Back to Journals » International Journal of Women's Health » Volume 17
Prenatal Screening for Monosomy X in the First Trimester: A Comparison of a Thai Predictive Model and the Fetal Medicine Foundation Algorithm
Authors Kongsung N, Tongprasert F ![]() , Kunanukulwatana C, Tongsong T
, Kunanukulwatana C, Tongsong T ![]()
Received 29 September 2025
Accepted for publication 17 November 2025
Published 24 November 2025 Volume 2025:17 Pages 4769—4778
DOI https://doi.org/10.2147/IJWH.S566415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Vinay Kumar
Nudchanad Kongsung,1 Fuanglada Tongprasert,1,2 Chayanid Kunanukulwatana,1 Theera Tongsong2
1Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 2Fetal Center, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Correspondence: Fuanglada Tongprasert, Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand, Tel +66-53-935552, Email [email protected]
Purpose: This study aimed to evaluate the performance of the first-trimester Fetal Medicine Foundation (FMF) algorithm in predicting monosomy X and compare it with a Thai NT-based model using nuchal translucency (NT) alone or combined with maternal serum markers.
Patients and Methods: This retrospective study analyzed 6,860 singleton pregnancies screened at 11– 13+6 weeks. Monosomy X risk was estimated based on the trisomy 21 risk calculated by the FMF algorithm and Thai logistic regression models based on NT alone, NT with pregnancy-associated plasma protein A (PAPP-A), and NT with PAPP-A and beta-human chorionic gonadotropin (β-hCG).
Results: Thirty cases of monosomy X were identified (0.4%), all of which were confirmed prenatally by invasive diagnostic procedures, including amniocentesis, chorionic villus sampling, or cordocentesis. The Thai model using NT and PAPP-A had the highest area under the receiver operating characteristic curve (AUC) of 0.953, with a sensitivity of 86.7% and a specificity of 94.1%. NT alone also showed strong performance (sensitivity 83.3%, specificity 94.4%). The FMF algorithm achieved the highest specificity (97.9%) but lower sensitivity (53.3%). Adding β-hCG did not improve performance.
Conclusion: NT alone or combined with PAPP-A outperformed the FMF algorithm for monosomy X screening, with NT alone being particularly useful in settings without biochemical testing. The FMF algorithm, while primarily designed for trisomy 21 risk estimation, can also provide monosomy X risk within the same report at no additional cost, which is especially valuable in resource-limited settings where biochemical testing or NIPT is not widely accessible.
Keywords: Turner syndrome, first trimester screening, nuchal translucency, PAPP-A, FMF algorithm
Introduction
Monosomy X, or Turner syndrome, is one of the most common sex chromosome abnormalities.1 Although prenatal diagnosis is possible in current practice, many cases remain undetected until later in life. Some affected fetuses may present with sonographic findings such as increased nuchal translucency (NT), hydrops fetalis, cystic hygroma, or other congenital anomalies.2 Early detection enables timely genetic counseling, prenatal diagnosis, and informed decision-making.3 In cases of severe anomalies, families may opt for pregnancy termination; if the pregnancy continues, prenatal diagnosis facilitates coordinated perinatal care and psychosocial support.4
First trimester screening for monosomy X typically relies on NT measurement, which is often more pronounced than in trisomy 21.5 Maternal serum markers—such as pregnancy-associated plasma protein-A (PAPP-A) and free β-human chorionic gonadotropin (β-hCG)—may enhance detection, although PAPP-A is generally reduced and β-hCG levels are variable, limiting their diagnostic value.6,7 Non-invasive prenatal testing (NIPT), which analyzes cell-free fetal DNA, provides high accuracy for detecting common aneuploidies, including monosomy X.8,9 However, its performance for monosomy X is inferior to that for trisomy 21, partly due to maternal X chromosome mosaicism and confined placental mosaicism. Additionally, the high cost of NIPT limits its accessibility in many low-resource settings.8,10
In practice, ultrasound remains the primary screening modality for monosomy X in prenatal care, with NT as the key marker.11 Although NT alone can aid in identifying affected fetuses, it is also incorporated into multivariable risk algorithms—such as the Fetal Medicine Foundation (FMF) algorithm—which integrate maternal characteristics, NT, fetal heart rate (FHR), and optionally serum biochemistry to assess the risk of common chromosomal abnormalities.12,13 The FMF algorithm is widely accessible and can function with or without biochemical input, making it particularly suitable for resource-limited settings, as previously published by our research group in a study on trisomy screening in a Thai cohort.14,15 However, it was originally designed to estimate trisomy 21 risk and not specifically for monosomy X. While it could theoretically predict monosomy X, its performance for this indication has not been evaluated. Accordingly, we conducted this study to assess the performance of the first trimester FMF algorithm, which estimates trisomy 21 risk, in predicting monosomy X in Thai pregnancies at 11–13+6 weeks of gestation and to compare its performance with that of a newly developed Thai model using NT alone or in combination with first trimester serum markers.
