Back to Journals » International Medical Case Reports Journal » Volume 19
Prenatal Detection of Proximal Femoral Focal Deficiency (PFFD) in Limited Resource Setting: A Case Report
Authors Arioseno YA, Pramatirta AY, Caropeboka MFA, Sanjaya MEJ, Adibrata AA ![]()
Received 27 September 2025
Accepted for publication 19 February 2026
Published 5 March 2026 Volume 2026:19 570672
DOI https://doi.org/10.2147/IMCRJ.S570672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Yossi Agung Arioseno,1 Akhmad Yogi Pramatirta,2 Muhamad Faizal Arif Caropeboka,1 Moch Erwin Jaya Sanjaya,1 Antony Abel Adibrata3
1Obstetrics and Gynecology Sub-Specialist Program, Faculty of Medicine, Padjadjaran University, Bandung, Indonesia; 2Department of Obstetrics and Gynecology, Faculty of Medicine/Dr. Hasan Sadikin General Hospital, Padjadjaran University, Bandung, Indonesia; 3Faculty of Medicine, Padjadjaran University, Bandung, Indonesia
Correspondence: Yossi Agung Arioseno, Email [email protected]
Abstract: Proximal femoral focal deficiency (PFFD) is a rare congenital skeletal malformation characterized by variable underdevelopment of the proximal femur. This report presents a 30-year-old, G4P3+0 woman with a pregnancy complicated by a fetus with left-sided PFFD with breech presentation and small-for-gestational-age features. Delivery was performed by elective cesarean section at 38 weeks showed a female neonate with confirmed unilateral PFFD affecting the left femur, classified as Aitken type D, with no associated congenital anomalies. The parents were referred for pediatric orthopedic, prosthetic, and rehabilitation counselling. This case highlights the importance of meticulous prenatal ultrasonography in detecting rare skeletal anomalies such as PFFD. Even in the absence of advanced imaging, 2D ultrasound can support timely diagnosis, parental counselling, and early multidisciplinary management to improve long-term functional outcomes.
Plain Language Summary: Proximal femoral focal deficiency (PFFD) is a very rare condition where the upper thigh bone does not fully develop, causing one leg to be shorter than the other. This may affect a child’s mobility and quality of life as they grow. In this case, PFFD was detected during pregnancy through routine ultrasound at 32 weeks. After birth, the diagnosis was confirmed by X-ray, which showed the left thigh bone was much shorter than the right. No other abnormalities were found. Finding PFFD before birth is important because it gives parents time to receive counselling and allows doctors to plan treatment after delivery. While advanced imaging can improve detection, this case shows that careful use of standard ultrasound can still identify the condition. Early diagnosis helps families access orthopedic, prosthetic, and rehabilitation services that can improve long-term mobility and daily function for affected children.
Keywords: fetal detail scan, case report, intrauterine diagnosis, prenatal ultrasound, proximal femoral focal deficiency, skeletal dysplasia
Introduction
Proximal femoral focal deficiency (PFFD), is a proximal-predominant subset of congenital femoral deficiency (CFD).1 PFFD is a rare congenital malformation of the lower limb, primarily affecting the hip and femur, and typically resulting in significant limb shortening, while CFD ranging from a mildly short but otherwise “normal-form” femur to very severe absence/malformation.1,2 Prenatal diagnosis of PFFD first reported in 1989 by ultrasonography examination, and exceptionally rare, presenting only 1 to 2 per 100,000 live births.3,4 PFFD is characterized by varying degrees of underdevelopment of the proximal femur, with a clinical spectrum ranging from mild femoral shortening to complete absence of the proximal femur and acetabulum.3 The etiology remains largely unknown, with most cases occurring sporadically and without identifiable genetic or environmental causes.1
Despite its rarity, PFFD can be incidentally detected during routine antenatal ultrasonography.5 Prenatal diagnosis of PFFD is important, because early recognition of this malformation before birth could provide useful information to parents and physicians regarding management and therapeutic planning to help the mother preparing the issues.6 This action highlighting the importance of prenatal evaluation in parental counselling and initiation of a management plan.7 This case reports a unilateral short femur identified at 32 weeks’ gestation via standard prenatal imaging, with subsequent confirmation of PFFD. Our findings highlight the importance of obstetric ultrasonography in the early detection of this condition, emphasizing the value of meticulous prenatal screening in identifying congenital skeletal abnormalities.
