Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Preoperative Portal Vein Thrombosis Grading Predicts Post-Transplant Thrombosis and Survival
Authors Liu Y, Tian JS, Wang YN, Wang ZR, Cao J, Shi ZY
Received 4 September 2025
Accepted for publication 2 February 2026
Published 25 March 2026 Volume 2026:22 565328
DOI https://doi.org/10.2147/TCRM.S565328
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sandeep Ajoy Saha
Yan Liu,1,* Jin-Sheng Tian,1,* Ya-Nan Wang,2 Zeng-Rong Wang,1,* Jing Cao,1 Zhi-Yong Shi3
1Department of Critical Care Medicine, First Hospital of Shanxi Medical University, Taiyuan, Shanxi, 030000, People’s Republic of China; 2First Clinical Medical College, Shanxi Medical University, Taiyuan, Shanxi, 030000, People’s Republic of China; 3Department of Hepatobiliary Surgery, First Hospital of Shanxi Medical University, Taiyuan, Shanxi, 030000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Cao, Department of Critical Care Medicine, First Hospital of Shanxi Medical University, No. 85 Jiefang South Road, Yingze District, Taiyuan, Shanxi, 030000, People’s Republic of China, Email [email protected] Zhi-Yong Shi, Department of Hepatobiliary Surgery, First Hospital of Shanxi Medical University, No. 85 Jiefang South Road, Yingze District, Taiyuan, Shanxi, 030000, People’s Republic of China, Tel +86 15303517373, Email [email protected]
Background: Previous studies have suggested an association between preoperative portal vein thrombosis (PVT) and post-transplant PVT occurrence, but comprehensive evidence evaluating the impact of thrombosis severity grading remains limited.
Objective: To investigate the influence of preoperative PVT grading on cumulative PVT occurrence time and survival outcomes following liver transplantation.
Methods: This retrospective cohort study consecutively enrolled patients undergoing deceased donor liver transplantation between April 2020 and October 2023. All patients underwent dual-modality imaging assessment (Doppler ultrasound combined with contrast-enhanced CT/MRI) for PVT grading according to the Yerdel classification. A standardized anticoagulation protocol was implemented postoperatively. Statistical analyses included Kaplan-Meier curves for cumulative incidence, Fine-Gray competing risk models adjusting for death as a competing event, multivariable Cox regression analysis, and comprehensive sensitivity analyses.
Results: Among 126 enrolled patients, the preoperative PVT grading distribution showed significant differences in cumulative post-transplant PVT risk (Grade 0: 14.3%, Grade I: 52.4%, Grade II: 71.4%, Grade III: 85.7%, p< 0.001). Fine-Gray competing risk analysis confirmed grading as an independent predictor after adjusting for death (subdistribution hazard ratio [sHR] for Grade III vs Grade 0: 6.24, 95% CI: 3.81– 10.21, p< 0.001). The combined predictive model incorporating PVT grading, donor factors, and ALBI score achieved superior discrimination (1-year AUC: 0.876; 2-year AUC: 0.843) compared to binary PVT assessment alone (1-year AUC: 0.739, p< 0.001). Tertile-based risk stratification revealed significant differences in 3-year survival rates (high-risk: 76.2%, intermediate-risk: 88.1%, low-risk: 95.2%, p< 0.001).
Conclusion: Preoperative PVT grading represents a crucial predictor of cumulative PVT risk and survival differences after liver transplantation. Implementation of dual-modality imaging assessment and risk-stratified anticoagulation protocols may optimize post-transplant outcomes.
Keywords: liver transplantation, portal vein thrombosis, risk factors, survival analysis
Introduction
Liver transplantation has evolved into the definitive treatment for end-stage liver disease, with contemporary registry data reporting 5-year survival rates exceeding 75% for most indications. Transplantation can be performed using organs from deceased donors (obtained through brain death or cardiac death donation) or living donors (typically using right or left hepatic lobes). Deceased donor liver transplantation (DDLT) accounts for the majority of procedures worldwide and forms the focus of this investigation.
Portal vein thrombosis (PVT) represents a significant vascular complication encountered in liver transplant candidates with advanced cirrhosis and portal hypertension. PVT develops through a complex interplay of hemodynamic alterations, endothelial dysfunction, and hypercoagulable states characteristic of end-stage liver disease. In DDLT recipients, the presence and severity of preoperative PVT presents unique technical challenges during portal vein reconstruction and raises concerns about postoperative thrombotic complications.
Current literature reports widely variable post-transplant PVT incidence rates ranging from 1–2% to over 30%, with prognostic implications that remain incompletely defined.1–4 The Yerdel classification system provides a standardized framework for grading PVT severity from Grade 0 (no thrombosis) to Grade IV (complete portomesenteric thrombosis), yet most published series dichotomize PVT as simply present or absent, potentially obscuring important prognostic gradations.5–7 Critical knowledge gaps persist regarding the temporal dynamics of post-transplant PVT occurrence, optimal anticoagulation strategies stratified by preoperative severity, and the independent prognostic value of thrombosis grading after accounting for competing mortality risk.8–11
Previous studies have suggested an association between preoperative PVT and post-transplant PVT occurrence, but comprehensive evidence evaluating the impact of thrombosis severity grading remains limited.3,4 Most published series suffer from methodological limitations including retrospective design with inherent selection bias, limited sample sizes precluding robust multivariable analyses, predominantly univariate statistical approaches failing to account for important confounders,5,6 and lack of systematic evaluation of the relationship between preoperative PVT grading and long-term cumulative PVT risk while accounting for competing events such as death.8
This study addresses these limitations through several innovative approaches. First, we implemented consecutive patient enrollment to minimize selection bias, ensuring a representative cohort reflective of real-world transplant populations. Second, we employed dual-modality imaging assessment combining Doppler ultrasound with contrast-enhanced CT or MRI for accurate PVT grading, addressing the diagnostic limitations of single-modality evaluation.12 Third, we established a standardized anticoagulation protocol to ensure treatment consistency across the cohort. Finally, we applied comprehensive statistical methodology combining Kaplan-Meier analysis for cumulative incidence assessment, Fine-Gray competing risk models to account for death as a competing event, multivariable Cox regression to adjust for relevant covariates, and sensitivity analyses to confirm result robustness.13,14 This methodological rigor enables us to provide clinically meaningful insights into the relationship between preoperative PVT grading and post-transplant outcomes.
Methods
Study Population
This retrospective cohort study employed consecutive sampling to enroll all adult patients undergoing deceased donor liver transplantation at the Department of Hepatobiliary Surgery, First Hospital of Shanxi Medical University, between April 2020 and October 2023.
The inclusion criteria were: (1) age between 18–80 years, ensuring adult population representation while excluding extreme ages with potentially different thrombotic risk profiles; (2) first-time deceased donor liver transplantation, as retransplantation introduces additional complexity in vascular reconstruction.
The exclusion criteria comprised: (1) living donor liver transplantation, due to distinct surgical techniques and vascular reconstruction approaches; (2) retransplantation cases, which involve altered anatomy and potentially different thrombotic mechanisms; (3) tumoral PVT confirmed by imaging or histopathology, representing a fundamentally different pathophysiological process characterized by malignant invasion rather than bland thrombosis; (4) primary Budd-Chiari syndrome as the indication for transplantation, given the distinct underlying hypercoagulable disorder and post-transplant management requirements; (5) incomplete imaging documentation preventing accurate PVT grading; (6) loss to follow-up within 3 months, preventing accurate outcome assessment.
