Back to Journals » Patient Preference and Adherence » Volume 20
Prescriber- and Patient-Level Characteristics Associated with Patient Adherence to Any Antipsychotics Among Patients with Schizophrenia in the United States
Authors Voegel A, Naranjo RR Jr, Diaz L, Vanden Eynde C, Wang Y, Pilon D, Benson C, Citrome L ![]()
Received 30 September 2025
Accepted for publication 28 January 2026
Published 17 February 2026 Volume 2026:20 570441
DOI https://doi.org/10.2147/PPA.S570441
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Arthur Voegel,1 Ronaldo R Naranjo Jr,2 Lilian Diaz,3 Claire Vanden Eynde,3 Yuxi Wang,3 Dominic Pilon,3 Carmela Benson,2 Leslie Citrome4
1Analysis Group, Inc., New York, NY, USA; 2Johnson & Johnson, Titusville, NJ, USA; 3Analysis Group, ULC, Montreal, QC, Canada; 4Department of Psychiatry & Behavioral Sciences, New York Medical College, Valhalla, NY, USA
Correspondence: Arthur Voegel, Email [email protected]
Purpose: Antipsychotic (AP) medication adherence is important for the management of schizophrenia. This study thus aimed to evaluate prescriber- and patient-level characteristics and long-acting injectable (LAI) treatment use among patients with schizophrenia to determine the association between these factors and AP adherence.
Patients and methods: Adult patients with schizophrenia in the United States were identified from Komodo Research Data (01/01/2016-06/30/2023). Patients were required to have been initiated on an oral or LAI AP (index date) during the intake period (07/01/2021-06/30/2022), by a provider who prescribed APs to ≥ 6 patients with schizophrenia over the intake period (index prescriber). Providers were characterized using quartiles of the proportion of LAIs over all APs prescribed during the intake period (non-LAI prescribers; Q1: low, ≤ 8.5% LAIs; Q2-3: intermediate, > 8.5% and < 27% LAIs; Q4: high, ≥ 27% LAIs). Adherence to any AP (proportion of days covered ≥ 80%) was reported over the fixed 12-month follow-up period, and factors associated with adherence were evaluated using multivariate logistic regression.
Results: In total, 22,255 patients were included (mean age: 40.9; male: 66%; Medicaid: 76%). At index, 82% and 18% of patients were initiated on an oral AP or LAI, respectively, with 10%, 21%, 47%, and 22% of index APs prescribed by non-, low-, intermediate-, and high-LAI prescribers, respectively. Prescription of the index AP by an intermediate- or high- LAI prescriber was associated with 39% and 63% higher odds of adherence, respectively, relative to non-LAI prescribers (both p< 0.001). Prescription of an LAI versus oral index AP was associated with 25% higher odds of adherence (p< 0.001). Patients of all racial/ethnic minorities had lower odds of adherence relative to White patients (all p< 0.050).
Conclusion: Adherence was higher among patients treated by high-LAI prescribers, indicating that familiarity with LAI treatment and awareness of adherence challenges may improve adherence rates among patients with schizophrenia.
Keywords: claims data, long-acting injectable, mental health, real-world outcomes
Background
Schizophrenia is a severe and chronic mental illness characterized by periods of delusions and hallucinations that begin in early adulthood.1,2 Affecting an estimated 0.31% to 0.64% of the United States (US) population, schizophrenia is associated with significant humanistic and economic burden due to its severe and often persistent symptoms.3–6 The American Psychiatric Association practice guidelines for schizophrenia recommend the use of antipsychotic (AP) medication, in addition to non-pharmacologic therapy, as part of a person-centered treatment plan.7 Long-term treatment for schizophrenia is often required and, consequently, AP adherence is important for managing symptoms, preventing relapses, and reducing healthcare costs.7–9
Several patient-level characteristics are associated with AP adherence rates, including both individual factors, such as age, depressive symptoms, insight into one’s illness, attitudes towards medications, substance use disorders, and comorbid physical illness, and social factors, such as income, education, and quality of life.10–13 In addition, the route of administration can also influence AP adherence. Although oral APs are commonly prescribed, they may pose adherence challenges due to the need for daily dosing.14 Conversely, long-acting injectable (LAI) APs are recommended for patients with adherence concerns and offer extended dosing intervals, with the once-every-6-months paliperidone palmitate (PP6M) offering the longest dosing interval.7,15
Real-world evidence has consistently shown that patients with schizophrenia treated with LAIs have better treatment adherence, improved clinical outcomes, and reduced healthcare resource utilization (HRU) compared to those receiving oral APs.16–21 Nevertheless, LAIs remain underutilized; among Medicaid beneficiaries who make up over 75% of the population of patients with schizophrenia in the US, only approximately 13% of patients with schizophrenia are prescribed an LAI.22,23 Clinician surveys have identified several factors underlying limited LAI use that include concerns over cost, administration logistics, stigmatization, adverse events, presumed adherence to oral APs, nonacceptance of LAI treatment, and the perception that LAIs should be reserved for later stages of illness, among other factors.24–26 Clinicians who prescribe LAIs more frequently report greater education on current LAI treatment guidelines within their practice and greater confidence in discussing and administering LAI treatment.24,25
Yet, broader real-world prescriber level factors remain understudied in the context of antipsychotic treatment for schizophrenia. Gaining a better understanding of prescriber-level characteristics may be important for identifying opportunities to support adherence and improve outcomes for individuals with schizophrenia. To address this gap, the present study evaluates how prescriber-level characteristics, beyond route of administration and patient-level factors, are associated with AP adherence among individuals with schizophrenia in the United States.
Methods
Data Source
Closed claims data spanning the period January 1, 2016, to June 30, 2023 were obtained from Komodo Research Data (KRD). Prior studies in mental health have used various claims databases to explore impacts of prescriber- and patient-level characteristics on prescribing patterns and treatment adherence in real-world settings.27–29 KRD specifically offers a robust, real-world data source with prescriber- and patient-level variables relevant for examining factors related to treatment adherence in schizophrenia, capturing a large and diverse population of providers and patients across a wide range of clinical practice settings. Closed claims from KRD account for over 170 million patient lives and are sourced directly from over 150 payers, including commercial, Medicare Advantage, and Medicaid payers, allowing to assess the complete patient journey during closed claims eligibility periods. KRD comprises diverse patient populations and contains comprehensive information on payer type, patient demographics, diagnoses and procedures, place of service, and prescription fills, including days of supply, quantity, and claim rejection status. Prescriber information is also available, including unique identifiers (hashed National Provider Identifiers [NPIs]), specialty, and 5-digit ZIP codes. KRD prescriber information was complemented with Center for Disease Control (CDC)30 Social Vulnerability Index (SVI) and rural-urban commuting area (RUCA)31 data to characterize the environment of the prescriber’s practice location. The SVI is a relative and continuous composite measure ranging from 0–1 incorporating components of poverty, unemployment, education level, minority status, and access to housing and transportation, with greater values reflecting greater social vulnerability.32 The RUCA codes classify US census tracts using measures of population density, urbanization, and daily commuting. RUCA codes range from 1 (metropolitan areas) to 10 (rural areas) and were classified in this study as urban (codes 1 to 6 indicating metropolitan to micropolitan areas) or rural (codes 7 to 10 indicating small town to rural areas).31
This study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514.
