Back to Journals » Clinical Interventions in Aging » Volume 20
Preoperative Cognitive Screening Predicts Postoperative Ambulatory Recovery: A Pilot Study
Authors Cotton JL, Anigbogu C, Stevens-Lapsley JE, Lum HD, Su Y, Bronsert M, Robinson TN, Rove JY
Received 30 January 2025
Accepted for publication 10 July 2025
Published 22 July 2025 Volume 2025:20 Pages 1063—1069
DOI https://doi.org/10.2147/CIA.S517690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Jake L Cotton,1 Chiagoziem Anigbogu,1 Jennifer E Stevens-Lapsley,2 Hillary D Lum,3 Yi Su,4 Michael Bronsert5 ,† Thomas N Robinson,1 Jessica Y Rove6
1Department of Surgery, University of Colorado School of Medicine, Aurora, CO, USA; 2Physical Therapy Program, Department of Physical Medicine and Rehabilitation, University of Colorado Anschutz Medical Campus, Aurora, CO, USA; 3Division of Geriatric Medicine, Department of Medicine, University of Colorado School of Medicine, Aurora, CO, USA; 4University of Colorado School of Medicine, Aurora, CO, USA; 5Surgical Outcomes and Applied Research Program, University of Colorado School of Medicine, Aurora, CO, USA; 6Division of Cardiothoracic Surgery, Department of Surgery, University of Colorado School of Medicine, Aurora, CO, USA
†Michael Bronsert passed away in October 2024
Correspondence: Jessica Y Rove, Division of Cardiothoracic Surgery, Department of Surgery, University of Colorado School of Medicine, 12631 East 17th Avenue, Aurora, CO, C310, USA, Email [email protected]
Purpose: Cardiac surgery patients are older adults at risk for postoperative physical impairment. We hypothesize that screening for mild cognitive impairment (MCI) using the Montreal Cognitive Assessment (MoCA) may identify patients at risk for delayed physical recovery.
Patients and Methods: This is a single center prospective cohort pilot study of patients undergoing elective cardiac surgery. Patients were screened preoperatively for MCI using the MoCA full version 8.1, with scores < 26 defined as a positive screen for MCI. Daily step count, as a practical measure of physical function, was continuously recorded from the preoperative period (baseline) through postoperative day 50 using a commercially available activity tracker.
Results: Eighteen patients met inclusion criteria. Eight (44%) screened positive for MCI and 10 (56%) screened non-impaired (NI). Baseline characteristics and operative outcomes were similar between the MCI and NI cohorts. The MCI cohort did not achieve their preoperative daily step count by postoperative day 50, whereas the NI cohort did so by postoperative day 37. There was a difference in median [IQR] postoperative daily step count (MCI: 3662[2292– 5704] vs NI: 4497[2532– 9216]; p < 0.001).
Conclusion: In a cohort of patients older than 60 undergoing cardiac surgery, a preoperative screen for MCI delayed postoperative physical recovery. A brief preoperative cognitive screen tool may identify patients who could benefit from early intervention for recovery of physical function.
Keywords: ambulation, postoperative recovery, cardiac surgery, cognitive impairment, MoCA
Introduction
As longevity increases, the number of older adults undergoing surgery is increasing.1,2 Hundreds of thousands of adults older than 60 years make up more than half of patients undergoing cardiac surgery in the United States.3 Older age is a risk factor for impaired mobility after surgery and other associated postoperative complications, including delirium.4,5 Multiple studies have demonstrated that postoperative ambulation positively impacts surgical outcomes and is associated with improved cognitive health including rates of delirium and dementia.6–11 Identifying older adults at risk for impaired postoperative mobility preoperatively could enable targeted interventions to enhance ambulation recovery and reduce morbidity.
The Montreal Cognitive Assessment (MoCA) is a validated screening tool to identify patients at risk for mild cognitive impairment (MCI).12 The full version MoCA was developed as a point of care test that can be administered in approximately ten minutes by a trained health-care professional after completion of a one-hour course.12 For these reasons, the MoCA was chosen as a feasible screening exam that can be easily administered without significant resources in a busy surgery clinic. Patients undergoing elective cardiac surgery with cardiopulmonary bypass represent an ideal model to examine how cognitive impairment before elective surgery impacts pre- and post-operative daily step count recovery in older adults as 1) the average patient is 60 years or older, community-dwelling and functionally independent and 2) factors impacting mobility and cognitive impairment can be assessed prospectively with the potential to intervene both before and soon after surgery to prevent or minimize postoperative impairment in mobility.