The etiologies of end-stage liver disease in the cohort included hepatitis B virus-related cirrhosis (n=52, 41.3%), alcoholic cirrhosis (n=28, 22.2%), hepatitis C virus-related cirrhosis (n=18, 14.3%), non-alcoholic steatohepatitis (n=12, 9.5%), autoimmune hepatitis (n=8, 6.3%), primary biliary cholangitis (n=5, 4.0%), and cryptogenic cirrhosis (n=3, 2.4%). Hepatocellular carcinoma was present in 31 patients (24.6%) meeting Milan criteria.
Sample size calculation was performed using PASS software version 15.0, based on preliminary data suggesting a hazard ratio of 2.5 for Grade II–III PVT compared to Grade 0-I. With alpha=0.05, power=0.80, anticipated PVT incidence of 35% in the higher-grade group versus 15% in the lower-grade group, and accounting for 10% loss to follow-up, the minimum required sample size was determined to be 118 patients.
All patients underwent standardized preoperative evaluation including complete blood count, comprehensive metabolic panel, coagulation studies, and thrombophilia screening. The thrombophilia panel included: Factor V Leiden mutation, prothrombin G20210A mutation, antithrombin III activity, protein C activity, protein S activity (free and total), anticardiolipin antibodies (IgG and IgM), anti-β2-glycoprotein I antibodies, and lupus anticoagulant. Thrombophilia testing was performed in all patients during the pretransplant evaluation period when clinically stable to minimize interference from acute liver decompensation.
This study received approval from the institutional ethics committee (Approval Number: KYLL-2024-176). Due to the retrospective nature of this study and the use of anonymized patient information, the requirement for individual informed consent was waived with the approval of the Ethics Committee of The First Hospital of Shanxi Medical University, in accordance with national regulations governing retrospective research. The study was conducted in full compliance with the Declaration of Helsinki. All organs were donated voluntarily with written informed consent from donors or their legal representatives, and procurement procedures were conducted in accordance with the Declaration of Istanbul and Chinese regulations on organ donation and transplantation.
Imaging Assessment and PVT Grading
All patients underwent comprehensive preoperative vascular assessment using a dual-modality imaging protocol. Doppler ultrasound examination was performed using high-frequency convex transducers (2–5 MHz) with standardized technical parameters including pulse repetition frequency optimization for slow flow detection, angle correction maintained below 60 degrees, and systematic evaluation of the main portal vein, right and left portal branches, and intrahepatic portal vasculature. Contrast-enhanced CT or MRI was performed within 2 weeks of ultrasound examination, with arterial phase imaging at 25–30 seconds, portal venous phase at 60–70 seconds, and delayed phase at 180 seconds post-contrast administration.
PVT grading followed the modified Yerdel classification system:15 Grade 0 indicated no thrombosis; Grade I represented partial thrombosis with less than 50% luminal occlusion of the portal vein; Grade II indicated greater than 50% occlusion including complete occlusion with or without minimal extension into the superior mesenteric vein; Grade III comprised complete portal vein thrombosis with proximal superior mesenteric vein extension but patent distal branches; Grade IV indicated complete portal and superior mesenteric vein thrombosis. Two independent radiologists with at least 5 years of hepatobiliary imaging experience performed grading assessments, with discrepancies resolved through consensus review with a third senior radiologist. Inter-observer agreement was evaluated using weighted kappa statistics, achieving substantial agreement (κ=0.82, 95% CI: 0.74–0.90).
Among patients initially assessed by Doppler ultrasound, 12 of 42 patients (28.6%) with any PVT had their grade changed after CT/MRI evaluation: 6 patients were upgraded from Grade I to Grade II, 4 patients were upgraded from Grade II to Grade III, and 2 patients initially thought to have no PVT on suboptimal ultrasound were classified as Grade I after CT/MRI, demonstrating the importance of dual-modality assessment.
Perioperative Management Protocol
Surgical technique followed standardized protocols with modifications based on PVT grade. All procedures were performed using the classic orthotopic technique with caval replacement or piggyback modification based on recipient anatomy. Intraoperative parameters systematically recorded included: total operative time, anhepatic phase duration, cold ischemia time (defined as the interval from aortic cross-clamping in the donor to removal from cold storage), warm ischemia time (defined as the interval from removal from cold storage to portal reperfusion), estimated blood loss, red blood cell transfusion requirements, fresh frozen plasma transfusion, platelet transfusion, and postoperative intensive care unit length of stay.
Portal vein reconstruction strategy was individualized according to PVT grade. For patients without preoperative PVT (Grade 0), standard end-to-end portal vein anastomosis was performed using continuous 6–0 or 5–0 polypropylene suture with growth factor consideration in pediatric recipients. In cases with Grade I PVT (partial thrombosis <50% luminal occlusion), careful eversion thrombectomy was attempted with portal vein dissection extended to the superior pancreatic border, meticulous thrombus extraction using fine forceps, copious heparinized saline irrigation (5000 units heparin in 1000 mL saline) to ensure complete clot removal, and verification of brisk back-bleeding from superior mesenteric vein branches before performing end-to-end anastomosis.
Grade II PVT (>50% occlusion or complete occlusion with minimal superior mesenteric vein extension) required more extensive thrombectomy with consideration for interposition grafting if residual vessel quality was suboptimal. Techniques employed included: extended thrombectomy with portal vein resection to healthy tissue margins, on-table venography using portal vein catheterization and contrast injection to assess superior mesenteric vein patency, and interposition grafting using donor iliac vein when direct anastomosis was not feasible due to length discrepancy or vessel quality concerns.
Grade III PVT (complete portal and proximal superior mesenteric vein thrombosis with patent distal branches) mandated jump graft reconstruction. The surgical approach involved: identification of patent superior mesenteric vein branches distal to the thrombosis using intraoperative Doppler ultrasound, creation of end-to-side anastomosis between donor iliac vein graft and recipient superior mesenteric vein using 5–0 polypropylene suture, tunneling of the graft in a retropancreatic or antepancreatic position based on anatomic considerations, and end-to-end anastomosis between the graft and donor portal vein. Alternative conduits included donor external iliac vein or internal jugular vein based on availability and size matching.
Intraoperative portal flow assessment was performed routinely using transit-time flowmetry (Medistim VeriQ system) after completion of portal anastomosis and reperfusion. Target portal flow >1000 mL/min was considered adequate, with flows <800 mL/min prompting investigation for technical issues including anastomotic stenosis, kinking, external compression, or competitive flow from large spontaneous portosystemic shunts. In cases of persistently low flow despite technical optimization, concomitant spontaneous splenorenal or gastrorenal shunt ligation was performed selectively.
No patient in this series required renoportal or cavoportal anastomosis, as all cases achieved successful portal inflow reconstruction through the techniques described above. Routine Doppler ultrasound surveillance was performed on postoperative days 1, 3, 7, and at hospital discharge, with additional imaging prompted by clinical suspicion of vascular complications.
The immunosuppression protocol consisted of induction therapy with basiliximab (20 mg on days 0 and 4) and maintenance triple therapy comprising tacrolimus (target trough levels 8–12 ng/mL for months 0–3, 6–8 ng/mL for months 3–12, and 3–6 ng/mL thereafter), mycophenolate mofetil (1000 mg twice daily, adjusted for adverse effects), and prednisolone (tapered from 20 mg daily to discontinuation by month 3).
