Back to Journals » International Medical Case Reports Journal » Volume 19
Pregnancy with Doubly Committed Subarterial Ventricular Septal Defect: Management Challenges and Delayed Maternal Risk Stratification
Authors Roseli A, Setiawan D, Cool CJ
Received 15 July 2025
Accepted for publication 20 January 2026
Published 3 February 2026 Volume 2026:19 553480
DOI https://doi.org/10.2147/IMCRJ.S553480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Anastasya Roseli,1 Dani Setiawan,1 Charlotte Johanna Cool2
1Department of Obstetrics and Gynecology, Faculty of Medicine, Padjadjaran University – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia; 2Department of Cardiology, Faculty of Medicine, Padjadjaran University – Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Anastasya Roseli, Email [email protected]
Introduction: Congenital heart disease is a leading cause of maternal morbidity and mortality during pregnancy, with ventricular septal defect (VSD) being one of the congenital anomalies that can lead to severe complications, especially if not managed continuously. The doubly committed subarterial (DCSA) subtype is particularly challenging in pregnancy due to risk of pulmonary hypertension and heart failure.
Case Presentation: A 29-year-old woman, G1P0A0, was referred at 38– 39 weeks of pregnancy with a diagnosis of VSD-DCSA subtype. The patient had progressive dyspnea since the seventh month of pregnancy and had a history of VSD since the age of 10, with treatment discontinued at age 15. Antenatal care was initially conducted by a midwife and referral to an obstetrician occurred after the onset of dyspnea. The patient received treatment from a cardiologist at District Hospital and was subsequently referred to Tertiary Hospital. Ultrasound examination revealed small gestational. NT-pro BNP was 194 pg/mL. Echocardiography confirmed a VSD-DCSA subtype and a high probability of pulmonary hypertension.
Management: The patient received bisoprolol 2.5 mg daily, furosemide 40 mg daily, and sildenafil 20 mg three times daily. The baby was delivered via cesarean section (CS) in with Apgar scores of 7 and 8 at 1 and 5 minutes. The patient was discharged in a stable condition.
Outcome: Postpartum follow-up showed stable hemodynamics and no dyspnea. The patient was referred for cardiology follow-up and long-acting reversible contraception.
Conclusion: Early maternal risk stratification and multidisciplinary care are essential to minimize complications in women with VSD. This case highlights the challenges of delayed referral and the importance of monitoring from the preconception through the postpartum period. The patient remained hemodynamically stable despite delayed referral, likely due to preserved cardiac function and timely medical intervention. A multidisciplinary approach involving obstetricians and cardiologists is essential to minimize risks to both mother and baby.
Keywords: ventricular septal defect, pulmonary hypertension, antenatal care
Background
Congenital heart disease (CHD) in women of reproductive age presents complex clinical considerations, especially during pregnancy.1,2 Cardiovascular disease is the leading cause of maternal morbidity and mortality in women with congenital heart disease.2 Ventricular septal defect (VSD) is one of the most common congenital anomaly, with the doubly committed subarterial (DCSA) type accounting for up to 30% of cases in Asia.3,4
VSD during pregnancy may lead to hemodynamic changes and complications due to physiological changes in the cardiovascular system.4–6 Ideally, maternal risk stratification is conducted in the preconception period using the modified World Health Organization (mWHO) classification to guide optimal. Continuous and comprehensive management of VSD is essential, considering its generally favorable prognosis. Multistage preparation including preconception, antenatal, intrapartum, and postpartum care is important to minimize complications.7,8
This case highlights the management challenges of late-presenting VSD-DCSA subtype in pregnancy, related complications, and suboptimal maternal risk stratification due to inadequate preconception care.
Case Presentation
A 29-year-old G1P0A0 woman was referred from a district hospital to a tertiary facility at 38–39 weeks of gestation with a diagnosis of VSD-DCSA subtype. She reported progressive dyspnea beginning at 7 months of gestation during exertion. She was previously diagnosed with VSD at age 10 and discontinued pediatric cardiology follow-up at 15 years old. There was no history of other chronic illnesses.
The patient’s lack of awareness regarding the potential risks associated with VSD resulted in the condition not being disclosed to the midwife during prenatal care. Throughout the pregnancy, the patient attended regular antenatal checkups with a midwife and was referred at 7 months gestation due to progressive dyspnea. Medical management was initiated in district hospital with bisoprolol 2.5 mg once daily, furosemide 40 mg once daily, and sildenafil 2.5 mg three times daily.
On admission, her blood pressure was 122/76 mmHg, heart rate 88 beat per minute, respiratory rate 22 times per minute and oxygen saturation 98%. The patient was classified as NYHA class II.