Study Design
Study Periods and Design
A retrospective cohort design was used to evaluate adherence to AP medications among adult patients with schizophrenia. The intake period spanned from July 1, 2021, to June 30, 2022, with the index date defined as the date of a newly initiated oral or LAI AP during the intake period (see Appendix Box 1 for full list of APs). Among patients with multiple qualifying index dates after applying all selection criteria, one index date was randomly selected. The baseline period was defined as 12 months preceding the index date and was used to describe patient characteristics, including demographics and presence of comorbidities. The follow-up period included the index date and the subsequent 12 months and was used to assess patient adherence to any APs.
Sample Selection
Patient Inclusion Criteria
Eligible patients with schizophrenia were selected for the study if they (i) had ≥2 outpatient claims on different dates or ≥1 inpatient claim with a diagnosis of schizophrenia (International Classification of Diseases, 10th Revision, Clinical Modification [ICD-10-CM]: F20.X, F21), with ≥1 claim prior to or on the index date, (ii) were ≥18 years at the start of the intake period, (iii) had initiated a new oral AP or LAI during the study intake period (ie, no claims for the index AP in the 12 months preceding the index date), (iv) had ≥12 months of continuous insurance, Medicare, or Medicaid eligibility both pre- and post-index, (v) had no diagnosis for bipolar disorder or pregnancy during the baseline period, and (vi) had an index AP prescriber who had prescribed to ≥6 patients with schizophrenia during the study intake period.
Prescriber Selection
Among patients meeting the selection criteria for this sample, the associated index AP prescribers were analyzed. While there is no established consensus in the literature on what constitutes sufficient prescribing experience in the treatment of schizophrenia, this data-driven approach was informed by the observed distribution of prescribing volumes among all patients with schizophrenia, and was selected to ensure the inclusion of a diverse and representative sample of prescribers across specialties, including psychiatrists, psychiatric nurse practitioners, and primary care physicians (PCPs), such as those in general practice, family medicine, and internal medicine, while maintaining sufficient prescribing volume to assess prescribing patterns.
As there are currently no standardized or clinically established criteria for classifying LAI prescribing patterns, a data distribution–based approach was used to classify prescribers based on their LAI prescribing ratio to all types of antipsychotics. This ratio ranges from 0 to 1, with higher values potentially reflecting greater ease or familiarity in prescribing LAIs to patients with schizophrenia, and lower values reflecting more selective LAI use. Quartiles of this ratio were used for stratification, as quartiles are widely used statistical thresholds that create transparent and reproducible categories and help ensure groups with adequate and reasonably balanced sample sizes. Accordingly, AP prescribers were categorized into 1 of 4 LAI prescribing patterns based on the proportion of LAIs to all types of APs prescribed to patients with schizophrenia during the intake period as follows: no LAI prescribed, low-LAI prescribers (first quartile [Q1], ≤8.5% LAIs), intermediate-LAI prescribers (second and third quartiles [Q2–Q3], >8.5% and <27% LAIs), high-LAI prescribers (fourth quartile [Q4], ≥27% LAIs).
Patient Characteristics
Patient demographic characteristics were evaluated on the index date and included age, sex, race, geographic region, and payer type. Patient clinical characteristics were evaluated in the 12-month period prior to the index date and included Quan-Charlson Comorbidity Index (Quan-CCI), number of comorbidities per the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision (DSM-5-TR), number of unique AP agents used, and presence of schizophrenia-related outpatient, emergency department, and inpatient visits. Index AP type was assessed on the index date.
Prescriber Characteristics
Prescriber characteristics were reported over the study intake period and included region of practice, specialty, practice setting (ie, rural or urban), and types of APs prescribed over the study intake period. Prescriber characteristics were evaluated at both the prescriber-level (eg, proportion of prescribers practicing in a particular region) and patient-level (eg, proportion of patients with an index AP prescriber from a particular region).
Outcome Measure
The primary study outcome was adherence to any AP reported over the fixed 12-month follow-up period. Adherence was defined as having a proportion of days covered (PDC) with any AP of ≥80%. More specifically, patients were considered adherent to APs if ≥80% of days over the fixed 12-month follow-up period were covered by an AP medication, based on AP days of supply.
Statistical Analysis
To assess patient and AP prescriber baseline characteristics, continuous variables were described with means, standard deviations, and medians, and categorical variables with frequencies and proportions.
A multivariate logistic regression at the patient level was used to evaluate index prescriber- and patient-related characteristics associated with adherence, reported using odds ratios (ORs), 95% confidence intervals (CIs), and p-values. Independent variables that may be associated with adherence outcomes were included in the model, comprising prescriber-related (LAI prescribing patterns, specialty, practice setting, and social vulnerability index), patient-related (age at index date, sex, region, payer type, Quan-CCI, DSM-5-TR comorbidities), and treatment related factors (index AP type, number of unique AP agents received in baseline, schizophrenia-related outpatient and emergency department visits; see Appendix Table 1 for the full list of variables included). All variables were included in the model, without further selection, to ensure that a comprehensive list of potential confounders was controlled for. To account for potential correlations in outcomes among patients treated by the same prescriber, generalized estimating equations were used with clustering at the prescriber level.
All statistical analyses were conducted using SAS version 8.3 (SAS Institute, Inc., Cary, NC).
Results
AP Prescriber Characteristics
A total of 10,826 prescribers were included in the study. Prescribers practiced in diverse regions across the US (South, 31.9%; West, 25.0%; Northeast, 22.7%; Midwest, 20.4%), predominantly (97.4%) in urban settings with a mean [median] SVI of 0.66 [0.73]. Almost half (49.2%) of the prescribers were psychiatrists, followed by psychiatric nurse practitioners (25.9%) and PCPs (11.7%) (Figure 1).