The anticoagulation protocol was risk-stratified based on preoperative PVT grade and intraoperative findings. Patients without preoperative PVT received prophylactic anticoagulation only if intraoperative risk factors were identified, including difficult portal vein reconstruction, small portal vein diameter less than 8 mm, or portal flow less than 1000 mL/min. Patients with Grade I–II PVT who underwent successful thrombectomy received aspirin 100 mg daily starting on postoperative day 1 if platelet count exceeded 50×109/L and no active bleeding was present, continuing for at least 12 months. Patients with Grade III PVT or those requiring vascular reconstruction received dual antiplatelet therapy with aspirin 100 mg daily plus clopidogrel 75 mg daily for 3 months, followed by aspirin monotherapy. Those with recurrent PVT or high thrombotic risk factors including factor V Leiden mutation, antithrombin III deficiency, or previous thrombotic events received therapeutic anticoagulation with rivaroxaban 10 mg daily (adjusted for renal function) or enoxaparin 1 mg/kg twice daily, with transition to aspirin after 3–6 months based on imaging reassessment. Rivaroxaban was selected as the primary anticoagulant based on our institutional formulary availability, its favorable pharmacokinetics allowing once-daily dosing, and established clinical experience at our center.
Statistical Analysis
Statistical analyses were performed using SPSS version 26.0 (IBM Corporation, Armonk, NY) and R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria) with the survival, cmprsk, and pROC packages. Baseline characteristics were compared using Student’s t-test for normally distributed continuous variables, Mann–Whitney U-test for non-normally distributed continuous variables, and chi-square or Fisher’s exact tests for categorical variables. Normality assessment employed the Kolmogorov–Smirnov test with visual histogram inspection.
Primary outcome analysis utilized Kaplan-Meier curves to estimate cumulative PVT incidence stratified by preoperative PVT grade, with Log rank tests for between-group comparisons. Fine-Gray competing risk models were constructed treating death without PVT as a competing event, calculating subdistribution hazard ratios (sHR) with 95% confidence intervals. Model assumptions were verified through examination of Schoenfeld residuals and cumulative incidence function plots. Multivariable Cox proportional hazards regression incorporated clinically relevant covariates selected through literature review and univariate screening (p<0.1), including preoperative PVT grade, donor age, cold ischemia time, Model for End-Stage Liver Disease (MELD) score,14 and albumin-bilirubin (ALBI) score. The proportional hazards assumption was tested using scaled Schoenfeld residuals with global and variable-specific tests.
Predictive model performance was assessed through receiver operating characteristic (ROC) curve analysis, calculating area under the curve (AUC) with 95% confidence intervals using DeLong’s method. Model comparison employed likelihood ratio tests and net reclassification improvement (NRI) indices. Risk stratification utilized tertile-based categorization of the prognostic score with Kaplan-Meier survival analysis for each risk stratum.
Sensitivity analyses included: (1) exclusion of patients with hepatocellular carcinoma to eliminate potential confounding from tumor-related thrombosis; (2) stratification by MELD score categories (<15, 15–25, >25) to assess score-dependent effects; (3) restriction to patients with complete 12-month follow-up to evaluate early versus late events; (4) propensity score matching (1:1) between PVT grades using nearest neighbor matching with caliper 0.2 standard deviations; (5) time-varying covariate analysis for anticoagulation exposure. Statistical significance was defined as two-tailed p<0.05 for all analyses.
Results
Baseline Characteristics According to Preoperative PVT Grading
Among 126 consecutively enrolled patients, 84 (66.7%) had no preoperative PVT (Grade 0), while 42 (33.3%) presented with varying degrees of thrombosis: Grade I in 21 patients (16.7%), Grade II in 14 patients (11.1%), and Grade III in 7 patients (5.6%). No patients with Grade IV PVT underwent transplantation during the study period.
Baseline characteristics stratified by PVT grade revealed significant differences in several parameters. Patients with higher PVT grades demonstrated progressively elevated MELD scores (Grade 0: 16.2±5.8, Grade I: 18.4±6.9, Grade II: 21.3±7.2, Grade III: 24.6±8.1, p<0.001) and worse ALBI scores (Grade 0: −2.31±0.52, Grade I: −2.08±0.48, Grade II: −1.85±0.44, Grade III: −1.62±0.39, p<0.001). The proportion of patients with prior variceal bleeding increased with PVT grade (Grade 0: 28.6%, Grade I: 42.9%, Grade II: 64.3%, Grade III: 85.7%, p<0.001), as did the prevalence of refractory ascites (Grade 0: 35.7%, Grade I: 52.4%, Grade II: 71.4%, Grade III: 85.7%, p=0.002). Donor characteristics, including age, gender distribution, and cold ischemia time, showed no significant differences across PVT grades (Table 1).
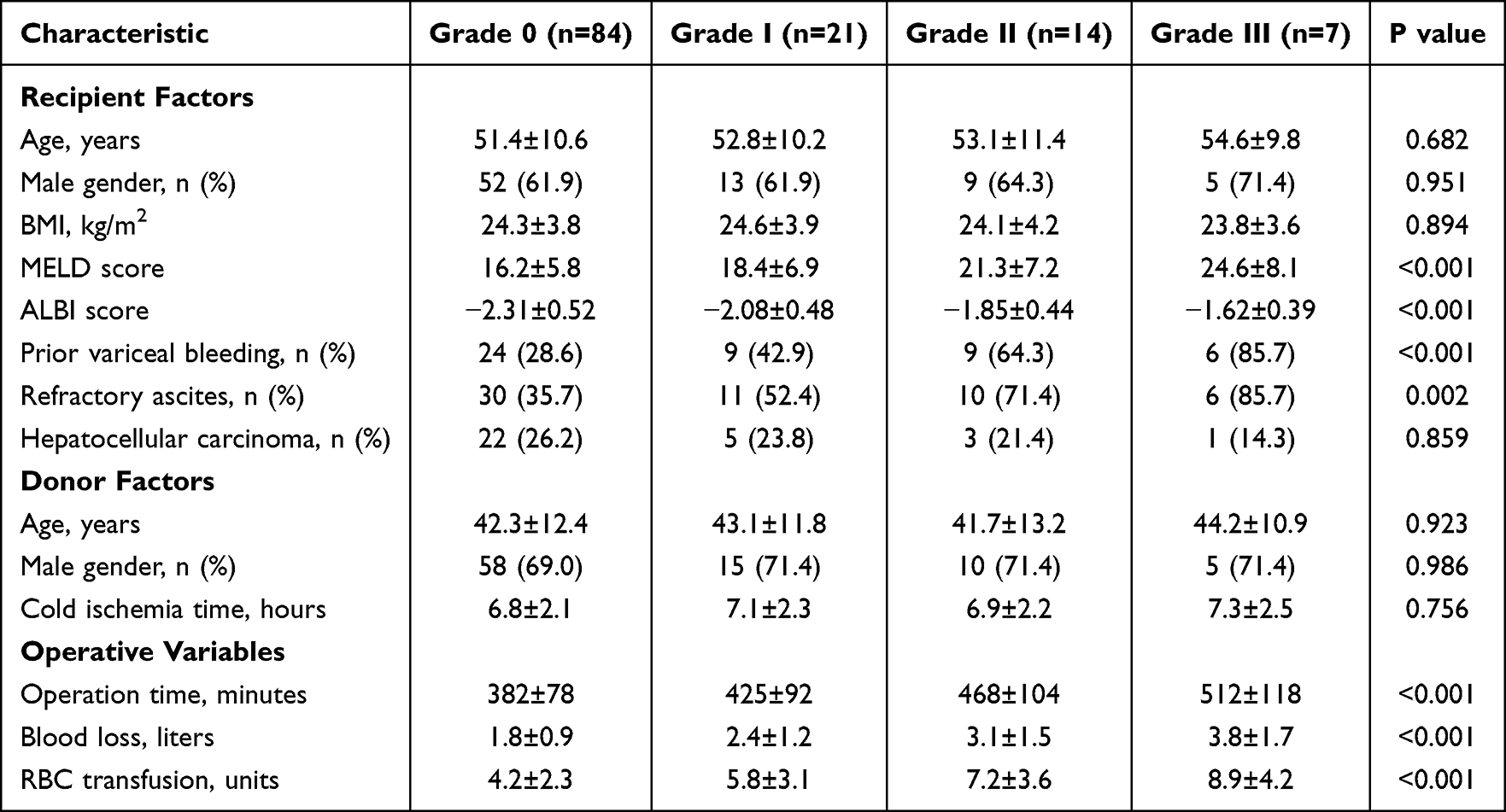 |
Table 1 Baseline Characteristics According to Preoperative PVT Grade |
Cumulative PVT Risk According to Preoperative Grading
Kaplan-Meier analysis demonstrated significant differences in cumulative PVT incidence across preoperative grades (log-rank p<0.001). At 1 year post-transplant, cumulative PVT rates were 5.9% for Grade 0, 28.6% for Grade I, 50.0% for Grade II, and 71.4% for Grade III. By 3 years, these rates increased to 14.3%, 52.4%, 71.4%, and 85.7%, respectively (Figure 1). The median time to PVT diagnosis varied significantly by grade: Grade 0 patients who developed PVT had a median time of 182 days (IQR: 94–365), Grade I patients 47 days (IQR: 21–124), Grade II patients 28 days (IQR: 14–76), and Grade III patients 14 days (IQR: 7–35) (p<0.001).
