Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Predisposition of functional genetic variants of A-kinase anchoring protein 10 toward acquired repolarization disorders in high-risk vascular surgery patients
Authors Biernawska J, Solek-Pastuszka J ![]() , Kazimierczak A
, Kazimierczak A ![]() , Safranow K
, Safranow K ![]() , Kaczmarczyk M, Zegan-Baranska M
, Kaczmarczyk M, Zegan-Baranska M ![]() , Zukowski M, Kotfis K
, Zukowski M, Kotfis K ![]()
Received 2 March 2018
Accepted for publication 11 May 2018
Published 26 July 2018 Volume 2018:14 Pages 1315—1322
DOI https://doi.org/10.2147/TCRM.S167086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Jowita Biernawska,1 Joanna Solek-Pastuszka,1 Arkadiusz Kazimierczak,2 Krzysztof Safranow,3 Mariusz Kaczmarczyk,4 Malgorzata Zegan-Baranska,5 Maciej Zukowski,5 Katarzyna Kotfis5
1Department of Anesthesiology and Intensive Therapy, Pomeranian Medical University, Szczecin, Poland; 2Department of Angiology and Vascular Surgery, Pomeranian Medical University, Szczecin, Poland; 3Department of Biochemistry and Medical Chemistry, Pomeranian Medical University, Szczecin, Poland; 4Department of Clinical and Molecular Biochemistry, Pomeranian Medical University, Szczecin, Poland; 5Department of Anesthesiology, Intensive Therapy and Acute Intoxications, Pomeranian Medical University, Szczecin, Poland
Purpose: We aimed at assessing the predisposition of A-kinase anchoring protein 10 (AKAP10) polymorphism toward acquired repolarization disorders in high-risk vascular surgery patients.
Patients and methods: One hundred adult patients (age =44–85 years), scheduled for an elective high-risk “open” vascular surgery procedure, were recruited. The electrocardiogram Holter monitor was used to assess repolarization stability from the beginning of the operation up to 24 hours afterward. The AKAP10 gene rs203462 polymorphism and cardiac complications were analyzed.
Results: Repolarization disturbances defined as QT interval duration corrected for heart rate (QTc) interval prolongation >500 ms and QTc interval dispersion >65 ms were recorded in 46 patients. A model of multivariate logistic regression showed that only the presence of allele G of the AKAP10 polymorphism was an independent risk factor for repolarization disturbances in the perioperative period (odds ratio =14.35; 95% CI =4.65–44.23; p<0.0001).
Conclusion: When the acquired QTc interval prolongation or QTc dispersion is associated with AKAP10 polymorphism, it may remain clinically silent.
Keywords: AKAP10, repolarization, vascular surgery, QTc, Holter
Introduction
Many vascular surgery procedures are performed in high-risk patients every day. The incidence of cardiac complications and death after vascular surgery remains relatively high despite advanced perioperative monitoring and improvement in therapeutic management.1–3 The assessment of dynamic changes of ventricular repolarization derangement may be a useful tool for predicting postoperative cardiac complications. Ventricular repolarization analysis using QT interval dispersion and QT interval duration corrected for heart rate (QTc) with a 12-lead electrocardiogram (ECG) or a Holter is rarely used in everyday practice. The relationship between intraoperative repolarization disturbances and clinical significance has not yet been studied in the vascular surgery patients.
The clinical manifestation of acquired repolarization disturbances may be quite variable: from clinically asymptomatic electrocardiographic abnormalities (clinically concealed QT interval prolongation) through ventricular ectopic beats, monomorphic or polymorphic ventricular tachycardia (such as torsade de pointes), and ventricular fibrillation to a sudden arrhythmic cardiac death.4–6 Acquired repolarization disturbances may be associated with patient and/or procedure. They could be caused by ischemia, electrolyte disturbances, metabolic or endocrine disorders, adrenergic stimulation, drug side effects, or genetic predisposition.7–16
Electrophysiological mechanism of repolarization disorder results from either the induction of beats or disturbance in conduction. The proper flow of ions, as well as the function of the ion channels, is crucial for the stability of ventricular repolarization.17 With the action of catecholamines, the sympathetic nervous system activates β-adrenergic receptors in cardiomyocytes. As a result, second messenger concentration rises (namely calcium ions and cyclic adenosine monophosphate [cAMP]), leading to the activation of cAMP-dependent protein kinase A (PKA) and ion channels. Activated PKA can phosphorylate a range of proteins involved in the regulation of electrical activity and contractility.18 A diverse family of proteins is engaged in the regulation of activity of cAMP/PKA and in calcium signaling within the cells. One of them is the A-kinase anchoring proteins (AKAPs) family, which is a group of structurally heterogeneous proteins encoded by AKAP genes. Modification of both the cardiac ion channels and the structure of channel-related proteins (ie, AKAP) may induce arrhythmias.