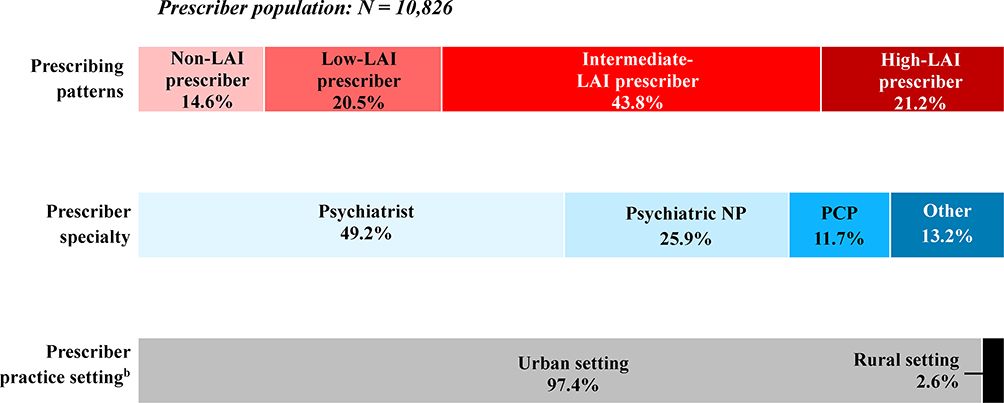 |
Figure 1 Prescriber characteristics.a Abbreviations: AP, antipsychotic; LAI, long-acting injectable; NP, nurse practitioner; PCP, primary care physician; SD, standard deviation; SVI, Social Vulnerability Index. Notes: a The proportions presented in Figure 1 are calculated at the prescriber level, representing the share of prescribers in each category out of the 10,826 prescribers included in the study. b Rural and urban areas were defined using Rural-Urban Commuting Area.33 The rural/urban classification were determined based on the ZIP code of the index AP prescriber’s practice location. |
Nearly all prescribers (99.3%) prescribed an oral AP during the study intake period, and 85.4% prescribed an LAI. Among prescribers who had prescribed ≥1 LAI during the intake period, the mean [median] proportion of LAIs to all types of APs was 19.6% [16.7%], and the majority (94.6%) prescribed a second-generation LAI. Nearly half (43.8%) were intermediate-LAI prescribers, 21.2% were high-LAI prescribers, 20.5% were low-LAI prescribers (Figure 1).
Among high-LAI prescribers, the mean [median] proportion of LAIs to all types of APs was 39.2% [35.5%], with 1.1% prescribing LAIs exclusively.
Patient Baseline Characteristics
A total of 22,255 patients met the eligibility criteria and were included in the study (Table 1). The patient mean (SD) age was 40.9 (14.3) years, and most were male (66.0%). Patients were racially and ethnically diverse (White, 31.3%; Black or African American, 31.3%; Hispanic or Latino, 17.2%) and geographically distributed across US regions (West, 29.7%; South, 29.3%; Northeast, 20.8%; Midwest, 20.2%). Nearly all patients were covered by Medicaid (76.2%) or Medicare Advantage (14.4%).
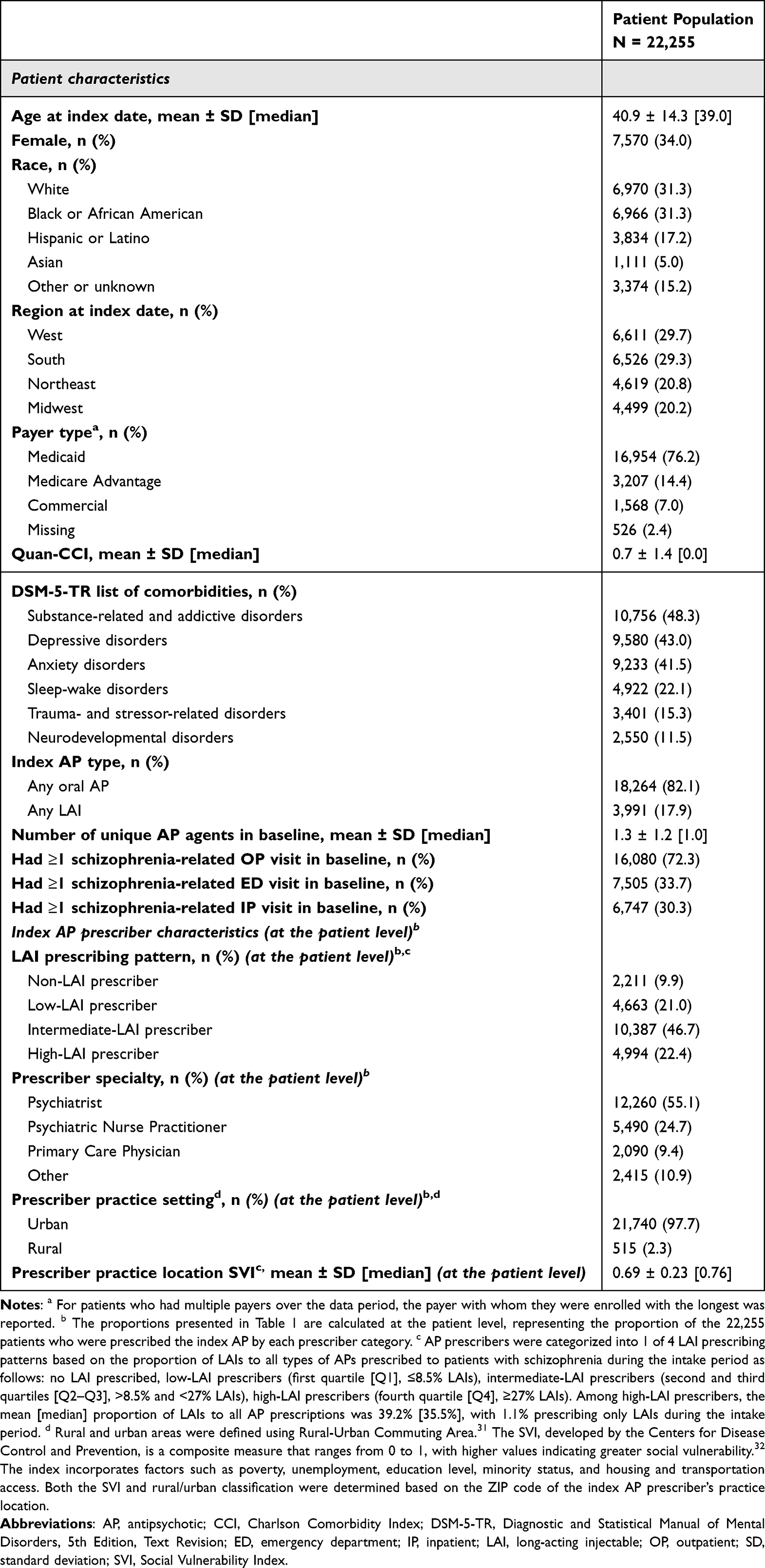 |
Table 1 Patient Baseline Characteristics |
During the baseline period, nearly half of patients had substance-related and addictive disorders (48.3%), depressive disorders (43.0%), or anxiety disorders (41.5%). At index, 82.1% of patients were initiated on an oral AP and 17.9% were initiated on an LAI, of which 78.3% received a second-generation LAI.