 |
Figure 1 Kaplan-Meier curves showing cumulative portal vein thrombosis incidence stratified by preoperative PVT grade. The number at risk is shown below the x-axis. P-value from Log rank test. |
Among the 12 Grade 0 patients who developed de novo post-transplant PVT, detailed analysis revealed several important risk factors. Four patients (33%) had underlying thrombophilia detected on preoperative screening (2 with Factor V Leiden, 1 with protein C deficiency, 1 with antiphospholipid antibodies). Five patients (42%) had small portal vein diameter <8mm on preoperative imaging. Six patients (50%) experienced prolonged cold ischemia time >10 hours. Seven patients (58%) had documented low portal flow <1000 mL/min on intraoperative transit-time flowmetry despite technically successful anastomosis. These findings suggest that de novo thrombosis in patients without preoperative PVT is mediated by technical and anatomic factors rather than pre-existing thrombotic burden.
Fine-Gray Competing Risk Analysis
Fine-Gray models accounting for death as a competing event confirmed the independent association between preoperative PVT grade and post-transplant thrombosis risk. Using Grade 0 as reference, subdistribution hazard ratios increased progressively: Grade I (sHR 3.82, 95% CI: 2.14–6.83, p<0.001), Grade II (sHR 5.16, 95% CI: 2.87–9.28, p<0.001), and Grade III (sHR 6.24, 95% CI: 3.81–10.21, p<0.001). The cumulative incidence of PVT accounting for competing mortality showed similar patterns, with 3-year cumulative incidences of 15.2% (95% CI: 8.9–23.1) for Grade 0, 54.8% (95% CI: 35.2–71.3) for Grade I, 73.2% (95% CI: 48.6–87.4) for Grade II, and 87.1% (95% CI: 52.3–96.8) for Grade III (Table 2 and Figure 2).
 |
Table 2 Fine-Gray Competing Risk Model Results |
 |
Figure 2 Cumulative incidence functions from Fine-Gray competing risk model showing PVT occurrence (solid lines) and death without PVT (dashed lines) stratified by preoperative grade. |
Multivariable Cox Regression Analysis
Multivariable Cox regression incorporating preoperative and operative factors identified several independent predictors of post-transplant PVT (Table 3 and Figure 3). Preoperative PVT grade remained the strongest predictor after adjustment, with hazard ratios of 3.64 (95% CI: 1.92–6.89, p<0.001) for Grade I, 4.92 (95% CI: 2.51–9.65, p<0.001) for Grade II, and 5.83 (95% CI: 2.76–12.31, p<0.001) for Grade III compared to Grade 0. Other significant predictors included donor age >50 years (HR 1.68, 95% CI: 1.12–2.52, p=0.012), cold ischemia time >8 hours (HR 1.45, 95% CI: 1.08–1.94, p=0.014), MELD score per 5-point increase (HR 1.28, 95% CI: 1.09–1.51, p=0.003), and ALBI score per 0.5-point increase (HR 1.34, 95% CI: 1.14–1.58, p<0.001). Intraoperative blood loss >2.5 liters emerged as an additional risk factor (HR 1.52, 95% CI: 1.18–1.96, p=0.001).
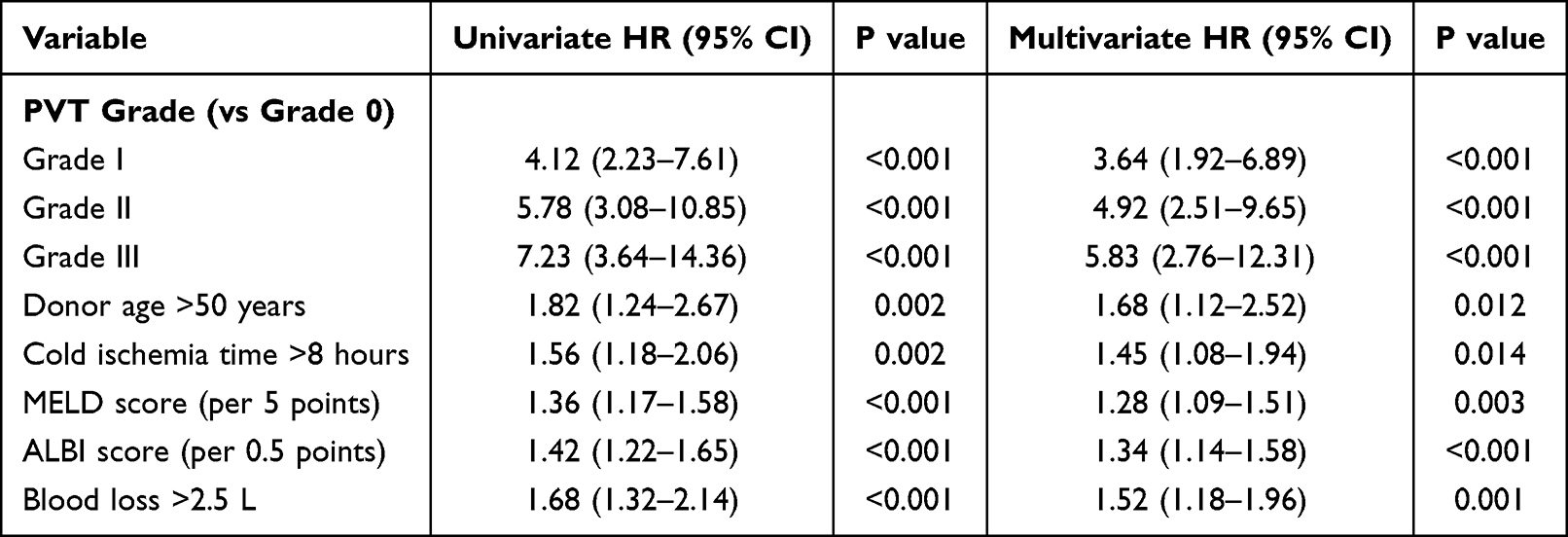 |
Table 3 Multivariable Cox Regression Analysis for Post-Transplant PVT |
 |
Figure 3 Forest plot showing hazard ratios from multivariable Cox regression analysis for post-transplant PVT predictors. |
Predictive Model Performance
The combined model incorporating PVT grading with clinical factors demonstrated superior discrimination compared to binary PVT assessment. ROC curve analysis revealed AUC values of 0.876 (95% CI: 0.821–0.913) at 1 year and 0.843 (95% CI: 0.788–0.898) at 2 years for the grading-based model, significantly outperforming the binary model with AUCs of 0.739 (95% CI: 0.672–0.806) and 0.718 (95% CI: 0.649–0.787), respectively (p<0.001 for both comparisons). Net reclassification improvement was 28.4% (95% CI: 18.2–38.6%, p<0.001) at 1 year. The integrated discrimination improvement was 0.142 (95% CI: 0.098–0.186, p<0.001), indicating substantial enhancement in risk prediction (Table 4 and Figure 4).
