Back to Journals » Drug Design, Development and Therapy » Volume 20
Preliminary Effects of Hydrogen-Oxygen Inhalation on Nodule Size, IL-6, and Neutrophils in Patients with Small Pulmonary Nodules
Authors Wei X, Zhang W, Li Y, Sha X, Yi H, Cui C ![]()
Received 25 February 2026
Accepted for publication 19 June 2026
Published 8 July 2026 Volume 2026:20 605134
DOI https://doi.org/10.2147/DDDT.S605134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Xiaohui Wei,1,* Wei Zhang,1,* Yuanyuan Li,1 Xiaojuan Sha,2 Hongpeng Yi,3 Chao Cui4
1Geriatrics Department, Dongying People’s Hospital (Dongying Hospital of Shandong Provincial Hospital Group), Dongying, Shandong, People’s Republic of China; 2Medical Records Department, Dongying People’s Hospital (Dongying Hospital of Shandong Provincial Hospital Group), Dongying, Shandong, People’s Republic of China; 3Department of TCM, Dongying Maternal and Child Health Hospital, Dongying, Shandong, People’s Republic of China; 4Scientific Research Department, Qilu Hospital of Shandong University Dezhou Hospital, Dezhou, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Cui, Scientific Research Department, Qilu Hospital of Shandong University Dezhou Hospital, Dezhou, Shandong, People’s Republic of China, Email [email protected]
Objective: To evaluate the effects of hydrogen-oxygen inhalation on nodule diameter and peripheral blood inflammatory factors in patients with small pulmonary nodules (SPNs), and to further analyze its efficacy in the smoking subgroup. The primary endpoint was the change in pulmonary nodule diameter before and after intervention; secondary endpoints included alterations in serum IL-6, CRP, peripheral blood neutrophil count, and Mayo malignant transformation risk score.
Methods: A total of 59 patients with SPNs confirmed by chest CT were enrolled and randomly divided into the observation group (hydrogen-oxygen inhalation, n=30) and control group (air inhalation, n=29). The intervention lasted 14 consecutive days, and all indicators were re-examined at 3-month follow-up. This study was registered in the Chinese Clinical Trial Registry (ChiCTR) with the registration number ChiCTR2300076152 (registration date: September 26, 2023).
Results: Baseline demographic and clinical characteristics were well balanced between the two groups (all P> 0.05). After intervention, the observation group had a significant reduction in nodule diameter by 0.64 mm (95% CI: 0.20– 1.08, P< 0.01). Serum IL-6 decreased by 1.36 pg/mL (95% CI: 0.70– 2.02, P< 0.01), and peripheral blood neutrophil count decreased by 1.14× 109/L (95% CI: 0.51– 1.77, P< 0.01). No significant pre- and post-intervention differences were observed in CRP level and Mayo malignant transformation risk score in either group (all P> 0.05). In the smoking subgroup, IL-6 level and neutrophil count also decreased significantly after hydrogen-oxygen inhalation (both P< 0.01), while CRP remained relatively stable.
Conclusion: Within the limitations of this single-center, small-sample study with a 3-month follow-up, hydrogen-oxygen inhalation can reduce SPN diameter and downregulate peripheral blood IL-6 and neutrophil levels, exerting a targeted anti-inflammatory effect especially in smoking patients. It may serve as a safe non-invasive adjuvant intervention for SPNs, while further multicenter large-sample studies are needed to validate its general applicability.
Keywords: hydrogen-oxygen inhalation, small pulmonary nodules, inflammatory factors, smoking, mayo malignant transformation risk score
Introduction
Lung cancer is one of the malignant tumors with the highest incidence and mortality rates worldwide. The core reasons for its poor prognosis and low 5-year survival rate are insufficient early diagnosis rates, with most patients being diagnosed at advanced stages.1 Small pulmonary nodules (SPNs) represent the early imaging manifestation of lung cancer, and the differentiation of their benign and malignant nature is a key focus and difficulty in clinical diagnosis and treatment. Most SPNs lack specific imaging features, with tiny lesions and difficult localization, making definitive diagnosis via needle biopsy challenging. Meanwhile, surgical treatment is prone to overtreatment. Currently, clinical practice mainly adopts follow-up observation with computed tomography (CT); however, such follow-up is associated with problems including a high false-positive rate and waste of medical resources.2 Therefore, exploring safe and effective non-surgical interventions for SPNs to delay nodule progression and improve the local pulmonary microenvironment holds important clinical significance for reducing the risk of lung cancer development.
As a reductive inert gas, hydrogen offers the advantages of high safety, easy availability and low cost, with no obvious toxic and side effects and high patient acceptability.3 In recent years, studies have revealed that hydrogen can regulate oxidative stress and inflammatory responses in the body through biological effects such as selective antioxidation, anti-inflammation and anti-apoptosis, thereby exerting a protective role in various diseases including pulmonary disorders and tumors.4 The classical selective antioxidant mechanism of hydrogen was first proposed by Ohsawa et al, whose landmark study was highly cited and recognized, suggesting that hydrogen could selectively scavenge highly toxic hydroxyl radicals (·OH) in the body; initially, this study also mentioned the potential scavenging effect on peroxynitrite anions (ONOO−), but this conclusion has been controversial in subsequent studies. A subsequent mechanistic study by Penders et al clarified that peroxynitrous acid (ONOOH) does not react with hydrogen, and the antioxidant effect of hydrogen is mainly attributed to its selective reaction with hydroxyl radicals rather than peroxynitrite anions, which has revised the classical understanding of hydrogen’s antioxidant targets without disturbing the normal redox balance, which lays a theoretical foundation for its clinical application.5 Notably, a multicenter randomized controlled trial by Zheng et al (2021, Respiratory Research) further validated the clinical efficacy of hydrogen-oxygen mixed inhalation, demonstrating that this therapy was superior to conventional oxygen therapy in alleviating pulmonary inflammation and improving clinical symptoms in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD), with favorable safety and tolerance.6 In addition, a latest mechanistic study by Negishi et al revealed a new target of molecular hydrogen, confirming that the Rieske iron-sulfur protein is a primary target of hydrogen, which provides a novel perspective for interpreting the biological mechanism of hydrogen beyond the classical free radical scavenging theory.7 Existing studies have verified that hydrogen can alleviate pulmonary inflammatory injury and inhibit pathological tissue remodeling, but its specific regulatory effect on SPNs, especially in smoking populations, has not been fully elucidated, and relevant clinical intervention evidence is still insufficient.
