Back to Journals » Journal of Pain Research » Volume 10
Preoperative intravenous ibuprofen does not influence postoperative narcotic use in patients undergoing elective hernia repair: a randomized, double-blind, placebo controlled prospective trial
Authors Sparber LS, Lau CSM, Vialet TS, Chamberlain RS
Received 20 January 2017
Accepted for publication 28 March 2017
Published 5 July 2017 Volume 2017:10 Pages 1555—1560
DOI https://doi.org/10.2147/JPR.S132836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Lauren S Sparber,1 Christine SM Lau,1,2 Tanya S Vialet,1 Ronald S Chamberlain1–4
1Department of Surgery, Saint Barnabas Medical Center, Livingston, NJ, USA; 2Saint George’s University School of Medicine, Grenada, West Indies; 3Department of Surgery, Banner MD Anderson Cancer Center, Gilbert, AZ, USA; 4Department of Surgery, New Jersey Medical School, Rutgers University, Newark, NJ, USA
Introduction: Inguinal and umbilical hernia repairs are among the most common surgical procedures performed in the US. Optimal perioperative pain control regimens remain challenging and opioid analgesics are commonly used. Preoperative nonsteroidal anti-inflammatory drug (NSAID) administration has been shown to reduce postoperative narcotic requirements. This study sought to evaluate the efficacy of perioperative intravenous (IV) ibuprofen on postoperative pain level and narcotic use in patients undergoing open or laparoscopic inguinal and/or umbilical hernia repair.
Methods: A single center, randomized, double-blind placebo-controlled trial involving patients ≥18 years undergoing inguinal and/or umbilical hernia repair was performed. Patients were randomized to receive 800 mg of IV ibuprofen or placebo preoperatively. Outcomes assessed included postoperative pain medication required and visual analog scale (VAS) pain scores.
Results: Forty-eight adult male patients underwent inguinal and/or umbilical hernia repair. Patients receiving IV ibuprofen used more oxycodone/acetaminophen (32% vs 13%) and IV hydromorphone (12% vs 8.7%), and fewer combinations of pain medications (44% vs 65.2%) in the first two postoperative hours compared to placebo (p=0.556). The IV ibuprofen group had more patients pain free (28% vs 8.7%, p=0.087) and lower VAS scores (3.08±2.14 vs 3.95±1.54, p=0.134) at 2 hours postoperatively, compared to the placebo group, however, this was not statistically significant. Similar pain levels at 1, 3, and 7 days, postoperative and similar use of rescue medications in both groups were observed.
Conclusion: Preoperative administration of IV ibuprofen did not significantly reduce postoperative pain among patients undergoing elective hernia repair. Considerable variability in postoperative narcotic analgesic requirement was noted, and larger scale studies are needed to better understand the narcotic analgesic requirements associated with IV ibuprofen in inguinal/umbilical hernia repair patients.
Keywords: NSAIDs, ibuprofen, pain, hernia repair, RCT
Introduction
Inguinal and umbilical hernia repair are among the most common surgical procedures performed in the US. Optimal perioperative pain control regimens remain challenging and opioid analgesics are most commonly used. Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to reduce narcotic requirements following several surgical procedures if given prior to anesthesia induction. The purported mechanism by preoperative NSAID administration works is by blocking the inflammatory cascade. Oral ibuprofen has been used since 1974 for the treatment of mild to moderate pain as well as for treatment of fever.1 Intravenous (IV) Caldolor® (Cumberland Pharmaceuticals Inc, Nashville, TN, USA) (ibuprofen) contains analgesic, anti-inflammatory and antipyretic properties. It is the first IV antipyretic approved by the US Food and Drug Administration (FDA), providing an alternate route for administration of ibuprofen when the oral route is not preferable.1
Southworth et al published the first randomized, double-blind, placebo controlled study for IV ibuprofen.2 These authors analyzed the effects of IV ibuprofen (400 and 800 mg) given every 6 hours on postoperative pain management for 406 patients scheduled to undergo elective orthopedic or abdominal surgery. Patients were randomly assigned in a 1:1:1 ratio to receive ibuprofen 400 mg IV, ibuprofen 800 mg IV, or placebo for a total of eight doses with the first dose administered in the operating room. Patients who received ibuprofen 800 mg IV experienced a reduction in morphine use, and pain at rest and with movement, compared with the placebo group, however there was a reported increased incidence of dizziness.2 IV ibuprofen has also been shown to significantly reduce fever in critically ill patients.3
The current study sought to evaluate the efficacy of perioperative IV ibuprofen on postoperative pain level and narcotic use in patients undergoing open or laparoscopic inguinal and/or umbilical hernia repair.