Case Presentation
A 30-year-old G4P3+0 (3 alive) woman was referred from local hospital to our hospital as tertiary hospital, due to skeletal dysplasia and breech presentation shown by routine two-dimension ultrasonography examination during second trimester antenatal care by local obstetrician. At the admission, she did not have any complaint. She estimated her gestational age (GA) at 32 weeks by last menstrual period. No history of congenital abnormalities in the family was reported. History of environmental exposure to industrial hazard, radiation, infections or drugs was denied by the patient. No history of chronic illnesses or assisted reproduction history was reported. Previous pregnancy showed there are no abnormalities, all of them were born spontaneously, led by local midwives, and all of her children are alive.
On examination, no significant abnormality was found, however, her anthropometry showed her body mass index was on underweight status (16.4 Kg/m2). High-resolution two-dimension fetomaternal ultrasound was performed, showed: a single live female fetus, intrauterine, breech position, corresponding to 32 weeks 2 days of gestation; (Transcranial doppler (TCD) equivalent to 32 weeks 3 days GA); estimated fetal weight was 1612 grams (4.7th percentile); Facial, thoracic, and abdominal features showed normal result; Side by side extremities ultrasonography (Figure 1) showed an abnormality as femur length discrepancy between right and left femur, with the femur length ratio was 0.5. The ultrasound impression was 32 weeks 4 days of pregnancy with Left Proximal Femoral Focal Deficiency (PFFD), small for Gestational Age and Breech position. Given the breech presentation, diagnosis of PFFD, and fetal growth restriction, an elective cesarean section was scheduled at 38 weeks’ gestation. Pomeroy sterilization was performed at the patient’s request following appropriate counseling and allowed by her husband because they already have 3 children.
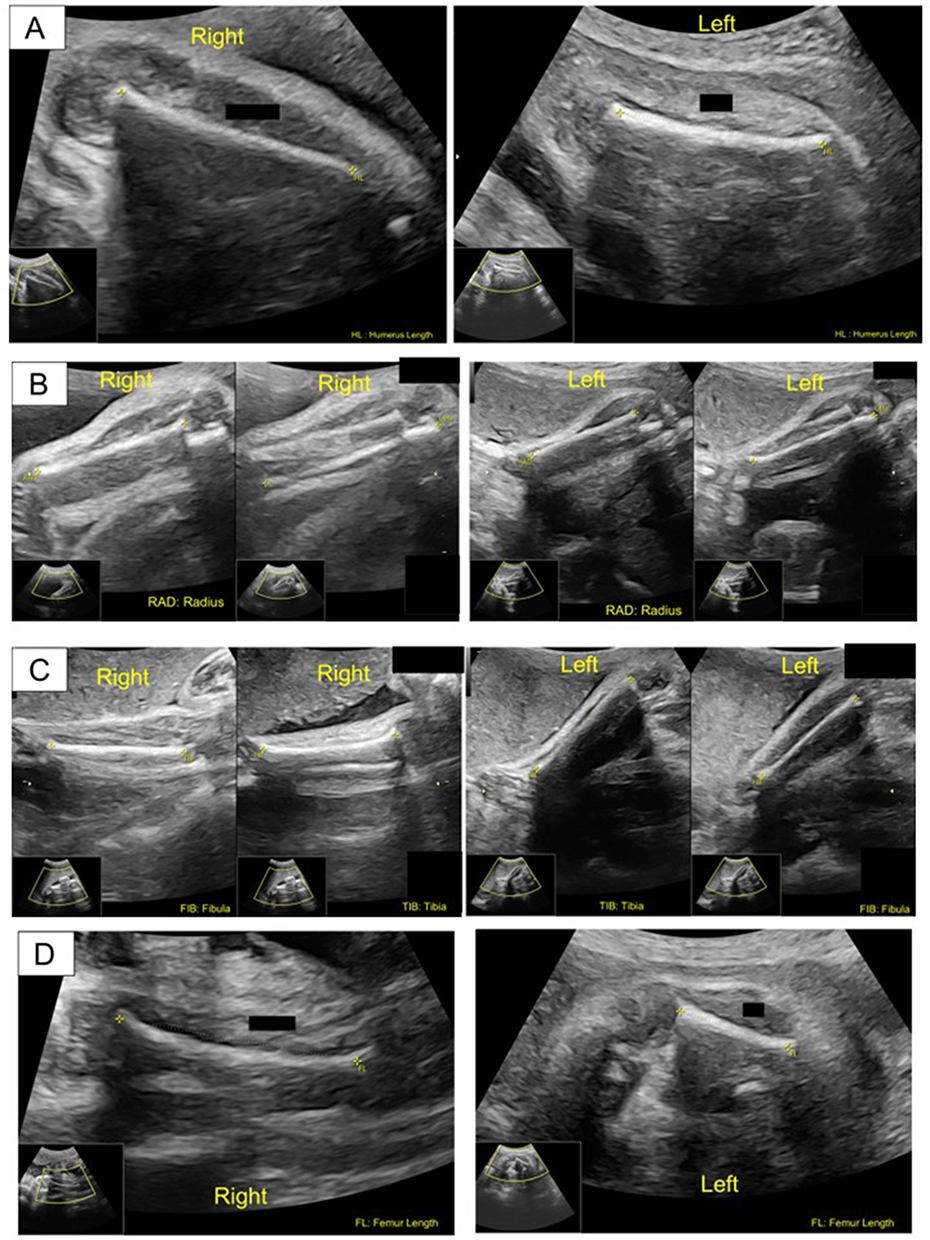 |