Based on the above research background and existing theoretical basis, this study proposed a pre-specified primary research hypothesis: hydrogen-oxygen inhalation can reduce the diameter of SPNs and improve the pulmonary inflammatory microenvironment in patients. Correspondingly, the primary endpoint was defined as the change in pulmonary nodule diameter before and after intervention, and secondary endpoints were set as alterations in serum interleukin-6 (IL-6), C-reactive protein (CRP), peripheral blood neutrophil count, and Mayo malignant transformation risk score. Circulating IL-6, CRP, and peripheral blood neutrophils are classic systemic inflammatory markers that can indirectly reflect the degree of local pulmonary inflammatory response and the imbalance of the pulmonary microenvironment. In view of this, the present study systematically investigated the regulatory effects of hydrogen-oxygen inhalation on nodule size, malignant transformation risk and inflammatory factors in patients with SPNs via a randomized controlled trial. Among these factors, serum IL-6 is a key proinflammatory cytokine closely linked to chronic pulmonary inflammation; peripheral blood neutrophil count and CRP can sensitively mirror systemic inflammatory activation that correlates with local pulmonary inflammatory status and SPN progression. These three indicators together constitute the key metrics for evaluating the pulmonary inflammatory microenvironment.8–10 Additionally, this study focused on analyzing the specific efficacy of hydrogen-oxygen inhalation in smokers, aiming to provide novel insights and evidence-based evidence for the clinical intervention of SPNs.
Materials and Methods
General Information
A total of 59 patients with small pulmonary nodules confirmed by chest CT were randomly enrolled in the Department of Respiratory and Critical Care Medicine of our hospital between February 2024 and February 2025. There were 36 males and 23 females, with an age range of 60–75 years and a mean age of 64.77 ± 3.12 years. Patients were divided into an observation group (n = 30) and a control group (n = 29) using a random number table method. Allocation concealment was implemented by assigning random grouping numbers in sealed opaque envelopes, which were opened sequentially after eligible participants completed baseline enrollment. All experiments involving human participants were performed in strict accordance with the Declaration of Helsinki. This study was approved by the Institutional Review Board of Dongying People’s Hospital (approval number: DYYX-2023-197), and written informed consent was obtained from all included patients. This study was registered with the Chinese Clinical Trial Registry (ChiCTR) on September 26, 2025, with the registration number ChiCTR2300076152. The official registration URL is https://www.chictr.org.cn/showproj.aspx?proj=76152.
This study was designed as a single-blind trial rather than a double-blind trial. Due to the distinct sensory characteristics of hydrogen-oxygen mixed gas and ambient air, blinding of patients and clinical operators was not feasible. However, outcome assessors, laboratory testing personnel and statistical analysts remained blinded to group allocation throughout the study.
Inclusion criteria: ① Aged ≥60 years; ② Diagnosed with solitary SPNs (diameter ≤10 mm) in accordance with the 2017 Fleischner Society guidelines and the 2018 NCCN Lung Cancer Screening Guidelines, with clinical recommendation for CT follow-up;11,12 ③ Complete baseline clinical data, imaging data and laboratory test results; ④ Able to cooperate with the entire course of intervention and follow-up.
Exclusion criteria: ① High malignant potential indicated by imaging, laboratory tests or needle biopsy, with clinical recommendation for surgical resection or voluntary surgical treatment by patients; ② Nodule diameter >10 mm or part-solid nodules; ③ Complicated with severe systemic infection, obstructive pneumonia, atelectasis, hilar lymphadenopathy or pleural effusion; ④ Presence of diffuse/multiple pulmonary nodules or suspected metastatic cancer; ⑤ Complicated with severe dysfunction of vital organs such as the heart, liver and kidney, or mental diseases that prevent cooperation with the study.
Therapeutic Regimens
Both groups received routine health guidance for SPNs, including smoking cessation, avoidance of dust exposure, and regular respiratory function training. Notably, unified and consistent smoking cessation guidance was provided for all participants in both groups throughout the trial, and no obvious smoking reduction or complete smoking quitting behavior was observed in enrolled smokers during the whole intervention and follow-up period. The smoking status and smoking burden of all patients remained basically stable at baseline level, which eliminates the confounding bias derived from smoking reduction and ensures that the improvement of relevant indicators is not attributed to changes in smoking habits. The observation group was administered inhalation of hydrogen-oxygen mixed gas via a hydrogen-oxygen generator (Model: AMS-H-03, manufactured by Shanghai Asclepius Meditec Co., Ltd.) at a flow rate of 3000 mL/min, with the volume fractions of hydrogen and oxygen being 66.6% and 33.3%, respectively. The control group inhaled ambient air using the same device, with identical operating procedures, operation duration, airflow rate, equipment noise, and wearing mode as the intervention group, to ensure consistent device sensory profile and guarantee placebo fidelity in the control group. For both groups, the inhalation was performed for a total of 4 hours per day, divided into two 2-hour sessions in the morning and evening, with continuous intervention for 14 days. Relevant indicators were re-examined at 3 months after the completion of intervention.
The 3-month follow-up duration was selected based on rigorous clinical and mechanistic rationales: Firstly, in accordance with the 2017 Fleischner Society Guidelines and 2018 NCCN Lung Cancer Screening Guidelines for small pulmonary nodules (≤10 mm), the routine initial follow-up interval for low-to-moderate risk SPNs is 3 months, which is the internationally recognized standard time point to observe early morphological changes of small nodules and avoid excessive or insufficient follow-up. Secondly, preclinical and clinical studies of hydrogen/oxygen therapy have confirmed that the anti-inflammatory and antioxidant regulatory effects of hydrogen require a certain time window to manifest: short-term follow-up (≤1 month) is difficult to detect stable changes in pulmonary nodule morphology and inflammatory factors, while 3 months is sufficient to observe the preliminary regulatory effect of hydrogen-oxygen inhalation on the pulmonary inflammatory microenvironment and nodule size, without excessive follow-up time that may introduce confounding factors. Thirdly, considering the slow progression of benign small pulmonary nodules and the minimal short-term malignant transformation risk, a 3-month follow-up can effectively evaluate the intervention effect while ensuring patient compliance and reducing medical resource consumption, which is consistent with the design logic of similar clinical studies on non-surgical intervention for SPNs.
Outcome Measures and Detection Methods
Study Endpoints
All study endpoints were strictly pre-specified and registered in the ChiCTR before patient enrollment. This study had a clearly defined pre-specified primary endpoint: the change in pulmonary nodule diameter before and after hydrogen-oxygen inhalation intervention. Pre-specified secondary endpoints included: changes in serum IL-6, CRP levels and peripheral blood neutrophil count before and after intervention; changes in Mayo malignant transformation risk score of SPNs. The smoking subgroup analysis was defined as a pre-specified exploratory analysis rather than a formal secondary endpoint.