Figure 1 showed sinus rhythm with left-axis deviation and left ventricular hypertrophy. Echocardiography revealed a 10–12 mm VSD with a left-to-right shunt and high probability of pulmonary hypertension.
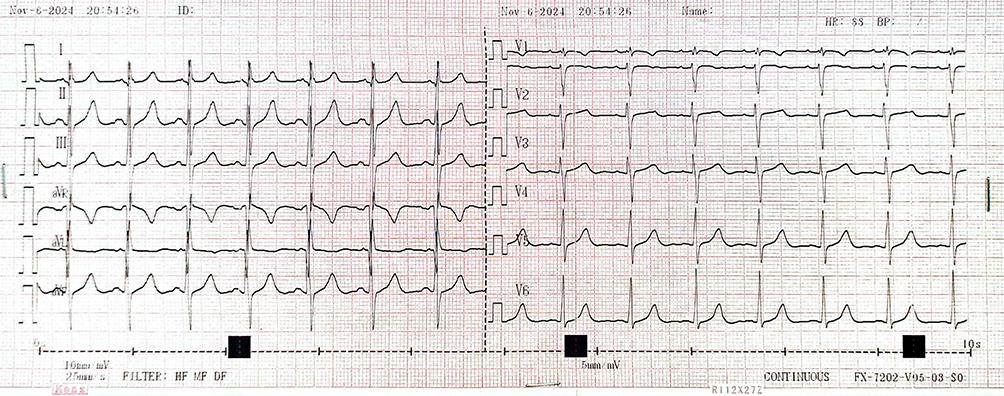 |
Figure 1 Electrocardiography Result. |
Figure 2 showed cardiotocography category I. Figure 3 showed fetal ultrasound revealed small for gestational age (SGA) findings. Laboratory tests showed elevated NT-proBNP levels at 194 pg/mL.
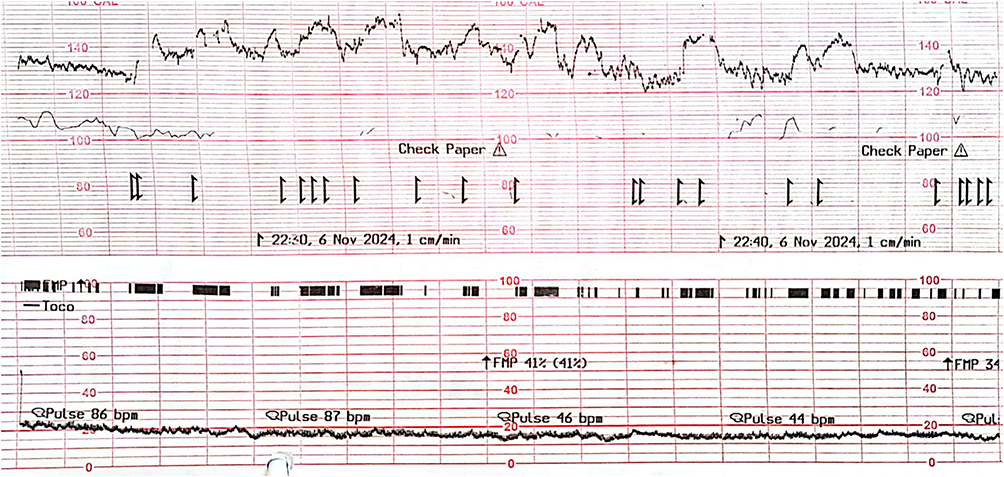 |
Figure 2 Fetal Cardiotocography Result. |
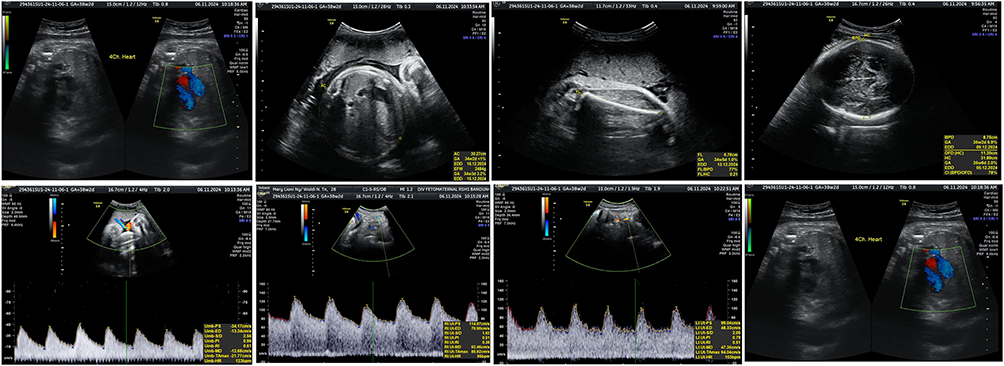 |
Figure 3 Ultrasonography Findings. |
Management
The patient underwent cesarean section and intrauterine device (IUD) insertion. A female infant was delivered weighing 2585 grams, length 48 cm, with APGAR scores of 7 at 1 minute and 8 at 5 minutes. The baby showed no signs of respiratory distress. In postpartum period, the mother remained hemodynamically stable and no complaint of dyspnea. She was managed with sildenafil 20 mg three times daily and discharged on postpartum day 2 with a referral for cardiology follow-up. After one year of follow-up, the patient was regularly monitored by a cardiologist and remained clinically stable without notable symptoms.