Nearly half of patients (46.7%) were prescribed their index AP by an intermediate-LAI prescriber, followed by 22.4% by high-LAI prescribers, 21.0% by low-LAI prescribers, and 9.9% by non-LAI prescribers. Of the 3,991 patients prescribed an LAI at index, 8.6%, 18.7%, and 32.9% were prescribed by a low-, intermediate-, and high-LAI index prescriber, respectively.
More than half of patients were prescribed an index AP by a psychiatrist (55.1%), followed by psychiatric nurse practitioners (24.7%), other specialty types (10.9%), and PCPs (9.4%) (Table 1).
Adherence to Any AP
Overall, 49.5% of patients were adherent to any AP at 12-month follow-up (Figure 2). Adherence trended higher with increasing LAI use among index AP prescribers, ranging from the lowest adherence among patients prescribed the index AP (38.7%) by non-LAI prescribers to the highest adherence among patients prescribed the index AP by high-LAI prescribers (56.0%).
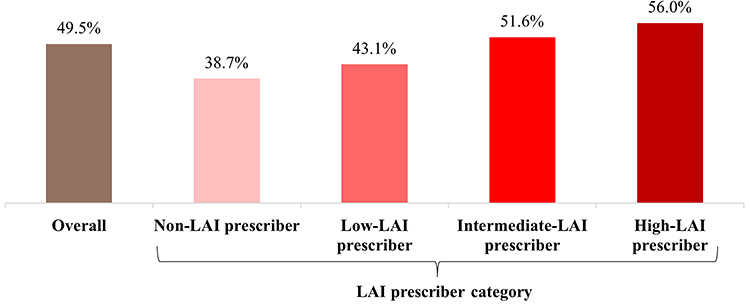 |
Figure 2 Proportion of patients adherenta to any AP at 12 months, by LAI prescriber category.b Abbreviations: AP, antipsychotic; LAI, long-acting injectables; PDC, proportion of days covered. Notes: a Adherence to any AP was defined as having a PDC with any AP ≥80%. PDC was defined as the sum of non-overlapping days of supply divided by a fixed 12-month period. b Figure 2 presents patient-level adherence proportions, indicating the percentage of patients who remained adherent to any AP at 12 months, overall and stratified by the prescriber category of the index AP. |
Characteristics Associated with Adherence
Index AP Prescriber Characteristics
Prescription of the index AP by an intermediate- or high-LAI prescriber was associated with 39% and 63% higher odds of adherence, respectively, relative to prescription by a non-LAI prescriber (both p<0.001; Figure 3). Higher SVI at the prescriber’s location was significantly associated with lower odds of adherence (p<0.001). Relative to patients whose index AP was prescribed by psychiatrists, adherence did not differ significantly for those prescribed by psychiatric nurse practitioners or PCPs, whereas those prescribed by other specialties (eg, emergency medicine, hospitalists) had significantly lower odds of adherence (OR: 0.89; p=0.021).
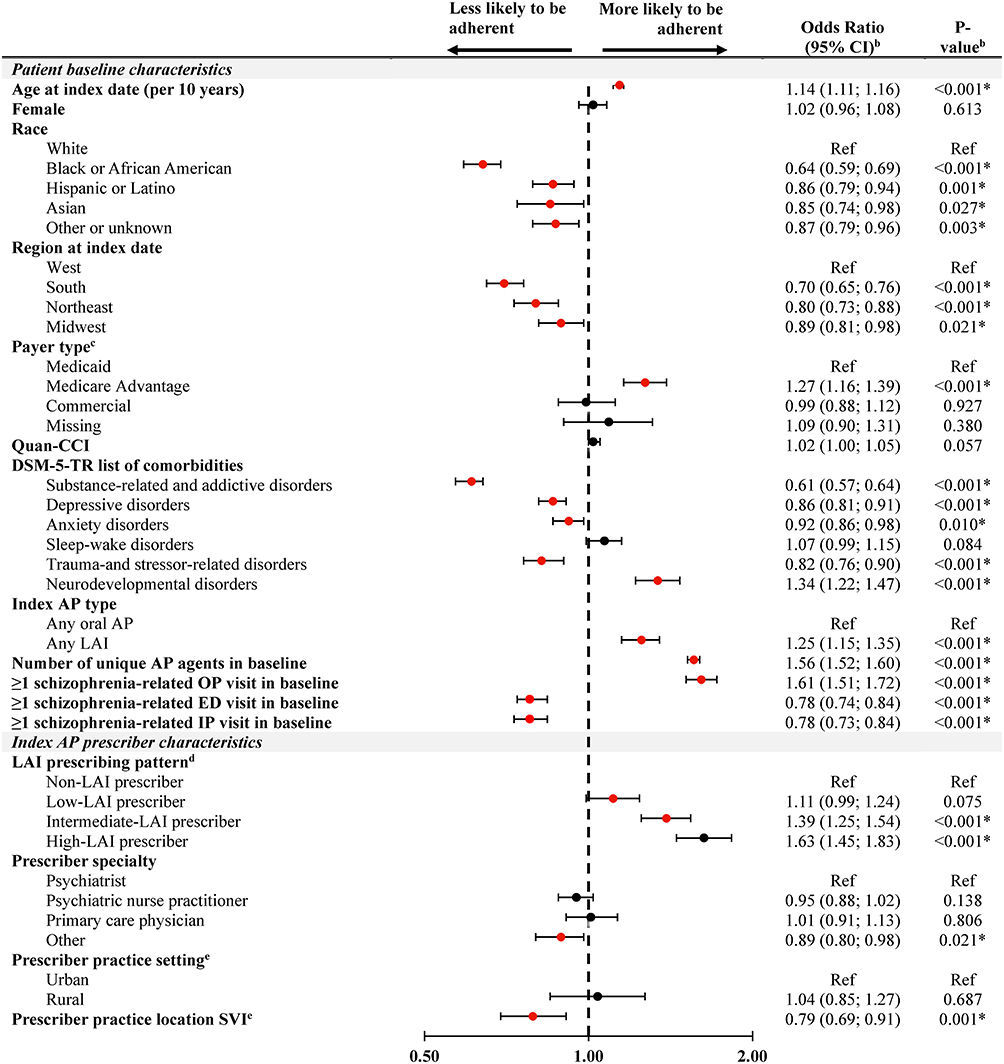 |
Figure 3 Prescriber- and patient-related characteristics associated with patient adherence (PDC ≥ 80%)a to any AP at 12-months. Abbreviations: AP, antipsychotic; CCI, Charlson Comorbidity Index; CI, confidence interval; DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision; ED, emergency department; IP, inpatient; LAI, long-acting injectable; OP, outpatient; PDC, proportion of days covered; Ref, reference category; SD, standard deviation; SVI, Social Vulnerability Index. Notes: * and red dots indicate statistical significance at 5%. a PDC was defined as the sum of non-overlapping days of supply divided by a fixed period of 12 months. b Odds ratios and p-values were generated using logistic regression models. c For patients who had multiple payers over the data period, the payer with whom they were enrolled with the longest was reported. d AP prescribers were categorized into 1 of 4 LAI prescribing patterns based on the proportion of LAIs to all types of APs prescribed to patients with schizophrenia during the intake period as follows: no LAI prescribed, low-LAI prescribers (first quartile [Q1], ≤8.5% LAIs), intermediate-LAI prescribers (second and third quartiles [Q2–Q3], >8.5% and <27% LAIs), high-LAI prescribers (fourth quartile [Q4], ≥27% LAIs). Among high-LAI prescribers, the mean [median] proportion of LAIs to all AP prescriptions was 39.2% [35.5%], with 1.1% prescribing only LAIs during the intake period. e Rural and urban areas were defined using Rural-Urban Commuting Area.33 The SVI, developed by the Centers for Disease Control and Prevention, is a composite measure that ranges from 0 to 1, with higher values indicating greater social vulnerability.32 The index incorporates factors such as poverty, unemployment, education level, minority status, and housing and transportation access. In this study, the mean ± SD [median] SVI in the area of the index AP prescribers was 0.69 ± 0.23 [0.76], based on the 2022 index.30 Both the SVI and rural/urban classification were determined based on the ZIP code of the index AP prescriber’s practice location. |
Index Treatment
Prescription of an LAI as the index AP was associated with 25% higher odds of adherence relative to prescription of an oral AP (p<0.001).
Patient Demographics, Clinical Characteristics, and AP Treatment History