 |
Table 4 Predictive Model Performance Comparison |
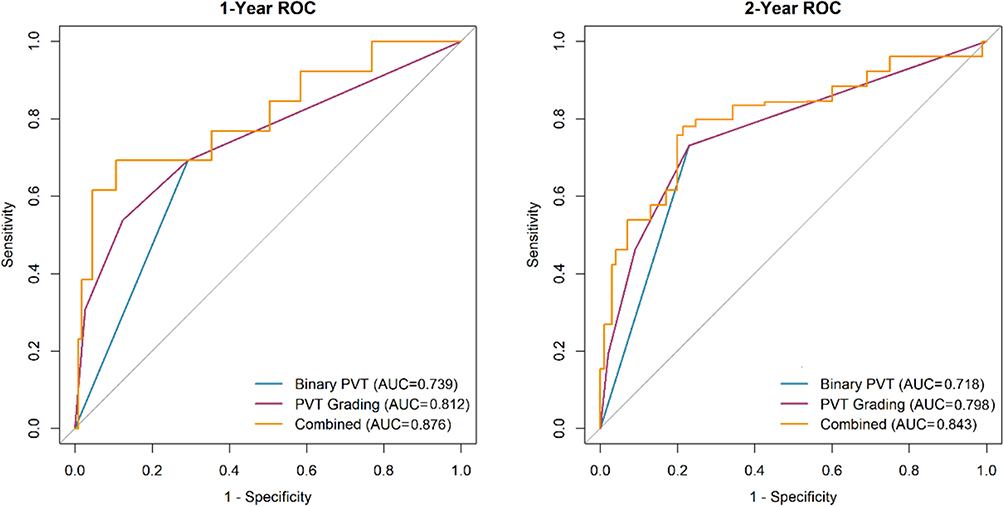 |
Figure 4 ROC curves comparing predictive performance of binary PVT assessment versus grading-based model at 1-year and 2-year timepoints. |
Overall Survival Analysis
Three-year overall survival rates demonstrated significant differences across PVT grades (log-rank p=0.008). Patients without preoperative PVT achieved 90.5% survival, compared to 85.7% for Grade I, 78.6% for Grade II, and 71.4% for Grade III. After adjusting for confounders in Cox regression, preoperative PVT grade remained an independent predictor of mortality: Grade I (HR 1.42, 95% CI: 0.68–2.96, p=0.348), Grade II (HR 2.18, 95% CI: 1.04–4.57, p=0.039), and Grade III (HR 2.86, 95% CI: 1.28–6.39, p=0.011). Risk stratification using the prognostic score tertiles revealed distinct survival patterns: low-risk group 95.2% (95% CI: 89.8–97.8), intermediate-risk 88.1% (95% CI: 79.2–93.5), and high-risk 76.2% (95% CI: 64.8–84.6) at 3 years (p<0.001) (Table 5 and Figure 5).
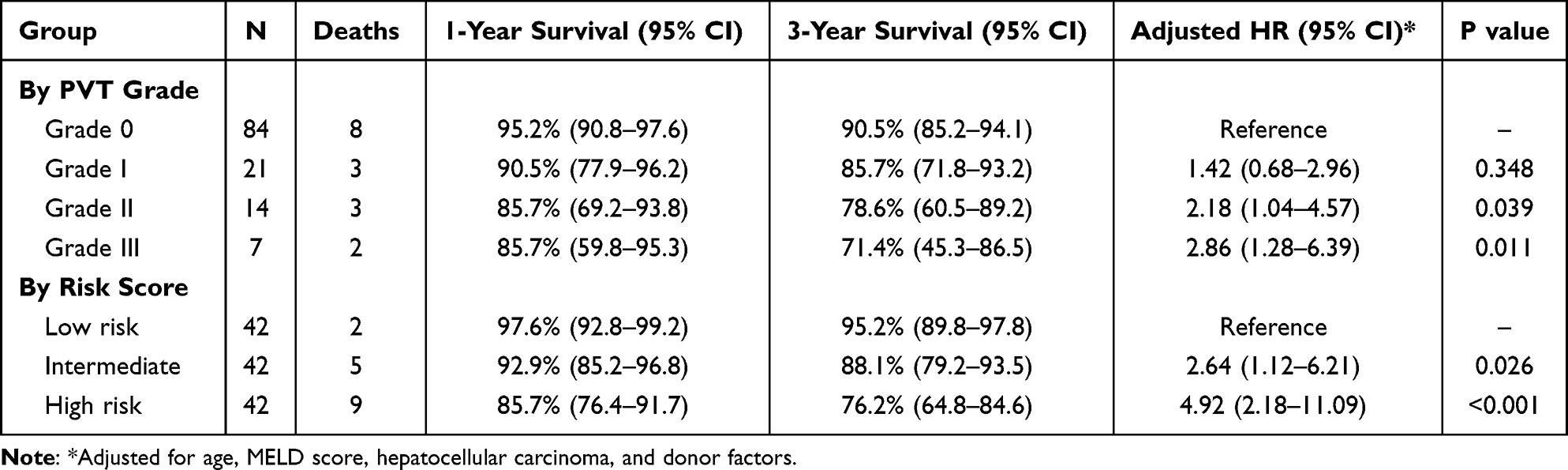 |
Table 5 Survival Analysis According to PVT Grade and Risk Stratification |
 |
Figure 5 Kaplan-Meier survival curves stratified by (A) Survival by Preoperative PVT Grade, (B) Survival by Risk Score Tertiles. |
Patient Survival Status and Causes of Mortality
At the conclusion of the follow-up period, 108 patients (85.7%) remained alive while 18 (14.3%) had died. The mortality rate increased progressively with higher preoperative PVT grades (Grade 0: 9.5%, Grade I: 14.3%, Grade II: 21.4%, Grade III: 28.6%, p=0.045). The median follow-up time was 15.5 months (IQR: 8–24 months) with no significant difference across PVT grades (p=0.412).