Methods
Participants and study design
A prospective, single center double-blinded randomized control trial with IV ibuprofen was compared to placebo. The trial was conducted at Saint Barnabas Medical Center, Livingston, NJ, USA between January 2011 and July 2013, and approval was obtained from Saint Barnabas Medical Center Institutional Review Board (IRB #10-37). The trial was registered with ClinicalTrials.gov with identifier NCT01297829. This trial was conducted according to Good Clinical Practice guidelines, but did not have external monitoring. Written informed consent was obtained from each participant prior to surgery. Inclusion criteria included age >18 years; no prior history of peptic ulcer disease, gastrointestinal bleeding or allergy to ibuprofen; and a creatinine level <1.5 mg/dL. All open and laparoscopic umbilical and /or inguinal hernia repairs performed by a single surgeon (RSC) using standardized technique were included. All surgical procedures were completed as elective procedures, and all patients were admitted to same day surgery the day of their surgery, and discharged home the same day.
Randomization
Randomization was conducted by an independent researcher, separate from the study investigators. Eligible patients were randomly assigned in a 1:1 ratio (via computer generated randomization) to receive either 800 mg of IV ibuprofen or normal saline placebo 30 minutes prior to incision.
Study intervention
The study intervention was a single dose of 800 mg of IV ibuprofen administered 30 minutes preoperatively for patients undergoing laparoscopic or open umbilical and/or inguinal hernia repair. The placebo consisted of normal saline. All drugs were mixed by the in-house pharmacy at Saint Barnabas Medical Center, and placed in an IV bag labeled with only the patient’s name and study name, with no indication of whether or not it was the active study drug or placebo. All IV bags were wrapped in the same color opaque tape to ensure both appeared the same. All IV bags were picked up from the pharmacy by a study investigator, and brought to the anesthesiologist in the operating room to administer. All study drugs were administered by the anesthesiologist, in the presence of a study investigator. All anesthesiologists involved in the study were informed of the study protocol and underwent appropriate training.
All patients received standardized anesthesia and were monitored by the anesthesiologist. Postoperative pain management was consistent in both intervention and control groups, and included IV hydromorphone, or oral oxycodone/acetaminophen, acetaminophen only or ibuprofen, or in combination. Postoperative pain medications were ordered by the anesthesiologist or treating surgeon, and administered by the registered nurses caring for the patient. Upon discharge, the patient was given standard prescriptions and instructed to take pain medications as needed. All patient care was carefully monitored by the treating surgeon.
Data collection and outcomes
Demographic and clinicopathological data including age, ethnic/racial origin, body mass index, comorbidities, daily medications, type of surgery (open inguinal hernia repair, laparoscopic inguinal hernia repair, open umbilical hernia repair, open umbilical and laparoscopic inguinal hernia repair) and operative time were collected on all patients. Type of pain medication requirement at 2 hours postoperatively and then 7 days postoperatively (no pain medication, acetaminophen/NSAIDs, oxycodone + acetaminophen, hydromorphone, combination of pain medications) as well as visual analog scale (VAS) pain score before surgery, 2 hours postoperatively, and then at 1, 3, and 7 days postoperatively, were also collected.