In this study, we seek to determine how preoperative potential MCI is related to preoperative daily step count and postoperative ambulatory recovery. We perform preoperative screening for MCI using the MoCA and track preoperative and postoperative daily steps continuously for 50 days after cardiac surgery. We hypothesize that patients who screened positive for MCI preoperatively will return to their baseline slower, increasing their risk for complications.
Materials and Methods
We performed a single center, prospective pilot study of patients ≥ 60 years old undergoing planned (elective, non-emergent) coronary and/or valve surgery with cardiopulmonary bypass. Exclusion criteria included patients with a pre-existing clinical diagnosis of dementia in the medical record, non-ambulatory patients or those without a smartphone. Data collection and analysis were conducted from September 2023 through August 2024. Study procedures were approved by Colorado Multiple Institutional Review Board (#23-1394) and comply with the Declaration of Helsinki.
After recruitment and written informed consent, participants were provided with and instructed to wear a commercially available activity tracker (Vivofit 4; Garmin Ltd, Schaffhausen, Switzerland) on their wrist. The activity tracker is validated to track steps with <2% deviation from the gold standard of video observation.13 Additionally, this tracker has a long battery life that does not require charging, allowing participants to continuously wear it for the duration of the study. Baseline daily step count was recorded for up to 30 days preoperatively. Daily step data from three particular days were not included in data analysis as these days did not have a full day of data collection: 1) day the watch was provided, 2) day of surgery, and 3) day the watch was returned. Postoperatively, daily steps were recorded for up to 50 days beginning on postoperative day one. The activity trackers did not require charging and patients were encouraged to wear the activity tracker day and night if able.14 Data from the watch was downloaded for each participant by syncing it with the Garmin Connect app (Garmin Ltd, Schaffhausen, Switzerland) on their smartphone.
After enrollment, patients were screened for MCI using the MoCA version 8.1. Using standard interpretation, participants scoring ≥ 26 were categorized as non-impaired (NI), while those scoring < 26 were categorized as screening positive for MCI.12 Operative and postoperative outcomes including operative approach, operative times, requirement of postoperative mechanical circulatory support, hospital length of stay, participation in cardiac rehabilitation, readmission, discharge destination and return to regular activities were obtained from chart review after return of the activity tracker.
Microsoft Excel (Microsoft, Redmond, WA, USA), the R Project for Statistical Computing (The R Foundation, Vienna, Austria) and REDCap (The REDCap Consortium, Nashville, TN, USA) were used for data management and analysis. Categorical variables were compared using Fisher Exact Test (n < 5) or Chi Squared Test (n ≥ 5). Nonparametric continuous variables (steps per day) were compared using the Wilcoxon rank sum test. P values < 0.05 were considered statistically significant.
Results
Twenty-one patients were enrolled and 18 were included in the analysis. Three patients withdrew from the study (one patient had a stroke, one patient voluntarily withdrew, one patient did not have surgery). Preoperative MoCA identified eight patients (44%) who screened positive for MCI and ten patients (56%) who were screened as NI. For the purpose of this research, we classify these patients into MCI and NI cohorts, although the MoCA is only a screening tool and not diagnostic. Preoperative characteristics including demographics are described in Table 1. There was no difference in baseline demographics or comorbidities. There was no difference in median [IQR] preoperative baseline steps (MCI: 7490 [4942–9763] vs NI: 8099 [6197–11,139]; p = 0.08).