Collection of Baseline and Follow-Up Data
Baseline data of patients in both groups were collected, including age, gender, smoking history and tumor history. Smoking status was categorized as current smoker, former smoker, and never smoker. Smoking burden was quantified using pack-years (1 pack-year = 20 cigarettes smoked per day for 1 year). For subgroup analysis, smokers were defined as individuals with a smoking history of at least 10 cigarettes per day for no less than 1 year, and tumor history. Peripheral blood inflammatory factors were detected and chest CT scans were performed before treatment and at 3 months after treatment to evaluate the imaging features and malignant transformation risk of pulmonary nodules. The smoking subgroup consisted of 14 patients in the observation group and 16 patients in the control group, and the relatively small sample size of this subgroup may limit the statistical power for detecting between-group differences.
Detection of Imaging Indicators
Chest plain scan was performed using a 64-slice spiral CT scanner. Scan parameters: slice thickness 1.00 mm, reconstructed with iterative reconstruction algorithm; contiguous axial images were used for nodule measurement. Image interpretation was conducted double-blindly by two radiologists with more than 5 years of experience in chest imaging diagnosis, and inconsistent opinions were confirmed through in-department consultation. Inter-reader agreement for nodule diameter measurement was assessed; the intraclass correlation coefficient (ICC) was 0.92, indicating excellent inter-observer reliability. Given the sub-centimeter size of included nodules, inter-reader measurement variability is approximately 0.6 mm, which is comparable to the reported between-group effect size of nodule diameter change in this study. On lung window settings (window width: 1400 HU, window level: −700 HU), the maximum transverse diameter and the perpendicular transverse diameter of pulmonary nodules at the largest cross-sectional level were measured, and the average value was taken as the nodule diameter (unit: mm). Each nodule was measured three times, and the mean value was adopted. The Mayo malignant risk prediction model was applied here only for exploratory comparative analysis between groups at baseline and 3-month follow-up. It is acknowledged that the original Mayo model was established and validated for pulmonary nodules of 4–30 mm detected by chest radiography, and excluded patients with a cancer history within 5 years. In addition, this model has not been formally validated for longitudinal dynamic risk score changes over a 3-month follow-up period in small solitary pulmonary nodules (≤10 mm) detected by chest CT. Therefore, the calculated Mayo risk scores in this study are for reference only and cannot be interpreted as precise clinical malignant probability prediction. The Mayo model was used to calculate the malignant transformation risk score of nodules, with the formula: Malignant probability = e^x / (1 + e^x), where x = −6.8272 + 0.0391×age + 0.7917×smoking history + 1.3388×tumor history + 0.1274×diameter + 1.0407×spiculation + 0.7838×upper lobe involvement.13
Detection of Inflammatory Factors
Five milliliters of fasting peripheral venous blood was collected from each patient, and the serum was separated by centrifugation and stored at −80 °C for subsequent detection. Serum IL-6 was measured by chemiluminescent immunoassay, CRP by immunoturbidimetry, and the absolute count of peripheral blood neutrophils by an automated hematology analyzer. All experimental procedures were performed in strict accordance with the manufacturers’ instructions for the corresponding kits and instruments.
Statistical Analysis
Prior to patient enrollment, a priori sample size calculation was performed based on the primary endpoint of pulmonary nodule diameter change. Setting α=0.05, β=0.2, and expecting a detectable intergroup difference with an estimated standard deviation, the required sample size was calculated. Considering a 10% loss to follow-up rate, a total of 59 participants (observation group n=30, control group n=29) were finally enrolled.
This study was reported following the CONSORT 2010 guideline, and a detailed CONSORT participant flow diagram documenting patient screening, eligibility assessment, randomization, group allocation, intervention implementation, and 3-month follow-up outcomes was provided (see Figure 1).
 |
Figure 1 CONSORT flow diagram of patient screening, enrollment, randomization, intervention and follow-up. |
Intervention adherence was strictly recorded throughout the trial. All enrolled 59 patients completed the full 14-day inhalation intervention as scheduled without protocol violation, withdrawal, or loss to follow-up, showing good treatment compliance.
Adverse event surveillance and safety evaluation were conducted throughout the intervention period and the 3-month follow-up. Physical discomfort, respiratory symptoms and any adverse reactions were routinely monitored. No intervention-related adverse events or severe adverse reactions occurred in either group during the whole study period, supporting the safety of hydrogen-oxygen inhalation intervention.
All data analyses were performed using the SPSS 27.0 statistical software package. Categorical data were presented as n (%), and the chi-square test was used for intergroup comparisons. Normally distributed continuous data were expressed as mean ± standard deviation (x±s), with the paired t-test for intragroup comparisons before and after treatment and the independent samples t-test for intergroup comparisons. The Mayo malignant transformation risk score showed a highly skewed distribution with standard deviation greater than the mean in both groups; thus, parametric t-test was not appropriate. The Mann–Whitney U-test was adopted for intergroup comparison and the Wilcoxon signed-rank test for intra-individual before-and-after comparison of Mayo scores. Non-normally distributed continuous data were reported as median (interquartile range) [M (Q1, Q3)] and analyzed using the Mann–Whitney U-test. To control type I error caused by multiple comparisons, the Bonferroni correction was applied for multiple secondary outcome comparisons; the threshold of statistical significance was adjusted accordingly. The smoking subgroup analysis was treated as exploratory, and no formal multiplicity adjustment was applied, whose results were only interpreted as hypothesis-generating findings. A two-sided P value < 0.05 was considered statistically significant. It should be acknowledged that the limited sample size of the overall cohort and the small smoking subgroup (14 vs 16) may lead to insufficient statistical power; some non-significant results may be attributable to underpowered analysis rather than a true lack of intergroup difference.
Results
Comparison of Baseline General Data Between the Two Groups
No statistically significant differences were observed between the observation group and the control group in terms of age, gender, smoking history, tumor history, baseline nodule diameter, inflammatory factors (IL-6, CRP, neutrophil count), and Mayo malignant transformation risk score (all P>0.05). The baseline data of the two groups were well balanced and comparable (Table 1). Notably, baseline IL-6 and peripheral blood neutrophil counts in both groups were within normal clinical reference ranges, and the baseline mean diameter of pulmonary nodules was 3–4 mm, which is close to the inherent measurement variability of routine thin-slice chest CT.
