to evaluate their association using cone-beam computed tomography (CBCT).
Methods: This retrospective cross-sectional study analyzed CBCT scans of Iraqi children aged 7– 12 years (N = 196). Root morphology was assessed in axial, coronal, and sagittal planes. Prevalence was calculated at the patient level (presence of ≥ 1 affected tooth). Associations between 3RME and 3RM6 were tested using the chi-square test, and age/sex were explored as predictors using logistic regression. Intra- and inter-examiner reliability were assessed with Cohen’s kappa.
Results: Three-rooted morphology was identified in 3/196 children for 3RME (1.53%; 95% CI 0.52– 4.40) and 10/196 children for 3RM6 (5.10%; 95% CI 2.80– 9.14). A significant association was observed between 3RME and 3RM6 (χ2(4, N = 196) = 96.48, p < 0.001; Cramér’s V = 0.50). Age and sex were not significant predictors (p > 0.05).
Conclusion: Three-rooted mandibular molars were uncommon in this Iraqi pediatric sample; however, 3RME co-occurred significantly with 3RM6, indicating a strong association that may be clinically useful for anticipatory diagnosis and treatment planning.
Keywords: molar teeth, mandibular deciduous second molars, mandibular permanent first molars, cone-beam computed tomography, radix entomolaris
Introduction
A knowledge of individual tooth anatomy is essential for proper treatment planning in all branches of dentistry, especially in endodontics, pedodontics, and orthodontics.1 A knowledge of root and canal anatomy is of the utmost importance in endodontics because the number and configuration of the roots and their canals, canal anatomy including the presence of any lateral or accessory canals, apical deltas, and the size and taper of the canal influence the outcome of pulpotomy and root canal therapy in both deciduous and permanent teeth.2–4 Additionally, in orthodontics, the number and shape of roots of the teeth can influence the rate of tooth movement, anchorage requirements, and final result of orthodontic treatment.5,6
Morphological and anatomical similarities between the deciduous second molar and the permanent first molar of the mandible are present,7 and a well-known anatomic variation is the existence of a supernumerary root, usually distolingual, also known as radix entomolaris (RE) or supernumerary root, which was described for the first time by Carabelli in 1844.8 The exact etiology is unknown, but it is believed to be of multifactorial origin, with a combination of genetic and environmental factors.2,9
The prevalence of Radix entomolaris (RE) differs between ethnic groups, and in European populations it has been found to be 3.4–4.2%,10,11 while it is 3% in African populations12 and generally below 5% in Indian and Eurasian groups.12,13 Much higher prevalence, up to 5% and 30%, have been found in East Asian and Native American populations, particularly in individuals of Mongoloid descent, which suggests a possible hereditary background of the trait.14,15 These geographical and ethnic differences were further supported by a 2022 meta-analysis by Aung and Myint, which showed significant regional differences in prevalence of three-rooted permanent mandibular first molar (3RM6).15
Despite this recognized ethnic variability, population-specific data for Iraqi children remain limited, and the relationship between three-rooted morphology in the deciduous mandibular second molar (3RME) and the permanent mandibular first molar (3RM6) is underreported in pediatric samples. Establishing pediatric prevalence is clinically relevant because early recognition of 3RME could alert clinicians to an increased likelihood of 3RM6 in the same patient, supporting anticipatory diagnosis and optimized access design, imaging decisions, and treatment planning.16,17
Therefore, the aim of this study was to determine the prevalence of three-rooted mandibular deciduous second molars (3RME) and permanent first molars (3RM6), and to evaluate their association in an Iraqi pediatric population using CBCT. The null hypothesis states that there is no significant association between the presence of 3RME and 3RM6 in this population.
Materials and Methods
Study Design and Ethical Approval
This retrospective cross-sectional study aimed to evaluate the anatomical features of 3RMEs and 3RM6s in an Iraqi pediatric sub-population. Ethical approval was obtained from the College of Dentistry, University of Sulaimani (Protocol Code: 564, Registration Number: 125/22, dated August 9, 2022).