Figure 1 Fetomaternal Ultrasound of fetal extremities. (A) Humerus length. Right humerus length: 4.78 cm (percentile < 1) ≈28 weeks 0 days. Left humerus length: 4.93 cm (<1 percentile) ≈29 weeks 0 days. (B) Radius-Ulna length. Right radius: 4.28 cm (percentile 31.3rd), ≈29 weeks 6 days. Right ulna 5.04 (percentile 21.0) ≈31 weeks 6 days. Left radius: 4.29 cm (percentile 31.9) ≈29 weeks 6 days. Left ulna: 4.97 cm (percentile 14.3) ≈31 weeks 3 days. (C) Tibia-Fibula length. Right tibia: 5.09 cm (percentile 8.6) ≈30 weeks 3 days. Right fibula 5.08 cm (percentile 33.2) ≈30 weeks 6 days. Left tibia: 5.16 cm (Percentile 13.5) ≈30 weeks 5 days. Left fibula: 4.84 cm (Percentile 18.9) ≈29 weeks 5 days. Left fibula 4.84 cm (Percentile 18.9) ≈29 weeks 5 days. (D) Femur length. Right femur length: 5.37 cm (percentile < 1) ≈28 weeks 3 days. Left femur length: 2.70 cm (percentile < 1) ≈18 weeks 2 days. |
During the procedure, the patient’s vital sign was normal and female baby was born. During neonatal resuscitation, it is concluded that her birth weight was 2325 grams, birth length was 41 Cm, APGAR score at 1st and 5th minute were 9 and 10, New Ballard score was consistent with gestational age of 38 to 40 weeks, and placental weight was 400 grams. No abnormality was observed from bony or facial features; however, abnormality was shown in her lower extremities. Her lower extremities showed there was leg length ratio abnormality (Figure 2), consistent with feto-maternal ultrasound 6 weeks prior, with the left leg was shorter than right leg (Figure 2A). PFFD was later confirmed through plain femur radiograph that showed significantly shortened left femoral bone (Figure 2B and C), with normal right femoral bone (Figure 2B and D). Computerized Tomography (CT) scan or Magnetic Resonance Imaging (MRI) has not been performed at the time this case report was written due to long waiting lists. Later, the parents were advised to counsel with pediatric orthopedic surgeons, prosthetists, and physical therapists to support both mobility and quality of life of the neonate.
