Back to Journals » Patient Preference and Adherence » Volume 14
Preferences for Hearing Aid Attributes Among People with Moderate or Greater Hearing Loss in Rural China: A Discrete Choice Experiment
Authors Zhu D, Shi X, Nicholas S ![]() , Ye X, Chen S, He P
, Ye X, Chen S, He P
Received 5 February 2020
Accepted for publication 6 March 2020
Published 25 March 2020 Volume 2020:14 Pages 643—652
DOI https://doi.org/10.2147/PPA.S248522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Dawei Zhu,1 Xuefeng Shi,2,3 Stephen Nicholas,4– 7 Xin Ye,1,8 Siyuan Chen,1,8 Ping He1
1China Center for Health Development Studies, Peking University, Beijing 100191, People’s Republic of China; 2School of Management, Beijing University of Chinese Medicine, Beijing 100029, People’s Republic of China; 3National Institute of Chinese Medicine Development and Strategy, University of Chinese Medicine, Beijing 100029, People’s Republic of China; 4School of Economics and School of Management, Tianjin Normal University, Tianjin 300074, People’s Republic of China; 5Australian National Institute of Management and Commerce, Sydney, NSW 2015, Australia; 6Research Institute for International Strategies, Guangdong University of Foreign Studies, Guangzhou 510420, People’s Republic of China; 7Newcastle Business School, University of Newcastle, Newcastle, NSW 2308, Australia; 8School of Public Health, Peking University, Beijing 100191, People’s Republic of China
Correspondence: Ping He
China Center for Health Development Studies, Peking University, No. 38 Xueyuan Road, Haidian District, Beijing 100191, People’s Republic of China
Tel/Fax +861082805709
Email [email protected]
Purpose: Hearing loss has not received sufficient attention, especially in low- and middle-income countries where more than 80% of the people with hearing loss reside. Little is known about the preference for hearing aids among people with hearing loss in developing countries. The aim of this study is to elicit the preferences for hearing aid attributes among rural Chinese adults with moderate or greater hearing loss and examine how preferences vary across different individual socioeconomic characteristics.
Patients and Methods: We interviewed 125 adults in two rural counties in Shandong province in China. A discrete choice experiment (DCE) with eight attributes, comprising out-of-pocket (OOP) costs, hearing aid style, effective in quiet settings and noisy settings, feedback (whistling), connectivity, water/sweat resistance and battery life, were employed to examine participants’ preference for hearing aids. Mixed logit models were used for the statistical analyses.
Results: While OOP costs, effectiveness in quiet settings, water/sweat resistance and battery life were significantly associated with choosing a hearing aid, rural Chinese adults with moderate or greater hearing loss valued effectiveness in noisy settings above other attributes of hearing aids, followed closely by lack of feedback. The preference of the attributes of OOP costs, in the canal hearing aids, effectiveness in noisy settings, connectivity and battery life varied across individual socioeconomic characteristics including sex, marriage, employment, income and education level.
Conclusion: Our study supported the view that the development of noise suppression and feedback cancellation systems remained the main challenge for the hearing aid industry. Since OOP costs were also associated with choosing a hearing aid, the policy advice is to improve reimbursements from insurance schemes and/or reduce the costs of hearing aids.
Keywords: hearing aids, discrete choice experiment, hearing loss, rural China
Introduction
With the World Health Assembly’s resolution on the prevention of deafness and hearing loss and the Lancet Commission on hearing loss, hearing loss has recently received increased attention.1,2 Hearing loss (26 dB or greater hearing threshold) was the fourth global leading cause of years lived with a disability (YLDs) in 2015,3 and disabling hearing loss (hearing loss greater than 40 dB in the better hearing ear in adults) is the second leading cause of disability worldwide and in China.4,5 It is estimated that 466 million people worldwide – or over 5% of the world’s population – have disabling hearing loss.6 According to a 2014–2015 population-based survey in four Chinese provinces, the age standardized prevalence rate of hearing loss was 15.84%, and moderate to profound hearing loss was 5.17% of the population.7 The prevalence of hearing loss increases with age and thus will surge with a rapid aging in China and around the world.8 According to the World Health Organization (WHO) report, over 900 million people, or 10% of world’s population, will suffer from hearing loss by 2050.6
Since hearing loss is irreversible for most people, hearing aid fitting is the common intervention, or standard of care, to treat permanent hearing loss.9 Untreated hearing loss affects an individual’s physical and psychological health,10,11 and many of them suffered from isolation and stigma and experienced a greater prevalence of unemployment and negative health outcomes.3,11–13 Poor health outcomes associated with hearing loss include psychological illnesses and higher utilization of health services.3,10 Fitting hearing aids can increase an individual’s quality of life by increasing activities of daily living and instrumental activities of daily living and enhancing social interaction, and decrease economic burden by decreasing healthcare utilization.12–14
Despite its multiple benefits, uptake of hearing aids in adults is relatively low, even in countries where hearing aids are freely available.15,16 The prevalence of hearing aid use was only 6.5% among adults with hearing loss in Germany,16 which is close to that in China.17 It is estimated that the global production of hearing aids is less than 10% of the unmet need for hearing aids.18 Previous studies have investigated the demand for hearing aids from the perspective of both individuals and the product.19–21 Population-based studies on hearing aid use suggested that individual sociodemographic characteristics and the degree of hearing loss were associated with hearing aids use.17 Consumer preference studies identified performance, including effectiveness in noisy environments and quiet environments, as the most important attribute of hearing aids.20,21 However, most of these studies have been conducted in developed countries. In developing countries, where two-third people with moderate or greater hearing loss reside, accessibility to hearing aids is extremely low, especially in rural area.22 What is the preference for hearing aid use among people with hearing loss in rural China, the world’s largest developing county?