Materials and Methods
This diagnostic study, conducted as a secondary analysis of an existing dataset, focused on pregnant women between 11 and 13+6 weeks of gestation who underwent first trimester aneuploidy screening at Maharaj Nakorn Chiang Mai Hospital, Chiang Mai, Thailand, between January 2010 and December 2023. The study received ethical approval from the Institutional Review Board of the Faculty of Medicine, Chiang Mai University (Research ID: OBG-2568-0182, approval date: 4 April 2025). The need for individual patient consent was waived because the study was a retrospective analysis of an existing anonymized database. All data were handled confidentially and in accordance with the Declaration of Helsinki.
Database Development
The database was developed as part of the project titled “Down Syndrome Screening of the National Research University of Thailand” by the Maternal-Fetal Medicine Team, Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University. Pregnant women attending the antenatal care clinic during their first trimester were invited to participate. Upon recruitment, they received genetic counseling, were offered first trimester aneuploidy screening, and provided written informed consent. All participants underwent first trimester aneuploidy screening through ultrasound examination and/or a combination of maternal serum biochemical markers, including PAPP-A and free β-hCG. Participants were also asked to provide detailed information on maternal characteristics (eg, age, body weight, ethnicity, smoking history, family medical history, pre-existing medical conditions, particularly diabetes) and obstetric history (eg, menstrual history, parity, gestational age at screening, and history of a previous child with aneuploidy). The collected demographic data, serum biochemical marker results, and ultrasound parameters—including crown-rump length (CRL), NT, and FHR—were prospectively recorded in the database. All participants were followed up to document final pregnancy outcomes, which were evaluated by obstetricians, while neonatal outcomes were assessed by the project’s pediatric team. The diagnosis of aneuploidies was confirmed through cytogenetic analysis of samples obtained via chorionic villus sampling, amniocentesis, cordocentesis, or postnatal investigation. For cases where chromosomal studies were not performed, the absence of aneuploidies was determined by neonatologists or pediatricians based on clinical characteristics.
Data Retrieval
Records from the database were accessed based on the following inclusion criteria: (1) singleton pregnancies, (2) gestational age between 11 weeks and 13+6 weeks as determined by CRL measurement at the time of recruitment, and (3) known fetal aneuploidy status. Pregnancies with congenital anomalies, chromosomal abnormalities other than monosomy X, medically indicated terminations before 24 weeks, or those without first-trimester NT measurement and biochemical screening (PAPP-A and β-hCG) were excluded.
Monosomy X Risk Determination
From the retrieved dataset, variables required for input into the FMF algorithm were validated by the first author (FT). These variables included maternal characteristics (date of birth and history of trisomy in a previous child), ultrasound findings (CRL, NT, and FHR) and biochemical markers (PAPP-A and β-hCG). Once validated, the data were extracted and provided to the authors (NK and CK), who were blinded to the final diagnosis. Individual risks for trisomy 21 were calculated using the FMF algorithm via its online platform, accessible at https://fetalmedicine.org/research/assess/ trisomies. These calculated risk estimates were repurposed as monosomy X risk values and incorporated into the main dataset for subsequent analysis. Monosomy X risk was then categorized into two groups: low risk (<1:250) and high risk (>1:250). Pregnancy outcomes, including fetal or neonatal karyotyping results, gestational age at delivery, birth weight, and any complications, were documented. Neonatal outcomes were classified as either normal or affected by monosomy X.
Development of the Thai Predictive Model
To develop the Thai predictive model, three binary logistic regression models were constructed: the first using NT alone; the second combining NT with PAPP-A (MoM); and the third incorporating NT, PAPP-A (MoM), and β-hCG (MoM). Each model was expressed as a logistic regression equation and used to generate the logit values for each case. The predicted probability of monosomy X for each model was then calculated using the inverse logit transformation of the linear predictor (lp), as follows: probability = elp/(1 + elp), where e is the base of the natural logarithm.
Statistical Analysis
Data were analyzed using Stata version 16 (StataCorp, College Station, TX, USA). Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as mean and standard deviation or median with interquartile range, depending on data distribution. Group differences in categorical variables were assessed using an exact probability test. For continuous variables, comparisons were made using either an independent t-test or the Mann–Whitney U-test, as appropriate. The performance of each prediction model was evaluated separately. Discriminative ability was assessed using the area under the receiver operating characteristic (ROC) curve (AUC), which served as the primary metric for model performance. Differences in AUCs were tested for statistical significance using the paired-sample design method proposed by DeLong et al,16 with a p-value of < 0.05 considered statistically significant. If no statistically significant differences were found, the simpler or less complex model was preferred. Calibration plots were constructed to assess the agreement between predicted probabilities of monosomy X and observed proportions. Diagnostic performance was further assessed by calculating sensitivity, specificity, positive predictive values (PPV), negative predictive values (NPV), and positive likelihood ratio (LR+) for each model, using a risk threshold of 1:250 to compare the FMF algorithm with the newly developed prediction models.