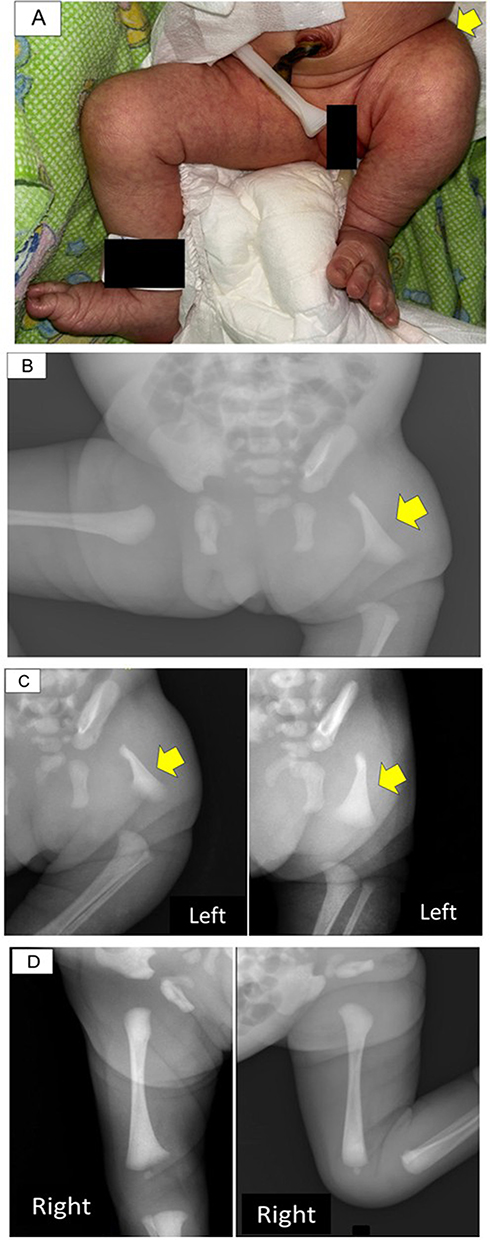 |
Figure 2 Postnatal examination. (A) Clinical examination, yellow arrow showed shortened of left lower limb compared to right lower limb. (B) Antero-posterior pelvic and thighs X-ray, yellow arrow showed short left femur with absence of femoral head with severe dysplastic and severely shortened femur. (C) Left femur x-ray, abduction and flexion position, yellow arrow showed an abnormal left lower limb with absence of femoral head and shortened femur. (D) Right femur x-ray, abduction and flexion position, a normal right lower limb. |
Discussion
Proximal femoral focal deficiency (PFFD) is an extremely rare congenital anomaly with only a limited number of cases reported in the literature.5,8–10 It was characterized by abnormal development of the subtrochanteric portion of the femur, resulting in shortening of the affected limb. Its estimated prevalence is approximately 1 to 2 per 100,000 live births.3,4 The exact etiology remains unknown, with most cases occurring sporadically and lacking identifiable genetic or environmental risk factors. Therefore, other common causes of short femur—such as aneuploidy (particularly trisomy 21), poorly controlled maternal diabetes, teratogenic drug exposure (eg, thalidomide), intrauterine infections, radiation exposure, or focal ischemia between the 4th and 8th week of gestation—should be excluded.1,10 In our case, none of those factors was identified; the only incidental finding on maternal condition was her underweight status.
