Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Prehospital Tranexamic Acid Combined with Blood Transfusion Reduced the Short-Term Mortality Risk in Trauma Patients at Risk for Hemorrhage
Received 30 August 2025
Accepted for publication 30 November 2025
Published 31 December 2025 Volume 2025:21 Pages 1915—1921
DOI https://doi.org/10.2147/TCRM.S564232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Zheng Qian, Bining Yang
Department of Emergency Medicine, The Fourth Affiliated Hospital of Soochow University (Suzhou Dushu Lake Hospital), Suzhou, People’s Republic of China
Correspondence: Zheng Qian, Department of Emergency Medicine, The Fourth Affiliated Hospital of Soochow University (Suzhou Dushu Lake Hospital), No. 9 Chongwen Road, Suzhou Industrial Park, Suzhou, 215000, People’s Republic of China, Email [email protected]
Background: Hemorrhage is a leading cause of preventable death in trauma. While both blood transfusion and tranexamic acid (TXA) improve outcomes, the combined effect of prehospital TXA and transfusion remains uncertain. This study aims to evaluate the impact of prehospital TXA combined with blood transfusion on short-term mortality in trauma patients at risk for hemorrhage.
Methods: We performed a retrospective cohort study of 408 adult trauma patients at risk for hemorrhage admitted between 2018 and 2023. Patients were grouped into transfusion only (n=240) or prehospital TXA plus transfusion (n=168). The primary outcome was 30-day mortality. Secondary outcomes included 24-hour mortality, transfusion requirements, multiple organ failure (MOF), and venous thromboembolism (VTE).
Results: Compared with transfusion alone, prehospital TXA plus transfusion significantly reduced 30-day mortality (14.3% vs 31.3%, p< 0.01) and 24-hour mortality (6.0% vs 19.6%, p< 0.01). The TXA group also had lower MOF incidence (14.3% vs 28.7%, p< 0.01) and required less plasma and crystalloid resuscitation, without an increase in VTE (p=0.17). Kaplan–Meier analysis confirmed a survival advantage (log-rank p< 0.01), and multivariate Cox regression identified combination therapy as an independent predictor of reduced 30-day mortality (HR=2.16, 95% CI: 1.35– 3.46, p< 0.01).
Conclusion: Prehospital TXA combined with transfusion significantly improves short-term survival and reduces organ failure in bleeding trauma patients, without increasing thromboembolic risk. These findings support early integration of TXA into prehospital transfusion protocols.
Keywords: trauma, hemorrhage, tranexamic acid, blood transfusion, short-term mortality
Introduction
Trauma is a major global health burden and remains a leading cause of death, particularly among young adults. According to the World Health Organization (WHO), injuries account for approximately 4.4 million deaths annually, representing nearly 8% of global mortality.1 Hemorrhage is the most preventable cause of trauma-related death, contributing to nearly 30–40% of early in-hospital mortality.2 Most fatal bleeding occurs within the first six hours after admission, underscoring the importance of timely and effective hemostatic interventions.3
Blood transfusion is the cornerstone of resuscitation in hemorrhagic trauma and has been shown to improve survival.4 However, transfusion is associated with risks such as coagulopathy, transfusion-related acute lung injury, and immunological complications.5,6 Adjunctive therapies that enhance the efficacy and safety of transfusion are therefore needed.
Tranexamic acid (TXA), a synthetic antifibrinolytic agent, inhibits plasminogen activation and stabilizes fibrin clots.7 The landmark CRASH-2 trial, which enrolled over 20,000 trauma patients worldwide, demonstrated that early TXA administration reduced all-cause mortality by nearly 10%, with the greatest benefit observed when given within three hours of injury.8 Subsequent studies have confirmed the survival benefit of TXA in both civilian and military trauma populations.9,10
While both TXA and transfusion are integral to modern trauma care, the combined effect of prehospital TXA and transfusion remains poorly characterized. In many trauma systems, TXA is administered by emergency medical services (EMS) before or alongside initiation of blood transfusion. Whether this combination confers incremental survival benefit beyond transfusion alone remains unclear. We therefore conducted a retrospective cohort study to evaluate the impact of prehospital TXA combined with blood transfusion on short-term mortality in trauma patients at risk for hemorrhage. We hypothesized that combination therapy would reduce short-term mortality compared with transfusion alone.