The main challenges of underuse of hearing aids in China are the lack of trained audiologists to provide rehabilitation, the absence of a supportive culture for hearing aid use and concern about the cost of hearing aid devices.23–25 In China, audiology is a relatively new profession, with only a 10 to 20-year history, and there are only about 1200 audiologists to provide audiological services, primarily located in urban areas.25 Chinese speakers do not seem to note a significant communication challenge until the hearing loss in the better ear reaches 40 dB HL or worse, and many Chinese older people view hearing loss as part of the aging process, which discourages any intervention.24 In China, there is almost no social insurance coverage for hearing aids, and patients pay out-of-pocket for hearing device.24,26 With the implementation of “Guidance on Medical Rehabilitation for the 13th Five-Year Plan (2016)” and “Healthy China Initiative 2019 to 2030”, investment in rehabilitation services is scheduled to increase dramatically, and knowledge of the factors that affect hearing aid preferences and willingness to pay (WTP) for hearing aids contributes to understanding these government initiatives.
Using discrete choice experiment (DCE), which is widely used in consumer preference studies, our study elicits the preferences for hearing aid attributes among rural Chinese adults with moderate or greater hearing loss and examines how preferences vary across individual socioeconomic characteristics. This study provides new information about individuals’ preferences and WTP for hearing aids in rural areas in China, providing a reference point for other developing countries that are also suffering from the heavy burden of hearing loss and low accessibility to hearing aids.
Materials and Methods
Sampling and Participants
Using a stratified random sampling method, we selected two rural counties, Yishui and Feixian, in Shandong province, which we divided into a high (Yishui) and low (Feixian) income county based on their GDP per capita. We conducted a face-to-face interview using questionnaires. Based on a list provided by the local Disabled Persons’ Federation, a government organization protecting the lawful rights and interests of all persons with disabilities in China, 100 rural residents with moderate or greater hearing loss in each county were randomly selected. Conducted in July 2019, 125 persons completed the survey with a response rate of 62.5%.
Discrete Choice Experiment
A discrete choice experiment (DCE) is a stated preference method that is widely used in health care to elicit preferences from participants without directly asking them to state their preferred options.27–29 The method assumes that individual decisions regarding a hearing aid can be determined by the attributes or characteristics of the product, such as the cost, effectiveness, style and feedback (whistling).28 These hearing aid attributes can be further specified by variants or levels of these attributes. For example, we specified the attribute of cost as RMB200 (USD29), RMB500 (USD71), RMB1000 (USD143). DCE presents participants with a reasonably straightforward task of making trade-offs between 2 or 3 competing hypothetical scenarios, each of which consists of a limited combination of these attributes/levels.30 The data from DCE can then be used to quantify the relative weights of the product attributes, which are the revealed individual utilities or values placed on each attribute/level.29 The DCE method also produces the choice probability, or the mean uptake, for the hearing aid and marginal rates of substitution across attributes.31 The DCE method can also be applied to obtain the WTP, or the maximum price a consumer will pay for a unit change in each non-monetary attribute of the hearing aid.31
Study Design
Based on previous studies20,21 and interviews with patients and experts, we selected eight hearing aid attributes and their levels. Table 1 sets out the attributes and levels for hearing aids. The eight most important attributes/levels comprised: (1) out-of-pocket (OOP) cost; (2) style of hearing aids; (3) effective in quiet settings; (4) effective in noisy settings; (5) feedback; (6) connectivity; (7) water/sweat resistance; and (8) battery life. Combining the eight attributes with each level results in 768 hypothetical hearing aids alternatives. Following the DCE method, we generated a sample of alternatives by using an orthogonal experimental design.27 Twenty-four choice questions were shown to sufficiently estimate all the main attributes.31 To avoid lower response rate and/or lower response reliability caused by presenting a single individual with a large amount of choice sets, we used a blocked design which divided the 24 choice sets into three different versions of the questionnaire containing 8 choice sets each.31 Each questionnaire started with a detailed description of the hearing aid attributes and their levels. The main part of each questionnaire comprised nine choice sets, with each question describing two alternative hearing aid scenarios in terms of the eight attributes and a no hearing aid option. Participants were then asked, “If you were actually offered the 2 hearing aids above, which would you prefer to choose?”