Multiple studies have shown that AKAP10 may be associated with the regulation of the cardiac rhythm and may account for cardiac repolarization disturbances.17–23 The exact molecular mechanism still needs to be elucidated. In our previous study, we showed that the AKAP10 polymorphism was associated with acquired repolarization disorders in kidney recipients during transplantation procedure.24 In turn, clinical significance of such polymorphism with a reference to specific perioperative factors in the field of vascular surgery remains unexplored.
The aim of the present study was to assess the predisposition of functional genetic variants of AKAP10 toward acquired repolarization disorders in high-risk vascular surgery patients.
Materials and methods
A prospective observational study was conducted in the Department of Anesthesiology, Intensive Therapy and Acute Intoxications of Pomeranian Medical University in Szczecin, Poland. The study was granted permission from the local bioethical committee of Pomeranian Medical University in Szczecin, Poland. Written informed consent was obtained from all participants. The study has been registered at the ClinicalTrials.gov website (NCT03188341).
The study group consisted of 100 patients (mean age: 66±9 years), predominantly (87%) male, diagnosed with abdominal subrenal aortic aneurysm (69%) or aortoiliac occlusive disease (31%), scheduled for an elective “open” vascular surgery procedure. The patients were included in the study for 2 years. Demographic, Holter, and laboratory data were collected immediately after the operation. Genetic analysis was performed in two rounds after a adequate number of samples had been gathered, and concluded within 1 year from the operation. All performed procedures were assessed as the highest surgical risk according to the European Society of Cardiology (ESC)/European Society of Anaesthesiology guidelines.25 Patient and procedure risks were assessed by Vascular Physiological and Operative Severity Score for the enumeration of Mortality and Morbidity (V-POSSUM) scoring system. Inclusion criteria were the following: adult patients diagnosed with abdominal subrenal aortic aneurysm or peripheral arterial disease scheduled for an elective “open” vascular surgery procedure. Exclusion criteria were the following: heart stimulation (paced rhythm), atrioventricular conduction disturbances, intraventricular conduction disturbances (defined by abnormal QRS morphology and duration >120 ms in the standard 12-lead ECG), any prior episode of atrial fibrillation documented by the standard 12-lead ECG or ECG Holter, antiarrhythmic drug treatment (except β-blockers), taking any drugs with proarrhythmic potential (according to the Guidance for Industry E14 Clinical Evaluation of QT/QTc Interval Prolongation and Proarrhythmic Potential for Non-Antiarrhythmic Drugs available in http://www.fda.gov/cder/guidance/index.htm), patient general status (uncontrolled diabetes and active infection), reoperation, and emergency operations. All patients who qualified for the study underwent general and/or regional anesthesia according to a local protocol (described in detail in our previous study).26 In the operating room, standard monitoring of vital functions was carried out, including an ECG, continuous invasive blood pressure and central venous pressure monitoring using an Infinity® Delta Monitor (Draeger G, Luebeck, Germany), and in some cases (American Society of Anaesthesiology IV) advanced hemodynamic monitoring by Vigileo™ Monitor (Edwards Lifesciences, Irvine, CA, USA). Fluid therapy, ephedrine boluses (Ephedrinum Hydrochloricum WZF; Polfa, Warszawa, Poland), dobutamine (Sandoz GmbH, Kundl, Austria), and/or noradrenaline (Levonor; Polfa, Warszawa, Poland) infusion were used according to the local protocol. Acute functional changes of the cardiovascular system were defined as follows: heart rate <50 or >120 bpm and/or blood pressure amplitude (maximal–minimal range) >50 mmHg for systolic pressure and/or 30 mmHg for diastolic pressure lasting longer than 10 minutes despite treatment within the first 24 hours after the beginning of the operation.27 Metabolic monitoring consisted of electrolytes and arterial blood gas analysis of samples drawn just prior to anesthesia induction and at the end of the procedure. The following parameters were analyzed: pH, lactate, hemoglobin, hematocrit, and potassium concentration (K+), using a GEM Premier 3000 (Werfen Company, San Diego, CA, USA).
Repolarization stability was assessed by Holter ECG recording. Immediately before anesthesia, continuous electrocardiographic recording was initiated using digital Holter ECG monitor type 300-7 (Suprima System, Oxford, UK) and maintained up to 24 hours after surgical procedure. Seven electrodes were placed in standard positions (type B). Type B, which generated ECG tracings in 3 leads: V5, V1, and III at a speed of 25 mm/s and standard amplification of 1 mV/cm. After manual trace analysis, a dedicated researcher (medical doctor) performed the evaluation, which consisted of arrhythmia classification and assessment of QTc according to Bazett formula (QTc = QT/RR1/2). Repolarization disturbances during the surgical procedure or within the first 24-hour period were defined as at least one of the following: corrected QT interval longer than 500 ms or the maximal–minimal corrected QT interval (dispersion) longer than 65 ms, evaluated by ECG Holter recording (subgroups encoded: “repolarization disturbances present” vs “repolarization disturbances absent”).