All procedures were performed in accordance with the ethical standards of the College of Dentistry, University of Sulaimani, and the Declaration of Helsinki. To ensure patient data confidentiality, all retrospective CBCT data used in this study were fully anonymized and de-identified prior to analysis. No personal identifying information and no direct identifiers (such as names, patient ID numbers, or contact details) were accessed, recorded, or reported. Access to the imaging archives was strictly controlled and limited to researchers involved in the anatomical evaluation.
Sample Selection
A total of 196 CBCT scans of Iraqi children aged 7–12 years were retrospectively collected from the archives of B&R and Baxshin Dental Centers (January 1, 2018 to June 30, 2021). All eligible scans were included regardless of root morphology in order to estimate prevalence. Scans were included if at least one mandibular deciduous second molar and/or mandibular permanent first molar was present and evaluable with adequate image quality to determine the number of roots and visualize root apices.
Deciduous second molars were included when external root resorption involved less than one-quarter of root length. Permanent first molars were included when more than two-thirds of root formation was completed. Teeth with extensive restorations (eg, posts/cores, crowns), previous endodontic treatment, root or crown fractures, severe caries compromising root assessment, or periapical lesions obscuring apical anatomy were excluded Scans with motion artifacts, severe beam-hardening artifacts, or inadequate contrast were excluded. Cases with missing age/sex data or outside the target age range were excluded. Minor restorations not affecting root visualization were permitted.
CBCT Imaging and Analysis
All CBCT scans were acquired using the GALILEOS Sirona Comfort PLUS unit (Sirona Dental Systems GmbH, Bensheim, Germany), featuring a spherical imaging volume of 15.4 cm and an isotropic voxel size of 0.125 or 0.25 mm. Imaging parameters were standardized (98 kVp, 3–5 mA, 14-second exposure time). The scans were processed using Sidexis XG software (v2.6) and Galileos Implant software (v1.9).
Root morphology was assessed in axial, coronal, and sagittal planes. A molar was classified as “three-rooted” if an additional distolingual root was present along with the mesial and distal roots.
Sample Size Calculation
Sample size was calculated using G*Power software (version 3.1.9.4). Assuming a small expected effect size based on Cohen’s criteria (|ρ| = 0.2), a significance level of α = 0.05, and 80% power, a total of 191 CBCT scans was determined to be necessary using a two-tailed point biserial correlation model.18,19 Although the minimum required sample size was 191, a total of 196 scans were included to enhance robustness and improve the reliability of the statistical analysis.
Reliability Assessment
To ensure consistency, a pilot study was conducted using 10 CBCT scans selected at random. Two trained examiners independently reviewed the images to identify three-rooted molars. A standard evaluation protocol was developed and refined after pilot testing. Intra- and inter-examiner reliability was assessed using Cohen’s kappa coefficient, with values above 0.8 indicating substantial agreement. Each examiner re-evaluated the same scans after a two-week interval to measure intra-examiner agreement.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics (v25). Descriptive statistics summarized age (mean ± SD), sex distribution, and patient-level prevalence of 3RME and 3RM6 with 95% confidence intervals. Associations were assessed using the chi-square test (with effect size reported as Cramér’s V). Logistic regression was used to explore age and sex as potential predictors. A p-value < 0.05 was considered statistically significant.
Results
Sample Selection and Demographics
Out of an initial pool of 290 CBCT scans from patients aged 7–12 years, 196 scans (103 males, 93 females) met the eligibility criteria and were included (Figure 1). The mean age was 9.08 ± 1.42 years (Table 1).