Results
A total of 9,612 participants were enrolled in the study. As illustrated in Figure 1, 2,752 (28.6%) were excluded due to the absence of serum biochemical marker results (95.0%), missing outcomes or incomplete data (3.2%), and the presence of common trisomies or other chromosomal aberrations (1.8%). The excluded chromosomal abnormalities included trisomy 21 (28 cases), trisomy 18 (9 cases), trisomy 13 (9 cases), 46,XY del(1)(q11), 46,X,inv(Y)pat, and 45,X/46,XY mosaicism. The remaining 6,860 participants were included in the analysis and classified as either normal or affected by monosomy X. The incidence of monosomy X in the study population was 30 cases (0.44%). All cases were confirmed prenatally by invasive diagnostic procedures, including chorionic villus sampling (25 cases), amniocentesis (3 cases), and cordocentesis (2 cases). A comparative analysis between pregnancies with normal chromosomes and those affected by monosomy X revealed no statistically significant differences in maternal age, gestational age at the time of screening, or FHR. However, NT measurements were significantly higher in the monosomy X group compared to the normal group, both in mean values (4.44 ± 2.85 vs 1.04 ± 0.41 MoM, p < 0.001) and median values (4.12 vs 1.00 MoM, p < 0.001). Additionally, PAPP-A levels were significantly lower in the monosomy X group. In contrast, β-hCG levels did not differ significantly between groups, suggesting limited utility of this marker alone for detecting monosomy X. Additional baseline characteristics are presented in Table 1.
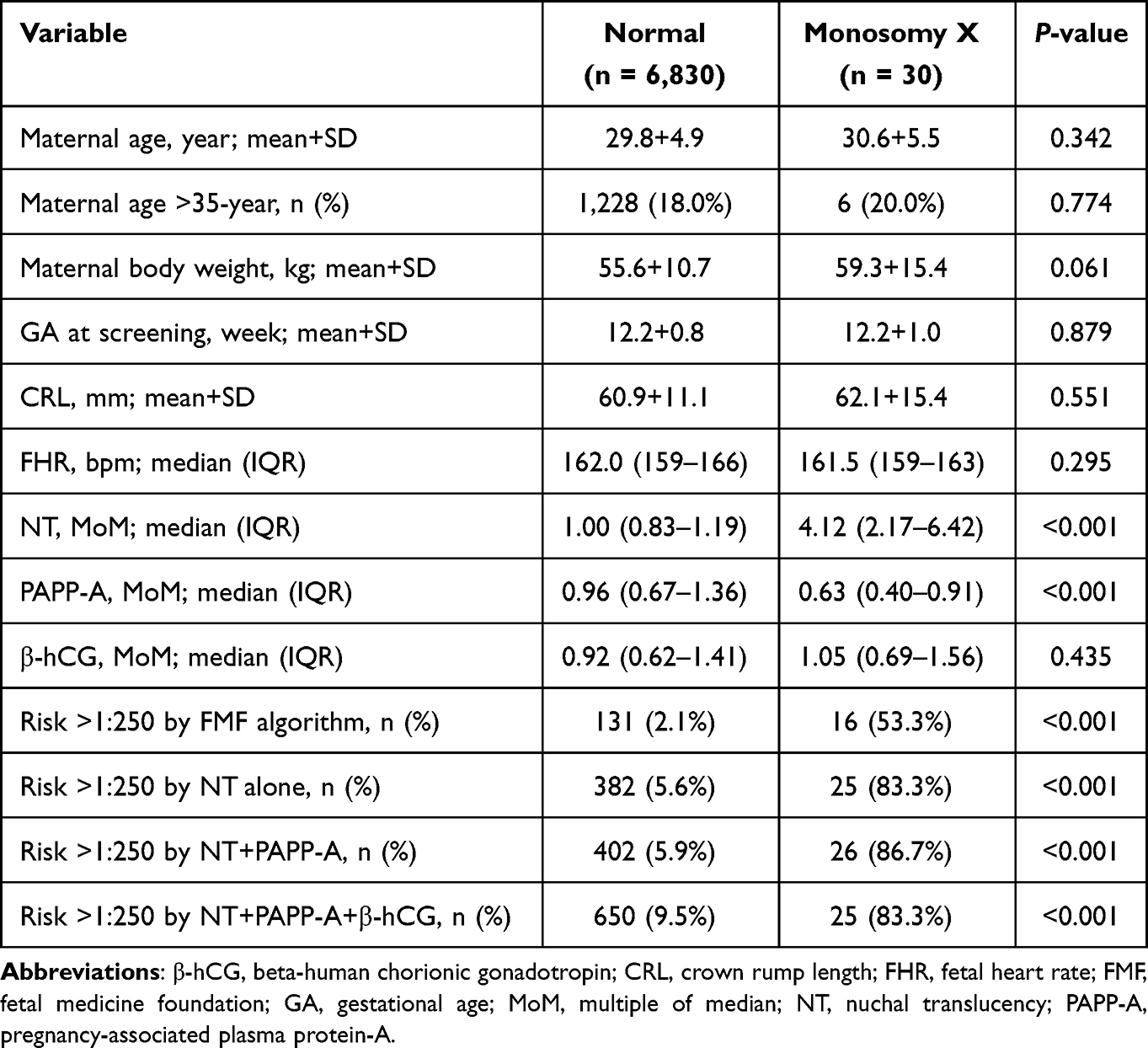 |
Table 1 Baseline Characteristics of Participants in the Study Cohort |
 |
Figure 1 Flowchart of participant enrollment. |
Risk assessment using the FMF algorithm, the Thai NT alone model, the NT + PAPP-A model, and the NT + PAPP-A + β-hCG model identified significantly higher proportions of high-risk cases (defined as risk > 1:250) among pregnancies affected by monosomy X, with detection rates of 53.3%, 83.3%, 86.7%, and 83.3%, respectively. The discriminative performance of different screening models was evaluated by ROC curve analyses as shown in Table 2 and Figure 2. The FMF algorithm demonstrated a significantly lower AUC compared to the NT alone model (AUC: 0.856; 95% CI: 0.779–0.933 vs 0.916; 95% CI: 0.834–0.997; p = 0.026). The NT + PAPP-A model increased the AUC to 0.953 (95% CI: 0.910–0.995), while the NT + PAPP-A + β-hCG model yielded an AUC of 0.950 (95% CI: 0.905–0.995); however, neither addition resulted in a statistically significant improvement compared to the NT alone model.