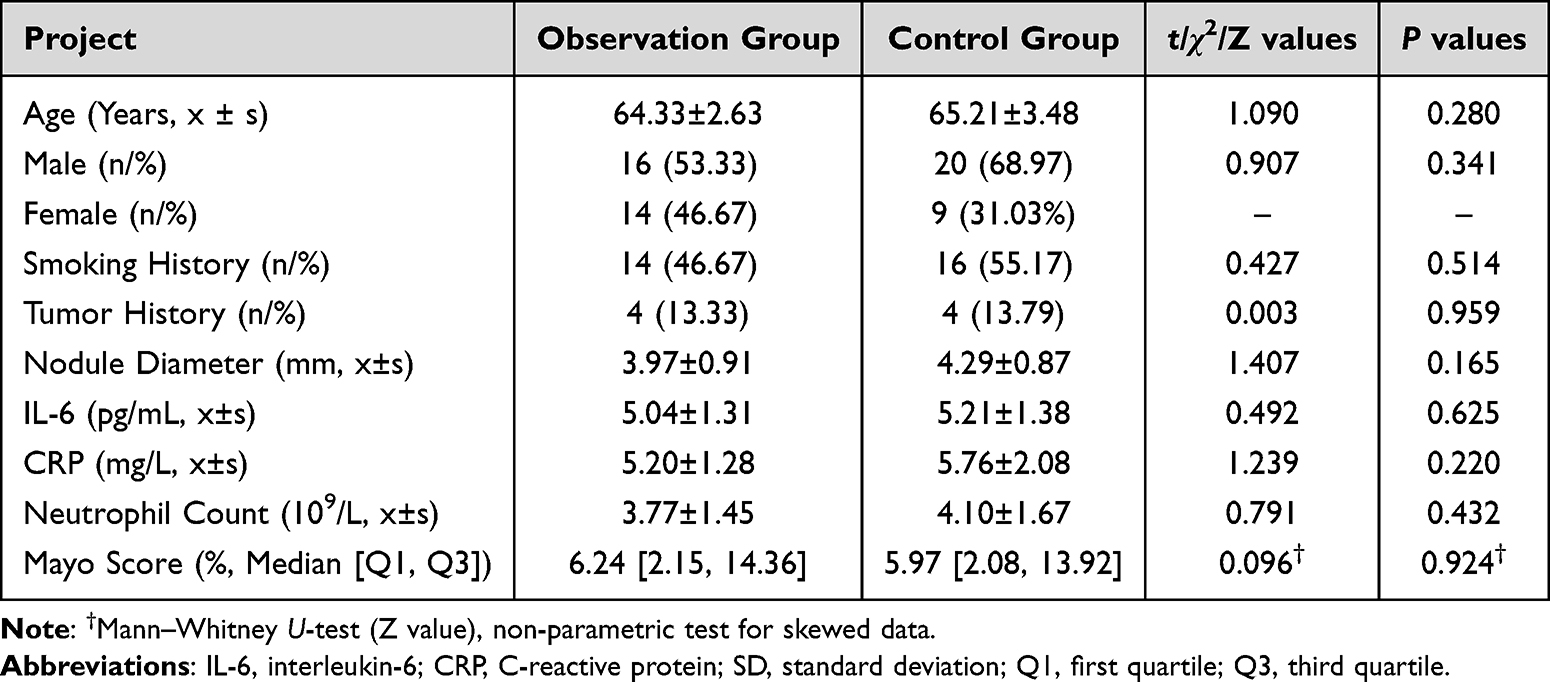 |
Table 1 Comparison of General Clinical Data Between the Observation Group and the Control Group |
Comparisons of Nodule-Related Indicators and Inflammatory Factors Between the Two Groups Before and After Treatment
After intervention, the nodule diameter, IL-6 level and peripheral blood neutrophil count in the observation group were significantly decreased compared with those before treatment (P<0.01), while no significant differences were found in CRP level and Mayo malignant transformation risk score in the observation group before and after treatment (P>0.05). No statistically significant differences were observed in all the above indicators in the control group before and after treatment (P>0.05). Intergroup comparison showed that the nodule diameter, IL-6 level and neutrophil count in the observation group after intervention were significantly lower than those in the control group (P<0.01), whereas there were no significant differences in CRP level and Mayo score between the two groups after intervention (P>0.05). Although the inter-group differences of the above indicators reached statistical significance, the effect sizes were modest, and the clinical significance of the 0.64 mm reduction in nodule diameter remains uncertain, as this magnitude is comparable to the inherent measurement variability of thin-slice CT for small pulmonary nodules of 3–4 mm. Representative imaging findings of pulmonary nodules are presented in Figure 2A. Figure 2B–E visualized the quantitative data of nodule-related indicators and inflammatory factors before and after intervention using histograms, with 95% confidence intervals (CIs) of effect sizes provided to reflect the range of therapeutic effects. Figure 2F presents the box plot of Mayo Score. Due to the highly skewed data distribution, data were expressed as median (interquartile range), and mean differences and corresponding 95% CIs were not calculated. Wilcoxon signed-rank test was used for within-group comparisons. No statistically significant differences were found in intra-group changes or post-treatment inter-group comparisons.