After the induction of anesthesia, 4 mL of blood was collected from all the patients into a probe with anticoagulant to enable genetic studies. Genomic DNA was isolated from peripheral blood leukocytes using the QIAamp Blood DNA Mini Kit (Qiagen, Hilden, Germany). Subsequently, we applied polymerase chain reaction (PCR) restriction fragment length polymorphism methods to investigate 1936A→G (I646V) (rs203462) AKAP10 polymorphism in the study population. Optimal PCR conditions (temperature–time profile and the number of cycles) for given primer pairs and conditions for restriction analysis of formed amplicons were identified in initial experiments. All amplifications were performed in a thermal cycler Mastercycler® gradient (Eppendorf, Warsaw, Poland). The 20 μL of reacting mixture contained 40 ng of genomic DNA, PCR buffer (10 mmol/L Tris–HCl, 50 mmol/L KCl, and 0.08% Nonidet P40; MBI Fermentas, Vilnius, Lithuania), deoxynucleotide triphosphate (200 mmol/L; MBI Fermentas), magnesium chloride (1.5 mmol/L; MBI Fermentas), sense and antisense primers – 4 pmol each (TIB Molbiol, Poznan, Poland), and 0.5 U of Taq polymerase (MBI Fermentas). Restriction fragments separated electrophoretically in a 3% agarose gel were stained with ethidium bromide. The separation was performed in a Tris/borate/EDTA buffer (0.089 mmol/L Tris, 0.089 mmol/L boric acid, and 2 mmol/L EDTA), at a temperature of 20°C and a voltage of 70 V. Restriction fragments were identified based on DNA markers (pUC Mix Marker 8; MBI Fermentas). The final stage was gel documentation using the G:BOX BioImaging System (Syngene, Cambridge, UK).
Postoperative cardiac complications were defined as acute coronary syndrome (ACS), acute cardiac failure, syncope, or sudden cardiac death (SCD) within the first 24 hours after beginning the surgical procedure. These events were diagnosed with clinical examination, ECG, laboratory tests, and echocardiography. The normal ranges of the biochemical results when considering ACS were defined as follows: troponin I: 0.01–0.2 μg/L and creatine kinase-MB: 17–35 IU/L. Table 1 presents the definitions of cardiac complications.
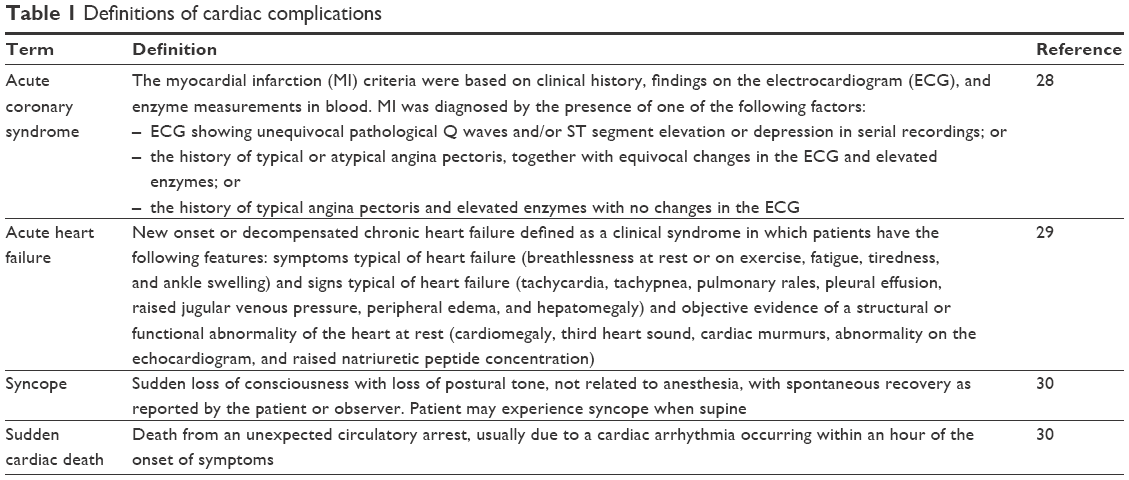 | Table 1 Definitions of cardiac complications |
Ventricular tachycardia was defined according to the American College of Cardiology/American Heart Association/ESC 2006 guidelines.30 Statistical analysis was performed using STATISTICA 13.1 PL software (Statistica, Tulsa, OK, USA). The normality of the data distribution was verified using Shapiro–Wilk test. Since most quantitative variables were nonnormally distributed, nonparametric Mann–Whitney test was used for their between-group comparisons. χ2 or Fisher’s exact test was used for quantitative variables, including genotypes. Multivariate logistic regression models were constructed to find independent predictors of repolarization disturbances or cardiac complications. A p-value <0.05 was considered statistically significant.