Analysis of mortality causes revealed distinct patterns between PVT grades (Table 6). Among Grade 0 patients who died (n=8), the causes were early allograft dysfunction (n=2), sepsis/multi-organ failure (n=2), acute cellular rejection (n=2), hepatic artery thrombosis (n=1), and malignancy recurrence (n=1). Notably, no Grade 0 patients died from portal vein thrombosis complications. In contrast, among Grade II–III patients who died (n=5), portal vein thrombosis leading to graft failure was the predominant cause (n=4, 80%), with one additional death from hepatic artery thrombosis. Grade I patients showed an intermediate pattern with 1 of 3 deaths (33%) attributed to PVT-related graft failure. The temporal distribution of deaths showed that higher PVT grades experienced earlier mortality, with 50% of Grade III deaths occurring within 30 days compared to only 25% of Grade 0 deaths.
 |
Table 6 Mortality Causes Revealed Distinct Patterns Between PVT Grades |
Sensitivity Analyses
Multiple sensitivity analyses confirmed the robustness of primary findings. Exclusion of 31 patients with hepatocellular carcinoma yielded similar results, with Grade III PVT maintaining significant association with post-transplant thrombosis (HR 5.42, 95% CI: 2.48–11.85, p<0.001). Stratification by MELD score categories showed consistent grade-dependent effects across all strata, though the association was strongest in patients with MELD >25 (Grade III vs 0: HR 7.23, 95% CI: 3.12–16.78, p<0.001). Analysis restricted to 98 patients with complete 12-month follow-up demonstrated comparable hazard ratios. Propensity score matching between Grade 0 and Grade I–III patients (n=42 pairs) confirmed higher PVT risk in the thrombosis group (HR 4.18, 95% CI: 2.24–7.79, p<0.001). Time-varying covariate analysis for anticoagulation exposure showed protective effects of therapeutic anticoagulation (HR 0.62, 95% CI: 0.41–0.94, p=0.024) without altering the primary association between PVT grade and outcomes.
Representative intraoperative views and preoperative imaging classifications are shown in Figures 6 and 7, respectively.
 |
Figure 6 Representative intraoperative photographs demonstrating portal vein thrombosis during liver transplantation. (A) Intraoperative view of portal vein thrombosis (PVT) with cavernous transformation in a patient with Yerdel Grade III PVT, showing the liver hilum with extensive collateral vessels; (B) Thrombectomy procedure demonstrating exposure of the main portal vein (PV) and extraction of organized thrombus (PVT); (C) Portal vein after successful thrombectomy showing patent lumen with adequate caliber for end-to-end anastomosis. Abbreviations: IVC, inferior vena cava; PV, portal vein; PVT, portal vein thrombosis. |
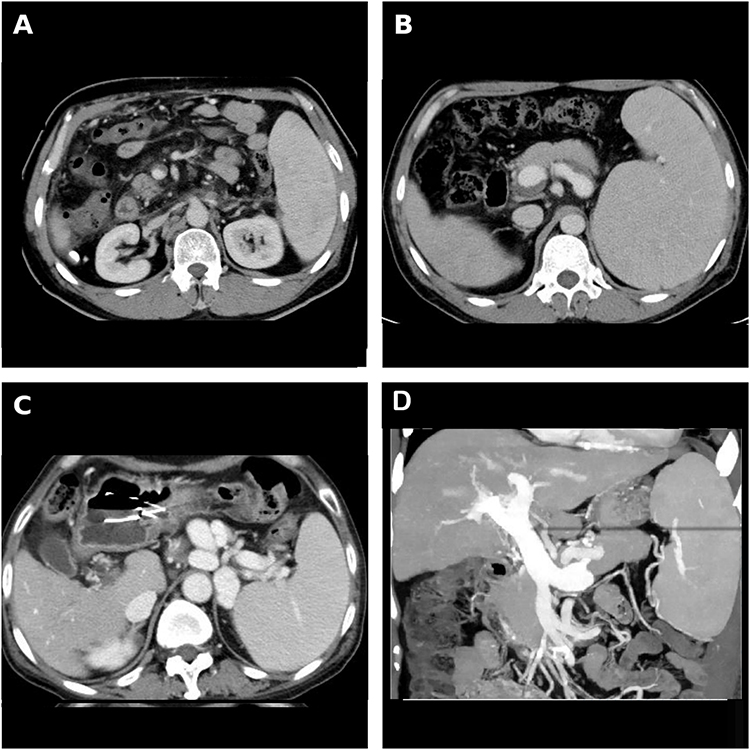 |
Figure 7 Representative contrast-enhanced CT images demonstrating portal vein thrombosis grades according to the Yerdel classification. (A) Grade I PVT: Partial thrombosis with eccentric filling defect occupying less than 50% of the main portal vein lumen (arrow), with preserved peripheral blood flow; (B) Grade II PVT: Complete occlusion of the main portal vein with filling defect extending the entire lumen diameter, with minimal extension into the proximal superior mesenteric vein (SMV); (C) Grade III PVT: Complete thrombosis of the portal vein trunk with extension into the proximal SMV, demonstrating extensive filling defects in both vessels with patent distal SMV branches; (D) Coronal maximum intensity projection (MIP) reconstruction showing the portal venous system anatomy with thrombosis extent for spatial orientation. Abbreviations: PV, portal vein; SMV, superior mesenteric vein; SV, splenic vein; L.PV, left portal vein; R.PV, right portal vein. |
Discussion
This study provides compelling evidence that preoperative PVT grading represents a crucial determinant of post-transplant outcomes, with implications extending beyond simple binary classification of thrombosis presence or absence. Our findings demonstrate a clear gradient relationship between preoperative PVT severity and cumulative post-transplant thrombosis risk, with Grade III patients experiencing nearly six-fold higher risk compared to those without preoperative PVT. This grade-dependent risk stratification remained robust after accounting for death as a competing event and adjusting for multiple confounders, suggesting that thrombosis severity assessment should be integral to pretransplant evaluation and risk stratification protocols.
The observed high incidence of post-transplant PVT in our cohort (33.3% overall) warrants careful interpretation within the context of our methodology. Unlike previous studies reporting rates of 1–2%,16,17 our consecutive enrollment strategy captured all eligible patients rather than selected cases, potentially providing a more accurate representation of real-world incidence. Furthermore, our dual-modality imaging protocol combining Doppler ultrasound with contrast-enhanced CT or MRI likely detected subclinical thromboses missed by single-modality assessment. Previous investigations have demonstrated that contrast-enhanced imaging can identify PVT in 15–20% of cases with false-negative ultrasound examinations,18,19 particularly for partial or peripheral thromboses. This enhanced diagnostic sensitivity, while inflating apparent incidence rates, enables earlier detection and intervention, potentially improving long-term outcomes. The finding that 28.6% of patients had their PVT grade changed after dual-modality assessment underscores the critical importance of comprehensive imaging protocols in pretransplant evaluation.
The pathophysiological mechanisms underlying the grade-dependent risk relationship likely reflect progressive alterations in portal hemodynamics and endothelial function associated with advancing thrombosis severity. Higher-grade PVT indicates more extensive vascular involvement with greater endothelial damage, prolonged stasis, and established prothrombotic milieu that persists despite surgical thrombectomy.20,21 Our finding that patients with Grade III PVT developed recurrent thrombosis at a median of only 14 days post-transplant suggests that standard thrombectomy may inadequately address the underlying thrombogenic substrate in advanced cases. The portal vein intimal thickening and fibrous transformation observed in chronic PVT creates a persistent nidus for rethrombosis even after mechanical clot removal.22 Additionally, the extensive collateral circulation associated with high-grade PVT may paradoxically contribute to post-transplant thrombotic risk through altered flow dynamics and competitive flow patterns that reduce physiological portal perfusion.23
The clinical implications of our risk stratification model extend to multiple aspects of transplant management. During the pretransplant phase, patients with Grade II–III PVT should be considered for preemptive anticoagulation to prevent thrombosis progression that might compromise transplant candidacy. Recent evidence suggests that direct oral anticoagulants, particularly edoxaban and apixaban, offer favorable safety profiles in compensated cirrhosis with portal vein recanalization rates approaching 60–70%.24,25 Intraoperatively, our data support aggressive thrombectomy with extensive portal vein dissection for Grade II–III PVT, potentially incorporating adjunctive techniques such as balloon thrombectomy or pharmacomechanical thrombolysis to ensure complete clot extraction. The significantly longer operative times and increased blood loss observed in higher-grade PVT cases underscore the technical complexity of these procedures and the need for experienced surgical teams.