Sample size
One-hundred twenty patients were screened (Figure 1). Fifty-seven patients did not meet inclusion criteria, and 15 patients refused participation in the study. Forty-eight patients were included in the study, with 25 patients receiving IV ibuprofen and 23 patients receiving the placebo.
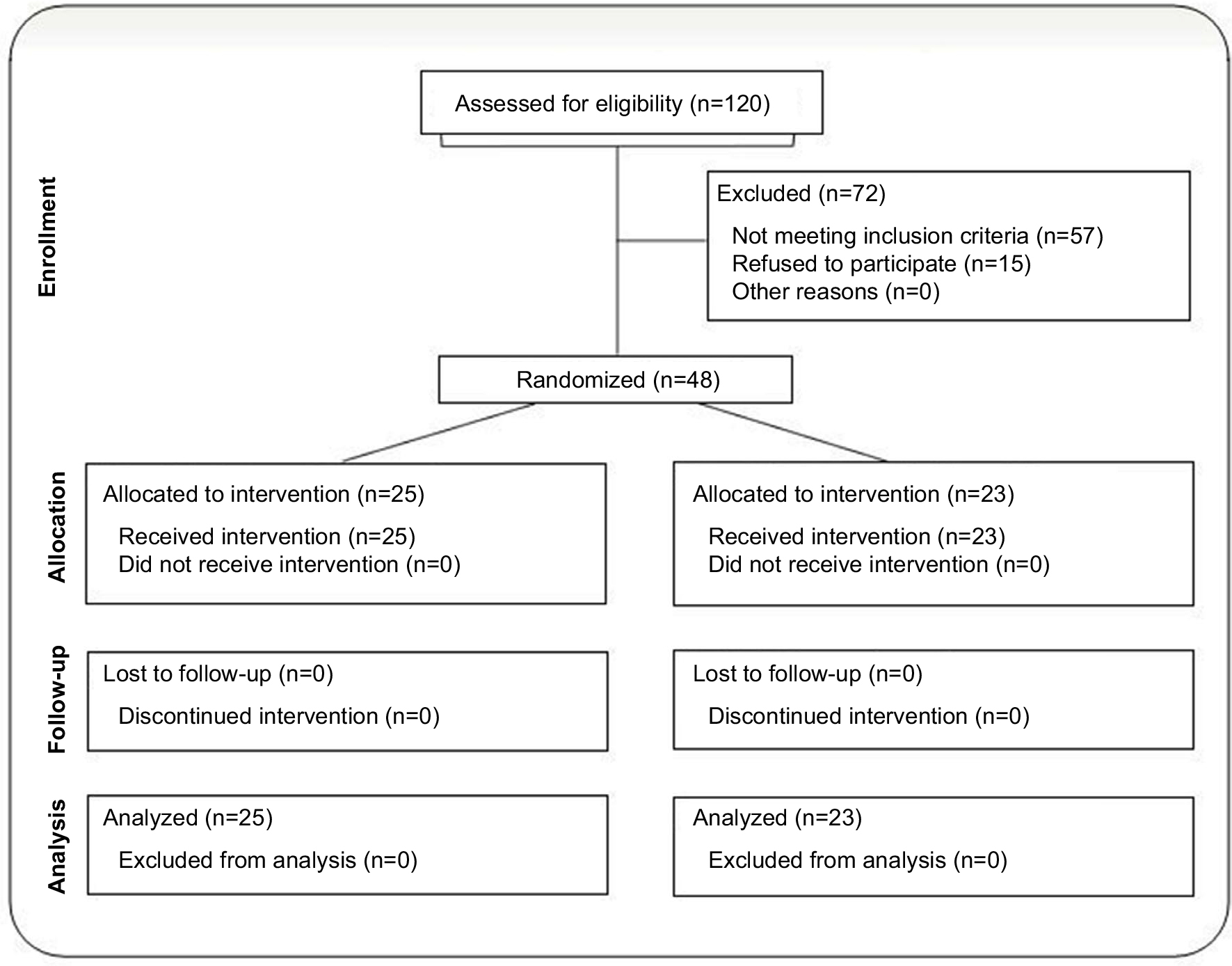 | Figure 1 Consort diagram illustrating patient enrollment, allocation, follow-up, and analysis. |
Data analysis
The patients were grouped into two mutually exclusive categories, namely those who received IV ibuprofen and those who received normal saline placebo. Categorical variables were compared using the Chi-square test, whereas continuous variables were compared using Student’s t-test and analysis of variance (ANOVA). All statistical analysis was conducted using IBM SPSS®v20.2.