. According to Johnson and Orme rule of thumb, our sample meets the requirement of the minimum sample size.32,33
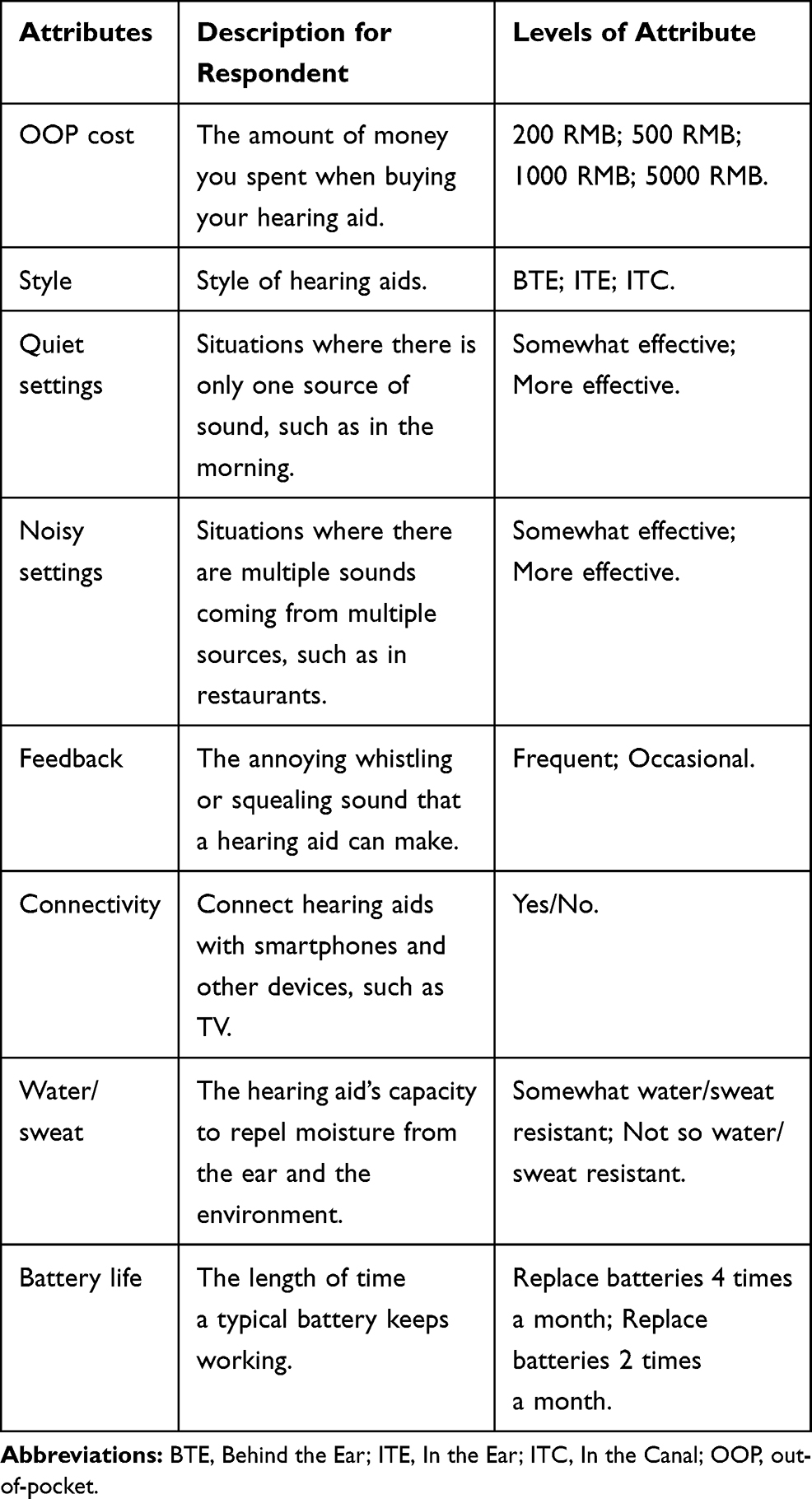 |
Table 1 Hearing Aid Attributes and Levels |
Non-DCE Variables
We collected information on participants’ sociodemographic characteristics and degrees of hearing loss. Sociodemographic variables consisted of sex (female or male), age (15–59 or 60 and above), spouse (yes or no), employment (employed or unemployed), income (RMB<10,000) or RMB≥10,000), education attainment (primary school or below or secondary school or higher) and social participation (0–1 or 2 and above). Social participation was measured by the number of engagements in leisure activities. Survey respondents were asked, “How many of 11 types of activities they participated in during the last month?”, which was a multiple choice question including 11 activities: (1) interacted with friends; (2) played Mahjong, chess, cards or went to a community club; (3) provided help to family, friends, or neighbors; (4) went to a sports, social, or other kind of club; (5) took part in a community-related organization; (6) performed volunteer or charity work; (7) cared for a sick or disabled adult; (8) attended an educational or training course; (9) made stock investments; (10) used the Internet; and (11) others, with a dichotomous 0–1 or 2 and above social participation variable formed. The degree of hearing loss was assessed by pure tone audiometry, which was conducted in quiet rooms (ambient noise≤30 dBA) by a professional audiometric technician. According to the recommendation by the China’s Disabled Persons’ Federation and WHO criteria, both ears were tested separately at 0.5, 1, 2, and 4 kHz to obtain the hearing threshold on each frequency point.22 Pure tone threshold averages in the better ear were calculated and formed into moderate to severe hearing loss (41–80 dB) or profound hearing loss (greater than 80 dB) dichotomous variable.34
Statistical Analyses
Descriptive statistics were used to analyze the non-DCE variables. We used a mixed logit model, with 500 Halton draws with normally distributed parameters, to estimate participants’ preferences for hearing aid attributes. The mixed logit model allowed for attribute coefficients to be randomly distributed, and improves the fit of the model significantly over conditional logit modelling.35 Each estimated coefficient is a preference weight and represents the relative contribution of the attribute level to the utility that respondents assign to an alternative. The monetary value for the hearing aid attributes, except the cost attribute, was calculated by the ratios between the coefficients of the out-of-pocket costs with the coefficients of the other hearing aid attributes (such as style of hearing aids, effective in quiet settings, feedback, and so on).31 Following previous studies, we also estimated the changes in the probability of individuals choosing a hearing aid with specified attributes.31,36,37 These predictions are useful to policy-makers as they show the predicted impact of alternative levels of hearing aid attributes on individuals’ preferences. We employed a set of models which included interaction between individuals’ characteristics (including sex, age group, marital status, employment status, income, education attainment, social participation and the degree of hearing loss) and all attributes of the hearing aids to estimate the potential difference in preference between groups of individuals.
A p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed in STATA 15 (Stata Corp, College Station, TX, USA).
Results
Characteristics of Participants
As shown in Table 2, 61.6% of participants were male, 52.8% were 60 years or above, 71.2% had a spouse, and 37.6% were unemployed. More than a half (54.4%) had household income above RMB10000; 37.6% had a secondary school diploma or higher; 46.4% of participants reported they engaged in less than two types of social activities during the last month; and 38.4% of the sample had hearing loss equal to or greater than 81 dB.