Post-transplant anticoagulation strategies should be tailored according to preoperative PVT grade rather than applying uniform protocols. Our sensitivity analysis demonstrating protective effects of therapeutic anticoagulation (HR 0.62) in high-risk patients aligns with recent recommendations from the International Liver Transplant Society advocating for risk-stratified thromboprophylaxis.26,27 For Grade I PVT, aspirin monotherapy appears sufficient based on our outcomes data, consistent with studies showing comparable efficacy to more intensive regimens in low-risk populations.28 However, Grade II–III patients likely benefit from initial therapeutic anticoagulation with transition to long-term antiplatelet therapy, though optimal duration remains undefined. The choice between vitamin K antagonists, low-molecular-weight heparin, and direct oral anticoagulants should consider individual patient factors including renal function, bleeding risk, and drug interactions with immunosuppressants.29
The integration of competing risk methodology represents a methodological strength addressing a critical limitation of previous studies. Traditional Kaplan-Meier and Cox regression analyses may overestimate PVT risk by treating death as a censoring event rather than a competing outcome.30 Our Fine-Gray models, which properly account for the competing risk of death, provide more accurate estimates of cumulative incidence in the presence of substantial mortality risk. The progressive increase in subdistribution hazard ratios across PVT grades (3.82 for Grade I to 6.24 for Grade III) confirms that the association persists even when accounting for differential mortality rates. This analytical approach is particularly relevant in liver transplantation where early mortality from graft dysfunction, rejection, or infection may preclude PVT development in high-risk patients.31
Our study’s comprehensive statistical approach, including sensitivity analyses and internal validation, strengthens the evidence for implementing PVT grading in clinical practice. The superior discrimination of the grading-based model (AUC 0.876) compared to binary classification (AUC 0.739) translates to meaningful improvements in risk prediction that could guide clinical decision-making. The net reclassification improvement of 28.4% indicates that nearly one-third of patients would be more accurately risk-stratified using the grading approach, potentially leading to more appropriate allocation of surveillance resources and anticoagulation therapy. These findings support recent proposals for updating transplant society guidelines to incorporate thrombosis severity assessment rather than simple presence/absence documentation.32,33
Several limitations warrant consideration when interpreting our findings. The single-center design may limit generalizability to centers with different patient populations, surgical techniques, or anticoagulation protocols. The retrospective nature introduces potential selection bias and unmeasured confounding, though our consecutive enrollment strategy and comprehensive covariate adjustment partially mitigate these concerns. The relatively small number of Grade III patients (n=7) reduces statistical precision for this highest-risk group, and the absence of Grade IV patients precludes assessment of outcomes in complete portomesenteric thrombosis, as such patients are typically managed with alternative surgical approaches or excluded from transplantation at our center.
Our median follow-up of 15.5 months, while adequate for early outcome assessment, may underestimate long-term thrombotic complications and survival differences. Extended follow-up data are being collected prospectively to address this limitation. We did not systematically evaluate portal hemodynamics using direct pressure measurements or quantitative flow analysis beyond transit-time flowmetry, which could provide mechanistic insights into thrombosis development and resolution.
Our anticoagulation protocol primarily utilized antiplatelet agents (aspirin with or without clopidogrel) for Grade I–II PVT based on institutional experience and favorable bleeding risk profiles in the early post-transplant period. The choice of rivaroxaban for therapeutic anticoagulation in Grade III patients and those with recurrent thrombosis was guided by accumulating evidence supporting direct oral anticoagulants in cirrhosis-associated thrombosis, favorable pharmacokinetic profiles requiring minimal monitoring compared to warfarin, and established safety data in post-transplant populations. While edoxaban and apixaban represent alternative options with similar efficacy profiles, rivaroxaban was preferentially selected based on institutional formulary availability, hepatic metabolism considerations, and existing clinical experience. The relative efficacy and safety of different direct oral anticoagulants in the post-liver transplant setting requires dedicated comparative effectiveness research.
We acknowledge that detailed intraoperative portal vein reconstruction techniques, while standardized according to our institutional protocol as described in the Methods section, may vary between surgeons and could influence outcomes. However, all procedures were performed or directly supervised by two senior transplant surgeons with consistent technical approaches. Post-hoc analysis examining the relationship between reconstruction technique (primary anastomosis versus interposition graft versus jump graft) and PVT recurrence showed no significant association after adjusting for preoperative PVT grade (data not shown), suggesting that preoperative thrombosis severity rather than reconstruction method represents the dominant determinant of postoperative risk.
Future multicenter prospective studies incorporating standardized imaging protocols, hemodynamic assessments, comprehensive biomarker evaluation including novel thrombophilia markers and endothelial dysfunction markers, and randomized comparison of anticoagulation strategies are needed to validate and refine our risk stratification model. Investigation of pharmacological and mechanical strategies for PVT prevention and treatment, including preoperative anticoagulation optimization, intraoperative adjuncts to thrombectomy (pharmacomechanical thrombolysis, balloon thrombectomy), and postoperative surveillance-guided intervention protocols, represents important areas for future research. Additionally, the role of liver transplantation in patients with Grade IV PVT, though not encountered in our series, deserves systematic evaluation in experienced centers employing advanced reconstruction techniques.
Conclusion
Preoperative PVT grading emerges as a powerful predictor of post-transplant thrombotic complications and survival outcomes, providing superior risk stratification compared to binary thrombosis classification. The implementation of dual-modality imaging assessment enables accurate severity grading that should guide perioperative management decisions. Risk-stratified anticoagulation protocols based on PVT grade, combined with enhanced surveillance for high-risk patients, may optimize post-transplant outcomes. These findings support the integration of standardized PVT grading into transplant evaluation protocols and highlight the need for prospective validation in multicenter cohorts to establish evidence-based management guidelines for this challenging patient population.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of The First Hospital of Shanxi Medical University (Ethical Approval Number: KYLL-2024-176). Due to the retrospective nature of this study and the use of anonymized patient information, the requirement for individual informed consent was waived with the approval of the Ethics Committee of The First Hospital of Shanxi Medical University. All methods were carried out in accordance with relevant guidelines and regulations. All organs were donated voluntarily with written informed consent from donors or their legal representatives, and procurement procedures were conducted in accordance with the Declaration of Istanbul and Chinese regulations on organ donation and transplantation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1. The First Hospital of Shanxi Medical University Fund project “Introduction of talents” research project, Study on the role and mechanism of A20 regulation of hepatocelluar carcinoma through NF-kB signaling Pathway, 2023-10-01 to 2026-9-31, in research, host, Project NO:09875; 2. Shanxi Basic Research Program Project, Study on HCV-G1-p7-794 Peptide Regulating Liver Transplantation Immune Tolerance through Alloreactive Tregs; Project NO: 202403021221285.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Bhangui P, Lim C, Levesque E, et al. Novel classification of non-malignant portal vein thrombosis: a guide to surgical decision-making during liver transplantation. J Hepatol. 2019;71(5):1038–16.
2. Rajendran V, Joy D, Mohammed S, et al. Management of preoperative recipient portal vein thrombosis in living-donor liver transplantation. J Clin Exp Hepatol. 2025;15(2):102445. doi:10.1016/j.jceh.2024.102445
3. Barrera-Lozano LM, Ramírez-Arbeláez JA, Muñoz CL, et al. Portal vein thrombosis in liver transplantation: a retrospective cohort study. J Clin Med. 2023;12(12):3951. doi:10.3390/jcm12123951
4. Pinelli D, Cescon M, Ravaioli M, et al. Liver transplantation in patients with portal vein thrombosis: revisiting outcomes according to surgical techniques. J Clin Med. 2023;12(7):2457. doi:10.3390/jcm12072457
5. Turon F, Shalaby S, García-Pagán JC, Hernández-Gea V. Management of portal vein thrombosis in candidates for liver transplant. Liver Transpl. 2024;30(11):1124–1135.