 |
Figure 2 Comparisons of Nodule-Related Indicators and Inflammatory Factors Between the Two Groups Before and After Treatment. (A) Imaging Findings of Pulmonary Nodules. Red arrows indicate the target pulmonary nodules in each image. All before/after CT image pairs within each patient are acquired at the same anatomical level. Imaging parameters: slice thickness = 1 mm, window width = 1400 HU, window level = −700 HU; the scale bar is inherently included in each image, located at the bottom and rightmost side of the image respectively. (B) Pulmonary Nodule Diameter. Data are expressed as mean ± standard deviation (SD). Intra-group mean differences (95% CI): observation group 0.64 (0.20, 1.08) mm, control group 0.10 (−0.32, 0.52) mm. Observation group (n=30): mean nodule diameter was 3.97 mm before treatment and 3.33 mm after treatment. Control group (n=29): mean nodule diameter was 4.29 mm before treatment and 4.19 mm after treatment. Paired t-test was used for intra-group comparisons. The mean reduction in nodule diameter in the observation group was statistically significant (P=0.006), while no significant change was observed in the control group (P=0.641). Inter-group comparison showed significant difference after treatment (P=0.000). (C) IL-6 Level. Data are expressed as mean ± SD. Intra-group mean differences (95% CI): observation group 1.36 (0.70, 2.02) pg/mL, control group 0.16 (−0.54, 0.86) pg/mL. Observation group (n=30): the mean IL-6 level was 5.04 pg/mL before treatment and 3.68 pg/mL after treatment. Control group (n=29): the mean IL-6 level was 5.21 pg/mL before treatment and 5.05 pg/mL after treatment. Paired t-test was used for intra-group comparisons. The decrease was statistically significant in the observation group (P=0.000), while no significant change was observed in the control group (P=0.655). Significant inter-group difference was identified after treatment (P=0.000). (D) CRP Level. Data are expressed as mean ± SD. Intra-group mean differences (95% CI): observation group 0.19 (−0.45, 0.83) mg/L, control group 0.28 (−0.72, 1.28) mg/L. Observation group (n=30): the mean CRP level was 5.20 mg/L before treatment and 5.01 mg/L after treatment. Control group (n=29): the mean CRP level was 5.76 mg/L before treatment and 5.48 mg/L after treatment. Paired t-test was used for intra-group comparisons. No significant pre- and post-intervention differences were found in either group (P=0.563, P=0.587, respectively). No significant inter-group difference was detected after treatment (P=0.239). (E) Neutrophil Count. Data are expressed as mean ± SD. Intra-group mean differences (95% CI): observation group 1.14 (0.51, 1.77) ×109/L, control group 0.25 −0.65, 1.15) ×109/L. Observation group (n=30): the mean neutrophil count was 3.77×109/L before treatment and 2.63×109/L after treatment. Control group (n=29): the mean neutrophil count was 4.10×109/L before treatment and 3.85×109/L after treatment. Paired t-test was used for intra-group comparisons. A significant reduction was detected in the observation group (P=0.001), and no obvious change was shown in the control group (P=0.582). Significant inter-group difference was observed after treatment (P=0.001). (F) Mayo Score. Data are presented as median (interquartile range) owing to the highly skewed distribution, with no mean difference and 95% CI calculated. Observation group (n=30): Baseline Mayo score was 4.24 [2.03, 10.48], and 4.00 [2.07, 9.02] after intervention. Control group (n=29): Baseline Mayo score was 5.00 [3.96, 10.72], and 4.81 [3.96, 10.72] after intervention. Wilcoxon signed-rank test was used for intra-group comparison. No significant intra-group difference was observed in both groups (P=0.859, P=0.984, respectively). No significant inter-group difference was found after treatment (P=0.946). |
Comparisons of Inflammatory Factors in the Smoking Subgroup Before and After Treatment
No statistically significant differences were found in baseline general data and inflammatory factors between smoking patients of the two groups (P>0.05). After intervention, the IL-6 level and neutrophil count in smoking patients of the observation group were significantly decreased compared with those before treatment (P<0.01), while the CRP level showed no obvious change (P>0.05). For smoking patients in the control group, there were no statistically significant differences in all inflammatory factors before and after treatment (P>0.05). Intergroup comparison indicated that the IL-6 level and neutrophil count in smoking patients of the observation group after intervention were significantly lower than those in smoking patients of the control group (P<0.01), and no significant difference was observed in the CRP level between the two subgroups (P>0.05) (Figure 3). This subgroup analysis provides exploratory evidence for the intervention effect in smoking populations, while the small sample size of the subgroup limits the definitive interpretation of the results.
 |
Figure 3 Comparisons of Inflammatory Factors in Smoking Patients Between the Two Groups Before and After Treatment. (A) IL-6 Level. Data are expressed as mean ± SD. Observation group (n=14): the mean IL-6 level was 5.33 pg/mL before treatment and 3.26 pg/mL after treatment. Control group (n=16): the mean IL-6 level was 5.66 pg/mL before treatment and 5.12 pg/mL after treatment. Paired t-test was used for intra-group comparisons. A significant decrease was found in the observation group (P=0.000), while no significant intra-group change was observed in the control group (P=0.270). Inter-group difference was significant after treatment (P=0.001). (B) CRP Level. Data are expressed as mean ± SD. Observation group (n=14): the mean CRP level was 5.71 mg/L before treatment and 5.15 mg/L after treatment. Control group (n=16): the mean CRP level was 5.82 mg/L before treatment and 5.53 mg/L after treatment. Paired t-test was used for intra-group comparisons. No significant pre- and post-intervention differences were detected in either group (P=0.155, P=0.690, respectively). No significant inter-group difference was observed after treatment (P=0.461). (C) Neutrophil Count. Data are expressed as mean ± SD. Observation group (n=14): the mean neutrophil count was 4.11×109/L before treatment and 2.30×109/L after treatment. Control group (n=16): the mean neutrophil count was 4.96×109/L before treatment and 4.91×109/L after treatment. Paired t-test was used for intra-group comparisons. The observation group showed a statistically significant reduction after intervention (P=0.000), and no obvious change was found in the control group (P=0.925). Significant inter-group difference was detected after treatment (P=0.000). |
Discussion
The formation and progression of SPNs result from the synergistic effects of multiple factors including oxidative stress imbalance, chronic inflammatory microenvironment disorder, and abnormal cell proliferation, among which local chronic pulmonary inflammation serves as a core pathophysiological process driving nodule hyperplasia and even malignant transformation.14 Persistent chronic inflammation can induce alveolar epithelial cell injury and interstitial fibrosis, activate inflammatory signaling pathways, and promote the release of proinflammatory cytokines, thus forming a vicious cycle of inflammation-injury-proliferation and ultimately increasing the risk of lung cancer.15 Currently, there is a lack of effective clinical interventions for SPNs. As a novel therapeutic gas, hydrogen, with its anti-inflammatory and antioxidant properties, provides a new direction for the intervention of SPNs. This preliminary randomized controlled trial confirmed that hydrogen-oxygen inhalation could significantly reduce the diameter of SPNs and downregulate the levels of peripheral blood IL-6 and neutrophil count, with exploratory subgroup findings suggesting potential anti-inflammatory trends in smoking patients; however, no formal treatment × smoking interaction analysis was performed to confirm a genuine subgroup-specific effect. Its core mechanism is closely associated with hydrogen-mediated regulation of the pulmonary inflammatory microenvironment and inhibition of oxidative stress injury.
