Back to Journals » Clinical and Experimental Gastroenterology » Volume 12
Preoperative esophagogastroduodenoscopy in patients without reflux symptoms undergoing laparoscopic sleeve gastrectomy: utility or futility?
Authors Mazahreh TS ![]() , Aleshawi AJ, Al-Zoubi NA, Allouh MZ
, Aleshawi AJ, Al-Zoubi NA, Allouh MZ ![]() , Jadallah KA
, Jadallah KA ![]() , Elayyan R, Novotny NM
, Elayyan R, Novotny NM ![]()
Received 17 May 2019
Accepted for publication 12 June 2019
Published 3 July 2019 Volume 2019:12 Pages 295—301
DOI https://doi.org/10.2147/CEG.S216188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Everson Artifon
Tagleb S Mazahreh,1 Abdelwahab J Aleshawi,1 Nabil A Al-Zoubi,1 Mohammed Z Allouh,2,3 Khaled A Jadallah,4 Rasheed Elayyan,1 Nathan M Novotny5
1Department of General Surgery and Urology, Faculty of Medicine, Jordan University of Science & Technology, Irbid 22110, Jordan; 2Department of Anatomy, Faculty of Medicine, Jordan University of Science & Technology, Irbid 22110, Jordan; 3Department of Anatomy, College of Medicine & Health Sciences, United Arab Emirates University, Al Ain 17666, UAE; 4Department of Internal Medicine, Faculty of Medicine, Jordan University of Science & Technology, Irbid 22110, Jordan; 5Department of Pediatric Surgery, Beaumont Children’s, Oakland University William Beaumont School of Medicine, Michigan 48073, USA
Aim: To evaluate the value of esophagogastroduodenoscopy (EGD) as a preoperative investigation in individuals without symptoms of Gastro-Esophageal Reflux Disease (GERD) who will undergo laparoscopic sleeve gastrectomy (LSG).
Materials and methods: After Institutional Review Board approval was obtained, patients scheduled for LSG were prospectively enrolled in the study between January 2016 and March 2018. Patients with symptoms of GERD were excluded from the study. Participants were randomly allocated to two groups: individuals who underwent EGD before the surgery as a usual routine investigation (Group A), and individuals who were scheduled without preoperative EGD (Group B). Patient demographics, endoscopic findings, endoscopic biopsy results, and histopathological findings of the resected parts of the stomach after LSG were analyzed and recorded. Additionally, operative characteristics and outcomes, and follow up findings were recorded and analyzed with appropriate statistical methods.
Results: A total of 219 individuals without symptoms of GERD underwent LSG were enrolled. Group A included 111 individuals (25 males and 86 females). Group B comprised 108 individuals (20 males and 88 females). The mean age and mean Body Mass Index (BMI) were similar in both groups. From Group A, 86 out of 111 individuals (77.5%) had no pathology identified on EGD, while 21 individuals (18.9%) were found to have areas of gastric erythema and biopsies showed active gastritis. All LSG operations were performed without any major complication. After one year, all individuals were assessed for the presence of symptomatic GERD and no significant difference was found between the two groups.
Conclusion: Preoperative EGD may not be mandatory for asymptomatic GERD individuals undergoing LSG as post-operative complications and early follow up for GERD symptoms are not significantly different. Further prospective studies with longer follow up are needed to evaluate the role of EGD in individuals undergoing LSG.
Keywords: esophagogastroduodenoscopy, GERD, obesity, laparoscopic sleeve gastrectomy
Introduction
Morbid obesity is a complex and life-threatening disease that is associated with significant co-morbidities.1 According to the World Health Organization, 650 million adults and more than 340 million children and adolescents (5–19 years of age) worldwide were obese in 2016.2 While weight-loss interventions through rigid diet and exercise programs are available, many obese individuals fail those methods. The field of bariatric surgery has become the mainstream care over the past three decades for the management of the most complicated cases of obesity.3,4
The most commonly performed bariatric procedures are LSG and Roux-en-Y gastric bypass (45.9% and 38.3% of all bariatric operations, respectively).5 Each bariatric procedure is tailored to the individual’s overall status and preexisting diseases. The findings from preoperative evaluation need to be taken into consideration when planning the surgery. Preoperative EGD is the best tool for addressing the upper gastrointestinal tract.6 EGD prior to LSG stems from the concern for development of GERD, either de novo or the worsening of preexisting disease.7,8 Thus, in theory, patients planning to undergo LSG could benefit from EGD.