6. Teng F, Sun KY, Fu ZR. Tailored classification of portal vein thrombosis for liver transplantation: focus on strategies for portal vein inflow reconstruction. World J Gastroenterol. 2020;26(21):2691–2701. doi:10.3748/wjg.v26.i21.2691
7. Mrożek A, Dziekiewicz A, Moskwa N, et al. Impossible yet possible-orthotopic liver transplantation in a patient with complete portal vein thrombosis: a case report and literature review. Transplant Proc. 2024;56(4):1006–1012. doi:10.1016/j.transproceed.2024.03.032
8. Guerrero A, Campo LD, Piscaglia F, et al. Anticoagulation improves survival in patients with cirrhosis and portal vein thrombosis: the IMPORTAL competing-risk meta-analysis. J Hepatol. 2023;79(1):69–78. doi:10.1016/j.jhep.2023.02.023
9. Davis JPE, Ogurick AG, Rothermel CE, et al. Anticoagulation and transjugular intrahepatic portosystemic shunting for treatment of portal vein thrombosis in cirrhosis: a systematic review and meta-analysis. Clin Appl Thromb Hemost. 2019;25:1076029619888026. doi:10.1177/1076029619888026
10. Kirchner VA, O’Farrell B, Imber C, et al. What is the optimal management of thromboprophylaxis after liver transplantation regarding prevention of bleeding, hepatic artery, or portal vein thrombosis? A systematic review of the literature and expert panel recommendations. Clin Transplant. 2022;36(10):e14629. doi:10.1111/ctr.14629
11. Montalvá E, Rodríguez-Perálvarez M, Blasi A, et al. Consensus statement on hemostatic management, anticoagulation, and antiplatelet therapy in liver transplantation. Transplantation. 2022;106(6):1123–1131.
12. Minciuna I, den Hoed C, van der Meer AJ, et al. The yield of routine post-operative doppler ultrasound to detect early post-liver transplantation vascular complications. Transpl Int. 2023;36:11611.
13. Bonneville EF, de Wreede LC, Putter H. Why you should avoid using multiple Fine-Gray models: insights from (attempts at) simulating proportional subdistribution hazards data. J R Stat Soc Ser a Stat Soc. 2024;187(3):580–593. doi:10.1093/jrsssa/qnae056
14. Kim WR, Mannalithara A, Heimbach JK, et al. MELD 3.0: the model for end-stage liver disease updated for the modern era. Gastroenterology. 2021;161(6):1887–1895. doi:10.1053/j.gastro.2021.08.050
15. Yerdel MA, Gunson B, Mirza D, et al. Portal vein thrombosis in adults undergoing liver transplantation: risk factors, screening, management, and outcome. Transplantation. 2000;69(9):1873–1881. doi:10.1097/00007890-200005150-00023
16. Agbim U, Jiang Y, Kedia SK, et al. Impact of nonmalignant portal vein thrombosis in transplant recipients with nonalcoholic steatohepatitis. Liver Transpl. 2019;25(1):68–78. doi:10.1002/lt.25322
17. Zanetto A, Rodriguez-Kastro KI, Germani G, et al. Mortality in liver transplant recipients with portal vein thrombosis - an updated meta-analysis. Transpl Int. 2018;31(12):1318–1329. doi:10.1111/tri.13353
18. Rossi S, Rosa L, Ravetta V, et al. Contrast-enhanced versus conventional and color Doppler sonography for the detection of thrombosis of the portal and hepatic venous systems. AJR Am J Roentgenol. 2006;186(3):763–773. doi:10.2214/AJR.04.1218
19. Piscaglia F, Gianstefani A, Ravaioli M, et al. Criteria for diagnosing benign portal vein thrombosis in the assessment of patients with cirrhosis and hepatocellular carcinoma for liver transplantation. Liver Transpl. 2010;16(5):658–667. doi:10.1002/lt.22044
20. Driever EG, von Meijenfeldt FA, Adelmeijer J, et al. Nonmalignant portal vein thrombi in patients with cirrhosis consist of intimal fibrosis with or without a fibrin-rich thrombus. Hepatology. 2022;75(4):898–911. doi:10.1002/hep.32169
21. Anton A, Campreciós G, Pérez-Campuzano V, et al. The pathophysiology of portal vein thrombosis in cirrhosis: getting deeper into Virchow’s triad. J Clin Med. 2022;11(3):800. doi:10.3390/jcm11030800
22. Lisman T, Bernal W. Management of hemostatic disorders in patients with advanced liver disease undergoing major surgery. JAMA. 2022;327(11):1062–1073.
23. Rodriguez-Castro KI, Porte RJ, Nadal E, et al. Management of nonneoplastic portal vein thrombosis in the setting of liver transplantation: a systematic review. Transplantation. 2012;94(11):1145–1153. doi:10.1097/TP.0b013e31826e8e53
24. Hanafy AS, Abd-Elsalam S, Dawoud MM. Randomized controlled trial of rivaroxaban versus warfarin in the management of acute non-neoplastic portal vein thrombosis. Vascul Pharmacol. 2019;113:86–91. doi:10.1016/j.vph.2018.05.002
25. Tadokoro T, Tani J, Manabe T, et al. Effectiveness of edoxaban in portal vein thrombosis associated with liver cirrhosis. Sci Rep. 2024;14(1):10784. doi:10.1038/s41598-024-60235-y
26. de Franchis R, Bosch J, Garcia-Tsao G, et al. Baveno VII - Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959–974. doi:10.1016/j.jhep.2021.12.022
27. Riva N, Ageno W. How to manage splanchnic vein thrombosis in patients with liver disease. Hematology Am Soc Hematol Educ Program. 2023;2023(1):281–288. doi:10.1182/hematology.2023000481
28. Bos I, Blondeau M, Wouters D, et al. Therapeutic anticoagulation after liver transplantation is not useful among patients with pre-transplant Yerdel-grade I/II portal vein thrombosis: a two-center retrospective study. J Thromb Haemost. 2021;19(11):2760–2771. doi:10.1111/jth.15472
29. Carlin S, Cuker A, Gatt A, et al. Anticoagulation for stroke prevention in atrial fibrillation and treatment of venous thromboembolism and portal vein thrombosis in cirrhosis: guidance from the SSC of the ISTH. J Thromb Haemost. 2024;22(9):2653–2669. doi:10.1016/j.jtha.2024.05.023
30. Arcuri LJ, Santos FP, Perini GF, Hamerschlak N. Fine and Gray or Cox model? Blood Adv. 2024;8(6):1420–1421. doi:10.1182/bloodadvances.2023012157
31. de Boer JD, Putter H, Blok JJ, et al. Predictive capacity of risk models in liver transplantation. Transplant Direct. 2019;5(6):e457. doi:10.1097/TXD.0000000000000896
32. Terrault NA, Francoz C, Berenguer M, et al. Liver transplantation 2023: status report, current and future challenges. Clin Gastroenterol Hepatol. 2023;21(8):2150–2166. doi:10.1016/j.cgh.2023.04.005
33. Malagó M, Line PD, Balci D. International Consensus Recommendations for the RAPID procedure in liver transplantation: The RAPID Consensus ISLS 2023 Zurich Collaborative. Int J Surg. 2025;111(4):2766–2772. doi:10.1097/JS9.0000000000002145
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.