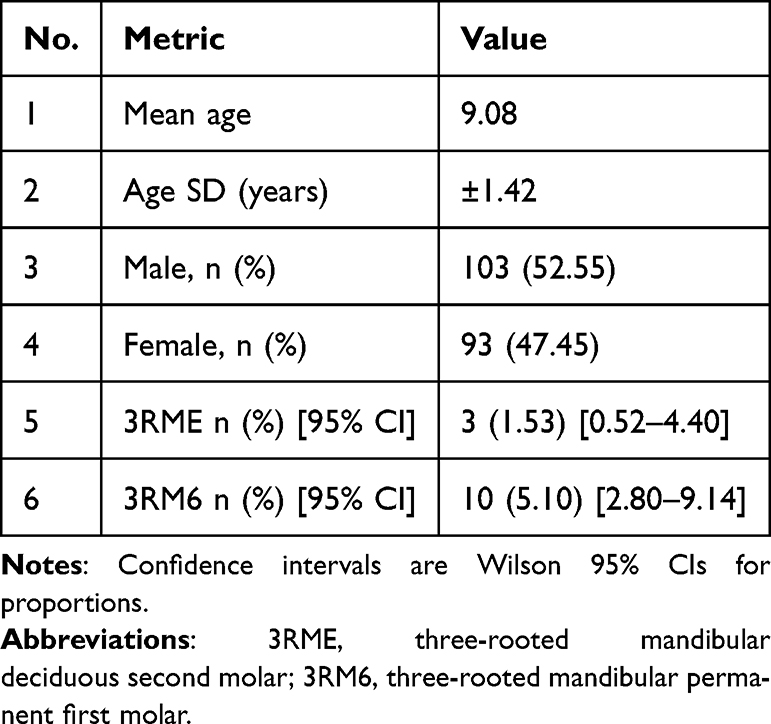 |
Table 1 Descriptive Characteristics of the Study Sample (N = 196) |
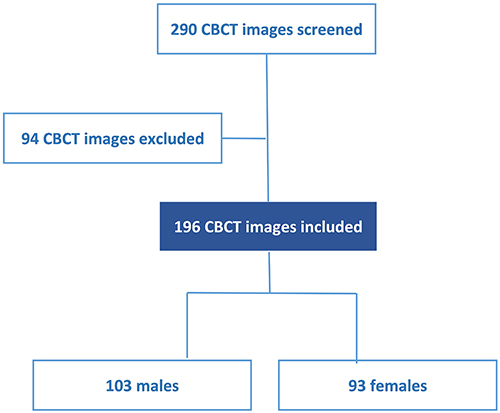 |
Figure 1 Flow diagram showing inclusion and exclusion of cone-beam computed tomography (CBCT) images. |
Prevalence of Three-Rooted Molars (Patient-Level)
Three-rooted mandibular deciduous second molars (3RME) were identified in 3/196 children (1.53%; 95% CI 0.52–4.40), including 2 unilateral cases (1.02%) and 1 bilateral case (0.51%). Three-rooted mandibular permanent first molars (3RM6) were identified in 10/196 children (5.10%; 95% CI 2.80–9.14), including 4 unilateral cases (2.04%) and 6 bilateral cases (3.06%).
Sex Distribution
Males showed slightly higher frequencies than females; however, the differences were not statistically significant (p > 0.05) (Figure 2).
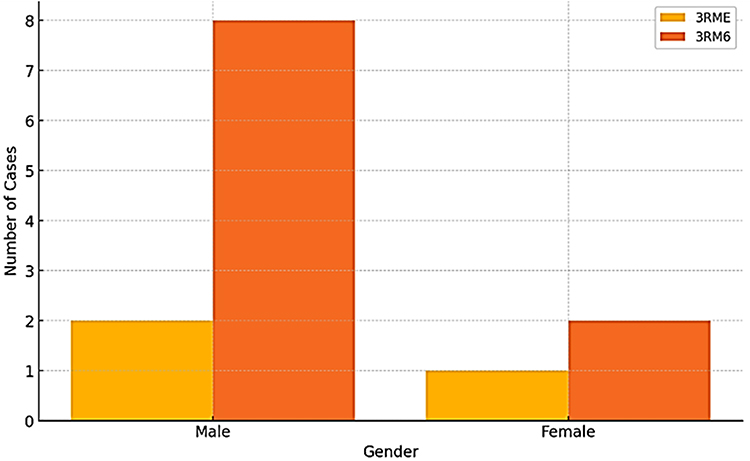 |
Figure 2 Bar chart showing prevalence of three-rooted mandibular deciduous second molars (3RME) and three rooted mandibular permanent first molars (3RM6) by gender. |
Association Between 3RME and 3RM6
A significant association was found between the presence of 3RME and 3RM6 using the chi-square test (χ2(4, N = 196) = 96.48, p < 0.001; Cramér’s V = 0.50). This indicates a strong association, as all patients identified with 3RME also exhibited 3RM6 in this sample; however, this observation is based on a very small number of cases and should be interpreted with caution (Table 2).