Frustratingly, guidelines, as well as clinical practices regarding routine preoperative EGD vary markedly. The European Association for Endoscopic Surgery recommends routine EGD or radiologic evaluation with a barium meal before bariatric surgery, whereas the Society of American Gastrointestinal and Endoscopic Surgeons recommends EGD only when clinical suspicion of a gastric pathology exists.9,10 A recent survey of British Obesity and Metabolic Surgery Society Members showed that 10% of bariatric units in the United Kingdom consider the preoperative EGD completely unnecessary, whereas 31% include EGD in their routine preoperative assessment.11 Concomitantly, this study aimed at investigating the utility of EGD prior to LSG operation in asymptomatic obese individuals in Jordan.
Materials and methods
This study was conducted at King Abdullah University Hospital (KAUH), a tertiary care center that is affiliated with the Jordan University of Science and Technology, located in Northern Jordan. After obtaining the IRB approval, we prospectively identified, assessed and followed those patients who were scheduled to undergo LSG surgery between January 2016 and March 2018. The following information were obtained: demographics (age, sex, and BMI), clinical characteristics, endoscopic and histopathological findings in individuals who underwent EGD before, length of hospitalization, immediate post-operative complications, histopathological findings from surgical specimens and symptoms of GERD after 1-year of follow up.
Any patient experiencing GERD symptoms was excluded. According to American College of Gastroenterology, these symptoms were mainly heartburn, regurgitation.12 The atypical symptoms (dyspepsia, epigastric pain, nausea, bloating, and belching), were considered to be associated with GERD only if they respond to a trial of Proton Pump Inhibitors (PPIs). The remaining individuals were randomly allocated to two groups; group A and group B. All individuals were stratified and signed an informed consent. Group A underwent EGD prior LSG as a routine investigation, while group B proceeded to LSG without preoperative EGD. The EGD reports for group A were reviewed to identify the presence of hiatal hernia or any other anatomical abnormality, and pathological conditions such as esophagitis, gastritis, duodenitis, and/or ulcers. Biopsies were taken from all individuals with suspected mucosal pathologies.
All individuals were admitted one day prior to surgery. Gastrectomy specimens were sent for histopathological examination and the results were categorized into normal gastric mucosa, active gastritis, chronic gastritis, and other non-gastric pathologies. The length of hospitalization was calculated from the operation day until the day of discharge. Immediate post-operative complications were carefully observed including bleeding and leakage. Also, symptomatic GERD was assessed at a 1-year follow up.
Setting
LSG operations were performed by single bariatric surgeon and the EGD procedures were performed by a consultant gastroenterologist at KAUH. All individuals followed the same procedural guidelines. With introducing of a 36 bougie, all LSG were performed with avoiding the narrowing at the junction of the vertical and horizontal parts of the sleeve. In addition, complete resection of the fundus was insured. Fuji Videogastroscope with ENDO-FLEX Biopsy Forceps (single use); 2.3 mm diameter, 180 cm length, with spike were utilized at EGD.
Statistical analysis
Data were entered into a spread sheet. Statistical analyses were performed using IBM SPSS Statistics Software (v.21), 2012. Categorical variables were described using the frequency distribution, while continuous variables were described using the mean ± Standard Error of the mean. Data was blocked into two groups and examined at the 95% Confidence Interval using Pearson’s chi-square test of association for categorical variables, and student’s t-test for continuous variables after testing for distribution normality. The normality of the distribution of data was tested using the Kolmogorov- Smirnov test. The Mann-Whitney test was used to assess the distribution for each quantitative variable across categories of different variables.
Results
Two hundred and seventy-two patients were eligible for LSG and were enrolled during the study period. Their preoperative characteristics are illustrated in Table 1. Fifty-one individuals were excluded from the study due to the presence of symptoms of GERD prior to LSG. The analyzed groups included 219 individuals (45 males and 174 females). Group A included 111 individuals (25 males and 86 females). Group B comprised 108 individuals (20 males and 88 females). There was no difference between the groups with regards to age (Group A =36.21, and Group B =36.08, P>0.05) or BMI (Group A =43.15, and Group B =43.02, P>0.05). Also, there is no age differences between males and females (males =33.9 and females =36.7).However, males have clinically significant higher BMI than females (males =45.3 and females =42.6) with (P=0.024).