Material and Methods
Population
We conducted a retrospective cohort study at a tertiary hospital between January 2018 and December 2023. All consecutive adult trauma patients admitted during the study period who met the eligibility criteria were screened. Patients younger than 18 years were excluded because the physiological characteristics, injury patterns, and transfusion protocols differ substantially between pediatric and adult trauma populations. Including pediatric patients could introduce heterogeneity and confound the interpretation of outcomes related to TXA and transfusion efficacy.
Inclusion criteria were: (1) age ≥18 years, (2) trauma patients at risk for hemorrhage, defined as systolic blood pressure (SBP) <90 mmHg, heart rate (HR) >110 beats/min, or transfusion of ≥1 unit of packed red blood cells (pRBC) within 24 hours after admission, and (3) Documentation of prehospital care (EMS record available). Exclusion criteria included: (1) isolated traumatic brain injury, drowning, or hanging, (2) prehospital cardiac arrest >5 minutes, (3) known pregnancy, (4) transfer from another hospital with incomplete transfusion/TXA data, and (5) documented contraindication to TXA (eg, history of thromboembolic disease or allergy).
Exposure
Patients were categorized into two groups: (1) transfusion only; (2) TXA plus transfusion. In this study, “transfusion” refers specifically to administration of blood products (pRBCs and plasma), not crystalloid or colloid fluids, which were recorded separately.
Blood transfusion in the prehospital setting is not universally available in China. Specialized EMS units carry pRBCs and can initiate transfusion in selected high-risk trauma patients following institutional massive transfusion protocol (MTP). Transfusion was triggered by hemodynamic instability, ongoing bleeding, hemoglobin <7 g/dL, or the need for surgical/interventional hemostasis.
Prehospital TXA was administered by EMS according to protocol: 1 g intravenous bolus over 10 minutes, followed by a 1 g infusion over 8 hours after hospital arrival if indicated. Prehospital transfusion was performed in hemodynamically unstable patients based on the MTP criteria outlined above.
Outcomes and Data Collection
The primary outcome was 30-day mortality. Secondary outcomes included 24-hour mortality, transfusion requirements within 24 hours, multiple organ failure (MOF), and venous thromboembolism (VTE).
Baseline data included demographics, mechanism of injury, prehospital variables (time, SBP, HR, Glasgow Coma Scale [GCS], crystalloid volume, and intubation), and emergency department (ED) parameters (SBP, HR, GCS). Injury severity was assessed using the Injury Severity Score (ISS). Resuscitation variables included transfusion of pRBCs and plasma, and crystalloid administration within 24 hours. Clinical outcomes were extracted from electronic records.
Statistical Analysis
The sample size was calculated to ensure adequate power to detect a clinically meaningful difference in 30-day mortality between groups. Assuming a difference of 15% in 30-day mortality between the transfusion-only group and the TXA plus transfusion group according to a previous study,11 a two-sided α of 0.05, and 80% power, a minimum of 150 patients per group was required. In this study, 168 patients in the TXA plus transfusion group and 240 patients in the transfusion-only group were included, which exceeded the required sample size and provided sufficient power to detect the expected difference.
Continuous variables are presented as mean and standard deviation (SD) and compared using the students’ t test. Categorical variables are presented as counts and percentages and compared using the Chi-square or Fisher’s exact test. Survival analysis was performed using the Kaplan–Meier method and compared with the Log rank test. Multivariate Cox proportional hazards regression was used to evaluate the association between treatment group and mortality outcomes after controlling potential confounding factors, with results reported as hazard ratios (HRs) and 95% confidence intervals (CIs).
All statistical analyses were performed using R software (version 4.2.3, R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value <0.05 was considered statistically significant.