It is worth noting that all detected indicators also show slight favorable changes in the air inhalation control group after follow-up, and this mild positive trend without statistical significance is comprehensively explained as follows. Firstly, all enrolled patients received unified standardized routine health management throughout the trial, including regular lifestyle guidance, smoking cessation advocacy, dust and harmful gas avoidance, and daily respiratory health training, which can naturally alleviate mild chronic pulmonary inflammation and improve physical metabolic state, bringing subtle beneficial changes to relevant inflammatory and nodule-related indicators. Secondly, benign small pulmonary nodules have inherent self-stable tendency and slight spontaneous fluctuation in the short term, and mild inflammatory nodules can achieve partial spontaneous remission with the improvement of general physical condition. Thirdly, psychological comfort and regular clinical follow-up supervision in the control group can produce certain non-specific placebo effects, which may indirectly improve systemic inflammatory levels to a certain extent. Fourthly, minor detection errors and natural physiological fluctuation of peripheral blood inflammatory indicators also contribute to this mild positive trend in the control group. Importantly, these subtle improvements in the control group are not statistically significant, while the observation group achieves obvious and statistically meaningful improvements, further verifying the unique intervention efficacy of hydrogen-oxygen inhalation.
The results of this preliminary study demonstrated that the nodule diameter in the observation group was significantly smaller than that in the control group at the 3-month follow-up after 14 days of hydrogen-oxygen inhalation intervention, suggesting that hydrogen-oxygen inhalation could effectively inhibit the progression of SPNs. This finding is closely associated with the selective antioxidant effect of hydrogen: a landmark study by Ohsawa et al proposed the classical antioxidant mechanism of hydrogen, which has been widely recognized but also exists academic controversies. This study initially proposed that hydrogen could selectively scavenge highly toxic hydroxyl radicals (·OH) in the body, and initially mentioned the potential reaction with peroxynitrite anions (ONOO−);16 however, subsequent rigorous mechanistic research by Penders et al confirmed that hydrogen does not react with peroxynitrite (ONOO−), and peroxynitrite is not a free radical, so the selective antioxidant effect of hydrogen is only limited to highly toxic hydroxyl radicals (·OH), without affecting physiological reactive oxygen species (ROS) such as superoxide anions and hydrogen peroxide, thus avoiding the disruption of the body’s normal redox balance.5 Meanwhile, a latest study by Negishi et al discovered a new molecular target of hydrogen, identifying the Rieske iron-sulfur protein as the primary target of hydrogen, which enriches the mechanistic system of hydrogen’s biological effects beyond free radical scavenging.7 Accumulated preclinical studies have indicated that hydrogen may exert pulmonary protective effects potentially through the Nrf2/HO-1-dependent pathway. These reported experimental findings, rather than data from the current trial, have shown that in a mouse model of sepsis, inhalation of 2% hydrogen significantly upregulated the expression of HO-1, a downstream target gene of Nrf2, in lung tissues, enhanced the activities of antioxidant enzymes such as superoxide dismutase (SOD) and catalase (CAT), reduced the production of malondialdehyde (MDA), an oxidative product, and simultaneously inhibited the release of HMGB1 and the expression of proinflammatory cytokines including TNF-α and IL-6. These effects alleviate oxidative stress and inflammatory injury in lung tissues, thereby suppressing abnormal pathological changes in the lungs.17 It is hypothesized that hydrogen may also possess potential antifibrotic bioactivity based on previous animal investigations; such antifibrotic and microenvironment-regulating effects have not been validated in our SPN cohort. Studies have verified that in a monocrotaline-induced pulmonary hypertension rat model, hydrogen inhalation can potentially regulate the function of mast cells in lung tissues, downregulate the expression of tryptase and TGF-β, inhibit the formation of collagen fibrils and the deposition of collagen fibers and elastic fibers in the extracellular matrix, and ameliorate the fibrotic phenotype of the local pulmonary tissue microenvironment.18 Combined with the nodule diameter reduction observed in our trial, we tentatively speculate that hydrogen may exert an inhibitory effect on the progression of SPNs by regulating the pulmonary interstitial microenvironment and suppressing the fibrotic process, which remains a mechanistic hypothesis to be further verified.
Abnormal expression of inflammatory cytokines represents a core hallmark of chronic pulmonary inflammation.19 Among these, IL-6, a key proinflammatory cytokine, has been reported to be capable of activating the NF-κB pathway, promote neutrophil infiltration and exacerbate pulmonary inflammatory injury;20,21 it also induces tumor cell proliferation and invasion, thus being closely correlated with the malignant transformation risk of SPNs.22 As the major inflammatory cells in peripheral blood, an elevated neutrophil count can reflect the activity of local pulmonary inflammation.23 The present study found that hydrogen-oxygen inhalation significantly downregulated the peripheral blood IL-6 levels and neutrophil counts in patients, with no significant changes in CRP levels observed between the two groups. Notably, the null finding for CRP is most parsimoniously attributed to inadequate statistical power due to the small overall sample size, as well as the potential inappropriateness of CRP as an outcome measure for localized pulmonary inflammation in sub-centimeter SPNs, rather than over-interpretation of indicator specificity. Based on existing literature, it is reasonable to hypothesize that hydrogen can inhibit the phosphorylative activation of the NF-κB pathway, block the transcription and release of proinflammatory cytokines, and reduce the infiltration and activation of neutrophils in the lungs, thereby specifically ameliorating the status of local pulmonary inflammation. Moreover, hydrogen may potentially modulate macrophage polarization toward the M2 anti-inflammatory phenotype according to previous mechanistic studies; however, macrophage polarization status was not examined in the present study. Such presumed M2 polarization activation could further suppress pulmonary inflammatory responses and downregulate the levels of proinflammatory cytokines such as IL-6. No significant difference in the Mayo malignant transformation risk score was observed between the two groups post-intervention. This null result is primarily driven by inadequate statistical power from the limited sample size and the inherent inappropriateness of the Mayo score as a longitudinal outcome for short-term intervention in small SPNs: the original Mayo model was designed for cross-sectional malignant risk prediction of 4–30 mm nodules, not for detecting short-term score changes in sub-centimeter low-to-moderate risk nodules, which aligns with the simpler explanation of suboptimal power and inappropriate outcome selection.
Subgroup analysis of smokers (n=14 vs 16) should be interpreted with extreme caution: this study did not conduct a formal treatment × smoking interaction test to verify whether the intergroup difference was genuinely modified by smoking status. The seemingly more pronounced reductions in IL-6 and neutrophil counts in the smoking subgroup may merely reflect random subgroup noise rather than a reliable specific advantage of hydrogen intervention in smokers. Smoking is a crucial risk factor for the formation and malignant transformation of SPNs; harmful substances such as nicotine, tar and polycyclic aromatic hydrocarbons in tobacco smoke can induce pulmonary oxidative stress injury, activate the NF-κB pathway as documented in prior research, and promote the massive release of proinflammatory cytokines including IL-6. Meanwhile, they induce neutrophil infiltration, leading to the formation of a persistent pulmonary inflammatory microenvironment and accelerating nodule progression.24 We speculate that hydrogen can reverse smoking-induced pulmonary injury through a dual mechanism: on the one hand, its selective antioxidant effect specifically scavenges the highly toxic hydroxyl radicals (·OH) induced by tobacco smoke (rather than a large number of toxic free radicals, and superoxide anions and peroxynitrite are not involved in this process), reducing oxidative damage to lung tissues; on the other hand, hydrogen is presumed to specifically inhibits the NF-κB inflammatory pathway activated by smoking, blocks the release of proinflammatory cytokines and reduces neutrophil infiltration, thereby ameliorating the pulmonary inflammatory state in smoking populations in a targeted manner. Given the small unbalanced subgroup size and lack of interaction testing, this subgroup finding is considered exploratory and hypothesis-generating rather than a definitive conclusion.