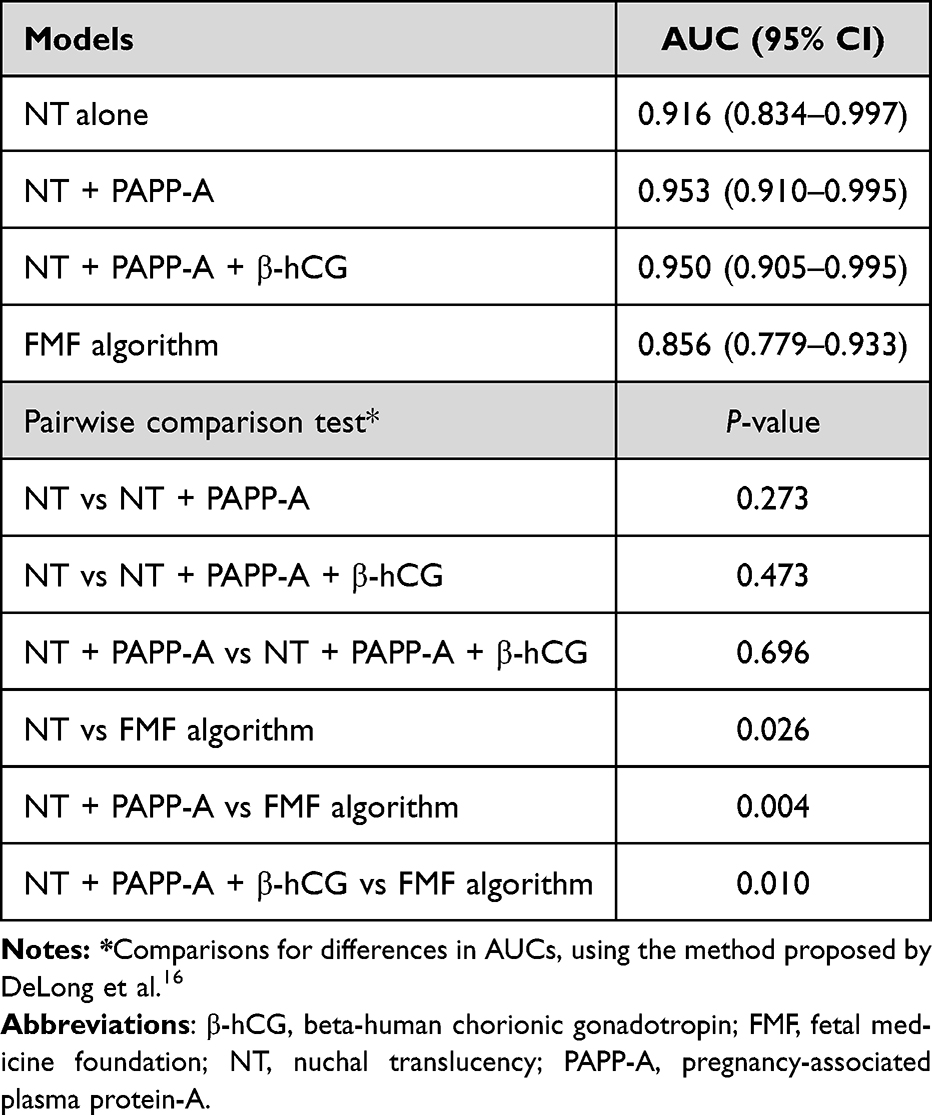 |
Table 2 Comparison of Areas Under the Roc Curves (AUCs) Between Various Models in Predicting Monosomy X in the First Trimester |
 |
Figure 2 Receiver operating characteristic (ROC) curves comparing the discriminative performance of the FMF algorithm, the NT alone model, the NT + PAPP-A model, and the NT + PAPP-A + β-hCG model in predicting monosomy X. The area under the curve (AUC) values were 0.856, 0.916, 0.953, and 0.950, respectively. |
A Thai predictive model was developed to estimate the probability of monosomy X in individual cases. The best-performing model, which included NT (MoM), PAPP-A (MoM), and a constant, is presented in Table 3. Equations of the three Thai predictive models are as follows:
 |
Table 3 Multivariable Logistic Regression Analysis for the Best First Trimester Predictive Model of Monosomy X Using NT and PAPP-A (MoM) |
- NT alone: log (XO) = −0.0576466 + 0.0586722 x (NT: MoM)
- NT+PAPP-A: log (XO) = −6.672417 + 1.295944 x (NT: MoM) −1.625955 x (PAPP-A: MoM)
- NT+PAPP-A+ β-hCG: log (XO) = −0.0545971 + 0.0585529 x (NT: MoM) −0.0050431 x (PAPP-A: MoM) + 0.0022343 x (β-hCG: MoM)
As summarized in Table 4, the NT alone model demonstrated high sensitivity (83.3%) and specificity (94.4%), with a strong positive likelihood ratio (14.9) and an excellent NPV (99.9%). The NT + PAPP-A model slightly improved sensitivity to 86.7%, with a marginal reduction in specificity (94.1%) and maintained a high NPV (99.9%). The NT + PAPP-A + β-hCG model did not improve overall detection, showing reduced specificity (90.5%) and PPV (3.7%), indicating a higher false-positive rate, although the NPV remained high at 99.8%. The FMF algorithm yielded the highest specificity (97.9%) and PPV (10.9%) but substantially lower sensitivity (53.3%), limiting its effectiveness. Overall, NT-based models, particularly when combined with PAPP-A, served as the most effective model for early detection of monosomy X. Figure 3 shows the calibration plot, demonstrating the calibration plot with excellent agreement between predicted and observed probabilities, with an observed-to-expected ratio of 1.000, calibration-in-the-large of 0.000, and a calibration slope of 1.000. The model showed excellent discrimination, with an AUC of 0.953, indicating strong predictive performance.