Older age was associated with 14% higher odds of adherence (p<0.001). Relative to White patients, all racial and ethnic minorities had lower odds of adherence, with the lowest odds of adherence observed among Black or African American patients (p<0.001).
Substance-related and addictive disorders, depressive disorders, anxiety disorders, and trauma- and stressor-related disorders were each associated with lower odds of adherence, whereas neurodevelopmental disorders were associated with higher odds of adherence (all p<0.050).
Each additional unique AP agent used during the baseline period was associated with 56% higher odds of adherence (p<0.001). A schizophrenia-related emergency department visit or hospitalization during the baseline period were each associated with 24% lower odds of adherence, while an outpatient visit during the baseline period was associated with 61% higher odds of adherence (all p<0.001).
Discussion
This real-world retrospective study assessed prescriber- and patient-related characteristics associated with AP medication adherence among patients with schizophrenia in the US. Over a 12-month follow-up period, only about half of patients were adherent (PDC ≥80%) to any AP medication. Notably, patients treated by intermediate- or high-LAI prescribers had greater odds of adherence compared to those treated by non-LAI prescribers, and patients prescribed an LAI as the index AP demonstrated higher adherence than those prescribed an oral AP. Conversely, lower odds of adherence were observed among certain patient subgroups, including those with comorbid disorders and individuals from racial or ethnic minorities. Together, these findings highlight the potential influence of prescriber- and patient-level characteristics on AP adherence among patients with schizophrenia and may suggest a need for greater prescriber awareness regarding LAI use in this population.
The adherence rate observed in the present study aligns with existing evidence and underscores the persistent challenges associated with treating schizophrenia. In the current analysis, 50% of patients were adherent to any AP over the 12-month follow-up period. A previous national description of Medicaid beneficiaries with schizophrenia reported an adherence rate of 56%, while prior studies have documented non-adherence rates ranging between 34% and 81%.34
Initiating an LAI versus an oral AP as the index treatment was associated with higher odds of adherence, supporting prior evidence that LAIs reduce the burden of daily medication-taking required for oral AP treatment, thereby improving adherence.17,34,35 However, despite their adherence benefits and their equivalent or superior efficacy and safety compared to oral APs,36 LAIs are relatively infrequently prescribed, and estimates vary by study. Analyses of Medicaid and Medicare beneficiaries estimated approximately 13% and 20% of patients with schizophrenia being prescribed an LAI, respectively.22,37 This gap highlights the need to alleviate barriers to LAIs, which may include logistical challenges that may be reduced with longer-acting formulations (ie, every 2, 3, or 6 months), as well as prescribers’ perception and education on the latest LAIs.22 By contrast, higher use has been observed in specific contexts; one study of community mental health centers in South Carolina found that 52% of patients with schizophrenia were prescribed an LAI.38 Although not nationally representative, these findings could suggest that greater uptake may be achievable in outpatient systems with established infrastructure to support LAI administration.
The odds of AP adherence increased with greater use of LAIs by the index prescriber, regardless of whether the index treatment was an oral AP or an LAI. This finding may reflect greater familiarity with clinical guidelines and current treatment options among intermediate- and high-LAI prescribers compared to low- and non-LAI prescribers, as well as a greater ability to recognize patients at risk of poor adherence.24 Intermediate- and high-LAI prescribers may also be more confident in discussing the benefits of LAIs and addressing patient concerns.24 Conversely, low LAI use may reflect prescriber beliefs that act as barriers to LAI prescribing, such as concerns about cost, stigma, adverse events, logistics of administration, anticipated patient nonacceptance, or the perception that LAIs are only appropriate for patients with adherence issues or severe symptoms.24–26 Despite these barriers, a recent US-based survey found that low-LAI and LAI-hesitant prescribers were motivated to use LAIs, suggesting that targeted education and support could help expand LAI prescribing.24 Notably, even among high-LAI prescribers, half prescribed LAIs for 35.5% or fewer of their AP prescriptions, underscoring continued opportunities to increase LAI use within this group.