Despite its rarity, PFFD might be incidentally detected during routine antenatal ultrasonography.5 However, accurate prenatal identification of PFFD remains challenging due to its rarity and the broad phenotypic spectrum.11 Diagnostic complexity is further compounded by subtle early sonographic findings, limited ultrasound resolution for detailed skeletal assessment, and potential misinterpretation due to fetal positioning and acoustic shadowing—especially among less experienced sonographers. Nevertheless, early prenatal identification is critical, as it allows timely parental counselling and planning for postnatal management.6,8 In our case, the diagnosis was made prenatally, at second trimester of gestation during routine ultrasonography antenatal care, so the patient could be referred for counselling and future management for the mother and foetus as soon as possible. This action was in accordance with Radler’s survey that stated 63% of mothers who gave birth to babies with PFFD would have preferred to learn the diagnosis before birth rather than after birth, highlighting the importance of prenatal evaluation in parental counselling and initiation of a management plan.7
PFFD can present as part of a broader congenital syndrome, such as femoral-fibula-ulna syndrome, and femoral-facial syndrome. In some cases, diagnosis is only made postnatally due to the subtlety of prenatal findings.10 However, in our case, no associated congenital anomalies were detected. This was confirmed through detailed prenatal ultrasonography of the fetal extremities and face, as well as postnatal clinical examination and femoral radiography.
Recent reports suggest that advanced imaging modalities such as 3D and 4D ultrasound, particularly with surface rendering, can enhance evaluation of fetal bony structures and limb motion, supporting more accurate diagnosis and treatment planning.12,13 Advances in ultrasound technology also could led to earlier diagnosis of PFFD in first trimester, Kudla et al report a case of PFFD diagnosed at 12 weeks of gestation using 3D and 4D ultrasound techniques, although typical detection occurs between 18 and 24 weeks of gestation.13,14 In our case, PFFD was detected in the patient through 2D ultrasound at 32 weeks gestation age. It should be noted that in author’s setting, 2D ultrasonography was the primary diagnostic modality utilized due to not all healthcare facilities are equipped with 3D or 4D ultrasound machines. Therefore, 2D ultrasound remains a valuable diagnostic tool when performed with appropriate technique especially in limited resource setting.
PFFD may present as either bilateral or unilateral limb deficiency, and the severity of PFFD is categorized based on the degree of lower extremity involvement.15 The unilateral form is more prominent, occurred in 85–90% of all cases.4 If unilateral was occurred, the right femur is the most frequent finding; however, in this case, the PFFD was found in left femur.16 The ratio of femoral length discrepancy in isolated cases is usually between 0.75 and 0.85.10 In our case, however, the femoral length discrepancy ratio was 0.5, marked discrepancy suggests severe hypoplasia thus needs early counseling about substantial projections. Several classifications have been introduced, but the most applied classification is Aitken’s classification which divides PFFD into four categories based on the radiographic appearance ranking from a benign form (A) to a severe form (D) according to the extent of femoral deficiency (Figure 3).17 On our case, the condition is unilateral, isolated, belongs to type D based on Figure 3. Previous report also said PFFD is more common in female than male (2:1), in line with this study that the condition was found in female fetus.16
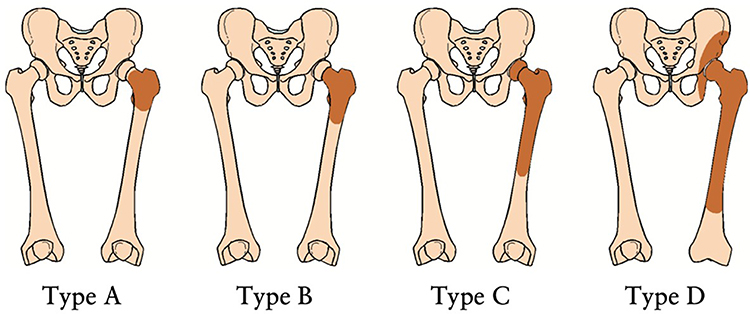 |