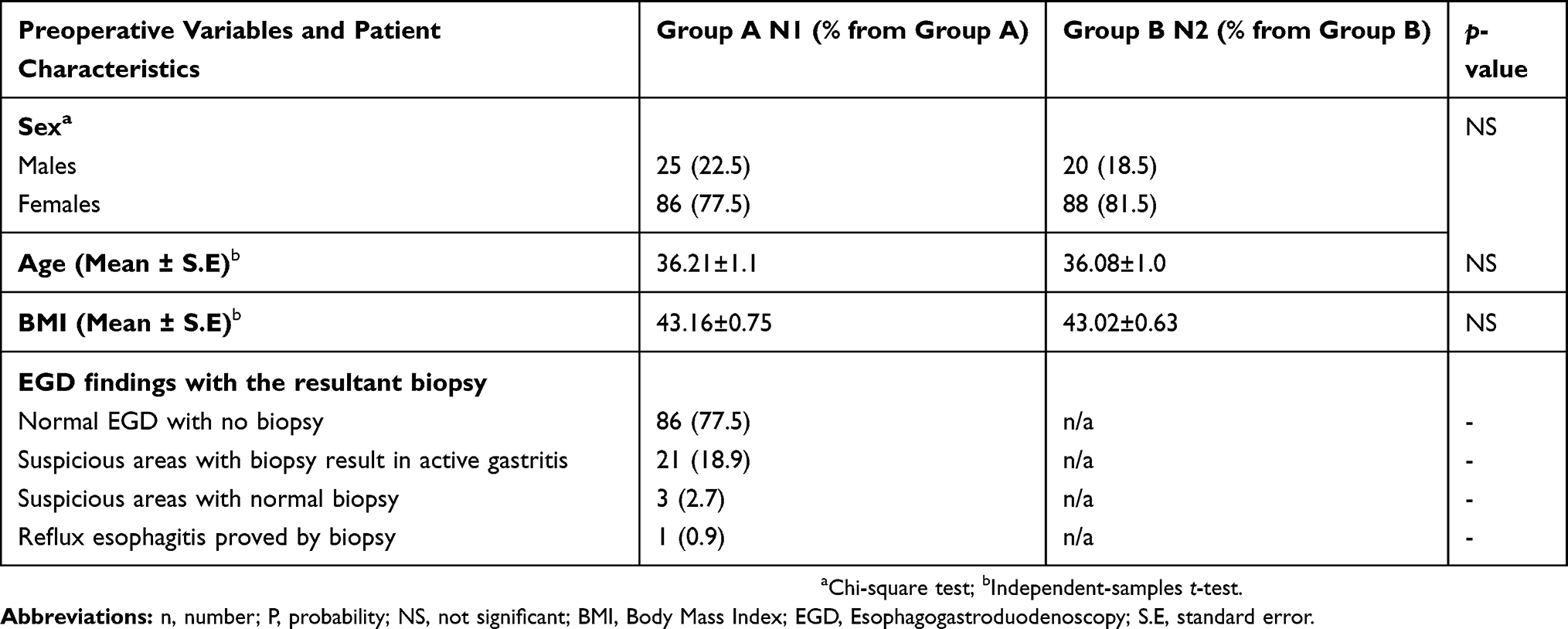 |
Table 1 Preoperative variables and patient characteristics |
Thirty-six individuals (32.4%) from group A were found to have grade 1 hiatal hernia. In addition, two patients with grade 2 hiatal hernias were identified and they underwent LSG with hiatus crus repair. No difference in the prevalence of hiatus hernia was found between males and females. No pathological mucosal lesions were identified in 86 individuals (77.5%) and biopsies were not taken. However, 21 individuals (18.9%) were found to have areas of gastric erythema on EGD and biopsies revealed active gastritis. Another three individuals (2.7%) showed gastric areas suspicious for gastritis and biopsies were taken, but the histopathological exam revealed normal gastric mucosa. One individual (0.9%) of this group was found to have reflux esophagitis which was confirmed by biopsy. In addition, no gender differences in term of endoscopic findings. No cases from group A had EGD-related complications such as bleeding or perforation, nor cardiopulmonary events related to conscious sedation.