The power of the study to detect an association of the AKAP10 rs203462 single-nucleotide polymorphism (SNP) with repolarization disorders recorded by Holter was estimated using PS program Version 3.0.43, given assumptions based on previous studies that the disorders ought to be present in 50% of patients and the frequency of G allele carriers in Polish population is 50%. The study sample size (n=100) was sufficient to detect with 80% probability the true effect degree of difference in frequency of Holter ECG disorders between G allele carriers and AA homozygotes measured as odds ratio (OR) equal to 0.304 or 3.289.
Ethics approval and consent to participate
The study was granted permission from the Bioethical Committee of Pomeranian Medical University in Szczecin, Poland (27.05.2008; BN-001/52/08).
Results
We recruited 100 patients (aged 66±9 years, range: 44–85). The mean value of the Physiology Score V-POSSUM was 14±3. All the patients were treated with aspirin and statins; 60% of the patients were treated with β-blocker because of ischemic heart disease, heart failure, or arterial hypertension. According to the demographic and clinical data, concomitant medications were continued in the perioperative period. No patient had kidney failure in the past medical history.
The mean blood loss during the procedure was 570±250 mL. Thirty-one percent of the patients needed vasopressors or inotropes boluses/infusion for hemodynamic stabilization. The drug most commonly used was ephedrine. No patient needed prolonged ventilatory support.
The study population had the following AKAP10 gene rs203462 polymorphism distribution: AA 53%, AG 35%, and GG 12%. The distribution was in concordance with Hardy–Weinberg equilibrium (p=0.146).
Perioperative causes of repolarization disturbances registered by Holter
There was no prolongation of the QTc interval nor QTc dispersion before the surgery. During the operation and within the first 24 hours, repolarization disturbances were registered in 36% of patients when defined as acquired QTc interval prolongation >500 ms and in 31% of patients when defined as QTc interval dispersion >65 ms. ECG Holter monitoring recorded nonsustained monomorphic tachycardia within the first 24 hours in six cases, yet it was only observed in the subgroup of patients with repolarization disturbances (p=0.007).
Regarding 24-hour ECG Holter records, patients were stratified into two groups depending on whether the repolarization disturbances were present or absent. Table 2 compares these data.
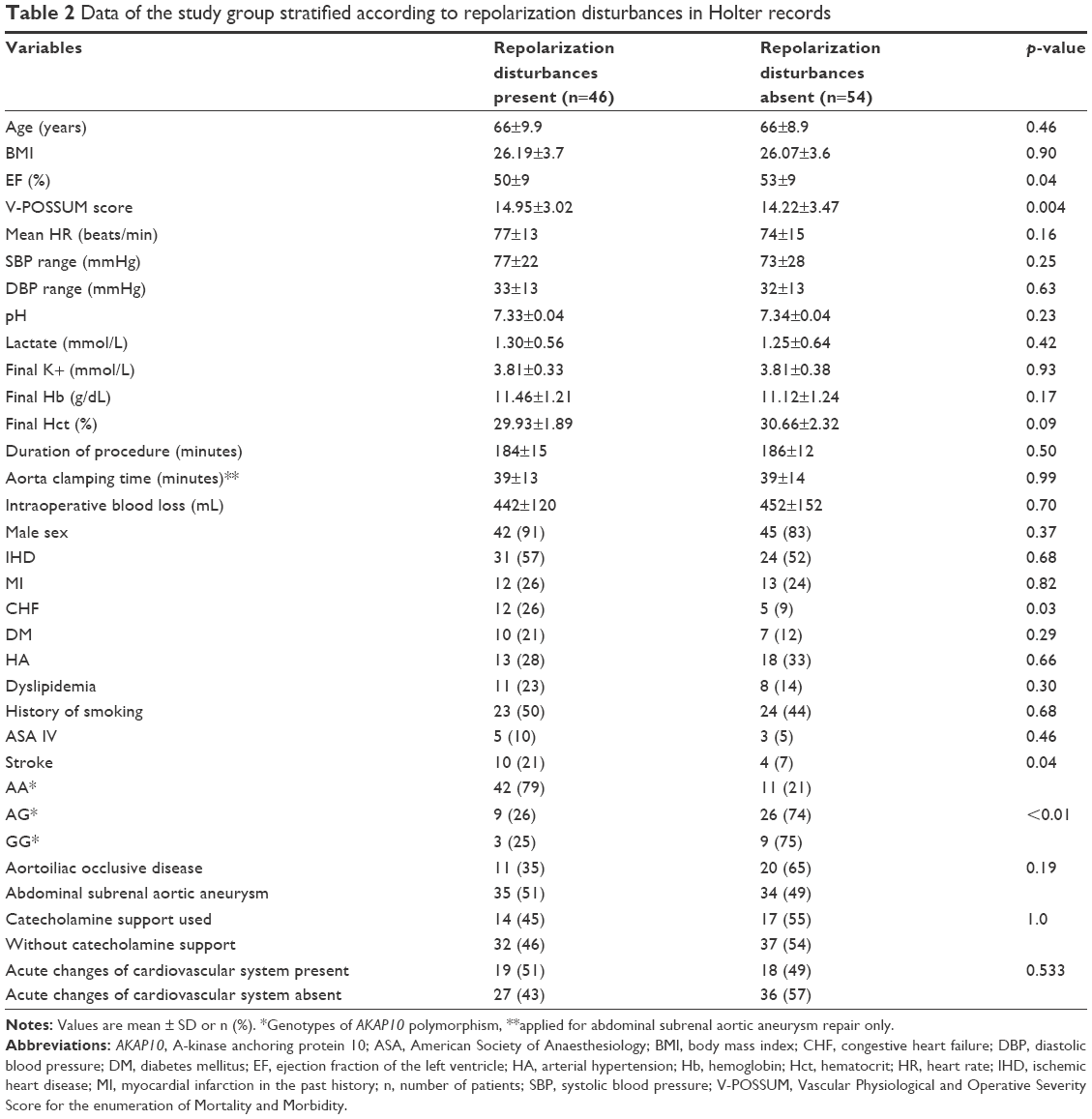 | Table 2 Data of the study group stratified according to repolarization disturbances in Holter records |