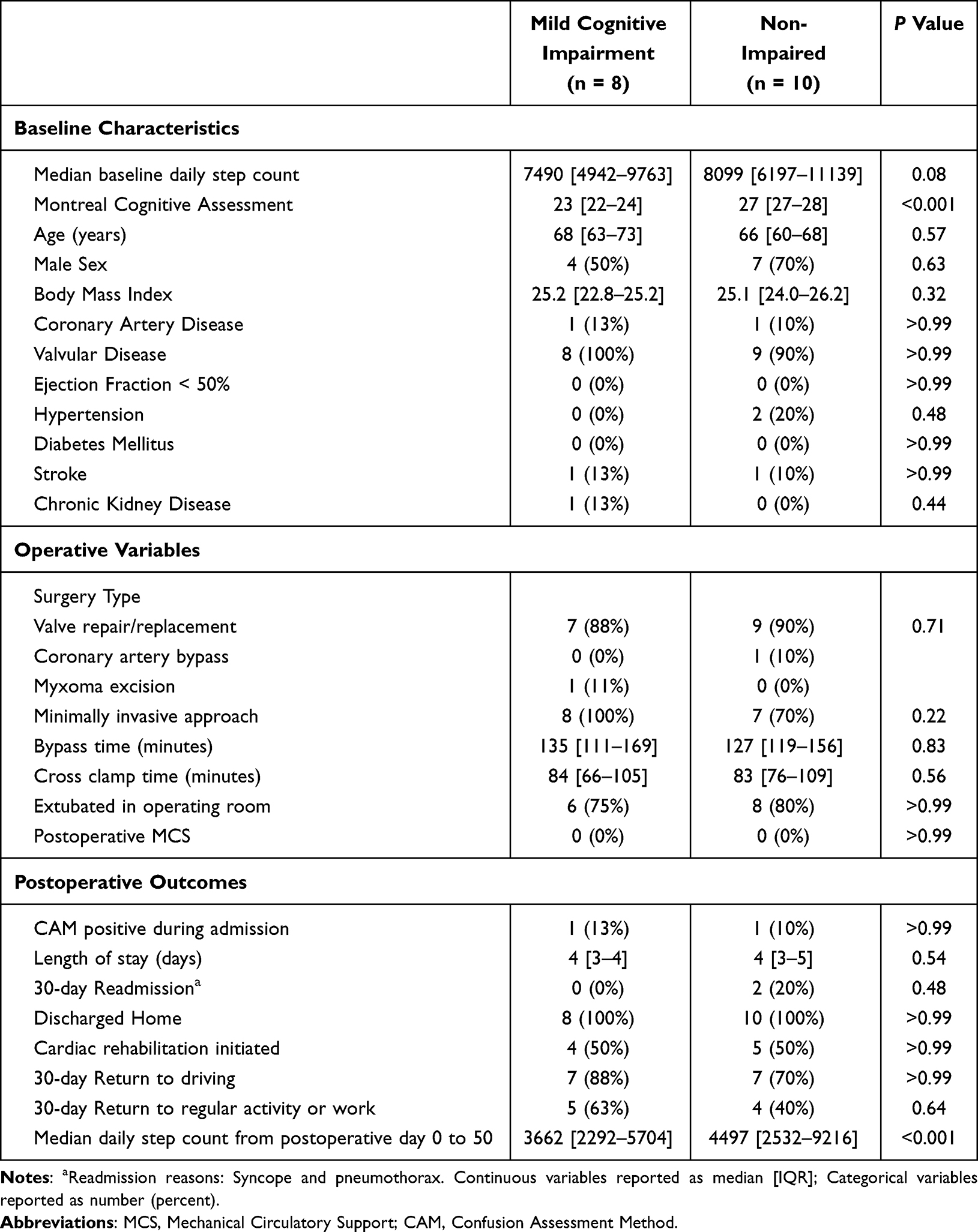 |
Table 1 Baseline Characteristics, Operative Variables and Postoperative Outcomes |
Operative and postoperative variables were compared between the NI and MCI cohorts, described in Table 1. There were no differences in operative approach (sternotomy versus sternotomy-sparing), cardiopulmonary bypass or aortic cross clamp times, operating room extubation rates, need for postoperative mechanical circulatory support, postoperative delirium (as determined by a positive Confusion Assessment Method for Intensive Care Unit [CAM-ICU] assessment) or hospital length of stay.
Postoperative ambulatory recovery is represented graphically for the MCI (Figure 1A) and NI (Figure 1B) cohorts. Daily step counts were positively correlated with postoperative day, showing an increasing trend with increasing postoperative day. The MCI cohort did not reach their preoperative baseline by postoperative day 50. The NI cohort reached their postoperative baseline by postoperative day 37. A comparison of median [IQR] postoperative daily step count by cohort revealed a statistical difference (MCI: 3662 [2292–5704] vs NI: 4497 [2532–9216]; p < 0.001).