Figure 3 The Aitken classification of PFFD. Type A– presence of femoral head with varus deformity; Type B– presence of femoral head but with delayed ossification; varus, mild acetabular dysplasia, and pseudarthrosis may occur; Type C– absence of femoral head as well as acetabular dysplasia and shortening of femur; and Type D– absence of femoral head with severe dysplastic and severely shortened femur. |
The postnatal evaluation is essential for confirming PFFD and establishing a comprehensive care plan that supports the patient through growth and development, especially as they grow and mature. As in our case, femur x-ray was performed to classify the PFFD and an MRI was subsequently recommended for further anatomical assessment, highlighted the value of both MRI and prenatal ultrasonography in characterizing PFFD. However, MRI may not always be feasible due to limitations such as availability, cost, acquisition challenges, or patient factors, such as in the case presented whereas due to limited resources the MRI queue for patients can be very long.18 CT scans can also be utilized, particularly when the acetabulum and proximal femur have begun to ossify, typically at an older age. Nevertheless, radiation exposure must be taken into consideration when selecting this modality.8
A range of treatment options exists for PFFD, and the chosen approach depends on several factors, including the severity of femoral deficiency, involvement of other limbs, stability of the hip and knee joints, presence of soft tissue contractures, and the family’s goals regarding function, appearance, and long-term quality of life. Treatment outcomes can vary significantly depending on the intervention strategy. In Aitken type D PFFD, the proximal femur and hip are severely dysplastic or absent, so prognosis depends primarily on functional adaptation rather than anatomic restoration.19 Without coordinated care, children often develop progressive limb-length discrepancy, inefficient gait, pelvic imbalance, and secondary spine/contralateral limb strain. Long-term outcomes are generally improved by early multidisciplinary management, consist of pediatric orthopedics, prosthetics, rehabilitation, and psychosocial support, with rehabilitation focused on early mobility, core and hip strengthening, contracture prevention, and gait training.8 Prosthetic planning is individualized and adjusted through growth, and surgical options may be considered to optimize prosthetic use and alignment.19 The overall goal is independent ambulation, endurance, and quality of life despite severe structural deficiency.8
Conclusion
Proximal femoral focal deficiency (PFFD) is a rare congenital anomaly that can be detected through careful prenatal ultrasonography. Early diagnosis enables timely counseling and postnatal planning. While advanced imaging may improve accuracy, high-quality and careful 2D ultrasound remains effective and reliable especially in resource-limited settings. A multidisciplinary approach is essential to optimize outcomes for affected neonates and parental counseling due to a long therapeutic journey.
Patient’s Perspective
After learning and careful explanation from obstetricians about the leg abnormalities in her fetus, she accepted its condition and the possible approach for the fetus in the future. She believed alongside with her husband, they could handle the situation and choose to continue to follow-up the neonate conditions at current hospital. She was grateful due to all of her pregnancy and future bills of her neonate’s medical expenses could be covered by Indonesia’s Universal Health Care System (BPJS), although other expenses such as transportations were not covered and she have to use her pocket money.
Ethical Approval and Informed Consent Patient Statement
This study adhered to the principles of the Declaration of Helsinki and institutional guidelines for case reports. Written informed consent was obtained from the patient including permission to publish the case details and any clinical images. All identifying information has been removed to ensure patient confidentiality.