There were no significant differences between groups regarding the type of surgery, metabolic parameters, duration of the procedure, aorta clamping time, or intraoperative blood loss. In the model of univariate logistic regression, the clinically important predictors of repolarization disturbances occurring in the 24-hour Holter ECG were the following: preoperative heart failure (OR =3.45; 95% CI =1.10–10.87; p=0.031) and a history of cerebral stroke (OR =3.47; 95% CI =0.99–12.13; p=0.048). The presence of G allele in the AKAP10 polymorphism (genotypes GG + AG) turned out to be a strong predictor of repolarization derangement in the perioperative period (OR =11.13; 95% CI =4.32–28.64; p<0.0001). Table 3 presents the data.
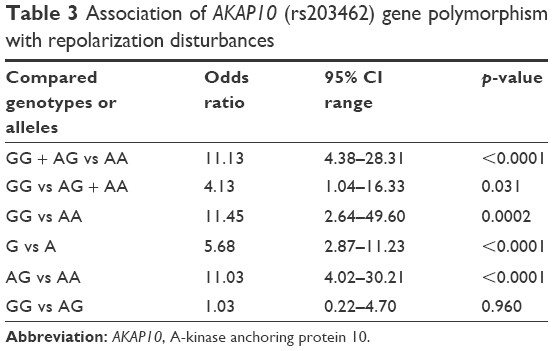 | Table 3 Association of AKAP10 (rs203462) gene polymorphism with repolarization disturbances |
In the model of multivariate logistic regression, considering age, sex, preoperative heart failure, stroke, and V-POSSUM score, only the presence of G allele in the rs203462 AKAP10 polymorphism constitutes an independent risk factor for repolarization disturbances in the perioperative period (OR =14.35; 95% CI =4.65–44.23; p<0.0001; GG + AG vs AA). Other clinical risk factors included in this model were insignificant predictors of the perioperative repolarization period disturbances (p>0.1).
Clinical significance of repolarization disturbances (first 24 hours)
The earlier-defined acute functional changes of the cardiovascular system and simultaneous repolarization disturbances occurred in 19 cases. There was no statistically significant association between them. We observed the following clinical picture: hypotension: 10 patients, bradycardia: three cases, and tachycardia: six patients. Acute hemodynamic decompensation that occurred during the operation was observed in 17 cases, and one that occurred within 24 hours after the operation was observed in only two cases. The acute functional changes of the cardiovascular system were observed at the following times: induction to general anesthesia (six patients), declamping of aorta (11 patients), and hypotension and episode of atrial fibrillation after operation (two patients).
After the surgical procedure, clinical significance of complications was assessed by clinical examination, ECG, laboratory tests, and echocardiography. Postoperative cardiac complications were diagnosed in five cases. ACS was confirmed in one case, and decompensation of chronic heart failure (CHF) was diagnosed in three cases. One patient died because of severe ventricular arrhythmia (SCD). Both ACS and SCD occurred in the subgroup that was free of repolarization disturbances. In turn, cases of decompensated CHF belonged to the repolarization disturbances subgroup. In all the above five cases, the first manifestation was hypotension observed after clamp release during abdominal aortic aneurysm procedures.