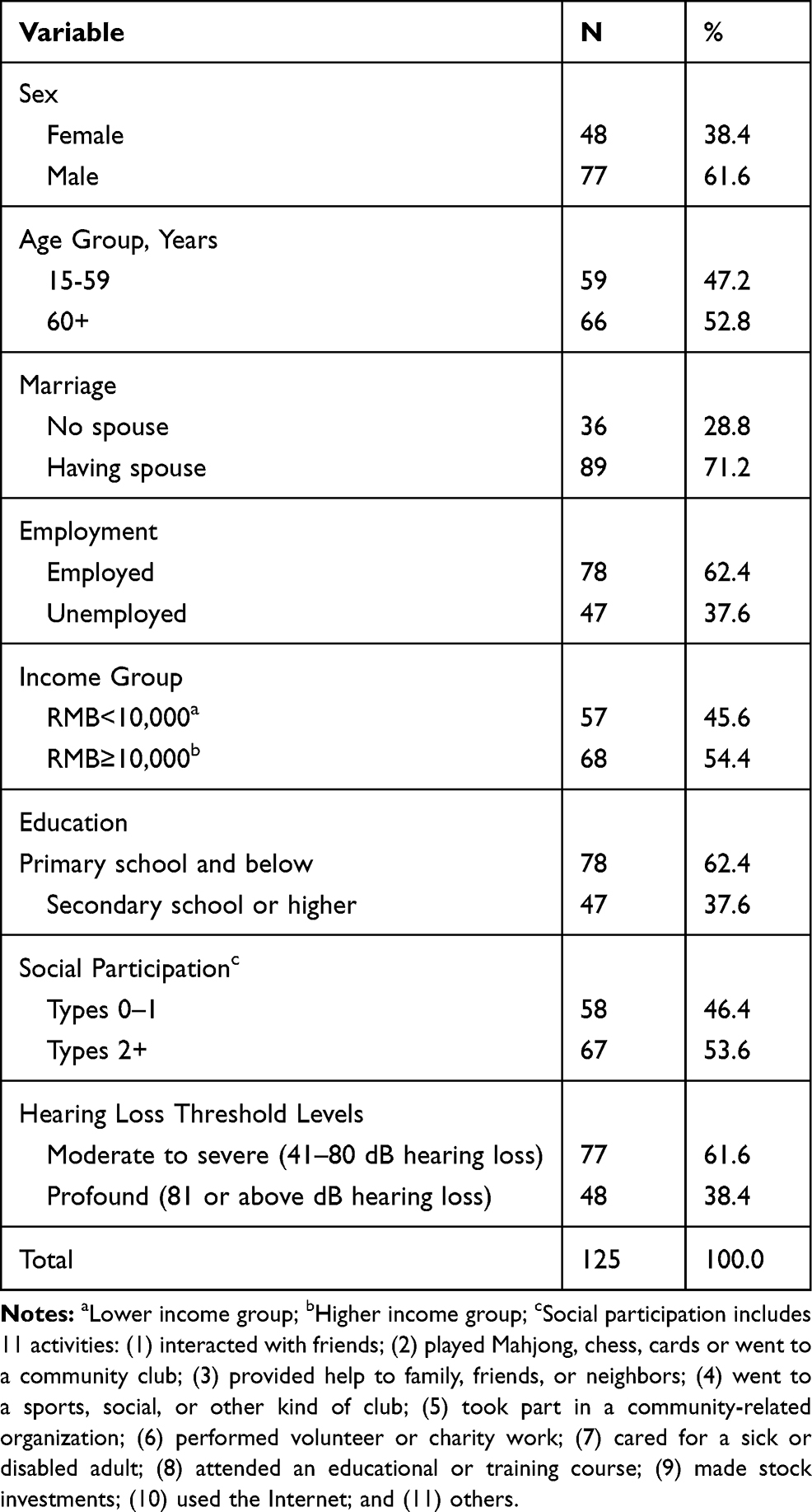 |
Table 2 Participant Characteristics |
General Preference for Hearing Aids
Table 3 shows the discrete choice model results for the general preferences for hearing aid attributes. The option of no hearing aid was chosen in 15% of the choice sets. Except style and connectivity, other attributes of hearing aids influenced individuals’ preferences for hearing aid attributes (p < 0.05). The attribute with the greatest magnitude of association with hearing aid preference was effectiveness of hearing aid in noisy settings, followed by lack of feedback and effectiveness in quiet settings. As expected, subjects showed a negative preference for OOP costs.
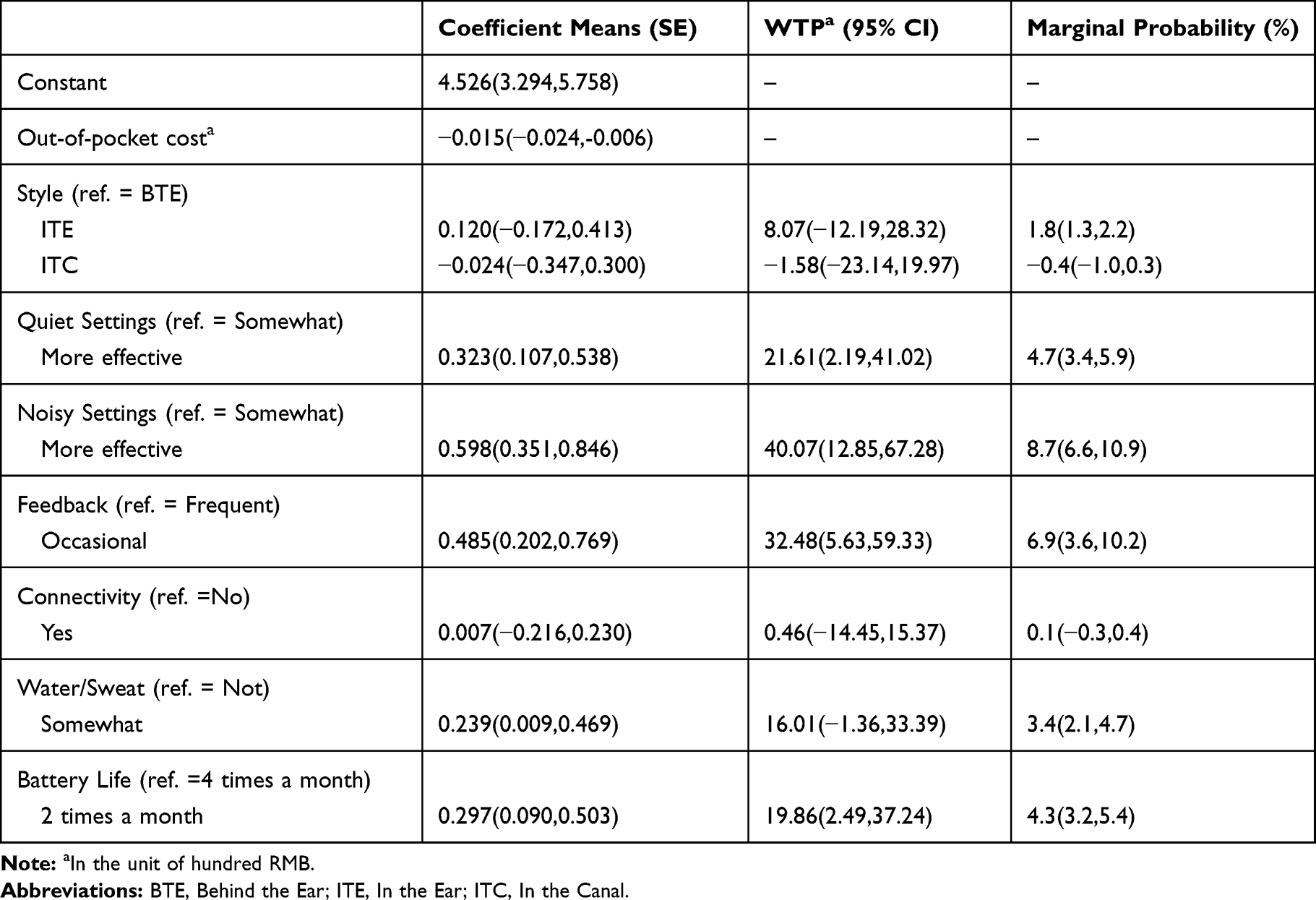 |
Table 3 General Results for a Discrete Choice Experiment Addressing Preferences for Hearing Aid Attributes |
The estimated mean WTP for hearing aid attributes are shown in the third column of Table 3. On average, individuals were willing to spend RMB4000 (USD571) in obtaining a hearing aid with more effectiveness in noisy settings than one with somewhat effectiveness. WTP for occasional feedback instead of frequent feedback was RMB3200 (USD457). Participants were willing to pay roughly RMB2000 (USD286) to get a hearing aid with more effectiveness in a quiet setting or with a longer battery life than one with somewhat effectiveness or a shorter battery life. WTP for somewhat water/sweat resistance instead of no water/sweat resistance was RMB1600 (USD229). An increase in effectiveness in noisy settings had a relatively large (8.7%) impact on the expected uptake and a decrease in frequency of feedback had a 6.9% impact on uptake.