Results
Demographics
Between January 2011 and July 2013, 48 male patients aged 20–75 years underwent laparoscopic or open inguinal and/or umbilical hernia repair at the St. Barnabas Medical Center by a single surgeon (RSC) using a standardized technique (Table 1). Among the 25 patients receiving IV ibuprofen, 19 (76.0%) patients were Caucasian, followed by four (16.0%) African Americans, and two (8.0%) Hispanics. In the placebo group, 19 (82.6%) patients were Caucasians, two (8.7%) were Hispanics, one (4.3%) was African American, and one (4.3%) was Asian. There was no significant difference amongst the groups with respect to ethnicity (p=0.437).
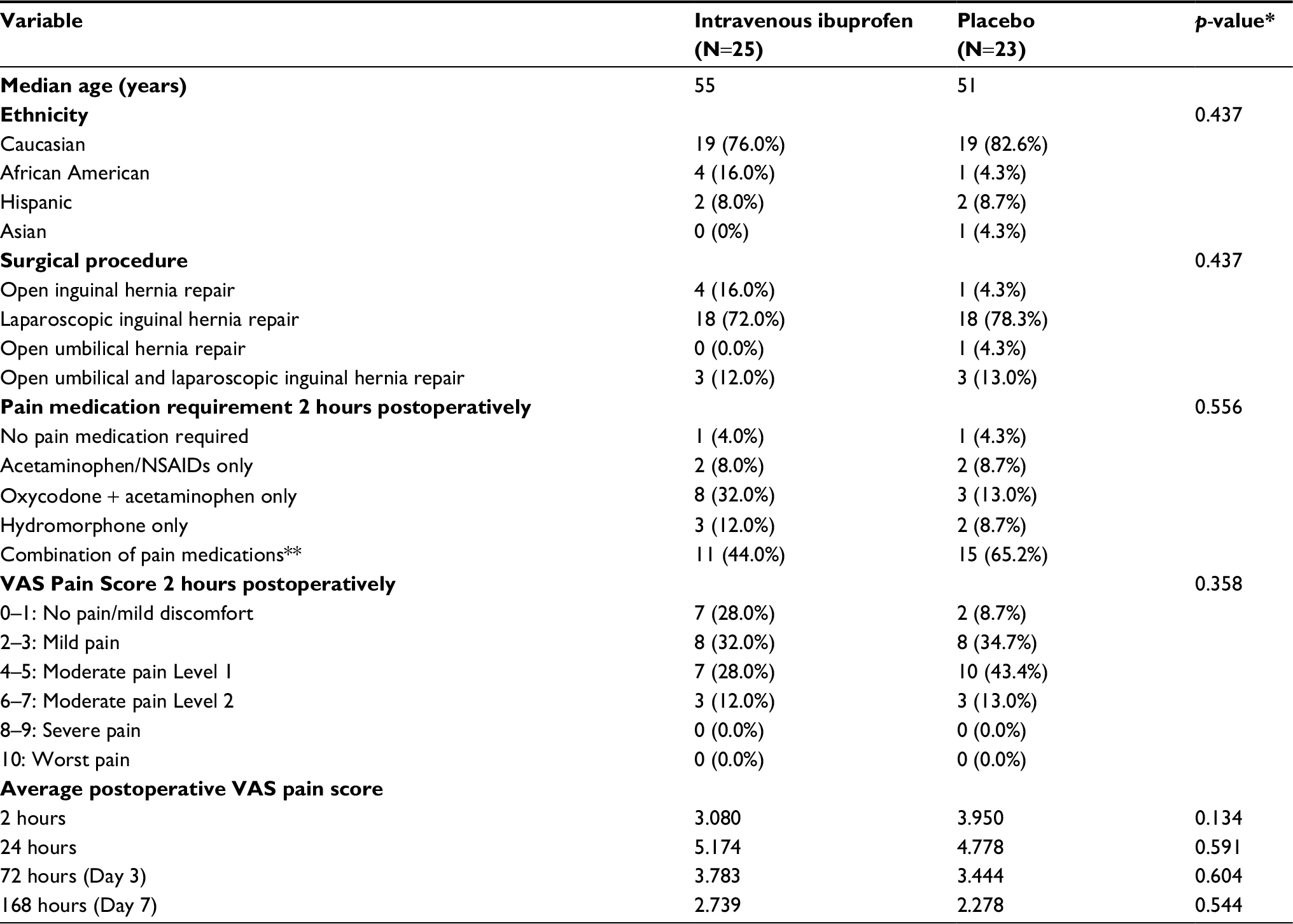 | Table 1 Comparison of patient groups receiving intravenous ibuprofen or placebo Notes: *p-value statistically significant <0.05; **combination of pain medications indicates a combination of acetaminophen/NSAIDs, oxycodone + acetaminophen, and hydromorphone. Abbreviations: VAS, visual analog scale; NSAID, non-steroidal anti-inflammatory. |
Surgical procedure
Laparoscopic inguinal hernia repair was the most common procedure in both groups (72.0% ibuprofen, 78.3% placebo). Among the patients in the IV ibuprofen group, 72.0% (n=18) underwent laparoscopic inguinal hernia repair, 16% (n=4) underwent an open inguinal hernia repair and 12% (n=3) underwent open umbilical and laparoscopic inguinal hernia repair. Of those receiving placebo, 78.3% (n=18) underwent laparoscopic inguinal hernia repair, 13.0% (n=3) underwent open umbilical and laparoscopic inguinal hernia repair, 4.3% (n=1) underwent open inguinal hernia repair and 4.3% (n=1) underwent open umbilical hernia repair. No significant difference amongst the groups with respect to surgical procedure was observed (p=0.437) (Table 1).
Postoperative pain medication requirement
Patients receiving IV ibuprofen required slightly more oxycodone/acetaminophen (32% vs 13%) and IV hydromorphone (12% vs 8.7%) than the placebo group in the first 2 hour period following surgery (Tables 1 and 2). Conversely, patients receiving placebo required more combinations of pain medications (65.2% vs 44%) in the same period. These variations were small however, and did not reach statistical significance (p=0.556).