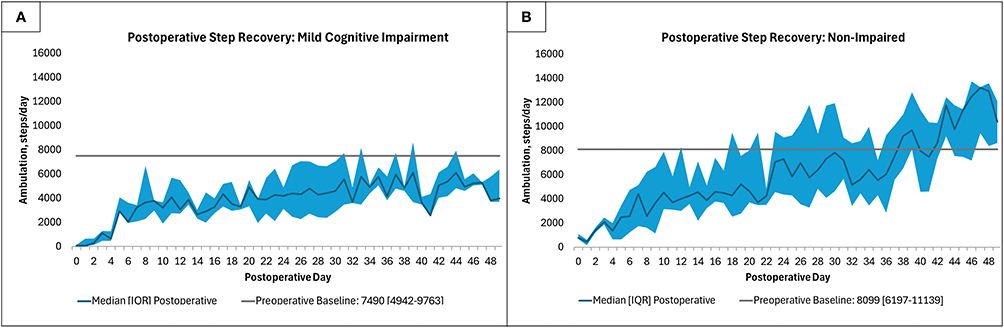 |
Figure 1 Postoperative step recovery was significantly delayed in (A) patients who screened positive for mild cognitive impairment before surgery, compared with (B) patients who had a normal cognitive screen before surgery, p < 0.001. |
There was no difference in evaluated postoperative metrics including hospital length of stay, participation in cardiac rehabilitation, readmission, discharge destination or return to preoperative activities at 30 days postoperative, Table 1.
Discussion
Our data demonstrate that older patients who screen positive for MCI during preoperative assessment for cardiac surgery have delayed ambulation recovery after cardiac surgery compared with their counterparts who do not screen positive for cognitive impairment. Patients without cognitive impairment returned to their preoperative baseline daily step count by postoperative day 37 and then subsequently exceed their preoperative baseline. Impaired mobility demonstrated within the potential MCI cohort is a risk factor for several postoperative complications, which has been demonstrated across surgical subspecialties.15–19 While we did not detect a difference in postoperative metrics within our cohort, this may be due to the study being underpowered for these outcomes. With a larger sample size, differences in these outcomes may become apparent. Additionally, despite not detecting a difference in clinical outcomes, predicting the postoperative ambulation recovery of patients may better help set patient expectations in the preoperative setting. Realistic expectations has been shown to improve patient satisfaction postoperatively.20
There is an aging population of patients undergoing cardiac surgery with a current median age of 63 years.21 As cardiac surgery operative mortality has improved, a call to action has been issued to widen the focus from survival, to optimizing the physical function and cognitive recovery of older adults.22,23 It is increasingly important for the perioperative care of older adults to integrate multidisciplinary recommendations from geriatricians and rehabilitation providers. Older adults undergoing cardiac surgery represent a population of community-dwelling, functionally independent adults at increased risk for undiagnosed MCI as evidenced by 44% of our cohort screening positive. We have demonstrated these patients have a stunted postoperative ambulatory recovery compared with their counterparts despite otherwise similar preoperative and operative characteristics. MCI as a risk factor can be rapidly detected in the presurgical or primary care setting with administration of a 10-minute MoCA. Furthermore, any health-care professional can become certified to administer the MoCA and implement this screening test in a busy, preoperative clinic visit. A positive screen for cognitive impairment with the MoCA may help identify patients, in a resource-limited setting, who will most benefit from early, targeted intervention for recovery of physical function after surgery and neurocognitive follow-up. Alternatively, preoperative cognitive training for this at risk group may have a positive impact on preoperative MCI or potentially on postoperative physiologic outcomes.