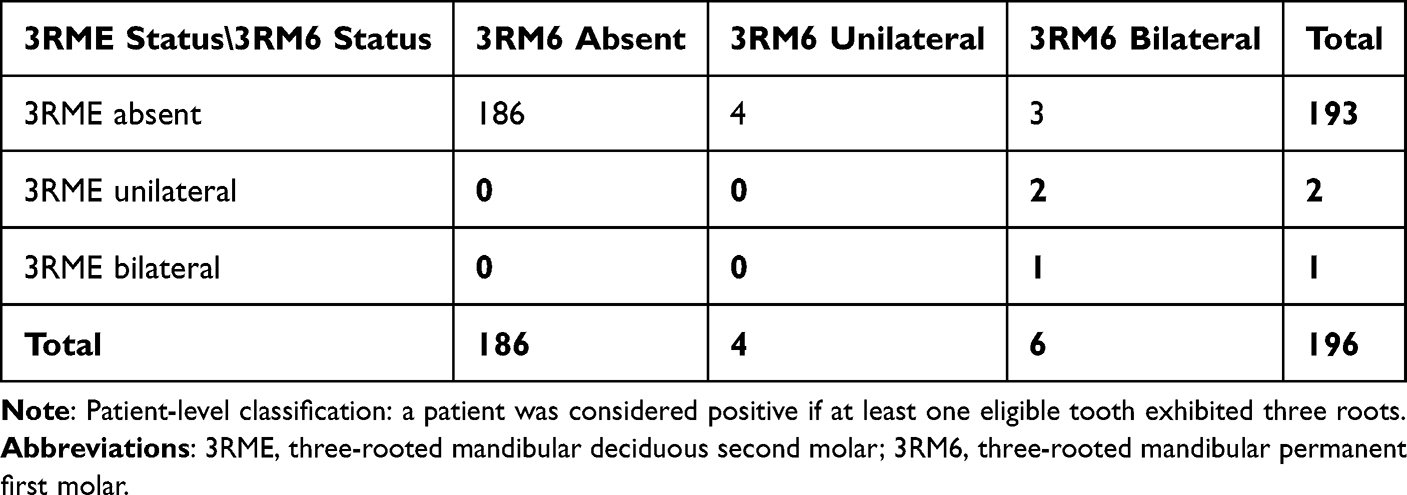 |
Table 2 Cross-Tabulation of Three-Rooted Mandibular Deciduous second Molars (3RME) and Three-Rooted Mandibular Permanent First Molars (3RM6) at the Patient Level (N = 196) |
Morphological Confirmation Using CBCT
Figure 3 presents clinical CBCT images and 3D reconstructions used to confirm the presence of three-rooted mandibular molars. The case is demonstrated through a series of axial slices (A–D) capturing the root morphology at various levels, a buccolingual cross-section (E) of the right side, and a 3D rendered lingual view (F) of the mandible. These views clearly delineate the accessory roots, identifying both the radix entomolaris in the first permanent molar and the additional root in the second deciduous molar.
