Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Predictors of Virological Failure after Adherence-Enhancement Counseling among First-Line Adults Living with HIV/AIDS in Kombolcha Town, Northeast Ethiopia
Authors Bisetegn G, Arefaynie M ![]() , Mohammed A
, Mohammed A ![]() , Fentaw Z
, Fentaw Z ![]() , Muche A
, Muche A ![]() , Dewau R
, Dewau R ![]() , Seid Y
, Seid Y
Received 11 November 2020
Accepted for publication 6 January 2021
Published 26 January 2021 Volume 2021:13 Pages 91—97
DOI https://doi.org/10.2147/HIV.S290531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Getachew Bisetegn,1 Mastewal Arefaynie,2 Anissa Mohammed,3 Zinabu Fentaw,3 Amare Muche,3 Reta Dewau,3 Yimer Seid1
1Dessie City Zonal Health Department, CDC-Ethiopia, Dessie, Ethiopia; 2Department of Reproductive and Family Health, School of Public Health, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia; 3Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia
Correspondence: Zinabu Fentaw
Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia
Tel +251-91-275-7286
Email [email protected]
Background: HIV virological failure is a common challenging problem, even after adherence-enhancement counseling. However, there have been few studies on the determinants of virological failure after adherence-enhancement counseling among adult patients on antiretroviral therapy in Ethiopia in general, and there is variation across clients and settings for unknown reasons. Therefore, this study aimed to identify predictors of virological failure after adherence-enhancement counseling among adults living with HIV/AIDS.
Methods: A case–control study was conducted in the town of Kombolcha from January 1, 2019 to March 30, 2019 using simple random sampling for 338 participants. Data were collected through face-to-face interviews for social and personal characteristics and document review for clinical profiles. Descriptive statistics were used for frequency, proportions, and summary measures. Binary logistic regression analysis was carried out to identify the predictors of virological failure after adherence-enhancement counseling among adults. For multivariate logistic regression,P< 0.05 was considered statistically significant. AORs are presented with 95% CIs.
Results: The odds of virological failure after adherence-enhancement counseling were higher following poor antiretroviral medication adherence (AOR 7.3, 95% CI 2.57– 20.79) and for patients who had had a first high viral load (≥ 10,000 copies/mL, (AOR 5, 95% CI 1.86– 13.56) and a history of opportunistic infection (AOR 3.7, 95% CI 1.11– 8.44) compared with their counterparts.
Conclusion: Poor antiretroviral medication adherence during adherence-enhancement counseling session, first viral load ≥ 10,000 copies/mL, and recent history of opportunistic infection were predictors of virological failure. Therefore, efforts should be strengthened to improve adherence to antiretroviral medication, which helps to boost immunity and suppress viral replication.
Keywords: HIV/AIDS, adherence-enhancement counseling, virological failure, case–control, Ethiopia
Introduction
HIV virological failure is a detectable viral load >1,000 copies/mL on two consecutive viral load measurements 3–6 months apart with adherence support between measurements after at least 6 months of starting a new antiretroviral treatment (ART) regimen.1,2 According to the current national guideline, two or more high viral load results (≥1,000 copies/mL) 3–6 months apart is considered the gold standard for treatment failure compared with immunological and clinical failure.2 This failure induces a premature switch to second-line treatment without prioritizing determinants other than adherence.3 Unlike first-line drugs, second-line drugs are more toxic and expensive,4 and most are not in fixed-dose combinations1 which is one of the factors in poor adherence.5
Poor adherence to ART is the most common reason for high viral load.6 Common factors for high viral load other than poor adherence include drug resistance,7 malabsorption, drug–drug interactions, drug-associated side effects,8 and type of regimen,9 and addressing these may be important in preventing virological failure. The current systematic review and meta-analysis shows that viral resuppression is >53% in patients with initial high viral loads.10 Globally, virological failure after adherence-enhancement counseling is a public health problem, as >50% of antiretroviral users fail to achieve it.11 Even local reports of virological failure after adherence-enhancement counseling show higher failure rates than global reports, though there has been limited reports on a national level.
Virological failure after adherence-enhancement counseling can lead to high mortality and morbidity.12 On the other hand, virological failure after adherence-enhancement counseling causes low productivity and increases economic dependence, and social problems. Not controlling viral loads increases the rate of transmission,13 which is a challenge in achieving an end to HIV/AIDS epidemics by 2030.14
Even though the WHO recommends enrolling all clients with high initial viral loads in adherence-enhancement counseling programs1 and Ethiopia adopted this policy in 2017, with every client with high viral load receiving counseling on a monthly basis,15 the impact of adherence-enhancement counseling in decreasing viral load is low. There have been a few studies on determinants of virological failure after adherence-enhancement counseling among adult patients on ART in Ethiopia in general, but there have been variations across clients and settings for for unknown reasons. As such, this study aimed to assess determinants of virological failure after adherence-enhancement counseling.