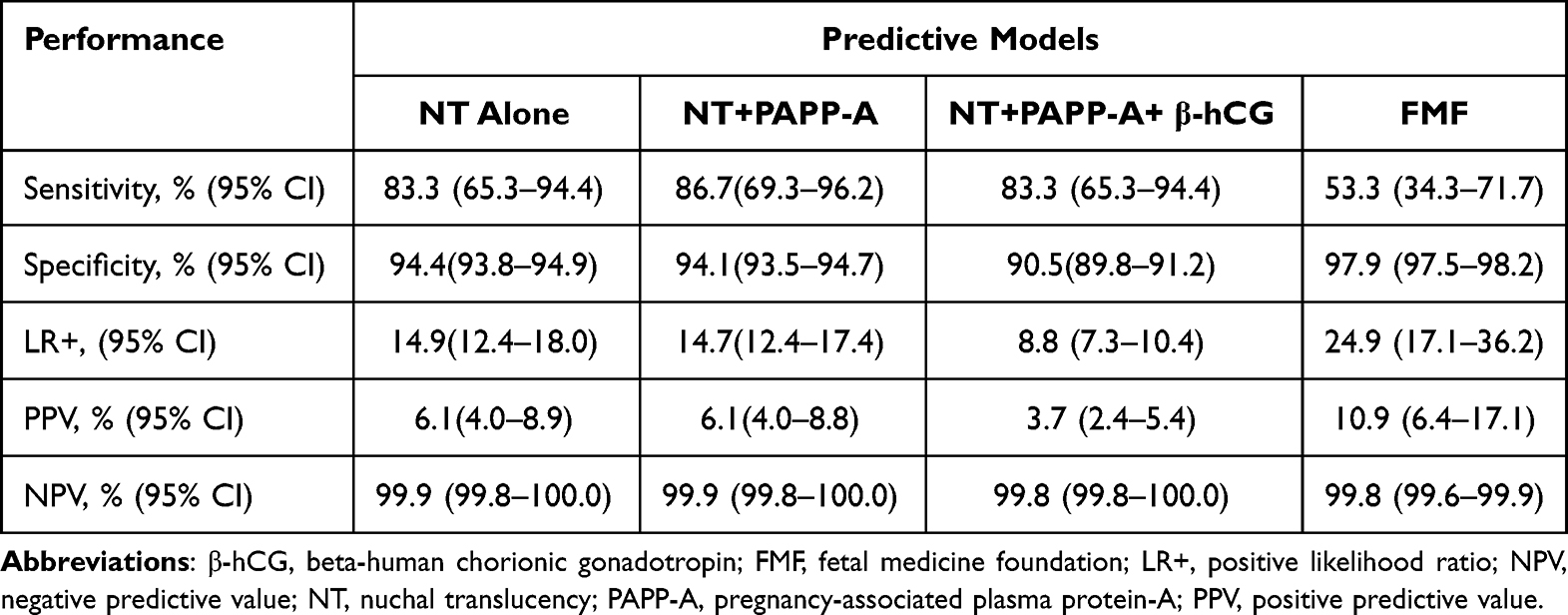 |
Table 4 Diagnostic Performance of First Trimester Screening Models for Monosomy X Using a Risk Cut-off of 1:250 |
 |
Figure 3 Calibration plot of the predictive model for monosomy X detection using nuchal translucency (NT) and pregnancy associated plasma protein A (PAPP-A). |
Discussion
The key insights from this study are: 1) The trisomy 21 risk calculated by the FMF algorithm can also predict monosomy X with high specificity but low sensitivity. 2) A newly developed model incorporating NT and PAPP-A significantly improves detection, increasing sensitivity from 53.3% to 86.7%. 3) NT alone has strong predictive value, with PAPP-A further enhancing performance, while β-hCG adds no value—consistent with previous reports of its limitation in predicting fetal monosomy X.7,17 These findings suggest that, beyond estimating trisomy 21, 18, and 13 risks, the FMF algorithm could provide greater value by directly reporting monosomy X risk rather than inferring it from trisomy 21 risk estimates.
NT alone also showed strong performance, with high sensitivity, specificity, and NPV, supporting its utility as a standalone marker in resource-limited settings. Previous studies consistently report increased NT thickness in monosomy X, even without structural anomalies or hydrops.2,5,11 NT measurement is widely available and routinely recommended during first trimester scans,18 offering practical use without requiring laboratory or blood testing. However, its accuracy is highly operator-dependent and susceptible to technical variability, especially in settings with limited ultrasound expertise.19 Even with semi-automated tools in modern ultrasound systems, NT assessment remains operator-dependent—particularly among less experienced practitioners—underscoring the importance of standardized training and adherence to measurement protocols.20 Although NT enlargement is a common feature in monosomy X, it is not unique to the condition and may also be seen in other chromosomal or structural anomalies, thereby limiting its diagnostic specificity.21,22 Nonetheless, when performed in experienced hands and controlled settings, NT remains a valuable screening tool and a key component of first trimester assessment for sex chromosome abnormalities.