Difference in Preference for Hearing Aids
Table 4 presents the results of eight interaction models. Male, higher income or higher education individuals showed a greater preference for effectiveness in noisy settings than female, lower income or lower education individuals. OOP costs were more important to individuals who had a spouse or were unemployed than those with no spouse or employed, and less important to individuals who have more social activities than less social actives. In the canal (ITC) hearing aids were more important in the higher education group than lower education group, and less important in the profound hearing loss group than the moderate hearing loss group. Individuals with a spouse also showed higher preference for connectivity than individuals without a spouse. Battery life was less important in the higher education group.
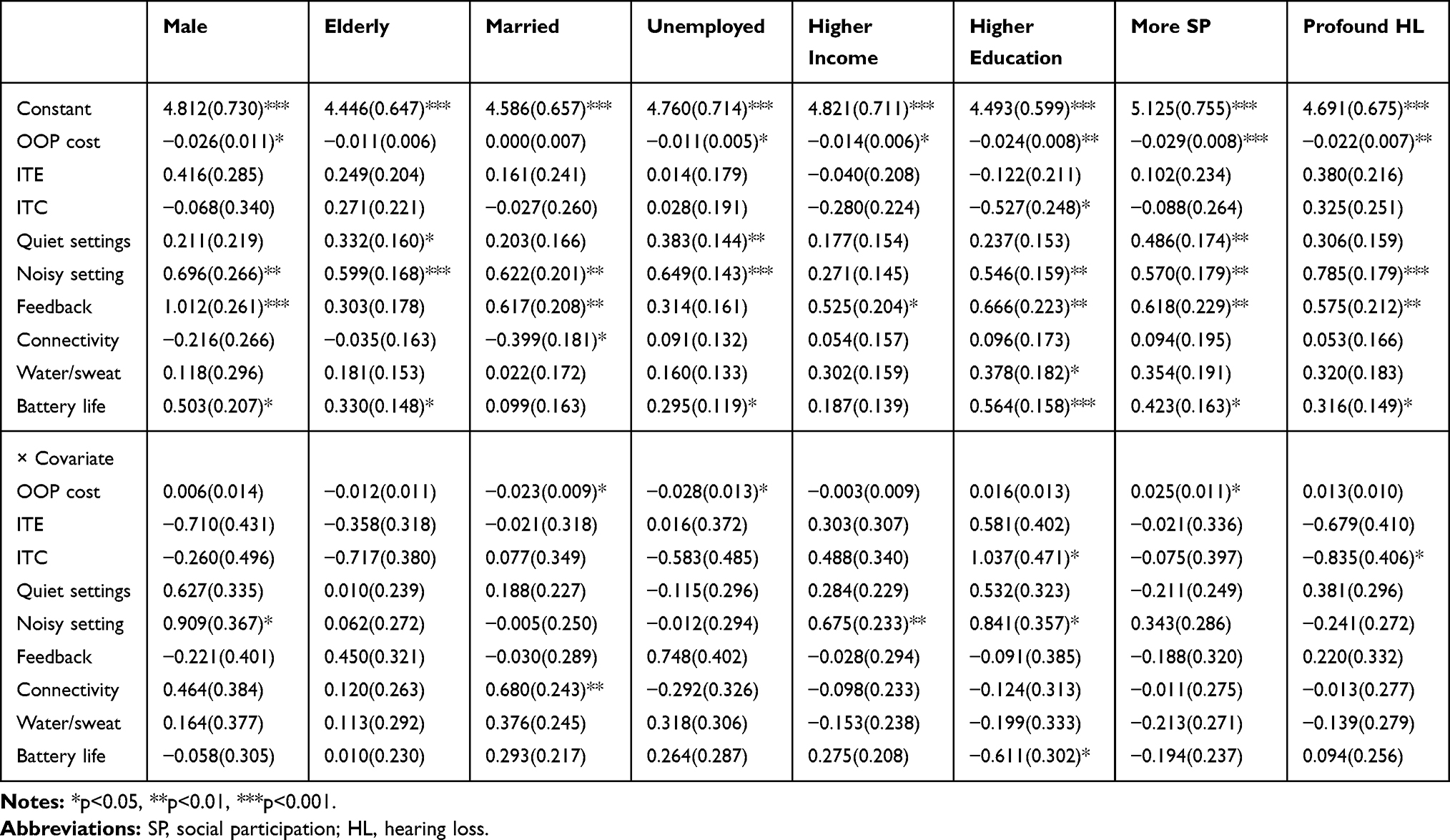 |
Table 4 Results with Interactions for Preferences for Hearing Aid Attributes |
Discussion
Our study used discrete choice experience to investigate the preferences for hearing aid attributes and their variations across individual characteristics for people with moderate or greater hearing loss. While OOP costs, effective in quiet settings, water/sweat resistance, and battery life were all significantly associated with choosing a hearing aid, our rural adults with moderate or greater hearing loss valued effectiveness in noisy settings above other attributes of hearing aids, followed closely by lack of feedback. OOP costs, ITC, effectiveness in noisy settings, connectivity and battery life showed significant differences across individual characteristics, except the age group.