The postoperative variables related to LSG with versus without EGD are shown in Table 2. All LSG operations were performed with minimal minor intraoperative and/or immediate postoperative complications (Two bleedings and no leaks in group A, and one bleeding and one leak in group B, P>0.05). The gastric sleeve histopathological specimens were studied and summarized in Table 2. Active gastritis was detected more frequently within group B (P<0.01), and chronic gastritis was discovered more in group A (P<0.01).
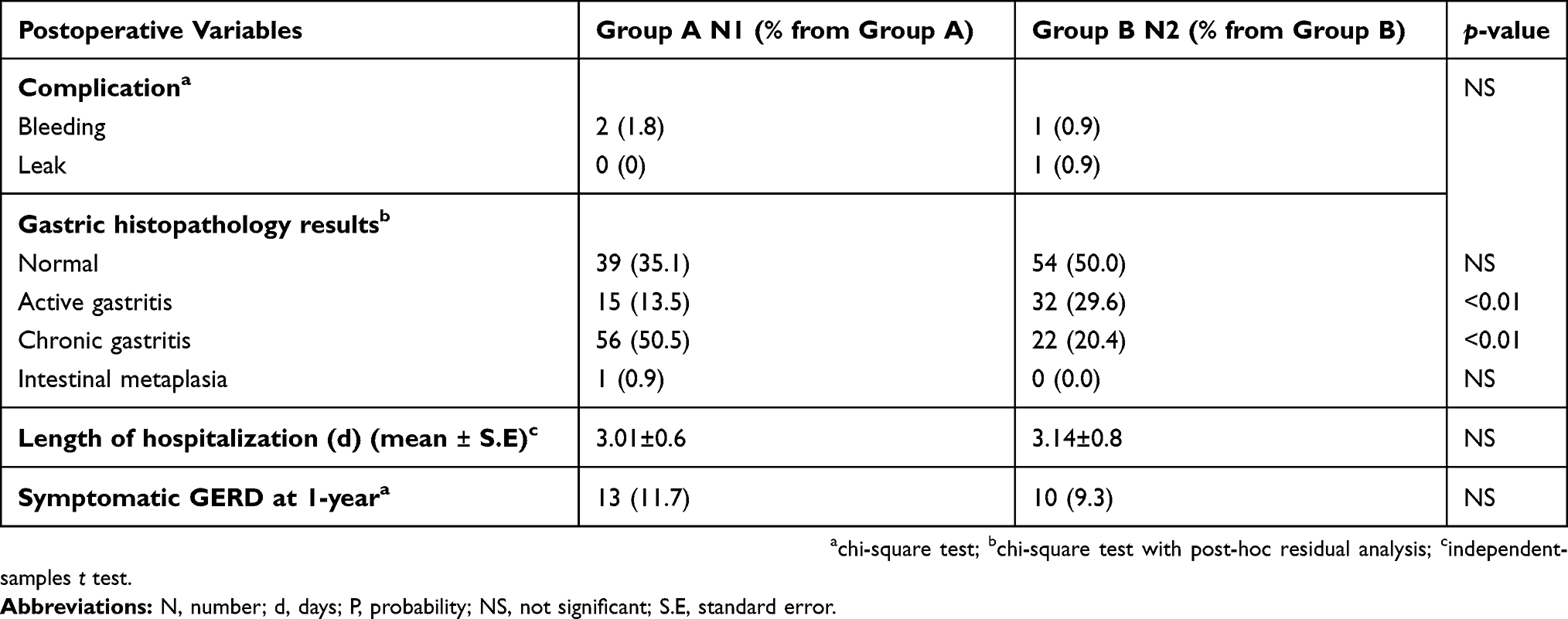 |
Table 2 Postoperative variables related to LSG with versus without EGD |
The mean of length of hospitalization was similar between both groups and was typically 3 days from the operation day to the day of discharge. PPI therapy was prescribed for all individuals on discharge day until one month post-operatively.
After one year, all individuals were assessed for the presence of GERD symptomatology and no significant difference was found between the two groups, with only few individuals complaining of GERD symptoms (Group A=13, and Group B=10, P>0.05). Those with GERD symptoms were treated with PPI therapy with consequent resolution of symptoms. It is worth to mention that the two patients with grade 2 hiatus hernia were not from the aforementioned patients who developed GERD after one year postoperatively.