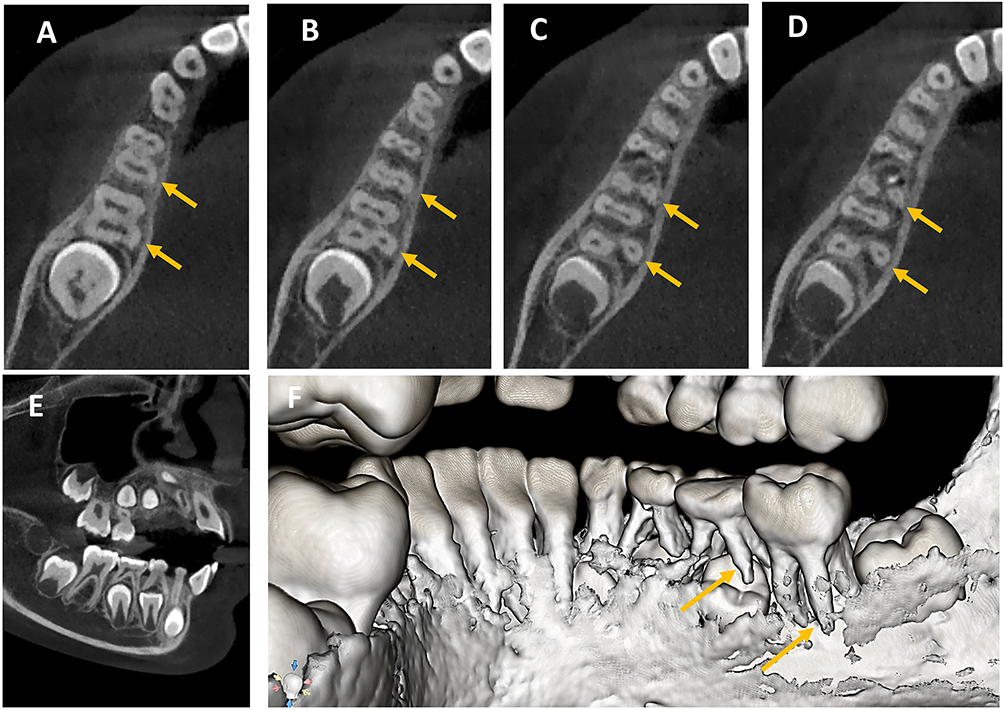 |
Figure 3 CBCT confirmation of three-rooted right mandibular molars. (A–D) A series of axial CBCT views at different root levels demonstrating the three-rooted morphology of the first permanent molar (3RM6) and the second deciduous molar (3RME). (E) Buccolingual CBCT view of the right mandibular quadrant. (F) Lingual view of the 3D rendered model showing the extra roots of the first permanent and second deciduous molars. Yellow arrows indicate the radix entomolaris of the first permanent molar and the extra root of the second deciduous molar. |
Predictors of 3RME and 3RM6
Logistic regression models assessed the effect of age and sex as predictors for 3RME and 3RM6:
3RME: Age: P = 0.39 and Sex: P = 0.66
3RM6: Age: P = 0.33 and Sex: P = 0.10
None of these factors were statistically significant, indicating that neither age nor sex significantly predicted the presence of three-rooted molars.
Discussion
The present study aimed to evaluate the anatomical variations of the mandibular deciduous second molars and permanent first molars in an Iraqi sub-population by using CBCT, and the retrospective nature of the study, along with a statistically appropriate sample size, calculated using G*Power, provided strong estimations of the prevalence of the investigated variables. CBCT provided high diagnostic accuracy and allowed detailed visualization of the root morphology, moreover, the limitations of 2D imaging, particularly in DL roots which may be obscured by overlapping anatomical structures in periapical radiographs, were minimized.17,20
The present study’s overall prevalence (3RME: 1.53%, 3RM6: 5.1%) falls within the global prevalence, and it emphasizes the wide variability of this trait in various ethnic populations, supporting the significance of genetic factors and geographical distribution in the prevalence of dental anatomical variations.16,21 The results of the present study are in line with the previous reports of significant geographical and ethnic variations in the prevalence of three-rooted mandibular molars.11,13,22
The statistically significant association between 3RME and 3RM6 observed in this study (p < 0.001) suggests a potential shared developmental or genetic basis influencing root morphology in both the deciduous and permanent dentitions. This aligns with findings from other populations, where anatomical traits in deciduous teeth were found to predict similar features in their permanent successors.7 Accordingly, the null hypothesis was rejected. This finding supports the concept that three-rooted morphology in the deciduous dentition may be associated with three-rooted morphology in the permanent dentition within the same patient. However, given the cross-sectional retrospective design, this association should be interpreted as correlational and not evidence of a shared developmental pathway or causality.