Discussion
The hemodynamic changes in VSD depend on the size of the defect, the pulmonary, and systemic vascular resistance. Large and persistent defect may lead to irreversible pulmonary vascular endothelial changes.4,5 Pregnancy induced physiological changes, particularly in the cardiovascular system, involve a 30–40% increase in cardiac output, peaking up to 75% during labor. In women with VSD, these changes can exacerbate disease progression and increase the risk of complications.6
Maternal and fetal risks and complications related to VSD are influenced by the nature of the cardiac lesion and any residual effects.8 Liu et al found that major adverse cardiac events (MACE) include arrhythmias (12.69%), heart failure (4.9%), and thromboembolic events (0.38%) such as stroke or pulmonary embolism. Other obstetric complications include pulmonary hypertension (26.6%), hemorrhage (13.17%), preeclampsia (6.54%), and gestational hypertension (2.21%). Fetal complications include prematurity (13.65%), low birth weight (8.56%), intrauterine growth restriction (1.15%), fetal distress (0.38%), fetal death (0.38%), and congenital malformations (0.19%).9
In this case, patient’s last cardiology visit occurred at age 15, with re-evaluation only initiated at age 29 during 7 months of pregnancy. Investigations included NT-proBNP measurement, electrocardiography, and echocardiography. The NT-proBNP level was elevated at 194 pg/mL. According to the American Heart Association, European Society of Cardiology, and the American Diabetes Association, elevated NT-proBNP is a marker to detect heart failure, with levels above 128 pg/mL at 20 weeks of pregnancy can be a predictive of adverse outcomes.10,11
Volume overload in chronic condition due to the defect may result in dilation of the right ventricle, pulmonary circulation, left atrium, and left ventricle, eventually causing systolic dysfunction and heart failure symptoms. This condition leads to increasing pulmonary vascular resistance.5 Electrocardiography revealed left ventricular hypertrophy and echocardiography confirmed left atrial and right ventricular dilation, concentric left ventricular hypertrophy, and increased tricuspid regurgitation velocity (TRVmax) to 3.6 meter/second and pulmonary artery systolic pressure (PASP) 62 mmHg—suggestive of high probability of pulmonary hypertension.
Fetal ultrasonography revealed a SGA fetus, likely related to maternal VSD. This finding aligns with Hardee et al, where small for gestational age is a common fetal complication in congenital heart disease. VSD patients has increased rates of SGA, respiratory distress, interventricular hemorrhage, and neonatal mortality (27.8%).8
Maternal risk stratification using the mWHO classification is ideally performed during preconception care, but in this case, was not feasible due to the late referral. The mWHO risk stratification system is one of the most accurate tools for assessing cardiovascular risk in pregnancy.10 Additional evaluations include electrocardiography, stress testing, echocardiography, and genetic counseling.8,10 The exercise stress test assesses functional capacity, targeting 80% of the predicted maximum heart rate.10 This test may reveal arrythmias in patient which had not been detected yet.1
This patient showed signs of high probability of pulmonary hypertension on echocardiography, ideally requiring right-heart catheterization—the gold standard for diagnosis. However, this procedure is typically avoided in third trimester due to risk for the mother and fetus. Therefore, accurate risk stratification was limited, impacting treatment decisions. However, despite the absence of routine cardiology follow-up during preconception and early antenatal period, the patient’s hemodynamic was stable. This may be attributed to a combination of compensatory cardiac mechanism and timely therapeutic intervention. The medical therapy during the third trimester, including beta blockers, diuretic, and pulmonary vasodilator may be contributed to preload and afterload which stabilizing hemodynamics prior to delivery.12,13 The absence of long-term follow-up and invasive hemodynamic assessment are study limitations.