Prescriber specialty was also associated with AP adherence. Patients who were prescribed the index AP by providers other than a psychiatrist, psychiatric nurse practitioner, or PCP, such as an emergency medicine provider or hospitalist, had lower odds of adherence to any AP at 12 months. Such instances may reflect treatment that was initiated in a non-specialized acute care setting, where limited follow-up, lack of provider continuity, or both may have contributed to poor AP adherence. Indeed, prior studies have shown that reduced continuity and challenges in care coordination contribute to suboptimal or unsafe hospital discharge care for up to 1 in 5 patients.39–41 Involving psychiatric specialists or PCPs in AP prescribing may therefore help promote more continuous and coordinated care, supporting ongoing medication adherence.42,43
Additionally, comorbidities such as substance use and depressive and anxiety disorders were associated with lower odds of adherence. These conditions can complicate illness management and may reduce patients’ motivation or ability to maintain a treatment routine, leading to reduced adherence rates.44,45 Finally, adherence odds were higher among older patients and those with neurodevelopmental disorders, potentially due to greater illness insight among older adults and increased caregiver support in both cases.13
Patients whose index prescribers were located in more socially vulnerable areas had lower odds of adherence, consistent with prior studies linking adverse social determinants of health to poorer medication adherence.46,47 Social vulnerability in the present study was assessed using the SVI, a measure designed by the Centers for Disease Control and Prevention to identify and quantify social vulnerability across US communities,30 and which has been consistently used to demonstrate the relationship between social determinants of health and health outcomes.48 Lower odds of adherence was also observed among racial and ethnic minority groups, aligning with well-documented racial and ethnic differences in medication adherence driven by disparities in affordability and access.49 This finding further highlights potential systemic barriers associated with AP adherence among patients with schizophrenia.
Limitations
This study was associated with several limitations. First, data were obtained from administrative claims sources and thus inaccuracies in diagnosis, procedure, or medication coding may have led to misclassifications. Second, prescription fills do not account for whether dispensed medication was taken as prescribed, limiting the ability to measure true adherence. This may have been more applicable to patients prescribed an oral AP as the index treatment, where daily adherence is more difficult to track. Subsequently, oral AP adherence may have been overestimated while the difference in adherence between patients initiated on an LAI versus an oral AP may have been underestimated. Third, the results may be subject to residual confounding due to unmeasured factors such as the patient–prescriber relationship, prescriber experience or training, and patient preferences or beliefs about treatment. Notably, prescriber age, years in practice, experience, and prior exposure to LAI continuing medical education were not available in the data and may have shaped prescribing decisions, as exposure to treatment guidelines, standards of care, and availability of LAI formulations has varied over time.50 Future research is warranted to further explore these associations. Fourth, the thresholds used to categorize AP prescribers were statistically rather than clinically defined and therefore may not map directly onto clinical practice. Nonetheless, the clear adherence gradient observed across the non-, low-, intermediate-, and high-LAI prescriber groups suggests that this stratification captured meaningful differences in practice patterns. Exploring alternate, clinically informed approaches to defining prescriber categories represent an additional area of future research. Fifth, as all patients in the KRD were insured, results may not be generalizable to the uninsured population. Finally, while the restriction to only include patients whose index AP prescriber had prescribed to ≥6 patients with schizophrenia during the intake period was data driven, this may further limit generalizability to the broader population of AP prescribers and their patients with schizophrenia.
Conclusion
Irrespective of the mode of administration, patients with schizophrenia treated by high-LAI prescribers had significantly higher rates of AP adherence over 12 months, suggesting that prescribing patterns and familiarity with LAIs influence patient adherence rates. The results also support that initiating an LAI versus an oral AP may increase adherence, further demonstrating the potential of LAIs to improve outcomes in schizophrenia management. Disparities in adherence observed among patients in areas with higher social vulnerability and among racial and ethnic minority groups highlight a potential health equity gap in schizophrenia care that warrants further investigation.
Previous Presentations
Part of the material in this manuscript was presented at the American Society of Clinical Psychopharmacology (ASCP) held May 27-29, 2025, in Scottsdale, AZ as a poster presentation.
Data Sharing Statement
The data that supports the findings of this study are available from Komodo Health. Restrictions apply to the availability of these data, which were used under license for this study.
Ethics Statement
The study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514.
Acknowledgments
Medical writing assistance was provided by professional medical writer, Molly Gingrich, MSc, an employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Johnson & Johnson, which funded the development and conduct of this study and manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is the conception, study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Johnson & Johnson. The study sponsor was involved in several aspects of the research, including the study design, interpretation of data, and writing of the manuscript. All authors contributed to the development of the manuscript and maintained control over the final content.
Disclosure
CB and RRN are employees of Johnson & Johnson. AV, LD, CV, YW and DP are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Johnson & Johnson, which funded the development and conduct of this study. LC reports personal consulting fees from AbbVie/Allergan, Acadia, Adamas, Adheretech, Alkermes, Alumis, Angelini, Astellas, Autobahn, Avanir, Axsome, Biogen, BioXcel, Bristol-Myers Squibb, Boehringer Ingelheim, Cadent Therapeutics, Cerevel, Clinilabs, COMPASS, Delpor, Draig Therapeutics, Eisai, Enteris BioPharma, HLS Therapeutics, Idorsia, INmune Bio, Impel, Intra-Cellular Therapies, Janssen, Karuna, Lundbeck, Luye, Lyndra, MapLight, Marvin, Medavante-ProPhase, Merck, Mitsubishi-Tanabe Pharma, Neumora, Neurocrine, Neurelis, Noema, Novartis, Noven, Otsuka, Ovid, Praxis, Recordati, Relmada, Reviva, Sage, Sumitomo/Sunovion, Supernus, Teva, University of Arizona, Vanda, Wells Fargo, and oneoff ad hoc consulting for individuals/entities conducting marketing, commercial, or scientific scoping research; speakers bureau for AbbVie/Allergan, Acadia, Alkermes, Angelini, Axsome, BioXcel, Bristol-Myers Squibb, Eisai, Idorsia, Intra-Cellular Therapies, Janssen, Lundbeck, Neurocrine, Neopharm, Noven, Otsuka, Recordati, Sage, Sunovion, Takeda, Teva, Vanda, and CME activities organized by medical education companies such as Medscape, NACCME, NEI, Vindico, and universities and professional organizations/societies; stocks in Bristol Myers Squibb, Eli Lilly, Johnson & Johnson, Merck, and Pfizer; stock options in Reviva; and royalties/publishing income from Taylor & Francis, Wiley, UpToDate, Springer Healthcare, and Elsevier. The authors report no other conflicts of interest in this work.