A slightly higher prevalence was recorded in males, however, there was no significant gender difference, because it has been reported that gender has minimal influence on the prevalence of supernumerary roots.2 Age was not found to be a significant factor, which agrees with the fact that root morphology is almost entirely determined at the time of tooth eruption and does not change significantly over time.23
The clinical significance of the three-rooted mandibular molar is that the treatment complexity increases due to difficulty in locating and negotiating the additional canal, and the curvature of the root is more complex, and the access cavity design is also more difficult. In radix entomolaris, the traditional triangular access cavity design often needs to be modified to trapezoidal or rectangular in order to have a better vision and location of the distolingual canal.2 If the extra DL canal is not located or negotiated, it would easily lead to incomplete debridement and obturation, and would compromise the long-term success of the treatment. The extra root also affects the anchorage and biomechanics in orthodontic treatment, and the three-rooted molars may respond to orthodontic force in a different way, while the unrecognized anatomical variations can affect the efficiency and the outcome of the movement. Therefore, a thorough pre-treatment radiographic assessment with high-quality images is essential for identifying the variations and incorporating the variations into the endodontic and orthodontic treatment plan.5
However, this study has some limitations, because it was a retrospective study that used pre-existing CBCT scans for specific clinical indications and not for population screening, which may introduce a selection bias. Moreover, the studied population was from a single ethnic background, an Iraqi subpopulation, and the findings should be interpreted with caution when generalized to other populations, therefore prospective multicenter studies on larger and more diverse populations are recommended to provide further information on the prevalence, distribution and clinical significance of these anatomical variations. A key limitation of this study is the very small number of positive cases, particularly for 3RME (n = 3), which limits statistical precision and may inflate the strength of observed associations. Additionally, a recent study using CBCT scans from a Brazilian subpopulation also showed regional and ethnic differences in radix molaris prevalence, thus highlighting the need for population-specific data on dental morphology and treatment planning.24
Conclusion
In this Iraqi pediatric CBCT sample, three-rooted mandibular deciduous second molars and permanent first molars were uncommon. A strong association was observed between 3RME and 3RM6, suggesting that detection of 3RME may be clinically useful for prompting careful assessment of 3RM6. Because this was a referral-based retrospective CBCT study with few positive cases, the findings should be interpreted cautiously, and larger multicenter studies are warranted.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (Ethics Committee) of the College of Dentistry, University of Sulaimani (Protocol Code: 564, Registration Number: 125/22, dated August 9, 2022).
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank the staff of B&R and Baxshin Dental Centers for their administrative support in accessing archived CBCT scans.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shabbir J, Zehra T, Najmi N, et al. Access cavity preparations: classification and literature review of traditional and minimally invasive endodontic access cavity designs. J Endod. 2021;47(8):1229–8. PMID: 34058252. doi:10.1016/j.joen.2021.05.007
2. Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod. 2007;33(1):58–63. PMID: 17185133. doi:10.1016/j.joen.2006.05.007
3. Moyaho-Bernal MA, Carrasco-Gutiérrez R, Jiménez-Flores R, et al. Prevalence of three-rooted primary mandibular first and second molars: clinical and radiographic findings in a Mexican population. Acta Odontol Latinoam. 2021;34(2):149–155. PMID: 34570863; Central PMCID: PMC10315086. doi:10.54589/aol.34/2/149
4. Duncan HF, El-Karim I, Dummer PMH, Whitworth J, Nagendrababu V. Factors that influence the outcome of pulpotomy in permanent teeth. Int Endod J. 2023;56(Suppl 2):62–81. PMID: 36334098. doi:10.1111/iej.13866
5. Nabbout F, Baron P. Anchorage in orthodontics: three-dimensional scanner input. J Int Soc Prev Community Dent. 2018;8(1):6–11. PMID: 29629323; Central PMCID: PMC5853044. doi:10.4103/jispcd.JISPCD_422_17
6. Gardner JD, Ha A, Lee S, Mohajeri A, Schwartz C, Place HMWY. How you load: a scoping review of the determinants of orthodontic mini-implant success. Appl Sci. 2025;15(17):9673. doi:10.3390/app15179673
7. Jiang C, Pei F, Wu Y, et al. Investigation of three-rooted deciduous mandibular second molars in a Chinese population using cone-beam computed tomography. BMC Oral Health. 2022;22(1):329. PMID: 35941577; Central PMCID: PMC9361676. doi:10.1186/s12903-022-02378-w
8. Carlsen O, Alexandersen V. Radix entomolaris: identification and morphology. Scand J Dent Res. 1990;98(5):363–373. PMID: 2293344. doi:10.1111/j.1600-0722.1990.tb00986.x
9. Steelman R. Incidence of an accessory distal root on mandibular first permanent molars in Hispanic children. ASDC J Dent Child. 1986;53(2):122–123. PMID: 3457033.