The inclusion of PAPP-A significantly improved the detection of monosomy X, highlighting its value as a biochemical marker. In this study, PAPP-A showed a strong inverse association with monosomy X risk, consistent with previous reports of reduced maternal serum PAPP-A levels in affected pregnancies (mean 0.49 MoM).6 This reduction may reflect impaired placental development and altered trophoblastic protein production. However, population and gestational age-related variability may limit its specificity when used alone. Thus, PAPP-A is better suited as a supportive marker that enhances sensitivity when combined with NT, rather than as a standalone tool. While the use of first trimester biochemical markers has declined in some settings due to the growing adoption of NIPT,23,24 such testing remains clinically relevant—particularly when integrated with combined screening protocols for conditions like preeclampsia.25
The FMF algorithm has been extensively validated and widely adopted for first trimester screening of common trisomies, particularly trisomy 21.26,27 A key advantage is its ability to function without biochemical markers, relying solely on maternal characteristics and ultrasound parameters such as NT, CRL, and FHR. This makes it suitable for resource-limited settings or where serum screening is unavailable. The algorithm is also freely accessible online, allowing standardized risk assessment across clinical sites. A recent study in a Southeast Asian population showed that the non-biochemical FMF model provided high accuracy for trisomy 21 screening in the first trimester, supporting its practical use across diverse settings.14 However, in this study, although the FMF algorithm showed the highest specificity and positive predictive value for monosomy X, its sensitivity was markedly lower, resulting in a higher false-negative rate. This likely reflects its original design for autosomal trisomies, where the distribution of screening markers differs from that of sex chromosome aneuploidies. This study strongly suggests that modifying the FMF algorithm to directly calculate the specific risk of monosomy X could enhance its overall utility.