Discussion
Much debate surrounds the preoperative evaluation of patients who would undergo LSG. Our study attempts to prospectively identify the utility of a costly and invasive procedure that often requires sedation or an anesthetic. We found clinically similar outcomes in both groups. Individuals who did not undergo EGD showed no difference in terms of development of GERD.
The primary motivator for a preoperative EGD before LSG is the fear of accelerating the course of preexisting GERD on esophageal mucosa, which could lead to intolerable reflux symptoms, Barrett’s esophagus, or even esophageal cancer.13 Undoubtedly, individuals with symptoms of GERD or any symptoms related to gastric pathology should have an EGD prior LSG.13 Since gastrointestinal symptoms do not always correspond to the extent of gastric lesions, EGD may still be needed for asymptomatic individuals. These findings in asymptomatic individuals may alter the timing or type of surgery. Mihmanli et al reported that 67% of the individuals who had routine EGD were found to have abnormal endoscopic findings, but only 17% of the individuals were symptomatic.14 Another study found similar results, with around a quarter of patients diagnosed with abnormal endoscopic findings were initially symptomatic.14
In fact, a previous study points out that the majority of the EGD findings were benign or mild and of little clinical significance.6 This raises the question of whether morbidly obese individuals undergoing bariatric surgical evaluation should routinely undergo EGD for evaluation of pathology and foregut anatomy. The instigation of GERD in previously asymptomatic individuals as well as the exacerbation of pre-existing reflux symptoms after LSG has been a main concern linked to the LSG procedure.15,16 The relationship between GERD and LSG is complex and multifactorial. First, the definition of GERD in studies reporting the evolution of the GERD after the LSG is often confusing and based on clinical and subjective appreciation of symptoms by the surgeon in the absence of any standardized questionnaires.15 The definition of hiatal hernia is based on EGD but also the gold standard is considered to be the subjective appreciation of the surgeon during surgery.15 Moreover, three technical errors explain many cases of GERD after LSG: relative narrowing at the junction of the vertical and horizontal parts of the sleeve, dilation of the fundus, and persistence of the hiatus hernia.15 In our study, we were careful to exclude any symptomatic patients and a precise estimation of the hiatus hernia was performed with EGD. In addition, LSG was performed with the aforementioned technical errors in mind taking great care to avoid these pitfalls. As a result, only 23 individuals out of 219 (3.2%) developed de novo GERD during the first year after LSG. No statistically significant difference was found between the two groups.
Bennett et al stated in their meta-analysis that in average-risk, asymptomatic bariatric surgery patients, preoperative EGD should be considered optional. They found that the proportion of EGD findings resulting in a change in surgical management was 7.8%. After removing benign findings with controversial impact on management (hiatal hernia, gastritis, peptic ulcer), this was found to be only 4%.6 Also, Parikh et al reported that selective approach to preoperative EGD may be considered, based on the patients’ symptoms, risk factors, and type of procedure planned as 92.4% of the total had a normal EGD or findings that did not change clinical management and only 7.6% had findings that delayed or altered surgery.17 In addition, Salama et al, recommended the justification of routine preoperative EGD for asymptomatic patients even in regions with low upper GI cancers as the EGD findings had low impact on the management of asymptomatic patients. Crural repair plus LSG was effective for hiatal hernia.18 Moreover, Schigt et al demonstrated that the yield of clinically relevant pathology in EGD before bariatric surgery is very low.19
On the other hand, Carabotti et al stated in their prospective study that the presence of symptoms cannot be considered as a valuable guide to indicate endoscopy since the majority of endoscopic lesions were asymptomatic and not H. pylori-related.20 Also, Madhok et al recommended both the preoperative EGD and a detailed clinical history regarding GERD symptoms be used as they may improve patient selection for LSG. They concluded that avoiding LSG in patients with symptomatic GERD and/or endoscopic evidence of any hiatus hernia or reflux esophagitis may improve procedure selection and reduce the need of conversion to RYGB for refractory reflux.21 Moreover, Mohammed et al recommended the preoperative EGD as the obese patients tend to have enlarged esophageal fat pads which stretches the hiatus. Thus performing a preoperative EGD may assist in making an intraoperative decision if