Almost half of the total utility of the hearing aids could be ascribed to their effectiveness, particularly in noisy settings. Our result showed that individuals valued the effectiveness of hearing aids in noisy settings as the most important attribute, which is consistent with previous studies in the US and Germany.20,21 Another feature of hearing aids, effectiveness in quiet settings, was ranked as the third most important factor in our study, but its contribution was only half of improved effectiveness in noisy settings. Existing studies have not yet reached a consensus on the relative importance of hearing aid effectiveness in quiet settings. A US study showed that the utility change from improved effectiveness in quiet settings was only one-third of the utility change of improved effectiveness in noisy settings which is close to our result,21 but quiet-noisy settings were almost equal in German research.20 The differences with the German results may be due to the different sociodemographic characteristics of the samples.
As expected, cost is also an important attribute of hearing aids in our sample. The effect of RMB4000 (USD571) reduction in cost, which is about one-third of annual consumption expenditure per capita in rural residents, was almost equal to the trade-off between more effective and somewhat effective hearing devices in a noisy setting. This means that theoretically, a RMB4000 (USD571) reduction in cost only increased hearing aid uptake by 8.7%. This implies that if a hearing aid with a price of RMB4000 (USD571) was provided free of charge, the uptake would only see a small increase. This finding fits well with those of previous studies that found the uptake of hearing aids was very low in countries where public funds are used to pay for them.38 In addition, our participants were willing to pay less for hearing aids than respondents in the Bridges et al sample.21 For example, individuals in our sample were willing to trade-off RMB4000 (USD571) in obtaining a hearing aid with more effectiveness in noisy settings than one with somewhat effectiveness, compared to RMB63000 (USD9000) trade-off in Bridges et al study. This may be due to the difference in the populations sampled, where the Bridges study sampled primarily wealthy, educated individuals whereas this study focused on rural residents with lower levels of education.
In our study, feedback and water/sweat resistance were all significantly associated with choosing a hearing aid, which is also consistent with previous studies.20,21 However, there are some differences in the relative rankings of each attribute. Participants valued lack of feedback more than water resistance, which is contrary to prior findings.21 In our sample, participants had greater degree of hearing loss than US respondents in Bridges et al’s research, which means our participants required greater hearing aid gain. However, products with higher gain control settings are more likely to experience feedback,39,40 so subjects with greater degree of hearing loss may care more about feedback than one with somewhat less effectiveness.
Battery life was an important attribute in our study while it was not a significant predictor in previous studies.21 Since hearing aid batteries are not a common battery type in China and the uptake of hearing aids tends to be very low in rural areas, hearing aid batteries are not readily available in most areas of rural China, and had to be ordered online or from a distant hearing aid store. In addition, replacing the battery is a relatively complex operation since its small size makes it difficult to operate, especially for older persons or patients with physical problems.24 Further, batteries are the ongoing cost after paying for the hearing aid itself. For these reasons, rural individuals in China may weigh more on battery life compared to people living in urban areas or more developed countries. We also found that the style and connectivity were not significantly associated with choosing a hearing aid. All our participants had greater degree of hearing loss which needed high-gain hearing aids. Neither the style of in the ear (ITE) or ITC could easily meet this need. Compared with the Western literature, elderly Chinese had fewer cosmetic concerns about hearing aids,23 which may reflect cultural differences between China and other countries. In addition, behind the ear (BTE) hearing aids have become smaller and decreased their visibility in recent years,40 which may influence the attractiveness of ITE or ITC devices. Since rural residents usually had less demand for connections with smartphones and other devices, they were less concerned about connectivity.41
To investigate how preferences may be affected by participants’ characteristics, we analyzed interactions between individual characteristics and hearing aids attributes. We found that male, higher income and higher educated participants cared more about hearing aid effectiveness in noisy settings. This is likely attributable to the different communication behaviors of these participants in numerous different noisy surroundings.20 Unemployed participants cared more about the hearing aid cost while unmarried or people with more social participations were less concerned about cost. Unemployed participants were likely to have a lower capacity to pay compared to employed participants. Previous research found that unmarried respondents have more intention to fit a hearing aid due to their desire to find a partner,42 and participants with more social activities may have high demand for hearing aids than those with lower social interactions.
Individuals in the higher education subgroup valued the battery life less than others, probably because they were more likely to have higher accessibility to battery charging facilities. Participants with a spouse viewed connectivity more important than those without a spouse, which may be due to Chinese married couples spending more time watching TV.43 In addition, participants in the higher education subgroup value ITC more than those in the low education group; and participants in the profound subgroup valued ITC less than other users. The size and style of the hearing aid had an influence on effectiveness, as well as the stigma, of wearing a hearing aid.44,45 The more visible the hearing aid, the more stigma, and the less visible, such as ITC hearing aids, the less effective.46 In our sample, the higher education subgroup cared more about stigma, and the profound hearing loss subgroup cared more about effectiveness.
Our study has several limitations. First, we selected the most relevant attributes based on the literature and interviews with experts in the field of hearing aids, which is unable to include all attributes of hearing aid preferences. Second, our sample only contained participants with moderate or greater hearing loss in one rural area of China with a relatively small sample size, so the generalization of our findings needs to be confirmed by further studies, especially testing for different geographical, social and economic characteristics. Third, we did not consider the effect of knowledge of hearing aid attributes on the preference for hearing aids although we analyzed whether the preferences differ between different levels of socioeconomic status.