Despite advances in prenatal screening, routine screening for sex chromosome aneuploidies, including monosomy X, is not universally recommended. ACOG and ISPD advise selective offering with appropriate counseling due to limitations in test accuracy and interpretation challenges.23,24 Nonetheless, early identification of monosomy X provides important clinical benefits, including timely counseling, diagnostic confirmation, and informed decision-making.3 In severe cases such as fetal hydrops or cystic hygroma, early diagnosis supports prognosis and pregnancy management, while in continuing pregnancies, it enables delivery planning, referral to specialized care, and psychosocial support.4 These benefits underscore the importance of improving access to reliable screening tools, particularly in low-resource settings where NIPT may be unavailable. Although NIPT provides high sensitivity for common aneuploidies, its positive predictive value for monosomy X remains relatively low due to biological factors such as confined placental mosaicism and maternal X-chromosome mosaicism. Therefore, NT-based screening continues to serve as a practical and complementary approach, offering cost-effective and accessible risk assessment that can be integrated into routine prenatal care across diverse clinical settings.
The strengths of this study are as follows: It represents the cohorts to evaluate monosomy X screening using both the FMF algorithm and population-specific predictive models. The retrospective review of a prospective database and blinded risk assessment strengthen the methodological rigor. However, limitations include the relatively low number of monosomy X cases, which may compromise the positive and negative predictive values despite excellent sensitivity and specificity. Additionally, the single-center design may limit generalizability. External validation through multicenter, prospective studies or in other ethnic populations should be encouraged.
Conclusions
NT-based screening models, particularly when combined with PAPP-A, possibly demonstrate superior performance in detecting monosomy X compared with the FMF algorithm, although this finding is based on a limited sample size and requires external validation. These models offer a practical, accessible, and cost-effective option for early risk assessment, especially in settings with limited access to NIPT or biochemical testing. Although the FMF algorithm provided high specificity, its lower sensitivity limits its utility for monosomy X screening. The findings underscore the importance of condition-specific models and support the integration of simplified approaches into routine prenatal care to improve early detection of sex chromosome aneuploidies. We should take advantage of first trimester screening for fetal trisomies by also calculating and reporting the risk of monosomy X. This can be accomplished within the same routine testing without additional cost or effort while significantly enhancing the utility of first trimester screening by expanding its scope from trisomies to include monosomy X. Further multicenter studies with larger sample sizes are warranted to validate and generalize these findings across diverse populations. Integration of this simplified screening approach into existing prenatal care programs could enhance early detection and accessibility in resource-limited settings.
Acknowledgments
The authors would like to thank the staff of the Maternal–Fetal Medicine Unit, Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University, for their support in data retrieval and clinical input.
Funding
This study was supported by Chiang Mai University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Martin-Giacalone BA, Lin AE, Rasmussen SA, et al. Prevalence and descriptive epidemiology of turner syndrome in the United States, 2000-2017: a report from the national birth defects prevention network. Am J Med Genet A. 2023;191(5):1339–1349. doi:10.1002/ajmg.a.63181
2. Papp C, Beke A, Mezei G, et al. Prenatal diagnosis of Turner syndrome: report on 69 cases. J Ultrasound Med. 2006;25(6):
3. Dorf ILH, Lou S, Skakkebæk A. Parental decision-making following a prenatal diagnosis of turner syndrome: a systematic review. Am J Med Genet C Semin Med Genet. 2025;e32140.
4. Gravholt CH, Andersen NH, Christin-Maitre S, et al. Clinical practice guidelines for the care of girls and women with Turner syndrome. Eur J Endocrinol. 2024;190(6):G53–g151. doi:10.1093/ejendo/lvae050
5. Kagan KO, Avgidou K, Molina FS, et al. Relation between increased fetal nuchal translucency thickness and chromosomal defects. Obstet Gynecol. 2006;107(1):6–10. doi:10.1097/01.AOG.0000191301.63871.c6
6. Spencer K, Tul N, Nicolaides KH. Maternal serum free beta-hCG and PAPP-A in fetal sex chromosome defects in the first trimester. Prenat Diagn. 2000;20(5):390–394. doi:10.1002/(SICI)1097-0223(200005)20:5<390::AID-PD824>3.0.CO;2-B
7. Viuff MH, Stochholm K, Uldbjerg N, et al. Only a minority of sex chromosome abnormalities are detected by a national prenatal screening program for down syndrome. Hum Reprod. 2015;30(10):2419–2426. doi:10.1093/humrep/dev192
8. Badeau M, Lindsay C, Blais J, et al. Genomics-based non-invasive prenatal testing for detection of fetal chromosomal aneuploidy in pregnant women. Cochrane Database Syst Rev. 2017;11(11):Cd011767. doi:10.1002/14651858.CD011767.pub2
9. Shear MA, Swanson K, Garg R, et al. A systematic review and meta-analysis of cell-free DNA testing for detection of fetal sex chromosome aneuploidy. Prenat Diagn. 2023;43(2):133–143. doi:10.1002/pd.6298
10. Dowlut-McElroy T, Davis S, Howell S, et al. Cell-free DNA screening positive for monosomy X: clinical evaluation and management of suspected maternal or fetal turner syndrome. Am J Obstet Gynecol. 2022;227(6):862–870. doi:10.1016/j.ajog.2022.07.004
11. Sebire NJ, Snijders RJ, Brown R, et al. Detection of sex chromosome abnormalities by nuchal translucency screening at 10-14 weeks. Prenat Diagn. 1998;18(6):581–584. doi:10.1002/(SICI)1097-0223(199806)18:6<581::AID-PD301>3.0.CO;2-6
12. The Fetal Medicine Foundation. Risk for trisomies at 11-13 weeks.Available from: https://www.fetalmedicine.org/research/assess/trisomies.