None of the genetic variants of the AKAP10 polymorphism turned out to be a predictor of acute functional changes of the cardiovascular system.
Discussion
The frequency of repolarization abnormalities is elevated in high-risk vascular patients. Its clinical importance and association with postoperative cardiac complications remain to be elucidated. In our study, ventricular repolarization disturbances were observed in almost half of the vascular surgery patients. The only factor independently associated with the occurrence of repolarization abnormalities in the 24-hour ECG Holter monitoring is the presence of G allele of the rs203462 polymorphism of AKAP10. Despite the presence of observed repolarization disturbances, none were clinically significant (ie, causing any clinical symptoms). The main result of the study was to prove the predisposition of functional genetic variants of AKAP10 toward clinically benign acquired repolarization disorders (QTc interval or dispersion prolongation) in high-risk vascular surgery patients. According to our knowledge, there are no similar studies available in the literature.
We defined limit values of repolarization disturbances (QTc >500 ms and QT dispersion >65 ms) based on our previous observations since there are no absolute QTc intervals or dispersion thresholds above which ventricular arrhythmia must occur.24,26 Botchorishvili et al concluded that QT dispersion longer than 70 ms is considered a risk factor of ventricular arrhythmia development in vascular surgery patients.31 Sahu et al concluded that QT dispersion in normal subjects should be ≤50 ms and that QTc dispersion >60 ms was associated with a twofold increase in SCD.32 We noticed repolarization disturbances in 46 patients (46%). No polymorphic ventricular tachycardia was detected. We observed paroxysmal monomorphic ventricular tachycardia in six cases. Episodes recorded by ECG Holter were very short and “clinically concealed” (as without hemodynamic decompensation). This observation cannot be explained by the simultaneous action of drugs. Masutani observed serious arrhythmias, respectively, in 10% and 11%, intraoperatively and postoperatively, among abdominal surgery patients.33 They showed the following risk factors: advanced age, ventricular extrasystoles, and untreated hypotension. No similar data exist for vascular surgery.
Several previous studies have analyzed a relationship between AKAP10 gene polymorphisms and cardiac repolarization disturbances among kidney transplant recipients and in newborns.24,34 The result of the kidney transplantation study indicates that the presence of allele G of the rs203462 AKAP10 polymorphism may predispose to prolongation of the QT interval when compared to allele A carriers.24 Łoniewska et al observed similar results in the newborns.34 The QT interval in GG homozygotes of AKAP10 was significantly longer (but still in range) when compared to A allele carriers (AG + AA). In both studies, repolarization disturbances did not provoke clinically significant arrhythmia or hemodynamic failure. Some authors believe that the genetic variant of AKAP10 is expressed as truncated forms unable to anchor PKA.18,21 Such a situation may lead to cardiac arrhythmias and SCD. The findings from studies on humans and mice have similar conclusions.17,21 On the other hand, an SNP 1936A→G (I646V) (rs203462) in D-AKAP2 (a product of AKAP10 gene, which can interact with PKA) is recognized as a cause of increased affinity of cAMP for PKA. It was found to correlate with a shorter PR interval, tachycardia, and abnormal heart rate variability – well-defined causes of SCD.17,18
Why some repolarization disturbances are clinically concealed or significant. The initiation of arrhythmia has multifactorial etiology. Although QTc interval or dispersion prolongation is almost always required to develop ventricular arrhythmia, it is not sufficient to trigger an arrhythmic episode.6 Many acquired factors may sustain tachyarrhythmia, leading to clinical features such as acute hemodynamic decompensation during ACS, acute circulatory failure, severe arrhythmias, syncope, and SCD. In the case of temporary short-acting triggering factors, ventricular arrhythmia may be inconstant and clinically concealed. Our results support this theory. Although 46% of our patients recorded repolarization disturbances, none have resulted in acute cardiac complications. Even though repolarization disturbances in perioperative Holter monitoring and acute functional changes of cardiovascular system were present at the same time in 19 patients, there were no statistically significant associations between them. Moreover, we have found that if the reason for QTc prolongation or QTc dispersion was the AKAP10 polymorphism, it was clinically silent. This supports the theory that in the case of induction of arrhythmia, clinical factors are more important than genetic predisposition. In contrast, Kukla et al have analyzed which of the electrocardiographic parameters indicate worse evolution in patients with acquired long QT syndrome and torsade de pointes.35 They defined values, which could predict benign evolution: slower ventricular rate during arrhythmia (<220 bpm) and shorter episodes <20 beats. In our population, we observed <20 ventricular beats during ventricular arrhythmia. It may explain why our repolarization disturbances were “concealed.” However, this finding shows that a continuous ECG recording is essential during and after the procedure because potentially rapid management and initiation of treatment may prevent the persistence of the arrhythmia. Therefore, factors leading to the acquired QT interval prolongation should be avoided, namely bradycardia, ion imbalance (hypokalemia, hypomagnesemia, and hypocalcemia), some drugs, acidosis, hypothermia, increased sympathetic activation, and intensive fluctuations in the tone of the autonomic nervous system.36
The results of our study indicate that the ECG Holter monitoring is a good tool to record repolarization disturbances present in high-risk vascular surgery patients. Despite recorded repolarization abnormalities, none of them caused acute cardiac complications within the first 24 hours after the surgical procedure. Several studies concluded that repolarization disturbances defined as QTc interval prolongation are seen during the early phase of myocardium ischemia and could be considered a risk factor.8 Despite some authors suggest utility of perioperative QTc assessment, it is not a routine management. Up until now, preoperative risk assessment encompasses clinical risk prediction, biochemical risk markers, and risk of procedure (surgery and anesthesia).1,36
This study had some important limitations. First, we assessed our cohort as at high risk based on clinical risk factors only. Second, we did not study cardiac ischemia based on ST segment depression detected by electrocardiographic cardiac Holter monitoring. Third, considering potential risk factors for the occurrence of repolarization disturbances, we did not analyze their elements separately due to a low number of patients.