In addition, all participants received unified smoking cessation guidance during the trial, yet no obvious smoking reduction or smoking cessation behavior occurred in smokers, and individual smoking status remained stable throughout the follow-up period. It is confirmed that the positive efficacy changes in this study are independent of smoking habit improvement, and smoking-related confounding interference has been effectively excluded.
The strengths of this study are as follows: a randomized controlled trial design was adopted with rigorous control of baseline data between the two groups to eliminate the interference of confounding factors, making the study design highly consistent with clinical practice; the trial was performed with single-blinded outcome assessment and reported in accordance with the CONSORT 2010 statement to improve methodological transparency; additionally, hydrogen-oxygen inhalation features non-invasiveness, safety, low cost and high patient acceptability, endowing it with a promising clinical application prospect. However, this study still has certain limitations fully matching the preliminary nature of this research. First, as a single-center study with a small sample size, although a priori sample size calculation was performed, the final enrolled cohort remained relatively small, leading to limited statistical power for secondary endpoints and subgroup comparisons; it may be subject to selection bias and insufficient statistical power to detect significant changes in secondary outcomes such as CRP and Mayo score, which is the primary reason for the null findings of these two indicators, and the generalizability of the results needs to be further verified by multi-center and large-sample studies. Second, the follow-up duration was relatively short, with only short-term effects observed at 3 months; thus, the long-term impact of hydrogen-oxygen inhalation on the progression and malignant transformation risk of SPNs cannot be determined, and it is necessary to extend the follow-up period to 1–3 years to track the dynamic changes in nodule morphology and size as well as the long-term prognosis of patients. Third, only routine peripheral blood inflammatory indicators (IL-6, CRP and neutrophil count) were detected in this study. We did not quantify the expression of Nrf2/HO-1, NF-κB pathway activity, M2 macrophage polarization markers, mast cell function-related molecules, or fibrosis-related biomarkers. Therefore, all discussions on these molecular and cellular mechanisms are speculative and based solely on published preclinical evidence, rather than direct experimental verification from the present cohort. Fourth, the influence of nodule morphology, density and location on the efficacy of hydrogen-oxygen intervention was not analyzed, failing to clarify the differential intervention effects of hydrogen-oxygen inhalation on different types of SPNs. Fifth, the selection of CRP and Mayo score as secondary outcomes may be inappropriate for this study cohort: CRP is a systemic inflammatory marker with low sensitivity to local pulmonary micro-inflammation, and Mayo score is not validated for short-term longitudinal evaluation of sub-centimeter SPNs, which contributed to the null results of these two indicators. Sixth, inter-reader measurement variability of chest CT nodule diameter was acknowledged but its potential impact on outcome interpretation was not fully quantified in statistical analysis. Seventh, although adverse events were monitored throughout the trial, detailed systematic reporting of adverse event profiles and safety outcomes was limited. Eighth, the application of Bonferroni correction for multiple comparisons was performed, but the inflated type I error risk across multiple secondary and subgroup endpoints cannot be fully excluded. Ninth, the clinical hydrogen-oxygen inhalation device used in this study (AMS-H-03) can only output fixed proportion mixed gas containing 66.6% hydrogen and 33.3% oxygen, and cannot independently adjust oxygen concentration or prepare hydrogen-air mixed gas for additional control group. The oxygen concentration of inhaled gas in the observation group is slightly higher than 21% oxygen concentration of ambient air in the control group, so we cannot completely rule out the potential interference effect of elevated oxygen concentration on the final efficacy results. In future research, we will further set up a hydrogen-air inhalation control group to strictly distinguish the biological effects derived from hydrogen gas rather than high-concentration oxygen. Subsequent studies will expand the sample size to improve statistical power, incorporate formal interaction tests to validate subgroup effects, optimize outcome measure selection by choosing more sensitive indicators for local pulmonary inflammation and dynamic risk assessment, extend the follow-up time, and detect more inflammatory and oxidative stress indicators. Combined with techniques such as single-cell sequencing and multi-omics analysis, we will formally validate the potential roles of the Nrf2/HO-1 and NF-κB pathways, macrophage polarization, mast cell regulation and anti-fibrotic mechanisms underlying the regulatory effect of hydrogen on SPNs, so as to provide a more solid theoretical basis for its clinical application.
In conclusion, this preliminary exploratory study confirmed that hydrogen-oxygen inhalation can significantly reduce the diameter of SPNs and effectively downregulate the peripheral blood levels of IL-6 and neutrophil count, exerting a tentative regulatory effect on local pulmonary inflammation. Subgroup trends in smoking patients should be interpreted cautiously as exploratory observations due to small sample size and absence of formal interaction testing, rather than a confirmed specific advantage. Given the limitations of single-center design, small sample size (n=59), short 3-month follow-up, and lack of systematic adverse event safety documentation, the present study cannot definitively establish hydrogen-oxygen inhalation as a confirmed safe, non-invasive clinical adjuvant intervention for SPNs. Our findings should be regarded as hypothesis-generating only, pending rigorous confirmation in future adequately powered multi-center trials with pre-specified primary endpoints, prolonged observational duration, and standardized systematic safety surveillance. Further high-level evidence is still required before recommending its routine clinical application for SPNs, especially smoking-related SPNs.
Data Sharing Statement
The individual participant data supporting the findings of this study are not available to be shared publicly, as they contain privacy-related information. Further data inquiries can be directed to the corresponding author.
Acknowledgments
The authors extend their sincere gratitude to all researchers who have contributed to this study.
Funding
The Project Supported by Dongying City Major Science and Technology Innovation Special Projects (2024ZDJH91).
Disclosure
The authors declare that they have no competing interests in this work. The hydrogen-oxygen generator manufacturer (Shanghai Asclepius Meditec Co., Ltd.) had no involvement in study design, data collection, statistical analysis, manuscript drafting, or decision for publication, and imposes no commercial bias on the study results and conclusions.