Methods
Study Setting, Area, and Design
An institution-based unmatched 1:1 case–control study design was employed. The study was conducted in Kombolcha town’s ART health centers from January 1, 2019 to March 30, 2019. Kombolcha is located in northeast Ethiopia, about 378 km from Addis Ababa and 494 km from the capital of the region — Bahirdar. There were 4,322 ART clients in the town, of which 1,148 were in Kombolcha 05 health center and 3,174 clients were in Kombolcha 03 health center (October 2018 SmartCare report). There was a total of 418 ART clients with initial high viral load undergoing adherence-enhancement counseling sessions in the study period (October 2018 high viral load register).
Population
Adult clients with high viral load results on first-line ART enrolled for adherence-enhancement counseling for 3–6 months, with complete adherence-enhancement counseling sessions and a second viral load measurement. Cases were adult clients on first-line ART whose second plasma viral load result was ≥1,000 copies/mL within 3–6 months after completing adherence-enhancement counseling. Controls were adult clients on first-line ART with second plasma viral load <1,000 copies/mL within 3–6 months after completing adherence-enhancement counseling.
Sample-Size Determination
The sample size was determined using Epi Info 7.2 StatCalc by taking current BMI as a key predictor of virological failure after adherence-enhancement support, which reulted in a large sample size to be the minimum for the current study.16 Assumptions were 95%) confidence, 80% power, and 1:1 control:case ratio, with 40% control exposure. Finally, the sample size derived was 306, and then by adding a 10% contingency, the final sample size was 338.
Participants and Data Collection
Two ART public health institutions were included in the study. Medical charts of adult clients who had completed adherence-enhancement counseling were included. A separate list of adults with completed adherence-enhancement counseling from September 2016 to August 2018 was extracted from the high viral load register at ART clinics in the facilities for cases and controls. On each separate list for cases and controls, simple random sampling was carried out using a lottery method based on medical record numbers. After interviews had been conducted, charts of these clients were reviewed during visits to the health facilities for drug refills. The data-collection tool was developed from national ART guidelines, adherence-enhancement counseling tools, and the literature.2 A supervisor was checked the data daily for completeness and consistency before submission for data entry.
Data Management and Analysis
Data were entered into Epi Data 3.1 and exported to Stata 14 for cleaning and analysis. Descriptive statistics were computed using frequencies, proportions, and summary statistics, such as means and ± SD. Hosmer–Lemeshow and omnibus tests were conducted to test necessary assumptions and model fitness for binary logistic regression, respectively. Bivariable logistic regression was run to identify determinants of virological failure after adherence-enhancement counseling, and variables withP<0.2 were entered into a multivariate binary logistic regression model. On multivariable logistic regression, P<0.05 was considered statistically significant, are with 95% CIs presented.
Ethical Considerations
Before undertaking the investigation, ethical clearance was obtained from the Ethical Review Committee of Wollo University, College of Medicine and Health Sciences. Consent letters were also obtained from Kombolcha Town Health Office and the health facilities. All participants were informed about the risks, benefits, and their full right to withdraw or refuse the study at any time. Adults and parents/legal guardians of clients under the age of 18 years provided written informed consent. Privacy and confidentiality of information given by each respondent were guaranteed through anonymity. Data were collected as per the Declaration of Helsinki, and data accessibility was limited to third parties.
Result
Sociodemographic Characteristics
A total of 338 HIV positive adults (169 cases and 169 controls) participated in this study. The mean age of the cases and the controls was 35±6 years) and 37±6 years, respectively. In sum, 95 (56.8%) of cases and 99 (57.9%) of controls were females, 96 (56.8%) cases and 99 (58.6%) controls currently married. More than three-quarters (130, 77.5%; 137, 80.5%) of cases and controls were urban dwellers, respectively. A majority of (70, 41.4%; 75, 44.4%) had primary school education among cases and controls, respectively. Regarding occupation, 38 (22.5%) cases and 33 (19.5%) controls were farmers (Table 1).