References
1. Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5. Schizophr Res. 2013;150(1):3–13. doi:10.1016/j.schres.2013.05.028
2. McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia-An overview. JAMA Psychiatry. 2020;77(2):201–210. doi:10.1001/jamapsychiatry.2019.3360
3. Kessler RC, Birnbaum H, Demler O, et al. The prevalence and correlates of nonaffective psychosis in the National Comorbidity Survey Replication (NCS-R). Biol Psychiatry. 2005;58(8):668–676. doi:10.1016/j.biopsych.2005.04.034
4. Wu EQ, Shi L, Birnbaum H, Hudson T, Kessler R. Annual prevalence of diagnosed schizophrenia in the USA: a claims data analysis approach. Psychol Med. 2006;36(11):1535–1540. doi:10.1017/S0033291706008191
5. Desai PR, Lawson KA, Barner JC, Rascati KL. Estimating the direct and indirect costs for community-dwelling patients with schizophrenia. J Pharm Health Serv Res. 2013;4(4):187–194. doi:10.1111/jphs.12027
6. Millier A, Schmidt U, Angermeyer MC, et al. Humanistic burden in schizophrenia: a literature review. J Psychiatr Res. 2014;54:85–93. doi:10.1016/j.jpsychires.2014.03.021
7. Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association practice guideline for the treatment of patients with schizophrenia. Am J Psychiatry. 2020;177(9):868–872. doi:10.1176/appi.ajp.2020.177901
8. Acosta FJ, Hernández JL, Pereira J, Herrera J, Rodríguez CJ. Medication adherence in schizophrenia. World J Psychiatry. 2012;2(5):74–82. doi:10.5498/wjp.v2.i5.74
9. Martin A, Bessonova L, Hughes R, et al. Systematic review of real-world treatment patterns of oral antipsychotics and associated economic burden in patients with schizophrenia in the United States. Adv Ther. 2022;39(9):3933–3956. doi:10.1007/s12325-022-02232-z
10. Misdrahi D, Dupuy M, Dansou Y, et al. Predictors of medication adherence in a large 1-year prospective cohort of individuals with schizophrenia: insights from the multicentric FACE-SZ dataset. Transl Psychiatry. 2023;13(1):341. doi:10.1038/s41398-023-02640-x
11. Guo J, Lv X, Liu Y, Kong L, Qu H, Yue W. Influencing factors of medication adherence in schizophrenic patients: a meta-analysis. Schizophrenia. 2023;9(1):31. doi:10.1038/s41537-023-00356-x
12. Kim J, Ozzoude M, Nakajima S, et al. Insight and medication adherence in schizophrenia: an analysis of the CATIE trial. Neuropharmacology. 2020;168:107634. doi:10.1016/j.neuropharm.2019.05.011
13. Kaur S, Baby RS, Padhy SK. Effectiveness of caregiver intervention for improving medication adherence on level of medication adherence and attitude toward medications among nonadherent patients with mental illness. Indian J Psychiatric Nurs. 2023;20(2):103–110. doi:10.4103/iopn.iopn_6_23
14. Zacker C, Puckett JT, Kamal-Bahl S. Real-world adherence and discontinuation of oral antipsychotics and associated factors in a national sample of US Medicare beneficiaries with schizophrenia. Clinicoecon Outcomes Res. 2024;16:567–579. doi:10.2147/ceor.S469001
15. Janssen Pharmaceutical Companies. Paliperidone palmitate highlights of prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/207946s017,022264s038,021999Ss40s041lbl.pdf.
16. Lin D, Thompson-Leduc P, Ghelerter I, et al. Real-world evidence of the clinical and economic impact of long-acting injectable versus oral antipsychotics among patients with schizophrenia in the United States: a systematic review and meta-analysis. CNS Drugs. 2021;35(5):469–481. doi:10.1007/s40263-021-00815-y
17. Pilon D, Tandon N, Lafeuille MH, et al. Treatment patterns, health care resource utilization, and spending in Medicaid beneficiaries initiating second-generation long-acting injectable agents versus oral atypical antipsychotics. Clin Ther. 2017;39(10):1972–85e2. doi:10.1016/j.clinthera.2017.08.008
18. Mathews M, Gopal S, Singh A, et al. Comparison of relapse prevention with 3 different paliperidone formulations in patients with schizophrenia continuing versus discontinuing active antipsychotic treatment: a post-hoc analysis of 3 similarly designed randomized studies. Neuropsychiatr Dis Treat. 2020;16:1533–1542. doi:10.2147/NDT.S221242
19. Marcus SC, Zummo J, Pettit AR, Stoddard J, Doshi JA. Antipsychotic adherence and rehospitalization in schizophrenia patients receiving oral versus long-acting injectable antipsychotics following hospital discharge. J Manag Care Spec Pharm. 2015;21(9):754–768. doi:10.18553/jmcp.2015.21.9.754
20. Correll CU, Citrome L, Haddad PM, et al. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J Clin Psychiatry. 2016;77(suppl 3):1–24. doi:10.4088/JCP.15032su1
21. Correll CU, Benson C, Emond B, et al. Comparison of clinical outcomes in patients with schizophrenia following different long-acting injectable event-driven initiation strategies. Schizophrenia. 2023;9(1):9. doi:10.1038/s41537-023-00334-3
22. Patel C, Pilon D, Gupta D, et al. National and regional description of healthcare measures among adult Medicaid beneficiaries with schizophrenia within the United States. J Med Econ. 2022;25(1):792–807. doi:10.1080/13696998.2022.2084234
23. Kadakia A, Catillon M, Fan Q, et al. The economic burden of schizophrenia in the United States. J Clin Psychiatry. 2022;83(6). doi:10.4088/JCP.22m14458
24. Velligan D, Salinas GD, Belcher E, et al. Clinician differences in attitudes and perceptions on the use of long-acting injectable antipsychotic agents in treating patients with schizophrenia: results from the US DECIDE survey. BMC Psychiatry. 2025;25(1):232. doi:10.1186/s12888-025-06565-1
25. Zhdanava M, Starr HL, Lefebvre P, et al. Understanding the health system conditions affecting the use of long-acting injectable antipsychotics in the treatment of schizophrenia in clinical practice: a US healthcare provider survey. Neuropsychiatr Dis Treat. 2022;18:1479–1493. doi:10.2147/ndt.S369494
26. Schwartz S, Carilli C, Mian T, Ruekert L, Kumar A. Attitudes and perceptions about the use of long-acting injectable antipsychotics among behavioral health practitioners. Ment Health Clin. 2022;12(4):232–240. doi:10.9740/mhc.2022.08.232
27. Hijazi BM, Popovici I, Nusair MB, Alvarez G. Patterns and factors associated with SSRI medication adherence: a retrospective study using pharmacy claims data. J Pharm Health Serv Res. 2023;14(4):392–400. doi:10.1093/jphsr/rmad041
28. Tang Y, Horvitz-Lennon M, Gellad WF, et al. Prescribing of clozapine and antipsychotic polypharmacy for schizophrenia in a large Medicaid program. Psychiatr Serv. 2017;68(6):579–586. doi:10.1176/appi.ps.201600041
29. Young GJ, Zhu T, Hasan MM, Alinezhad F, Young LD, Noor EAM. Patient outcomes following buprenorphine treatment for opioid use disorder: a retrospective analysis of the influence of patient- and prescriber-level characteristics in Massachusetts, USA. Addiction. 2025;120(1):152–163. doi:10.1111/add.16684
30. Agency for Toxic Substances and Disease Registry. CDC/ATSDR SVI Fact Sheet. Available from: https://www.atsdr.cdc.gov/place-health/php/svi/svi-fact-sheet.html.