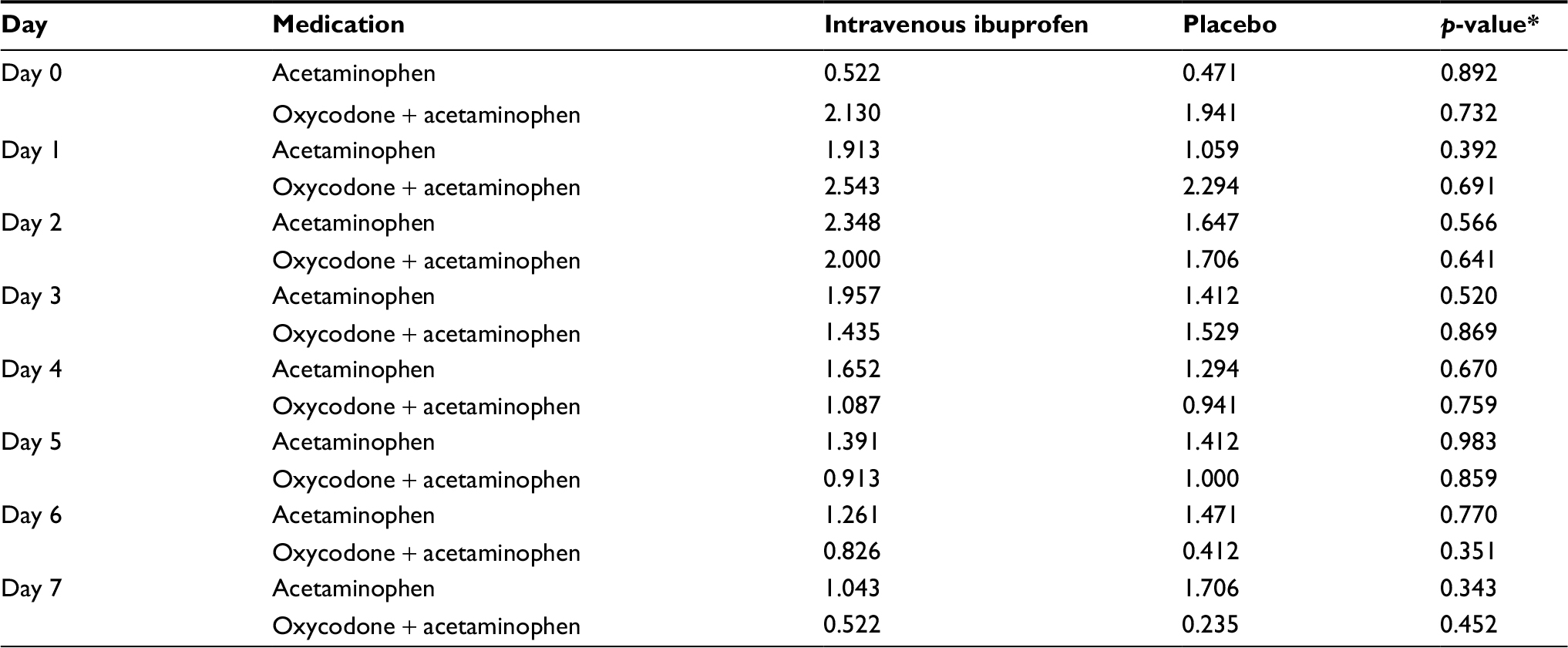 | Table 2 Comparison of the postoperative analgesic requirements among patient groups receiving intravenous ibuprofen or placebo Note: Values refer to average number of pills required for each patient. *p-value statistically significant <0.05. |
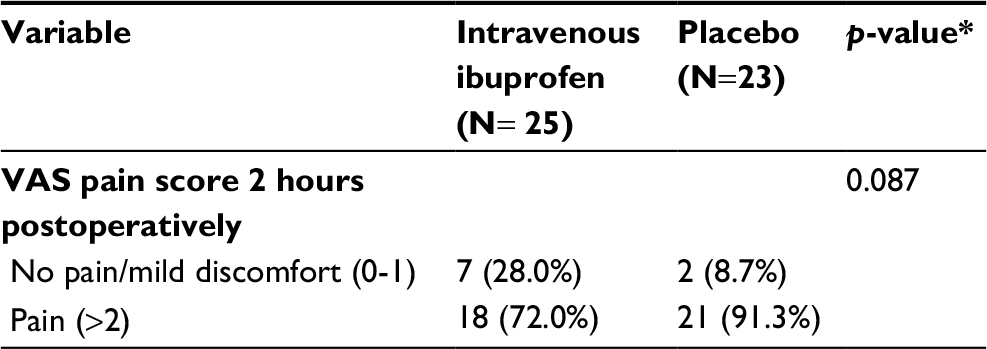 | Table 3 VAS pain score comparison receiving intravenous ibuprofen or placebo Note: *p-value statistically significant <0.05. Abbreviation: VAS, visual analog scale. |
VAS pain score results
The IV ibuprofen group had more patients pain free at two hours postoperatively compared to the placebo group (28.0% vs 8.7%, p=0.087) and the mean/median VAS score was also slightly lower in the IV ibuprofen group (3.08±2.14 vs 3.95±1.54, p=0.134), although neither reached statistical significance (Tables 1 and 2). Pain levels recorded on patient completed questionnaires showed similar levels of pain at 1 (5.17 vs 4.78; p=0.591), 3 (3.78 vs 3.44; p=0.604), and 7 days (2.74 vs 2.28; p=0.544) postoperatively and similar use of rescue medications between the IV ibuprofen and placebo groups.