References
1. Smolarz B, Łukasiewicz H, Samulak D, Piekarska E, Kołaciński R, Romanowicz H. Lung cancer-epidemiology, pathogenesis, treatment and molecular aspect (Review of Literature). Int J Mol Sci. 2025;26(5):2049. doi:10.3390/ijms26052049
2. Park S, Choe J, Kim IH, et al. Prognostic variability in non-small cell lung cancer with pathologic separate nodules in the same lobe at CT. Radiology. 2025;316(1):e241492. doi:10.1148/radiol.241492
3. Chen JB, Kong XF, Qian W, et al. Two weeks of hydrogen inhalation can significantly reverse adaptive and innate immune system senescence patients with advanced non-small cell lung cancer: a self-controlled study. Med Gas Res. 2020;10(4):149–12. doi:10.4103/2045-9912.304221
4. Jiang Z, Ainiwaer M, Liu J, Ying B, Luo F, Sun X. Hydrogen therapy: recent advances and emerging materials. Biomater Sci. 2024;12(16):4136–4154. doi:10.1039/d4bm00446a
5. Penders J, Kissner R, Koppenol WH. ONOOH does not react with H2: potential beneficial effects of H2 as an antioxidant by selective reaction with hydroxyl radicals and peroxynitrite. Free Radic Biol Med. 2014;75:191–194. doi:10.1016/j.freeradbiomed.2014.07.025
6. Zheng ZG, Sun WZ, Hu JY, et al. Hydrogen/oxygen therapy for the treatment of an acute exacerbation of chronic obstructive pulmonary disease: results of a multicenter, randomized, double-blind, parallel-group controlled trial. Respir Res. 2021;22(1):149. doi:10.1186/s12931-021-01740-w
7. Negishi S, Ito M, Hasegawa T, et al. The Rieske iron-sulfur protein is a primary target of molecular hydrogen. Redox Biol. 2025;88:103952. doi:10.1016/j.redox.2025.103952
8. Gou X, Xu W, Liu Y, et al. IL-6 prevents lung macrophage death and lung inflammation injury by inhibiting GSDME- and GSDMD-mediated pyroptosis during pneumococcal pneumosepsis. Microbiol Spectr. 2022;10(2):e0204921. doi:10.1128/spectrum.02049-21
9. Lei Y, Cao C, Tang R, Liu Y. Peripheral blood inflammatory biomarkers neutrophil/ lymphocyte ratio, platelet/lymphocyte ratio and systemic immune-inflammation index/albumin ratio predict prognosis and efficacy in non-small cell lung cancer patients receiving immunotherapy and opioids. BMC Cancer. 2025;25(1):664. doi:10.1186/s12885-025-14060-9
10. VanDevanter DR, Heltshe SL, Skalland M, et al. C-reactive protein (CRP) as a biomarker of pulmonary exacerbation presentation and treatment response. J Cyst Fibros. 2022;21(4):588–593. doi:10.1016/j.jcf.2021.12.003
11. MacMahon H, Naidich DP, Goo JM, et al. Guidelines for management of incidental pulmonary nodules detected on CT images: from the fleischner society 2017. Radiology. 2017;284(1):228–243. doi:10.1148/radiol.2017161659
12. Provenzale D, Gupta S, Ahnen DJ, et al. NCCN guidelines insights: colorectal cancer screening, version 1.2018. J Natl Compr Canc Netw. 2018;16(8):939–949. doi:10.6004/jnccn.2018.0067
13. Swensen SJ, Silverstein MD, Ilstrup DM, Schleck CD, Edell ES. The probability of malignancy in solitary pulmonary nodules. Application to small radiologically indeterminate nodules. Arch Intern Med. 1997;157(8):849–855.
14. Tian T, Lu J, Zhao W, et al. Associations of systemic inflammation markers with identification of pulmonary nodule and incident lung cancer in Chinese population. Cancer Med. 2022;11(12):2482–2491. doi:10.1002/cam4.4606
15. Wu J, He Z, Zhuang W, et al. Mechanisms of inflammation-driven lung cancer: from external influences to internal regulation. Clin Immunol. 2025;279:110572. doi:10.1016/j.clim.2025.110572
16. Ohsawa I, Ishikawa M, Takahashi K, et al. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007;13(6):688–694. doi:10.1038/nm1577
17. Yu Y, Yang Y, Yang M, Wang C, Xie K, Yu Y. Hydrogen gas reduces HMGB1 release in lung tissues of septic mice in an Nrf2/HO-1-dependent pathway. Int Immunopharmacol. 2019;69:11–18. doi:10.1016/j.intimp.2019.01.022
18. Atiakshin D, Kostin A, Alekhnovich A, et al. The role of mast cells in the remodeling effects of molecular hydrogen on the lung local tissue microenvironment under simulated pulmonary hypertension. Int J Mol Sci. 2024;25(20):11010. doi:10.3390/ijms252011010
19. Agusti A, Singh D, Faner R. Treatment of chronic obstructive pulmonary disease: current pipeline and new opportunities. Nat Rev Drug Discov. 2026;25(2):98–115. doi:10.1038/s41573-025-01290-6
20. Gu M, Pang Z. Luteolin inhibits inflammation and M1 macrophage polarization in the treatment of Pseudomonas aeruginosa-induced acute pneumonia through suppressing EGFR/PI3K/AKT/NF-kappaB and EGFR/ERK/AP-1 signaling pathways. Phytomedicine. 2025;141:156663. doi:10.1016/j.phymed.2025.156663
21. Imakiire S, Kimuro K, Yoshida K, et al. Activated factor X inhibition ameliorates NF-kappaB-IL-6-mediated perivascular inflammation and pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol. 2025;329(1):L183–L196. doi:10.1152/ajplung.00303.2024
22. Guo JH, Thuong LHH, Jiang YJ, et al. Cigarette smoke promotes IL-6-dependent lung cancer migration and osteolytic bone metastasis. Int J Biol Sci. 2024;20(9):3257–3268. doi:10.7150/ijbs.94339.eCollection2024
23. Wittermans E, van de Garde EM, Voorn GP, et al; Santeon-CAP study group. Neutrophil count, lymphocyte count and neutrophil-to-lymphocyte ratio in relation to response to adjunctive dexamethasone treatment in community-acquired pneumonia. Eur J Intern Med. 2022;96:102–108. doi:10.1016/j.ejim.2021.10.030
24. Langan RC, Goodbred AJ. Pulmonary Nodules: common Questions and Answers. Am Fam Physician. 2023;107(3):282–291.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.