Results
A total of 408 trauma patients at risk for hemorrhage were included, of whom 168 (41.2%) received prehospital TXA combined with blood transfusion and 240 (58.8%) received blood transfusion alone. As shown in Table 1, patients in the TXA group were significantly older (p<0.01). Sex distribution and mechanism of injury were similar between groups. Prehospital physiological parameters showed that the TXA group had higher SBP (p=0.03) and GCS (p=0.04) but received less crystalloid (p<0.01). Upon ED arrival, they had lower HR (p<0.01), higher GCS (p<0.01), and slightly lower SBP (p=0.04). ISS did not differ significantly (p=0.85). Both groups received comparable pRBC volumes (p=0.51), but the TXA group required significantly less plasma (p<0.01) and crystalloids (p<0.01).
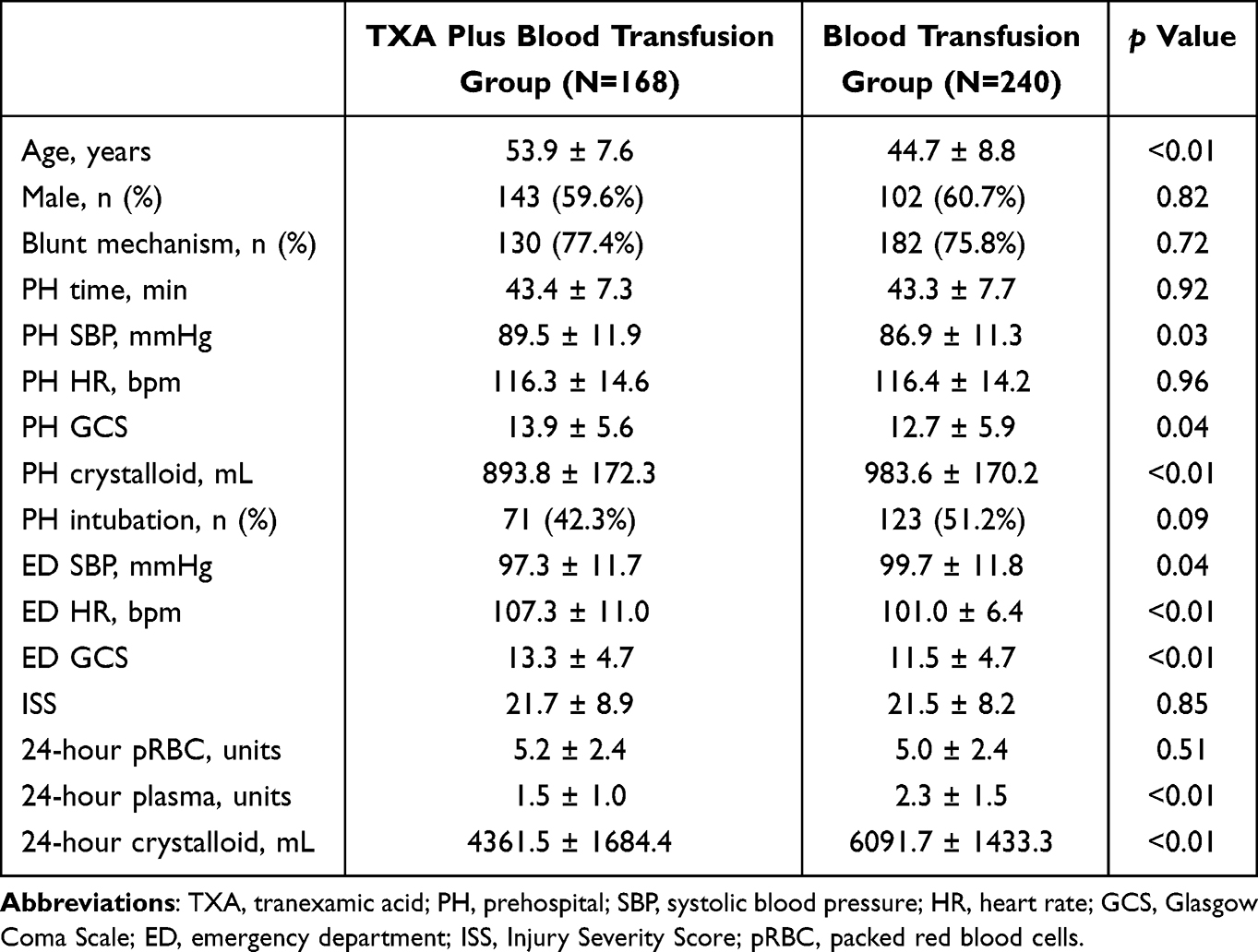 |
Table 1 Comparison of Patients’ Characteristics Between Tranexamic Acid (TXA) Combined with Blood Transfusion Group and Blood Transfusion Group |
Short-term mortality was markedly reduced in patients treated with prehospital TXA in addition to transfusion (Figure 1). Specifically, 30-day mortality was 14.3% in the TXA group versus 31.3% in the transfusion-only group (p<0.01), and 24-hour mortality was 6.0% versus 19.6%, respectively (p<0.01). MOF occurred less frequently with TXA (14.3% vs 28.7%, p<0.01), while VTE incidence did not differ (p=0.17).