13. Lüthgens K. Comparison of the new PRC software with the established algorithm of the FMF UK for the detection of trisomy 21 and 18/13. Fetal Diagn Ther. 2008;24(4):376–384. doi:10.1159/000165116
14. Kunanukulwatana C, Tongprasert F, Luewan S, et al. Effectiveness of fetal medicine foundation’s non-biochemical risk calculation algorithm in detection of common trisomies screening at 11-13 weeks of gestation: 12 years’ experience in Northern Thailand. Int J Womens Health. 2025;17:1693–1699. doi:10.2147/IJWH.S526271
15. Tongprasert F, Kunanukulwatana C, Luewan S, et al. Prenatal screening for trisomy 21 in the first trimester: a comparison of a Thai non-biochemical predictive model and the fetal medicine foundation algorithm. Int J Gynaecol Obstet. 2025. doi:10.1002/ijgo.70305
16. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–845. doi:10.2307/2531595
17. Spencer K, Heath V, Flack N, et al. First trimester maternal serum AFP and total hCG in aneuploidies other than trisomy 21. Prenat Diagn. 2000;20(8):635–639. doi:10.1002/1097-0223(200008)20:8<635::AID-PD868>3.0.CO;2-U
18. Bilardo CM, Chaoui R, Hyett JA, et al. ISUOG Practice Guidelines (updated): performance of 11-14-week ultrasound scan. Ultrasound Obstet Gynecol. 2023;61(1):127–143. doi:10.1002/uog.26106
19. Borrell A. Promises and pitfalls of first trimester sonographic markers in the detection of fetal aneuploidy. Prenat Diagn. 2009;29(1):62–68. doi:10.1002/pd.2182
20. Kagan KO, Abele H, Yazdi B, et al. Intraoperator and interoperator repeatability of manual and semi-automated measurement of increased fetal nuchal translucency according to the operator’s experience. Prenat Diagn. 2011;31(13):1229–1233. doi:10.1002/pd.2868
21. Bilardo CM, Müller MA, Pajkrt E, et al. Increased nuchal translucency thickness and normal karyotype: time for parental reassurance. Ultrasound Obstet Gynecol. 2007;30(1):11–18. doi:10.1002/uog.4044
22. Grande M, Jansen FA, Blumenfeld YJ, et al. Genomic microarray in fetuses with increased nuchal translucency and normal karyotype: a systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2015;46(6):650–658. doi:10.1002/uog.14880
23. American College of Obstetricians and Gynecologists, Society for Maternal-Fetal Medicine. Screening for fetal chromosomal abnormalities: ACOG practice bulletin, number 226. Obstet Gynecol. 2020;136(4):e48–e69. doi:10.1097/AOG.0000000000004084
24. Benn P, Borell A, Chiu R, et al. Position statement from the aneuploidy screening committee on behalf of the board of the international society for prenatal diagnosis. Prenat Diagn. 2013;33(7):622–629. doi:10.1002/pd.4139
25. Poon LC, Shennan A, Hyett JA, et al. The international federation of gynecology and obstetrics (FIGO) initiative on pre-eclampsia: a pragmatic guide for first-trimester screening and prevention. Int J Gynaecol Obstet. 2019;145 Suppl 1(S1):1–33. doi:10.1002/ijgo.12802
26. Chasen ST, Sharma G, Kalish RB, et al. First-trimester screening for aneuploidy with fetal nuchal translucency in a United States population. Ultrasound Obstet Gynecol. 2003;22(2):149–151. doi:10.1002/uog.174
27. Snijders RJ, Noble P, Sebire N, et al. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10-14 weeks of gestation. Fetal Med Foundation First Trimester Screening Group Lancet. 1998;352:343–346.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Fetal Medicine Foundation’s Non-Biochemical Risk Calculation Algorithm in Detection of Common Trisomies Screening at 11–13 weeks of Gestation: 12 Years’ Experience in Northern Thailand
Kunanukulwatana C, Tongprasert F, Luewan S, Tongsong T
International Journal of Women's Health 2025, 17:1693-1699
Published Date: 5 June 2025