Acknowledgments
The authors thank the Obstetrics and Gynecology Department staff at Hasan Sadikin General Hospital for their support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Agrawal U, Taqi M, Tiwari V. Congenital femoral deficiency. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
2. Nossov SB, Hollin IL, Phillips J, Franklin CC. Proximal femoral focal deficiency/congenital femoral deficiency: evaluation and management. J Am Acad Orthop Surg. 2022;30(13):e899–7. doi:10.5435/JAAOS-D-21-01186
3. Shaw SC, Prasad M, Manrai K. Proximal femoral focal deficiency. Med J. 2023;79(3):360–361. doi:10.1016/j.mjafi.2020.11.006
4. Jeanty P, Kleinman G. Proximal femoral focal deficiency. J Ultrasound Med. 1989;8(11):639–642. doi:10.7863/jum.1989.8.11.639
5. Gerscovich EO, Sekhon S, Loehfelm TW, Greenspan A. Fetal ultrasound: early diagnosis and natural evolution of proximal femoral focal deficiency. J Ultrason. 2017;17(71):294–298. doi:10.15557/JoU.2017.0043
6. D’Ambrosio V, Pasquali G, Squarcella A, et al. Prenatal diagnosis of proximal focal femoral deficiency: literature review of prenatal sonographic findings. J Clin Ultrasound. 2016;44(4):252–259. doi:10.1002/jcu.22306
7. Radler C, Myers AK, Hunter RJ, Arrabal PP, Herzenberg JE. Prenatal diagnosis of congenital femoral deficiency and fibular hemimelia. Prenat Diagn. 2014;34(10):940–945. doi:10.1002/pd.4396
8. Uduma FU, Dim EM, Njeze NR. Proximal femoral focal deficiency – a rare congenital entity: two case reports and a review of the literature. J Med Case Rep. 2020;14(1):27. doi:10.1186/s13256-020-2350-y
9. Thomas MM, Tosson AMS, Taher MB. Unilateral isolated proximal femoral focal deficiency in an egyptian infant and review of literature. J Child Sci. 2020;10(01):e126–33. doi:10.1055/s-0040-1716918
10. Lin TH, Chung CH, Shih JC, Lin CH, Lee CN, Su YN. Prenatal diagnosis of proximal femoral focal deficiency: a case report and literature review. Taiwan J Obstet Gynecol. 2013;52(2):267–269. doi:10.1016/j.tjog.2013.04.020
11. Fahim R, Thomas Z, DiDomenico LA. Pediatric forefoot pathology. Clin Pod Med Surg. 2013;30(4):479–490. doi:10.1016/j.cpm.2013.07.007
12. Mailath‐Pokorny M, Timor‐Tritsch IE, Monteagudo A, Mittal K, Konno F, Santos R. Prenatal diagnosis of unilateral proximal femoral focal deficiency at 19 weeks’ gestation: case report and review of the literature. Ultrasound Obstet Gynecol. 2011;38(5):594–597. doi:10.1002/uog.8995
13. Llanes AC, Venard E, Youn S, Van Tassel D, Goncalves LF, Belthur MV. The significance and limitations of pre- and postnatal imaging in the diagnosis and management of proximal focal femoral deficiency. Diagnostics. 2025;15:1302. doi:10.3390/diagnostics15111302
14. Kudla MJ, Beczkowska-Kielek A, Kutta K, Partyka-Lasota J. Proximal femoral focal deficiency of the fetus - early 3D/4D prenatal ultrasound diagnosis. Med Ultrason. 2016;18(3):397–399. doi:10.11152/mu.2013.2066.183.kud
15. Bedoya MA, Chauvin NA, Jaramillo D, Davidson R, Horn BD, Ho-Fung V. Common patterns of congenital lower extremity shortening: diagnosis, classification, and follow-up. RadioGraphics. 2015;35(4):1191–1207. doi:10.1148/rg.2015140196
16. Ifesanya AO, Omololu BA. Case report: proximal focal femoral deficiency in Ibadan a developing Country’s perspective and a review of the literature. Niger J Paediatr. 2012;39(2):75–78. doi:10.4314/njp.v39i2.8
17. Fairbank TJ. Proximal femoral focal deficiency–a congenital anomaly. J Bone Jt Surg Br. 1971;53(4):776. doi:10.1302/0301-620X.53B4.776-a
18. Dautt‐Leyva JG, Canizalez‐Román A, Acosta Alfaro LF, Gonzalez‐Ibarra F, Murillo‐Llanes J. Maternal and perinatal complications in pregnant women with urinary tract infection caused by Escherichia coli. J Obstet Gynaecol Res. 2018;44(8):1384–1390. doi:10.1111/jog.13687
19. Ahmed KA, Das R, Sarma K, Das BK, Saikia D. Prosthesis for unilateral isolated proximal focal femoral deficiency: a case report and review of the literature. Cureus. 2024;16(6):e63210. doi:10.7759/cureus.63210
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.