Upon more detailed analysis, which included analyzing the VAS results into no pain (0–1) versus a pain group (>2) there is a trend towards a reduction in postoperative pain (p=0.087). Similarly, a slight reduction in VAS pain scores were also observed when comparing patients who experienced no pain or mild pain versus those with moderate pain or severe pain, although results were not statistically significant (p=0.254).
Adverse events
One patient in the placebo group experienced nausea and dizziness following surgery. One patient in the IV ibuprofen group complained of tingling at the IV site following surgery. No major serious adverse events were reported, and no readmissions or re-exploration surgeries were required.
Discussion
Effective postoperative pain management is crucial in all surgical patients. Most patients report some degree of pain following surgery, and approximately one third of patients report severe pain.4 In addition to improved patient comfort, adequate pain management reduces the risk of postoperative complications, including fewer pulmonary embolisms and deep vein thrombosis, faster wound healing, earlier mobilization, earlier return of gastrointestinal function, as well as earlier return to baseline functioning.5 Although opioids are effective analgesics, they have numerous undesirable side effects such as hypotension, sedation, and prolonged postoperative ileus which has led to the evaluation of a variety multimodal analgesics, including preoperative NSAIDs.
The current study demonstrated a slight reduction in postoperative pain with the use of IV ibuprofen, although results were not statistically significant, possibly due to inadequate sample size or degree severity and duration of pain generally experienced in the study population. No statistically significant difference was observed in the postoperative analgesic medication requirements for either group as well.
Contrary to the results of our study, previous published studies with larger sample sizes have demonstrated the efficacy of 800 mg IV ibuprofen in reducing postoperative pain and postoperative morphine consumption. Southworth et al (2009) conducted a randomized controlled trial (RCT) involving 406 patients undergoing elective abdominal or orthopedic surgery (139 patients receiving 800 mg IV ibuprofen, 134 patients receiving 400 mg IV ibuprofen, and 134 patients receiving placebo) and reported significant reductions in postoperative pain with the use of 800 mg IV ibuprofen but not 400 mg IV ibuprofen.2 Similarly, Kroll et al conducted an RCT with 319 patients undergoing hysterectomy and reported significant reductions in postoperative pain as well as earlier time to ambulation with the use of 800 mg IV ibuprofen compared to placebo.6
By reducing postoperative pain, NSAIDs can reduce the need for opioid medications and therefore spare the patient from opioid related adverse events such as hypotension, bradycardia, sedation, and respiratory depression. However, NSAID use also has been associated with gastrointestinal complications, such as gastric ulcer disease. Southworth et al published a cumulative safety profile on IV ibuprofen involving 1,601 patients (1,149 patients who received at least one dose of IV ibuprofen and 452 patients receiving placebo) and reported lower rates of adverse events with the use of IV ibuprofen (60% vs 85%) compared to placebo. The three most common side effects included nausea (26% vs 47%), vomiting (9% vs 14%), and constipation (7% vs. 14%). Similar reductions in adverse events rates were seen among elderly patients >65 years.7
In addition to improving patient comfort and reducing opioid related side effects, preoperative IV ibuprofen has been reported to improve patient quality of life. Le et al reported improved overall patient quality of recovery.8 In their study involving 55 adults, Quality of Recovery questionnaire scores were significantly lower in the placebo group, while those receiving IV ibuprofen remained at baseline.8 Furthermore, patients receiving IV ibuprofen had significantly lower intraoperative levels of epinephrine and norepinephrine levels and postoperative levels of cortisol compared to those receiving placebo.8