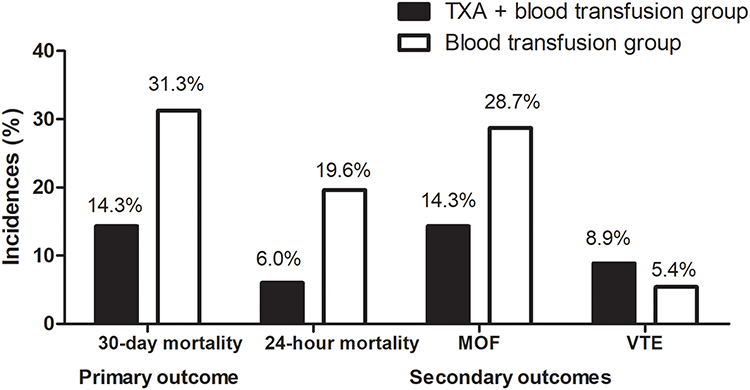 |
Figure 1 Comparison of the primary and secondary outcomes between prehospital tranexamic acid (TXA) combined with transfusion group and transfusion alone group. |
Kaplan–Meier analysis (Figure 2) demonstrated a survival advantage in the TXA group (log-rank p<0.01). Multivariate Cox regression (Table 2) confirmed that TXA plus transfusion independently reduced 30-day mortality (HR=2.16, 95% CI: 1.35–3.46, p<0.01). MOF (HR=3.50, 95% CI: 2.35–5.23, p<0.01) was also independent mortality predictors.
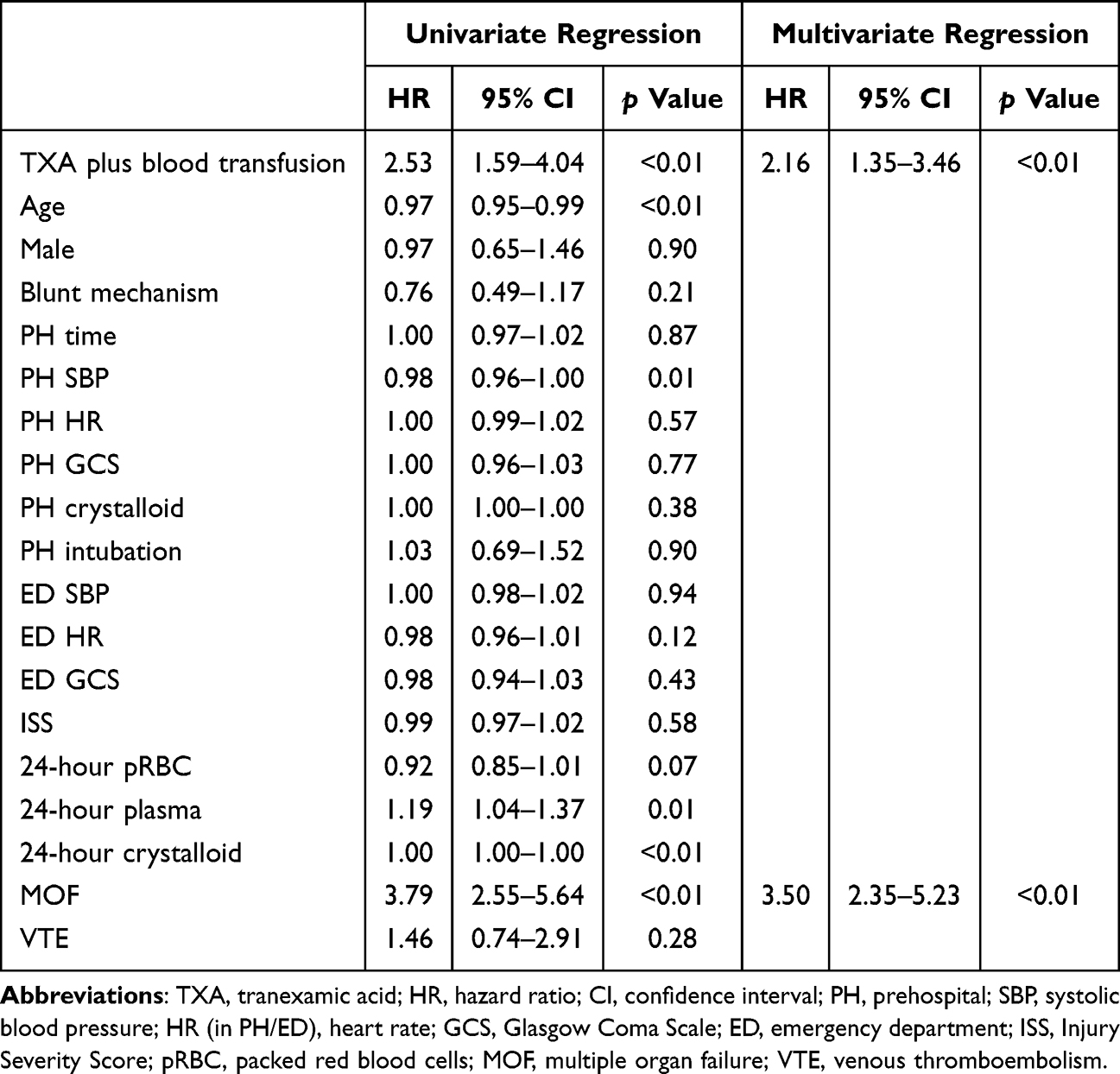 |
Table 2 Univariate and Multivariate Cox Regression to Explore the Association Between Tranexamic Acid (TXA) Combined with Blood Transfusion and the Risk of 30-Day Mortality |