Despite these limitations, our study has several strengths. We believe this is the first study to estimate individuals’ preferences for hearing aid attributes in rural areas of a developing country with low hearing aid accessibility. We also provide new information about individuals’ preferences and WTP for hearing aids. Our findings verified that the low acquisition rate of hearing aids cannot simply be explained by the cost factors, but was determined by more complex decision-making process, particularly weight on hearing aid performance. Although the findings may be limited by the study’s location and sample size, a direct policy implication is the priority of providing high-performance hearing aids with long battery life and low OOP cost, which will increase the uptake of hearing aids in rural China. Development of sufficient noise suppression and feedback cancellation systems are still the main technical challenges for the hearing aid industry. If the government or health insurance schedule could reimburse a larger proportion of the OOP costs of hearing aids or reduce the cost of hearing aids, there would be an improved rate of hearing aid purchase in rural China. In addition, improving the appearance and connectivity of hearing aids would increase the uptake of hearing aids among some specific subgroups.
Conclusions
Our findings support the fact that the effectiveness of hearing aids in noisy settings was the most important attribute in the preference for hearing aid attributes among individuals with moderate or greater hearing loss in rural China, followed by feedback, effectiveness in quiet settings, battery life, and water/sweat resistance. OOP cost was significantly associated with choosing a hearing aid. In addition, preferences and WTP for hearing aids were influenced by sex, marital status, employment, income, education, social participation and the severity of hearing loss.
Abbreviations
YLDs, years lived with a disability; WHO, World Health Organization; WTP, willingness to pay; DCE, discrete choice experimentation; ITE, in the ear; ITC, in the canal; OOP, out-of-pocket.
Data Sharing Statement
The raw data (transcripts) of this study cannot be shared, to maintain participant privacy. Summary data are available from the corresponding author on reasonable request.
Ethics and Consent Statement
The study was approved by the Ethics Committee of Peking University (No. IRB00001052-19046). Participants’ informed written consent was obtained for the study contents, purposes, protocols, data confidentiality and anonymity procedures, and participants’ freedom to discontinue the study at any stage was explained and consent agreed.
Author Contributions
Dawei Zhu: study design, field investigation, data analysis, and drafting the manuscript. Xin Ye, Siyuan Chen and Xuefeng Shi: participating the study design, field investigation and revising the manuscript. Stephen Nicholas: revising the manuscript and contributing the language editing of the manuscript. Ping He: study concept and design, critical revision of the manuscript, and supervising all aspects of the work. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by National Natural Science Foundation of China (No.71874005) and the Peking University’s Start-up Fund (No. BMU2018YJ004). The study sponsor has no role in study design, data analysis and interpretation of data, the writing of manuscript, or the decision to submit the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHA.70.13. World Health Assembly resolution on prevention of deafness and hearing loss. Resolutions and decisions, annexes. Geneva: Seventieth World Health Assembly; May 31, 2017. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA70/A70_R13-en.pdf?ua=1&ua=1.
2. Wilson BS, Tucci DL, O’Donoghue GM, Merson MH, Frankish H. A Lancet Commission to address the global burden of hearing loss. Lancet. 2019;393(10186):2106–2108. doi:10.1016/S0140-6736(19)30484-2
3. Wilson BS, Tucci DL, Merson MH, O’donoghue GM. Global hearing health care: new findings and perspectives. Lancet. 2017;390(10111):2503–2515. doi:10.1016/S0140-6736(17)31073-5
4. Zheng X, Zhang L, Chen G, Pei L. Prevalence of visual, hearing, speech, physical, intellectual and mental disabilities in China, 2006. Chin J Epidemiol. 2008;29(7):634–638.
5. World Health Organization, World bank. World Report on Disability. Geneva: WHO; 2011.
6. World Health Organization. Deafness and hearing loss. Deafness and hearing loss. 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss.
7. Hu X, Zheng X, Ma F, Long M. Prevalence of hearing disorders in China: a population-based survey in four provinces of China. Chin J Otorhinolaryngol Head Neck Surg. 2016;51(11):819–825. doi:10.3760/cma.j.issn.1673-0860.2016.11.004
8. Stevens G, Flaxman S, Brunskill E, Mascarenhas M, Mathers CD, Finucane M. Global and regional hearing impairment prevalence: an analysis of 42 studies in 29 countries. Eur J Public Health. 2013;23(1):146–152. doi:10.1093/eurpub/ckr176
9. Arlinger S. Negative consequences of uncorrected hearing loss-a review. Int J Audiol. 2003;42:2S17–2S20. doi:10.3109/14992020309074639
10. Genther DJ, Frick KD, Chen D, Betz J, Lin FR. Association of hearing loss with hospitalization and burden of disease in older adults. JAMA. 2013;309(22):2322. doi:10.1001/jama.2013.5912
11. West JS. Hearing impairment, social support, and depressive symptoms among U.S. adults: a test of the stress process paradigm. Soc Sci Med. 2017;192:94–101. doi:10.1016/j.socscimed.2017.09.031
12. Dawes P, Cruickshanks KJ, Fischer ME, Klein BEK, Klein R, Nondahl DM. Hearing-aid use and long-term health outcomes: hearing handicap, mental health, social engagement, cognitive function, physical health, and mortality. Int J Audiol. 2015;54(11):838–844. doi:10.3109/14992027.2015.1059503
13. Willink A, Reed NS, Lin FR. Cost-benefit analysis of hearing care services: what is it worth to medicare?: hearing care for medicare beneficiaries. J Am Geriatr Soc. 2019;67(4):784–789. doi:10.1111/jgs.15757
14. Barton GR, Bankart J, Davis AC, Summerfield QA. Comparing utility scores before and after hearing-aid provision: results according to the EQ-5D, HUI3 and SF-6D. Appl Health Econ Health Policy. 2004;3(2):103–105. doi:10.2165/00148365-200403020-00006
15. Barker F, Mackenzie E, Elliott L, Jones S, de Lusignan S. Interventions to improve hearing aid use in adult auditory rehabilitation. Cochrane ENT Group, ed. Cochrane Database Syst Rev. 2016. doi:10.1002/14651858.CD010342.pub3
16. Löhler J, Walther LE, Hansen F, et al. The prevalence of hearing loss and use of hearing aids among adults in Germany: a systematic review. Eur Arch Otorhinolaryngol. 2019;276(4):945–956. doi:10.1007/s00405-019-05312-z
17. He P, Wen X, Hu X, et al. Hearing aid acquisition in Chinese older adults with hearing loss. Am J Public Health. 2018;108(2):241–247. doi:10.2105/AJPH.2017.304165
18. The Lancet. Hearing loss: an important global health concern. Lancet. 2016;387(10036):2351. doi:10.1016/S0140-6736(16)30777-2
19. Vestergaard Knudsen L, Öberg M, Nielsen C, Naylor G, Kramer SE. Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: a review of the literature. Trends Amplif. 2010;14(3):127–154. doi:10.1177/1084713810385712
20. Meister H, Lausberg I, Walger M, von Wedel H. Using conjoint analysis to examine the importance of hearing aid attributes. Ear Hear. 2001;22(2):142–150. doi:10.1097/00003446-200104000-00007
21. Bridges JFP, Lataille AT, Buttorff C, White S, Niparko JK. Consumer preferences for hearing aid attributes: a comparison of rating and conjoint analysis methods. Trends Amplif. 2012;16(1):40–48. doi:10.1177/1084713811434617
22. World Health Organization. Facts about deafness. Facts about deafness. 2019. Available from: http://www.who.int/deafness/facts/en/.