Conclusion
Our study showed that the repolarization disturbances assessed by acquired prolongation of the QTc interval and QTc dispersion were common in vascular surgery patients during the perioperative period. ECG Holter monitoring was a useful tool for the detection of ventricular repolarization abnormalities. The role of genetic variants of AKAP10 was important in diagnosing predisposition for acquired ventricular repolarization disturbances. When the QTc interval prolongation or QTc dispersion was associated with AKAP10 polymorphism, it may remain clinically silent.
Acknowledgments
This work was supported by Pomeranian Medical University, Szczecin, Poland. We received funds for covering the costs to publish in open access from Pomeranian Medical University, Szczecin, Poland.
Author contributions
JB designed the study, collected the data, analyzed the results, and wrote the manuscript. JSP analyzed the results and provided critical review of the manuscript. AK analyzed the results, collected the data, and provided critical review of the manuscript. KS and MK designed and performed statistical analysis. MZB, MZ, and KK made substantial contributions to the conception of the work and critically reviewed the manuscript. All the authors read and approved the final manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Biccard BM, Naidoo P, de Vasconcellos K. What is the best pre-operative risk stratification tool for major adverse cardiac events following elective vascular surgery? A prospective observational cohort study evaluating pre-operative myocardial ischaemia monitoring and biomarker analysis. Anaesthesia. 2012;67:389–395. | ||
Ferrante AM, Moscato U, Colacchio EC, Snider F. Results after elective open repair of pararenal abdominal aortic aneurysms. J Vasc Surg. 2016;63:1443–1450. | ||
Devereaux PJ, Sessler DI. Cardiac complications in patients undergoing major noncardiac surgery. N Engl J Med. 2015;373:2258–2269. | ||
Tse G, Yan BP. Traditional and novel electrocardiographic conduction and repolarization markers of sudden cardiac death. Europace. 2017;19:712–721. | ||
Sauer AJ, Selvaraj S, Aguilar FG, et al. Relationship between repolarization heterogeneity and abnormal myocardial mechanics. Int J Cardiol. 2014;172:289–291. | ||
Johnston J, Pal S, Nagele P. Perioperative torsade de pointes: a systematic review of published case reports. Anesth Analg. 2013;117:559–564. | ||
Kleber AG, Rudy Y. Basic mechanisms of cardiac impulse propagation and associated arrhythmias. Physiol Rev. 2004;84:431–488. | ||
Kenigsberg DN, Khanal S, Kowalski M, Krishnan SC. Prolongation of the QTc interval is seen uniformly during early transmural ischemia. J Am Coll Cardiol. 2007;49:1299–1305. | ||
Biernawska J, Kaźmierczak J, Kotfis K, Żukowski M. The influence of regional anaesthesia and local anaesthetics on cardiac repolarization. Anaesthesiol Intensive Ther. 2016;48:135–141. | ||
Galluzzo A, Gallo C, Battaglia A, et al. Prolonged QT interval in ST-elevation myocardial infarction: predictors and prognostic value in medium-term follow-up. J Cardiovasc Med (Hagerstown). 2016;17:440–445. | ||
Vandael E, Vandenberk B, Vandenberghe J, Willems R, Foulon V. Risk factors for QTc-prolongation: systematic review of the evidence. Int J Clin Pharm. 2017;39:16–25. | ||
Murakawa Y, Yamashita T, Ajiki K, et al. Is the QT interval an indicator of autonomic state? Jpn Heart J. 2000;41:713–721. | ||
Dilaveris PE. Molecular predictors of drug induced prolongation of the QT interval. Curr Med Chem Cardiovasc Hematol Agents. 2005;3:105–118. | ||
Owczuk R, Wujtewicz MA, Zienciuk-Krajka A, Lasińska-Kowara M, Piankowski A, Wujtewicz M. The influence of anesthesia on cardiac repolarization. Minerva Anestesiol. 2012;78:483–495. | ||
Li M, Ramos LG. Drug-induced QT prolongation and torsades de pointes. P T. 2017;42:473–477. | ||
Porthan K, Marjamaa A, Viitasalo M, et al. Relationship of common candidate gene variants to electrocardiographic T-wave peak to T-wave end interval and T-wave morphology parameters. Heart Rhythm. 2010;7:898–903. | ||