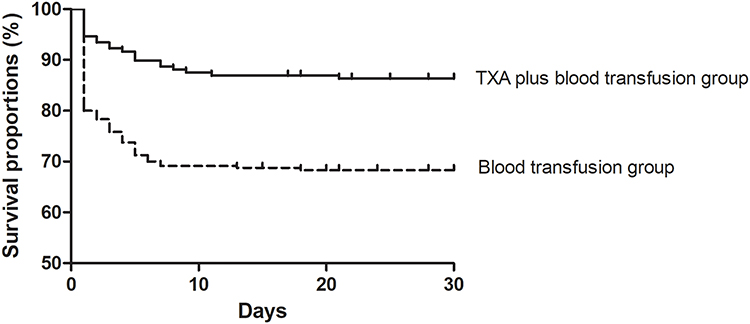 |
Figure 2 Kaplan–Meier survival curves depicting 30-day mortality risk in patients receiving prehospital tranexamic acid (TXA) combined with transfusion versus transfusion alone. |
Discussion
This study demonstrates that prehospital TXA administration combined with blood transfusion significantly reduced both 24-hour and 30-day mortality in trauma patients at risk for hemorrhage, with lower MOF incidence and no increase in VTE. These findings highlight the synergistic effect of antifibrinolytic therapy and transfusion in early trauma resuscitation.