23. Wong LLN, McPherson M. Universal hearing health care: where do audiology and hearing aids fit? ASHA Leader. 2008;13(17):14–18. doi:10.1044/leader.WB2.13172008.14
24. Ji F, Chen A-T, Wang Q-J. Hearing loss in the aged: status and interventions in China. Hear Balance Commun. 2015;13(2):51–57. doi:10.3109/21695717.2015.1032719
25. Zhao F, Manchaiah V, St. Claire L, et al. Exploring the influence of culture on hearing help-seeking and hearing-aid uptake. Int J Audiol. 2015;54(7):435–443. doi:10.3109/14992027.2015.1005848
26. Yong M, Willink A, McMahon C, et al. Access to adults’ hearing aids: policies and technologies used in eight countries. Bull World Health Organ. 2019;97(10):699–710. doi:10.2471/BLT.18.228676
27. Mangham LJ, Hanson K, McPake B. How to do (or not to do) … Designing a discrete choice experiment for application in a low-income country. Health Policy Plan. 2009;24(2):151–158. doi:10.1093/heapol/czn047
28. Ryan M. Discrete choice experiments in health care. BMJ. 2004;328(7436):360–361. doi:10.1136/bmj.328.7436.360
29. Ryan M, Bate A, Eastmond CJ, Ludbrook A. Use of discrete choice experiments to elicit preferences. Qual Saf Health Care. 2001;10(Supplement 1):i55–i60. doi:10.1136/qhc.0100055
30. Ryan M, Gerard K, Amaya-amaya M, eds. Using Discrete Choice Experiments to Value Health and Health Care. Dordrecht: Springer; 2008.
31. Hensher DA, Rose JM, Greene WH. Applied Choice Analysis: A Primer. Cambridge; New York: Cambridge University Press; 2005.
32. Johnson R, Orme B Getting the most from CBC. Sawtooth Software Research Paper. 2003.
33. de Bekker-grob EW, Donkers B, Jonker MF, Stolk EA. Sample size requirements for discrete-choice experiments in healthcare: a practical guide. Patient. 2015;8(5):373–384. doi:10.1007/s40271-015-0118-z
34. World Health Organization. International classification of functioning, disability and health (ICF). Available from: http://www.who.int/classifications/icf/en/.
35. Hole AR, Kolstad JR. Mixed logit estimation of willingness to pay distributions: a comparison of models in preference and WTP space using data from a health-related choice experiment. Empir Econ. 2012;42(2):445–469. doi:10.1007/s00181-011-0500-1
36. de Bekker-grob EW, Hofman R, Donkers B, et al. Girls’ preferences for HPV vaccination: A discrete choice experiment. Vaccine. 2010;28(41):6692–6697. doi:10.1016/j.vaccine.2010.08.001
37. Brown DS, Johnson FR, Poulos C, Messonnier ML. Mothers’ preferences and willingness to pay for vaccinating daughters against human papillomavirus. Vaccine. 2010;28(7):1702–1708. doi:10.1016/j.vaccine.2009.12.024
38. Smith J, Mitchell P, Wang J, Leeder S. A health policy for hearing impairment in older Australians: what should it include? Aust N Z Health Policy. 2005;2(1):31. doi:10.1186/1743-8462-2-31
39. Agnew J. Acoustic feedback and other audible artifacts in hearing aids. Trends Amplif. 1996;1(2):45–82. doi:10.1177/108471389600100202
40. Almufarrij I, Munro KJ, Dawes P, Stone MA, Dillon H. Direct-to-consumer hearing devices: capabilities, costs, and cosmetics. Trends Hear. 2019;23:2331216519858301. doi:10.1177/2331216519858301
41. Liu X. Analysis of the demand for internet consumption among rural residents in China. J Commercial Econ. 2013;17:31–32.
42. Fu J. The research on the attitude and the influence factors of the hearing aids for 16-59 year old persons with hearing disability; 2015.
43. Zhou X. Study of the status and influencing factors of entertainment and television programs in China; 2011.
44. Wallhagen MI. The stigma of hearing loss. Gerontologist. 2010;50(1):66–75. doi:10.1093/geront/gnp107
45. Erler SF, Garstecki DC. Hearing loss- and hearing aid-related stigma: perceptions of women with age-normal hearing. Am J Audiol. 2002;11(2):83–91. doi:10.1044/1059-0889(2002/020)
46. Strange A, Johnson A, Ryan B-J, Yonovitz A. The stigma of wearing hearing aids in an adolescent aboriginal population. Aust N Z J Audiol. 2008;30(1):19–37. doi:10.1375/audi.30.1.19
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.