10. Sperber GH, Moreau JL. Study of the number of roots and canals in Senegalese first permanent mandibular molars. Int Endod J. 1998;31(2):117–122. PMID: 9868938. doi:10.1046/j.1365-2591.1998.00126.x
11. Ferraz JA, Pécora JD. Three-rooted mandibular molars in patients of Mongolian, caucasian and Negro origin. Braz Dent J. 1993;3(2):113–117. PMID: 8241760.
12. Gu Y, Lu Q, Wang H, Ding Y, Wang P, Ni L. Root canal morphology of permanent three-rooted mandibular first molars--part I: pulp floor and root canal system. J Endod. 2010;36(6):990–994. PMID: 20478452. doi:10.1016/j.joen.2010.02.030
13. Yew SC, Chan K. A retrospective study of endodontically treated mandibular first molars in a Chinese population. J Endod. 1993;19(9):471–473. PMID: 8263456. doi:10.1016/S0099-2399(06)80536-4
14. Abella F, Patel S, Durán-Sindreu F, Mercadé M, Roig M. Mandibular first molars with disto-lingual roots: review and clinical management. Int Endod J. 2012;45(11):963–978. PMID: 22681628. doi:10.1111/j.1365-2591.2012.02075.x
15. Aung NM, Myint KK. Three-rooted permanent mandibular first molars: a meta-analysis of prevalence. Int J Dent. 2022;2022:9411076. PMID: 35386547; Central PMCID: PMC8979718. doi:10.1155/2022/9411076
16. Martins JNR, Gu Y, Marques D, Francisco H, Caramês J. Differences on the root and root canal morphologies between asian and white ethnic groups analyzed by cone-beam computed tomography. J Endod. 2018;44(7):1096–1104. PMID: 29861062. doi:10.1016/j.joen.2018.04.001
17. Armenta HB, Mireles AGR, Martinez JS, et al. Prevalence and classification of C-shaped canal and radix in mandibular molars using cone-beam computed tomography on Mexican population. Dent J. 2024;12(7):212. PMID: 39056999; Central PMCID: PMC11275415. doi:10.3390/dj12070212
18. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
19. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
20. Mahmood MA, Faris TM, Abdalrahim RH, Jalal RA. Anatomical relationship between the roots of erupted maxillary posterior teeth and maxillary sinus using CBCT in Sulaimani City (A Retrospective Study). Sulaimani Dent J. 2025;10(2):1–7. doi:10.17656/sdj.10168
21. Mohan S, Thakur J. Prevalence of radix entomolaris in India and its comparison with the rest of the world. Minerva Dent Oral Sci. 2022;71(2):117–122. PMID: 34755993. doi:10.23736/S2724-6329.21.04561-7
22. Javed MQ, Srivastava S, Alotaibi BBR, Bhatti UA, Abulhamael AM, Habib SR. A Cone beam computed tomography-based investigation of the frequency and pattern of radix entomolaris in the Saudi Arabian population. Medicina. 2023;59(11):2025. PMID: 38004074; Central PMCID: PMC10673087. doi:10.3390/medicina59112025
23. Talabani RM, Abdalrahman KO, Abdul RJ, Babarasul DO, Hilmi Kazzaz S. Evaluation of radix entomolaris and middle mesial canal in mandibular permanent first molars in an Iraqi subpopulation using cone-beam computed tomography. Biomed Res Int. 2022;2022:7825948. PMID: 35860794; Central PMCID: PMC9293536. doi:10.1155/2022/7825948
24. Martins Araújo de Oliveira Y, Mendes Gomes MC, Nascimento MFDS. Prevalence of radix molaris in mandibular molars of a subpopulation of Brazil’s Northeast region: a cross-sectional CBCT study. Sci Rep. 2025;15(1):22651. PMID: 40594628; Central PMCID: PMC12214600. doi:10.1038/s41598-025-06790-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.