Scott JD, Santana LF. A-kinase anchoring proteins: getting to the heart of the matter. Circulation. 2010;121:1264–1271. | ||
Soni S, Scholten A, Vos MA, van Veen TAB. Anchored protein kinase A signaling in cardiac cellular electrophysiology. J Cell Mol Med. 2014;18:2135–2146. | ||
Diviani D, Maric D, Pérez López I, Cavin S, del Vescovo CD. A-kinase anchoring proteins: molecular regulators of the cardiac stress response. Biochim Biophys Acta. 2013;1833:901–908. | ||
Chen L, Marquardt ML, Tester DJ, Sampson KJ, Ackerman MJ, Kass RS. Mutation of an A-kinase-anchoring protein causes long-QT syndrome. Proc Natl Acad Sci U S A. 2007;104:20990–20995. | ||
Tingley WG, Pawlikowska L, Zaroff JG, et al. Gene-trapped mouse embryonic stem cell-derived cardiac myocytes and human genetics implicate AKAP10 in heart rhythm regulation. Proc Natl Acad Sci U S A. 2007;104:8461–8466. | ||
Neumann SA, Tingley WG, Conklin BR, et al. AKAP10 (I646V) functional polymorphism predicts heart rate and heart rate variability in apparently healthy, middle-aged European-Americans. Psychophysiology. 2009;46:466–472. | ||
Kammerer S, Burns-Hamuro L, Ma Y, et al. Amino acid variant in the kinase binding domain of dual specific A kinase-anchoring protein 2: a disease susceptibility polymorphism. Proc Natl Acad Sci U S A. 2003;100:4066–4071. | ||
Żukowski M, Bohatyrewicz R, Biernawska J et al. Association of the A1936G (rs203462) of A-kinase anchoring protein 10 polymorphisms with QT interval prolongation during kidney transplantation. Transplant Proc. 2009;41:3036–3038. | ||
The Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery; European Society of Cardiology (ESC), Poldermans D, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009;30:2769–2812. | ||
Biernawska J, Kaczmarczyk M, Kotfis K, et al. Electrophysiological, hemodynamic, and metabolic response to open procedure or endovascular repair of infrarenal aortic aneurysms. Ann Vasc Surg. 2014;28:1659–1664. | ||
Thompson JP, Boyle JR, Thompson MM, Strupish J, Bell PR, Smith G. Cardiovascular and catecholamine responses during endovascular and conventional abdominal aortic aneurysm repair. Eur J Vasc Endovasc Surg. 1999;17:326–333. | ||
Mendis S, Thygesen K, Kuulasmaa K, et al. World Health Organization definition of myocardial infarction: 2008–09 revision. Int J Epidemiol. 2011;40:139–146. | ||
McMurray JJ, Adamopoulos S, Anker SD, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787–1847. | ||
Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death – executive summary: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death) Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Eur Heart J. 2006;27:2099–2140. | ||
Botchorishvili I, Sharashidze N, Pargalava N, Pagava Z, Saatashvili G. Differences in ECG characteristics and co-morbidities among patients who underwent elective surgical repair. Georgian Med News. 2016;Nov:47–51. | ||
Sahu P, Lim PO, Rana BS, Struthers AD. QT dispersion in medicine: electrophysiological holy grail or fool’s gold? QJM. 2000;93:425–431. | ||
Masutani M. [Holter electrocardiographic findings in surgical patients during the perioperative period]. Masui. 1992;41:401–412. Japanese. | ||
Łoniewska B, Kaczmarczyk M, Clark JS, Gorący I, Horodnicka-Józwa A, Ciechanowicz A. Association of functional genetic variants of A-kinase anchoring protein 10 with QT interval length in full-term Polish newborns. Arch Med Sci. 2015;11:149–154. | ||
Kukla P, Jastrzębski M, Fijorek K, et al. Electrocardiographic parameters indicating worse evolution in patients with acquired long QT syndrome and torsades de pointes. Ann Noninvasive Electrocardiol. 2016;21:572–579. | ||
Duncan D, Wijeysundera DN. Preoperative cardiac evaluation and management of the patient undergoing major vascular surgery. Int Anesthesiol Clin. 2016;54:1–32. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.