Synergy with Existing Evidence
Our findings are consistent with those reported by Deeb et al,11 who analyzed data from the STAAMP trial and demonstrated that patients receiving both prehospital TXA and pRBCs had improved survival compared with those who received either treatment alone or neither. In line with their study, we observed a significant reduction in both 24-hour and 30-day mortality among patients treated with prehospital TXA in combination with transfusion. Importantly, our study included a larger sample size than the STAAMP trial analysis, thereby providing additional validation that TXA and transfusion act synergistically to improve outcomes in trauma patients at risk for hemorrhage. These consistent results across different cohorts strengthen the robustness of the evidence and highlight the potential clinical relevance of combined therapy in the early management of bleeding trauma patients.
Interpretation of Hemodynamic Findings
Interestingly, we observed that patients in the TXA group presented with slightly higher SBP in the prehospital setting, but lower SBP upon ED admission compared with those who received transfusion alone. This paradox may be explained by several factors. First, patients identified by EMS as high-risk for hemorrhage may have received TXA early during the compensatory phase of shock, when catecholamine-driven vasoconstriction maintained SBP at relatively higher levels. However, as bleeding progressed during transport, these patients entered the decompensated phase, leading to lower SBP at ED arrival. Second, the selection bias inherent to clinical decision-making may have contributed: patients perceived as more severely injured were more likely to be prioritized for TXA, which could explain their greater hemodynamic deterioration by the time of ED assessment.
Reduction in Resuscitation Requirements and Mechanism
Another notable finding was that the TXA group required significantly less plasma and crystalloid resuscitation compared with the transfusion-only group. This aligns with the antifibrinolytic mechanism of TXA, which stabilizes clot formation and reduces ongoing blood loss, thereby lowering the need for adjunctive fluid replacement.12 Excessive crystalloid infusion is known to exacerbate coagulopathy and tissue edema, while large plasma volumes may contribute to transfusion-related complications.13 Therefore, by reducing the requirement for these interventions, TXA may indirectly improve patient outcomes and decrease secondary organ dysfunction.
Safety Profile: Thromboembolic Risk
Importantly, we found no increase in VTE events among patients treated with TXA, supporting the safety profile observed in prior trials and meta-analyses.14 Although concerns remain regarding potential thrombotic complications, the current evidence—including our study—suggests that TXA use in trauma is not associated with clinically significant elevations in thromboembolic risk.
Clinical Implications
This study has several clinical implications. First, our findings support the routine integration of TXA into prehospital trauma protocols, particularly in systems where blood transfusion can also be initiated before hospital arrival. Second, the reduction in MOF suggests that TXA not only improves survival but also reduces morbidity, which may have downstream benefits in resource utilization and long-term recovery. Third, given that the greatest benefit of TXA occurs when administered early, emphasis should be placed on timely recognition of hemorrhage risk by EMS providers and rapid delivery of TXA in the field.
Limitations
Nevertheless, several limitations must be acknowledged. First, this was a retrospective single-center study with a limited sample size, which may restrict the external validity of our findings. Future multicenter prospective studies with larger populations are warranted to confirm these results. Selection bias may have influenced treatment allocation, as patients perceived to be at higher risk of bleeding were more likely to receive TXA. Although multivariate Cox regression was performed to adjust for confounding factors, residual confounding cannot be excluded. In addition, our dataset did not capture detailed information on fibrinolytic activity or coagulation parameters, which could have provided mechanistic insight into the observed outcomes. Finally, VTE events may have been underdiagnosed due to the lack of systematic screening.
Conclusion
In summary, our study demonstrates that prehospital TXA administration in combination with blood transfusion is associated with reduced short-term mortality and decreased risk of multiple organ failure in trauma patients at risk for hemorrhage, without increasing thromboembolic complications. Importantly, these conclusions are based on clearly defined prehospital transfusion practices in specialized EMS units, transfusion of blood products (pRBCs and plasma) rather than crystalloids, and institutional criteria for initiating transfusion. These findings support the early integration of TXA into prehospital resuscitation protocols alongside blood transfusion, highlighting the importance of timely antifibrinolytic therapy in improving trauma outcomes.