We recognize the limitations of our study and the results presented herein should be interpreted in the context of these limitations. Postoperative complications were low in this cohort of patients undergoing elective cardiac surgery, however future studies need to examine whether delayed ambulation is associated with longer term deficits in physical function, postoperative cognitive impairment, patient reported outcomes, or increased health-care utilization. Furthermore, with evidence demonstrating delirium impacts ambulation recovery, future studies should examine how preoperative MoCA may be associated with postoperative delirium, cognitive function and ambulation recovery. Future work will also examine if this relationship between preoperative cognitive impairment and postoperative ambulatory recovery is similar with older adults receiving other types of surgery, and whether short and longer term complications are impacted. This study is also a single center, single surgeon pilot cohort and should be expanded to allow for better generalizability. Future work will evaluate interventions and resources that can be allocated for patients with MCI to aid in their postoperative functional and cognitive recovery. Daily step counts serve as a unique surrogate for preoperative function and are a modifiable variable, pre and postoperatively.24 Wearing an activity tracker as a primary intervention or as part of a broader physical activity intervention can increase daily step counts in older adults including those with cardiovascular disease.25–27 Lastly, median baseline daily step count is approaching statistical significance between the two cohorts, which may impact the significance of differences in postoperative ambulation recovery, although this will require a larger cohort to investigate.
Conclusion
In a cohort of patients older than 60 years undergoing elective cardiac surgery, a high proportion (44%) screened positive for MCI. Preoperative screening for MCI using the MoCA can identify patients at risk for impaired functional recovery after cardiac surgery. Early intervention and resources for these patients may help prevent postoperative complications.
Abbreviations
MCI, mild cognitive impairment; MoCA, Montreal Cognitive Assessment; NI, non-impaired; IQR, interquartile range; CAM-ICU, confusion assessment method for intensive care unit; MCS, mechanical circulatory support.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Informed Consent
This work was approved by Colorado Multiple Institutional Review Board (#23-1394). This study complies with the Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent for participation in the study.
Acknowledgments
The work herein was presented at the 62nd Annual Meeting of the Eastern Cardiothoracic Surgical Society (2024).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Dr Jennifer Stevens-Lapsley reports grants from NIH and VA, outside the submitted work. The authors declare no other potential conflicting interest with respect to the research, authorship, and/or publication of this article.
References
1. Fowler AJ, Abbott TEF, Prowle J, Pearse RM. Age of patients undergoing surgery. Br J Surg. 2019;106(8):1012–1018. doi:10.1002/bjs.11148
2. Etzioni DA, Liu JH, Maggard MA, Ko CY. The aging population and its impact on the surgery workforce. Ann Surg. 2003;238(2):170–177. doi:10.1097/01.SLA.0000081085.98792.3d
3. Kim KM, Arghami A, Habib R, et al. The society of thoracic surgeons adult cardiac surgery database: 2022 update on outcomes and research. The Annals of Thoracic Surgery. 2023;115(3):566–574. doi:10.1016/j.athoracsur.2022.12.033
4. Jin Z, Hu J, Ma D. Postoperative delirium: perioperative assessment, risk reduction, and management. Br J Anaesth. 2020;125(4):492–504. doi:10.1016/j.bja.2020.06.063
5. Tse L, Bowering JB, Schwarz SK, Moore RL, Sztramko R, Barr AM. Incidence and risk factors for impaired mobility in older cardiac surgery patients during the early postoperative period. Geriatr Gerontol Int. 2015;15(3):276–281. doi:10.1111/ggi.12269
6. Borges MGB, Borges DL, Ribeiro MO, Lima LSS, Macedo KCM, Nina V. Early mobilization prescription in patients undergoing cardiac surgery: systematic review. Braz J Cardiovasc Surg. 2022;37(2):227–238. doi:10.21470/1678-9741-2021-0140
7. Del Pozo Cruz B, Ahmadi M, Naismith SL, Stamatakis E. Association of daily step count and intensity with incident dementia in 78 430 adults living in the UK. JAMA Neurol. 2022;79(10):1059–1063. doi:10.1001/jamaneurol.2022.2672
8. Moradian ST, Najafloo M, Mahmoudi H, Ghiasi MS. Early mobilization reduces the atelectasis and pleural effusion in patients undergoing coronary artery bypass graft surgery: a randomized clinical trial. J Vasc Nurs. 2017;35(3):141–145. doi:10.1016/j.jvn.2017.02.001
9. Robinson TN, Kovar A, Carmichael H, Overbey DM, Goode CM, Jones TS. Postoperative delirium is associated with decreased recovery of ambulation one-month after surgery. Am J Surg. 2021;221(4):856–861. doi:10.1016/j.amjsurg.2020.08.031
10. Rosowicz A, Brody JS, Lazar DJ, et al. Early ambulation is associated with improved outcomes following colorectal surgery. Am Surg. 2023;89(12):5225–5233. doi:10.1177/00031348221142590
11. Takahashi T, Kumamaru M, Jenkins S, Saitoh M, Morisawa T, Matsuda H. In-patient step count predicts re-hospitalization after cardiac surgery. J Cardiol. 2015;66(4):286–291. doi:10.1016/j.jjcc.2015.01.006
12. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
13. Foster JI, Williams KL, Timmer BHB, Brauer SG. Concurrent validity of the Garmin Vivofit®4 to accurately record step count in older adults in challenging environments. J Aging Phys Act. 2022;30(5):833–841. doi:10.1123/japa.2021-0231
14. Vivofit 4 owner’s manual. 2017. Available from: https://www8.garmin.com/manuals/webhelp/vivofit4/EN-US/vivofit_4_OM_EN-US.pdf.
15. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91–115. doi:10.1093/ejcts/ezy301
16. Cerantola Y, Valerio M, Persson B, et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: enhanced Recovery After Surgery (ERAS(®)) society recommendations. Clin Nutr. 2013;32(6):879–887. doi:10.1016/j.clnu.2013.09.014
17. Debono B, Wainwright TW, Wang MY, et al. Consensus statement for perioperative care in lumbar spinal fusion: enhanced Recovery After Surgery (ERAS®) Society recommendations. Spine J. 2021;21(5):729–752. doi:10.1016/j.spinee.2021.01.001
18. Dort JC, Farwell DG, Findlay M, et al. Optimal perioperative care in major head and neck cancer surgery with free flap reconstruction: a consensus review and recommendations from the enhanced recovery after surgery society. JAMA Otolaryngol Head Neck Surg. 2017;143(3):292–303. doi:10.1001/jamaoto.2016.2981
19. Higgins RM, Helm M, Gould JC, Kindel TL. Preoperative immobility significantly impacts the risk of postoperative complications in bariatric surgery patients. Surg Obes Relat Dis. 2018;14(6):842–848. doi:10.1016/j.soard.2018.02.025
20. Zhang H, Glassman SD, Bisson EF, Potts EA, Jazini E, Carreon LY. Patient expectations impact patient-reported outcomes and satisfaction after lumbar fusion. Spine J. 2024;24(2):273–277. doi:10.1016/j.spinee.2023.09.023
21. Metkus TS, Alviar CL, Baird-Zars VM, et al. Presentation and outcomes of patients with preoperative critical illness undergoing cardiac surgery. JACC Adv. 2023;2(2):100260. doi:10.1016/j.jacadv.2023.100260
22. Damluji AA, Forman DE, van Diepen S, et al. Older adults in the cardiac intensive care unit: factoring geriatric syndromes in the management, prognosis, and process of care: a scientific statement from the American heart association. Circulation. 2020;141(2):e6–e32. doi:10.1161/cir.0000000000000741
23. Forman DE, Rich MW, Alexander KP, et al. Cardiac care for older adults. Time for a new paradigm. J Am Coll Cardiol. 2011;57(18):1801–1810. doi:10.1016/j.jacc.2011.02.014
24. Suri A, VanSwearingen J, Baillargeon EM, et al. Association of gait quality with daily-life mobility: an actigraphy and global positioning system based analysis in older adults. IEEE Trans Biomed Eng. 2024;71(1):130–138. doi:10.1109/tbme.2023.3293752
25. Ashur C, Cascino TM, Lewis C, et al. Do wearable activity trackers increase physical activity among cardiac rehabilitation participants? A systematic review and meta-analysis. J Cardiopulm Rehabil Prev. 2021;41(4):249–256. doi:10.1097/hcr.0000000000000592
26. Brickwood KJ, Ahuja KDK, Watson G, O’Brien JA, Williams AD. Effects of activity tracker use with health professional support or telephone counseling on maintenance of physical activity and health outcomes in older adults: randomized controlled trial. JMIR mHealth uHealth. 2021;9(1):e18686. doi:10.2196/18686
27. Brickwood KJ, Watson G, O’Brien J, Williams AD. Consumer-based wearable activity trackers increase physical activity participation: systematic review and meta-analysis. JMIR mHealth uHealth. 2019;7(4):e11819. doi:10.2196/11819
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.