Limitations
Although the current study identified no benefit to preoperative IV ibuprofen in the studied population, there are several significant limitations to this study. First, this was a single center study and the sample size of this study was small, with only 48 patients in total. Second, the patients were all men, making generalization of these findings across genders impossible. Third, the majority of patients in the current study underwent laparoscopic inguinal hernia repair which is generally associated with mild pain of limited duration which is reflected by the limited pain medication requirement in the placebo. The choice of this population may have diluted an ability to demonstrate a difference (positive or negative) if one exists. Lastly, both open and laparoscopic repair techniques were included, which limits the ability to draw conclusions on when to use preoperative IV ibuprofen. Patients undergoing open techniques are more likely to experience postoperative pain, and may benefit more from preoperative IV ibuprofen. Further large scale studies assessing the impact of IV ibuprofen on both open and laparoscopic hernia repairs are required. Lastly, no cost analysis was conducted with the current study, and further research should be undertaken to analyze the pharmacoeconomics associated with the use of ibuprofen/acetaminophen, compared to narcotics.
Conclusion
Preoperative administration of IV ibuprofen did not significantly reduce postoperative pain among patients undergoing elective hernia repair in this prospective randomized controlled trial. Due to the considerable variability noted in postoperative narcotic usage and the different approach and surgical procedures included, a larger study is needed to better understand the narcotic analgesic requirements associated with IV ibuprofen in open and laparoscopic inguinal hernia and umbilical hernia patients.
Acknowledgment
This study was supported by an unrestricted research grant from Cumberland Pharmaceuticals Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
Caldolor® Product Monograph. 2009. 7-9-2010. https://online.epocrates.com/drugs/549210/Caldolor/Monograph. Accessed June 26, 2017. | ||
Southworth S, Peters J, Rock A, Pavliv L. A multicenter, randomized, double-blind, placebo-controlled trial of intravenous ibuprofen 400 and 800 mg every 6 hours in the management of postoperative pain. Clin Ther. 2009;31:1922–1935. | ||
Morris PE, Promes JT, Guntupalli KK, Wright PE, Arons MM. A multi-center, randomized, double-blind, parallel, placebo-controlled trial to evaluate the efficacy, safety, and pharmacokinetics of intravenous ibuprofen for the treatment of fever in critically ill and non-critically ill adults. Crit Care. 2010;14: Epub 2010 Jun 30. | ||
Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97:534–540. | ||
Koh W, Nguyen KP, Jahr JS. Intravenous non-opioid analgesia for peri- and postoperative pain management: a scientific review of intravenous acetaminophen and ibuprofen. Korean J Anesthesiol. 2015;68:3–12. | ||
Kroll PB, Meadows L, Rock A, Pavliv L. A multicenter, randomized, double-blind, placebo-controlled trial of intravenous ibuprofen (i.v.-ibuprofen) in the management of postoperative pain following abdominal hysterectomy. Pain Pract. 2011;11:23–32. | ||
Southworth SR, Woodward EJ, Peng A, Rock AD. An integrated safety analysis of intravenous ibuprofen (Caldolor(®)) in adults. J Pain Res. 2015;8:753–765. | ||
Le V, Kurnutala L, SchianodiCola J, et al. Premedication with intravenous ibuprofen improves recovery characteristics and stress response in adults undergoing laparoscopic cholecystectomy: a randomized controlled trial. Pain Med. 2016. [Epub ahead of print]. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.