repair is merited.22 More controversy, Praveenraj et al concluded that preoperative EGD yielded a high proportion of endoscopic abnormalities even in asymptomatic patients.23 In addition, Schneider et al recommended performing abdominal ultrasound and EGD before bariatric surgery as they reveal findings, which influence the therapeutic approach.24 Wolter et al emphasize the importance of preoperative EGD because relevant findings in routine preoperative endoscopy are rare but can have significant influence on surgical decision making in bariatric patients independent from the type of bariatric procedure.25 More, Dakour-Aridi et al, Samakar et al, and Santonicola et al reported the routine hiatus hernia repair at the time of LSG does not show an improvement in GERD symptoms.26–29
In general, despite its close relationship with a wide range of gastric disorders, individuals infected with H. pylori are asymptomatic.6 Its assessment is more important for individuals who will undergo Roux-en-Y gastric bypass rather than LSG as H. pylori is a risk factor for peptic ulcer disease, premalignant, or even malignant lesion which we fear about in Roux-en-Y gastric bypass.30 Papasavas et al emphasized that no postoperative adverse effects related to H. pylori status were observed in individuals undergoing LSG.31 Moreover, Loewen et al reported that the endoscopic finding of gastritis/duodenitis, and not the presence of H. pylori, was significantly related to ulcer formation.32
The incidence of upper gastro-intestinal malignancy in asymptomatic individuals is very low.6,30 From the reported outcomes in the Bennett et al review, low rates were detected, with a proportion of gastric malignancy of 0.4%.6 Also, the risk of gastric cancer remains low even in the setting of intestinal metaplasia, with a standardized incidence ratio in a low-risk population of only 2.3%.6 However, the most significant risk has been found in the excluded stomach after Roux-en-Y gastric bypass.6,32
EGD carries general complications that include, but not limited to, perforations which can occur anywhere in the gastrointestinal tract, bleeding, cardio-pulmonary complications, sedation-related complications, infections and allergic reaction to drugs.33 Generally, diagnostic upper endoscopy can be successfully performed under moderate sedation, formerly known as “conscious sedation.” However, bariatric patients are known to require higher sedative doses than non-obese individuals which lead to increased sedation risks.34 In addition, a higher BMI has been thought to be associated with an increased risk of cardio-pulmonary complications during procedural sedation. This may be due to obstructive sleep apnea, pulmonary hypertension, and restrictive lung disease, which are reported to be common in obese patients.35
Our study is not without limitations. The follow up of reflux related symptoms was only for one year which could be construed as short for the development of GERD symptoms. Additionally, due to insurance restraints, our patients could not afford postoperative EGD to evaluate any possible progression of the known hiatal hernias or for migration of the gastroesophageal junction into the chest.
Conclusion
Preoperative EGD may not be mandatory for asymptomatic GERD individuals undergoing LSG as post-operative complications and early follow up for GERD symptoms are not significantly different. Further prospective studies with longer follow up are needed to settle down the ongoing debate about the utility of EGD in individuals undergoing LSG.
Abbreviation list
EGD, Esophago-Gastro-Duodenoscoy; GERD, Gastro-Esophageal Reflux Disease; LSG, Laparoscopic Sleeve Gastrectomy; BMI, Body Mass Index; PPIs, Pump Inhibitors; KAUH, King Abdullah University Hospital.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author.
Ethics and patient consent
Written informed consent was obtained from the patients for publication. Institutional approval was obtained from the Institutional Review Board at Jordan University of Science and Technology. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mathus-Vliegen EM. The role of endoscopy in bariatric surgery. Best Pract Res Clin Gastroenterol. 2008;22(5):839–864. doi:10.1016/j.bpg.2008.07.002
2. World Health Organization. Obesity and overweight. Switzerland: World Health Organization; 2015 Jan. [
3. Wolfe BM, Kvach E, Eckel RH. Treatment of obesity: weight loss and bariatric surgery. Circ Res. 2016;118(11):1844–1855. doi:10.1161/CIRCRESAHA.116.307591
4. Gómez V, Bhalla R, Heckman MG, et al. Routine screening endoscopy before bariatric surgery: is it necessary? Bariatr Surg Pract Individuals Care. 2014;9(4):143–149. doi:10.1089/bari.2014.0024
5. Himpens J, Ramos A, Welbourn R, Kinsman R, Walton P Fourth IFSO global registry report 2018. Dendrite Clinical Systems Ltd, The Hub, Station Road, Henley-on-Thames, Oxfordshire, RG9 1AY, United Kingdom. ISBN 978–0–9929942-7-3; 2018.