31. U.S. Department of Agriculture Rural-Urban Commuting Area Codes; 2023.
32. Centers for Disease Control and Prevention/Agency for Toxic Substances and Disease Registry/Geospatial Research A, and Services Program. CDC/ATSDR Social Vulnerability Index [2022]. Available from: https://www.atsdr.cdc.gov/place-health/php/svi/svi-data-documentation-download.html.
33. U.S. Department of Housing and Urban Development. HUD USPS ZIP CODE CROSSWALK FILES. Available from: https://www.huduser.gov/portal/datasets/usps_crosswalk.html.
34. Bramante S, Di Salvo G, Maina G, Rosso G. Paliperidone palmitate: a breakthrough treatment for schizophrenia? A review on patient adherence levels, healthcare resource utilization and costs. Neuropsychiatr Dis Treat. 2023;19:519–530. doi:10.2147/NDT.S374696
35. Patel C, Emond B, Lafeuille MH, et al. Real-world analysis of switching patients with schizophrenia from oral risperidone or oral paliperidone to once-monthly paliperidone palmitate. Drugs Real World Outcomes. 2020;7(1):19–29. doi:10.1007/s40801-019-00172-9
36. Vita G, Tavella A, Ostuzzi G, et al. Efficacy and safety of long-acting injectable versus oral antipsychotics in the treatment of patients with early-phase schizophrenia-spectrum disorders: a systematic review and meta-analysis. Ther Adv Psychopharmacol. 2024;14:20451253241257062. doi:10.1177/20451253241257062
37. Li P, Benson C, Geng Z, Seo S, Patel C, Doshi JA. Antipsychotic utilization, healthcare resource use and costs, and quality of care among fee-for-service Medicare beneficiaries with schizophrenia in the United States. J Med Econ. 2023;26(1):525–536. doi:10.1080/13696998.2023.2189859
38. Lohman MC, Scott V, Verma M, Jones P, Fields E. Distribution and correlates of long-acting injectable antipsychotic use among community mental health center patients. Psychiatry Res. 2025;345:116378. doi:10.1016/j.psychres.2025.116378
39. Tyler N, Hodkinson A, Planner C, et al. Transitional care interventions from hospital to community to reduce health care use and improve patient outcomes: a systematic review and network meta-analysis. JAMA Network Open. 2023;6(11):e2344825. doi:10.1001/jamanetworkopen.2023.44825
40. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
41. Wright N, Rowley E, Chopra A, Gregoriou K, Waring J. From admission to discharge in mental health services: a qualitative analysis of service user involvement. Health Expect. 2016;19(2):367–376. doi:10.1111/hex.12361
42. Naylor MD, Shaid EC, Carpenter D, et al. Components of comprehensive and effective transitional care. J Am Geriatr Soc. 2017;65(6):1119–1125. doi:10.1111/jgs.14782
43. Solomon P, Hanrahan NP, Hurford M, DeCesaris M, Josey L. Lessons learned from implementing a pilot RCT of transitional care model for individuals with serious mental illness. Arch Psychiatr Nurs. 2014;28(4):250–255. doi:10.1016/j.apnu.2014.03.005
44. Neyra A, Parro-Torres C, Ros-Cucurull E, Carrera I, Echarri E, Torrens M. Management of schizophrenia and comorbid substance use disorders: expert review and guidance. Ann Gen Psychiatry. 2024;23(1):40. doi:10.1186/s12991-024-00529-7
45. Gast A, Mathes T. Medication adherence influencing factors-An (updated) overview of systematic reviews. Syst Rev. 2019;8(1):112. doi:10.1186/s13643-019-1014-8
46. Wilder ME, Kulie P, Jensen C, et al. The impact of social determinants of health on medication adherence: a systematic review and meta-analysis. J Gen Intern Med. 2021;36(5):1359–1370. doi:10.1007/s11606-020-06447-0
47. Adeoye-Olatunde OA, Hastings TJ, Blakely ML, Boyd L, Aina AB, Sherbeny F. Social determinants of health and medication adherence in older adults with prevalent chronic conditions in the United States: an analysis of the National Health and Nutrition Examination Survey (NHANES) 2009-2018. Pharmacy. 2025;13(1):20. doi:10.3390/pharmacy13010020
48. Higginbotham JK, Segovia LM, Rohm KL, Anderson CM, Breitenstein SM. Social vulnerability index and health outcomes in the United States: a systematic review. Fam Community Health. 2025;48(2):81–96. doi:10.1097/fch.0000000000000421
49. Ding A, Dixon SW, Ferries EA, Shrank WH. The role of integrated medical and prescription drug plans in addressing racial and ethnic disparities in medication adherence. J Manag Care Spec Pharm. 2022;28(3):379–386. doi:10.18553/jmcp.2022.28.3.379
50. Citrome L. New second-generation long-acting injectable antipsychotics for the treatment of schizophrenia. Expert Rev Neurother. 2013;13(7):767–783. doi:10.1586/14737175.2013.811984
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.