Comprehensive, continuous care for VSD is essential due to the generally favorable prognosis. Preconception through postpartum planning helps mitigate complications, guided by mWHO classification.7,8 Preconception counseling should be individualized.10 Multidisciplinary approach involving obstetricians and cardiologists. It should evaluate the primary defect, surgical history, comorbidities, and any residual effects.1 Pregnant women in mWHO class III–IV should receive care in tertiary centers with monthly or more frequent visits if there is worsening condition.1,14
Delivery planning should begin at 28 weeks of pregnancy. Vaginal delivery is preferred for mWHO classes I–III, while cesarean section is recommended for mWHO class IV. In this case, cesarean section was indicated due to high probability of pulmonary hypertension and limited diagnostic options in late pregnancy.
The 24–48 hour postpartum period carries the highest risk due to a 60–80% increase in cardiac output.8 Hemodynamic changes may persist for 6–12 weeks postpartum, necessitating close monitoring. Long-acting non-hormonal contraception is recommended in women with septal heart defects.2
Conclusion
Early maternal risk stratification and multidisciplinary management are essential to reduce complications in women with congenital heart disease. This case illustrates that even with delayed referrals, appropriate intervention can prevent adverse outcomes. Strengthening preconception screening and referral pathways remains critical for optimal maternal and neonatal outcomes.
Ethical Approval
No formal ethical clearance was required for the publication of this case. The authors confirm that written informed consent for publication of this case report and any accompanying images were obtained from the patient and her spouse. The patient was informed in detail about the case content and agreed to its publication.
Consent for Publication
The patient provided written informed consent for publication of the case report and accompanying images.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Van Hagen IM, Roos-Hesselink JW. Pregnancy in congenital heart disease: risk prediction and counselling. Heart. 2020;106(23):1853–5. doi:10.1136/heartjnl-2019-314702
2. Lindley KJ, Bairey Merz CN, Asgar AW, et al. Management of women with congenital or inherited cardiovascular disease from pre-conception through pregnancy and postpartum: JACC focus seminar 2/5. J Am Coll Cardiol. 2021;77(14):1778–1798. doi:10.1016/j.jacc.2021.02.026
3. Kuswiyanto RB, Rahayuningsih SE, Apandi PR, Hilmanto D, Bashari MH. Transcatheter closure of doubly committed subarterial ventricular septal defect: early to one-year outcome. Int J Cardiol Congenit Hear Dis. 2021;2:100081.
4. Dakkak W, Alahmadi M, Oliver T. Ventricular septal defect. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
5. Lilly LS. Pathophysiology of Heart Disease: A Collaborative Project of Medical Students and Faculty. Lippincott Williams & Wilkins; 2012.
6. Kepley JM, Bates K, Mohiuddin SS. Physiology, maternal changes. In: StatPearls. StatPearls Publishing; 2023.
7. Yanagisawa Y, Goda A, Takeuchi S, et al. Successful management and risk stratification by exercise right heart catheterization before pregnancy in a patient with pulmonary arterial hypertension. CJC Open. 2023;5(4):312–314. doi:10.1016/j.cjco.2023.01.004
8. Canobbio MM, Warnes CA, Aboulhosn J, et al. Management of pregnancy in patients with complex congenital heart disease: a scientific statement for healthcare professionals from the American heart association. Circulation. 2017;135(8):50–87. doi:10.1161/CIR.0000000000000458
9. Liu Y, Li Y, Zhang J, et al. Pregnancy complications and outcomes among women with congenital heart disease in Beijing, China. Front Cardiovasc Med. 2022;8. doi:10.3389/fcvm.2021.765004
10. Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J. 2018;39(34):3165–3241. doi:10.1093/eurheartj/ehy340
11. Bayes‐Genis A, Docherty KF, Petrie MC, et al. Practical algorithms for early diagnosis of heart failure and heart stress using NT‐proBNP: a clinical consensus statement from the heart failure association of the ESC. Eur J Heart Fail. 2023;25(11):1891–1898. doi:10.1002/ejhf.3036
12. Delaney M, Matthews DC. Hemolytic disease of the fetus and newborn: managing the mother, fetus, and newborn. Hematol Am Soc Hematol Educ Progr. 2015;2015(1):146–151. doi:10.1182/asheducation-2015.1.146
13. Lammers AE, Diller GP, Lober R, et al. Maternal and neonatal complications in women with congenital heart disease: a nationwide analysis. Eur Heart J. 2021;42(41):4252–4260. doi:10.1093/eurheartj/ehab571
14. Kementerian Kesehatan Republik Indonesia. Buku KIA (Kesehatan Ibu dan Anak). Direktorat Jenderal Kesehatan Masyarakat. 2024.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.