6. Bennett S, Gostimir M, Shorr R, Mallick R, Mamazza J, Neville A. The role of routine preoperative upper endoscopy in bariatric surgery: a systematic review and meta-analysis. Surg Obes Relat Dis. 2016;12(5):1116–1125. doi:10.1016/j.soard.2016.04.012
7. Du-Pree CE, Blair K, Steele SR, Martin MJ. Laparoscopic sleeve gastrectomy in individuals with preexisting gastroesophageal reflux disease: a national analysis. JAMA Surg. 2014;149(4):328–334.
8. Felsenreich DM, Kefurt R, Schermann M, et al. Reflux, sleeve dilation, and Barrett’s esophagus after laparoscopic Sleeve gastrectomy: long-term follow-up. ObesSurg. 2017;27(12):3092–3101.
9. Sauerland S, Angrisani L, Belachew M, et al. Obesity surgery: evidence-based guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc. 2005;19(2):200–221.
10. SAGES Guidelines Committee. SAGES guidelines for clinical application of laparoscopic bariatric surgery. Surg Endosc. 2008;22(10):2281–2300. doi:10.1007/s00464-008-9913-0
11. Zanotti D, Elkalaawy M, Hashemi M, Jenkinson A, Adamo M. Current status of preoperative oesophago-gastro-duodenoscopy (OGD) in bariatric NHS units- a BOMSS survey. Obes Surg. 2016;26(9):2257–2262. doi:10.1007/s11695-016-2304-z
12. Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2013;108(3):308–328. quiz 329. doi:10.1038/ajg.2012.444
13. Genco A, Soricelli E, Casella G, et al. Gastroesophagealreflux disease and Barrett’s esophagus after laparoscopic sleeve gastrectomy: a possible, underestimated long-term complication. Surg Obes Relat Dis. 2017;13(4):568–574. doi:10.1016/j.soard.2016.11.029
14. Mihmanli M, Yazici P, Isil G, Tanik C. Should we perform preoperative endoscopy routinelyin obese individuals undergoing bariatric surgery? Bariatr Surg Pract Individuals Care. 2016;11(2):73–77. doi:10.1089/bari.2015.0050
15. Soricelli E, Casella G, Baglio G, Maselli R, Ernesti I, Genco A. Lack of correlation between gastroesophageal reflux disease symptoms and esophageal lesions after sleeve gastrectomy. Surg Obes Relat Dis. 2018;14(6):751–756. doi:10.1016/j.soard.2018.02.008
16. Daes J, Jimenez ME, Said N, Daza JC, Dennis R. Laparoscopic sleeve gastrectomy: symptoms of gastroesophageal reflux can be reduced by changes in surgical technique. Obes Surg. 2012;22(12):1874–1879. doi:10.1007/s11695-012-0746-5
17. Parikh M, Liu J, Vieira D, et al. Preoperative endoscopy prior to bariatric surgery: a systematic review and meta-analysis of the literature. Obes Surg. 2016;26(12):2961–2966. doi:10.1007/s11695-016-2232-y
18. Salama A, Saafan T, El Ansari W, Karam M, Bashah M. Is routine preoperative esophagogastroduodenoscopy screening necessary prior to laparoscopic Sleeve gastrectomy? review of 1555 cases and comparison with current literature. Obes Surg. 2018;28(1):52–60. doi:10.1007/s11695-017-2813-4
19. Schigt A, Coblijn U, Lagarde S, Kuiken S, Scholten P, van Wagensveld B. Is esophagogastroduodenoscopy before Roux-en-Y gastric bypass or sleeve gastrectomy mandatory? Surg Obes Relat Dis. 2014;10(3):411–417. quiz 565–566. doi:10.1016/j.soard.2014.01.015
20. Carabotti M, Avallone M, Cereatti F, et al. Usefulness of upper gastrointestinal symptoms as a driver to prescribe gastroscopy in obese patients candidate to bariatric surgery. A prospective study. Obes Surg. 2016;26(5):1075–1080. doi:10.1007/s11695-015-1861-x