Ethics Approval and Informed Consent
The study was approved by the institutional review board of The Fourth Affiliated Hospital of Soochow University (IRB No. 2017011). All procedures were conducted according to the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was waived by the Ethics Committee of The Fourth Affiliated Hospital of Soochow University due to the retrospective nature. Patient data confidentiality was strictly maintained, and all data were anonymized prior to analysis to protect participant privacy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Sawe HR, Mulwafu W, Chokotho L. et al. Fall injuries in sub-saharan Africa: analysis of prospective injury registry from 23 health facilities in Malawi and Tanzania. BMC Emerg Med. 2023;23(1):42. doi:10.1186/s12873-023-00805-x
2. Torres CM, Kent A, Scantling D, et al. Association of whole blood with survival among patients presenting with severe hemorrhage in us and Canadian adult civilian trauma centers. JAMA Surg. 2023;158(5):532–540. doi:10.1001/jamasurg.2022.6978
3. Wang H, Yang L. Applications of injectable hemostatic materials in wound healing: principles, strategies, performance requirements, and future perspectives. Theranostics. 2023;13(13):4615–4635. doi:10.7150/thno.86930
4. Feinberg GJ, Tillman AC, Paiva ML, et al. Maintaining a whole blood-centered transfusion improves survival in hemorrhagic resuscitation. J Trauma Acute Care Surg. 2024;96(5):749–756. doi:10.1097/TA.0000000000004222
5. Cho MS, Modi P, Sharma S. Transfusion-related acute lung injury. In: Statpearls. Treasure Island (FL) companies: Statpearls; 2025.
6. Goel R, Tobian AAR, Shaz BH. Noninfectious transfusion-associated adverse events and their mitigation strategies. Blood. 2019;133(17):1831–1839. doi:10.1182/blood-2018-10-833988
7. Cai J, Ribkoff J, Olson S, et al. The many roles of tranexamic acid: an overview of the clinical indications for txa in medical and surgical patients. Eur J Haematol. 2020;104(2):79–87. doi:10.1111/ejh.13348
8. Roberts I, Shakur H, Coats T, et al. The crash-2 trial: a randomised controlled trial and economic evaluation of the effects of tranexamic acid on death, vascular occlusive events and transfusion requirement in bleeding trauma patients. Health Technol Assess. 2013;17(10):1–79. doi:10.3310/hta17100
9. Cole E, Davenport R, Willett K, et al. Tranexamic acid use in severely injured civilian patients and the effects on outcomes: a prospective cohort study. Ann Surg. 2015;261(2):390–394. doi:10.1097/SLA.0000000000000717
10. Almuwallad A, Cole E, Ross J, et al. The impact of prehospital txa on mortality among bleeding trauma patients: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2021;90(5):901–907. doi:10.1097/TA.0000000000003120
11. Deeb AP, Hoteit L, Li S, et al. Prehospital synergy: tranexamic acid and blood transfusion in patients at risk for hemorrhage. J Trauma Acute Care Surg. 2022;93(1):52–58. doi:10.1097/TA.0000000000003620
12. Sawant S, Deshpande SV, Wamborikar H, et al. The impact of tranexamic acid on blood loss management in primary total knee arthroplasty: a comprehensive review. Cureus. 2024;16(7):e65386. doi:10.7759/cureus.65386
13. Chatrath V, Khetarpal R, Ahuja J. Fluid management in patients with trauma: restrictive versus liberal approach. J Anaesthesiol Clin Pharmacol. 2015;31(3):308–316. doi:10.4103/0970-9185.161664
14. Li Y, Tian M, Zhong W, et al. Prehospital tranexamic acid decreases early mortality in trauma patients: a systematic review and meta-analysis. Front Med (Lausanne). 2025;12:1552271. doi:10.3389/fmed.2025.1552271
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.