21. Madhok BM, Carr WR, McCormack C, et al. Preoperative endoscopy may reduce the need for revisional surgery for gastro-oesophageal reflux disease following laparoscopic sleeve gastrectomy. Clin Obes. 2016;6(4):268–272. doi:10.1111/cob.12153
22. Mohammed R, Fei P, Phu J, Asai M, Antanavicius G. Efficiency of preoperative esophagogastroduodenoscopy in identifying operable hiatal hernia for bariatric surgery patients. Surg Obes Relat Dis. 2017;13(2):287–290. doi:10.1016/j.soard.2016.08.015
23. Praveenraj P, Gomes RM, Kumar S, et al. Diagnostic yield and clinical implications of preoperative upper gastrointestinal endoscopy in morbidly obese patients undergoing bariatric surgery. J Laparoendosc Adv Surg Tech A. 2015;25(6):465–469. doi:10.1089/lap.2015.0041
24. Schneider R, Lazaridis I, Kraljević M, Beglinger C, Wölnerhanssen B, Peterli R. The impact of preoperative investigations on the management of bariatric patients; results of a cohort of more than 1200 cases. Surg Obes Relat Dis. 2018;14(5):693–699. doi:10.1016/j.soard.2018.01.009
25. Wolter S, Duprée A, Miro J, et al. Upper gastrointestinal endoscopy prior to bariatric surgery-mandatory or expendable? An analysis of 801 cases. Obes Surg. 2017;27(8):1938–1943. doi:10.1007/s11695-017-2622-9
26. Dakour Aridi HN, Tamim H, Mailhac A, Safadi BY. Concomitant hiatal hernia repair with laparoscopic sleeve gastrectomy is safe: analysis of the ACS-NSQIP database. Surg Obes Relat Dis. 2017;13(3):379–384. doi:10.1016/j.soard.2016.09.037
27. Dakour Aridi H, Asali M, Fouani T, Alami RS, Safadi BY. Gastroesophageal reflux disease after laparoscopic Sleeve gastrectomy with concomitant hiatal hernia repair: an unresolved question. Obes Surg. 2017;27(11):2898–2904. doi:10.1007/s11695-017-2702-x
28. Samakar K, McKenzie TJ, Tavakkoli A, Vernon AH, Robinson MK, Shikora SA. The effect of laparoscopic sleeve gastrectomy with concomitant hiatal hernia repair on gastroesophageal reflux disease in the morbidly obese. Obes Surg. 2016;26(1):61–66. doi:10.1007/s11695-015-1737-0
29. Santonicola A, Angrisani L, Cutolo P, Formisano G, Iovino P. The effect of laparoscopic sleeve gastrectomy with or without hiatal hernia repair on gastroesophageal reflux disease in obese patients. Surg Obes Relat Dis. 2014;10(2):250–255. doi:10.1016/j.soard.2013.09.006
30. Saarinen T, Kettunen U, Pietiläinen KH, Juuti A. Is preoperative gastroscopy necessary before sleeve gastrectomy and Roux-en-Y gastric bypass? Surg Obes Relat Dis. 2018;14(6):757–762. doi:10.1016/j.soard.2018.01.021
31. Papasavas PK, Gagne DJ, Donnelly PE, et al. Prevalence of Helicobacter pylori infection and value of preoperative testing and treatment in individuals undergoing laparoscopicRouxen-Y gastric bypass. Surg Obes Relat Dis. 2008;4(3):383–388. doi:10.1016/j.soard.2008.01.006
32. Loewen M, Giovanni J, Barba C. Screening endoscopy before bariatric surgery: a series of 448 individuals. Surg ObesRelat Dis. 2008;4(6):709–712. doi:10.1016/j.soard.2008.02.009
33. Gupta R, Reddy DN. Management of complications of GI endoscopy. Indian J Gastroenterol. 2006;25(Suppl. 1):S29–328.
34. Schumann R. Anaesthesia for bariatric surgery. Best Pract Res Clin Anaesthesiol. 2011;25(1):83–93. doi:10.1016/j.bpa.2011.02.011
35. Vargo JJ. Procedural sedation and obesity: waters left uncharted. Gastrointest Endosc. 2009;70(5):980–984. doi:10.1016/j.gie.2009.07.003
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.