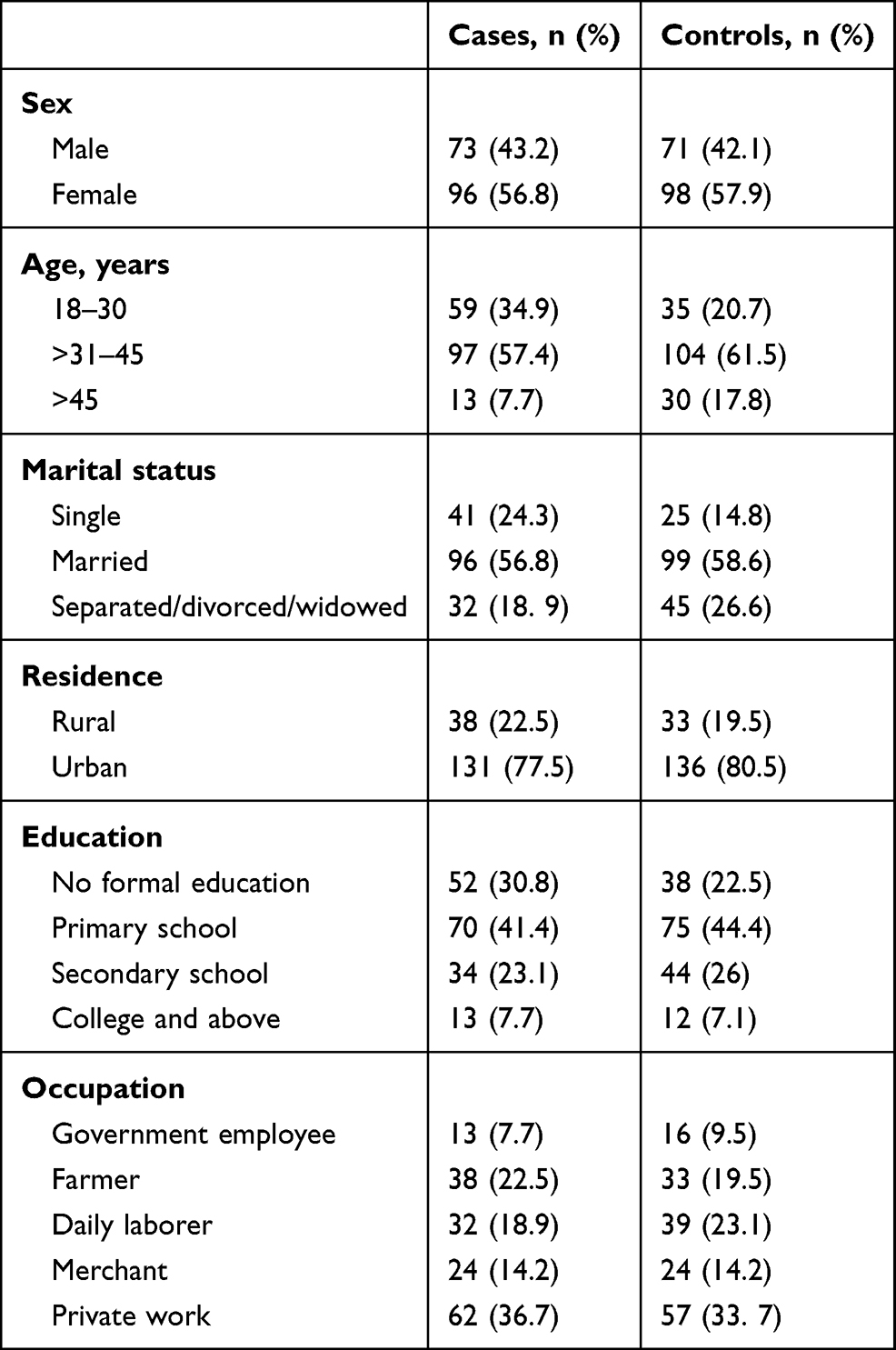 |
Table 1 Sociodemographic Characteristics of Adult First-Line ART Clients With VF After Adherence-Enhancement Counseling in Kombolcha, Northeast Ethiopia, May 2019 |
Behavioral and Clinical Characteristics
Among the participants, 70 (41.4%) cases and 55 (32.5%) controls reported consistent use of condoms before initial high viral load. Most respondents (146, 86.4%; 143, 84.6%) were nonsmokers among cases and controls, respectively. A majority(153, 90.5%; 151%, 89.9) were not drinking among cases and controls, respectively. Khat chewers numbered 53 (31.4%) and 53 (31.4) in cases and controls, respectively. Regarding disclosure status and partner’s HIV status, 145 (85.8%) and 102 (60.4%) cases and 140 (84.3%) and 93 (55%) controls had disclosed their HIV status and HIV-positive partner, respectively. A majority of respondents — 149 (88.2%) cases and 145 (85.8%) controls — had no hospital-admission history. In sum, 41 (24.3%) cases and 58 (34.3%) controls had a history of antiretroviral drug discontinuation (Table 2).
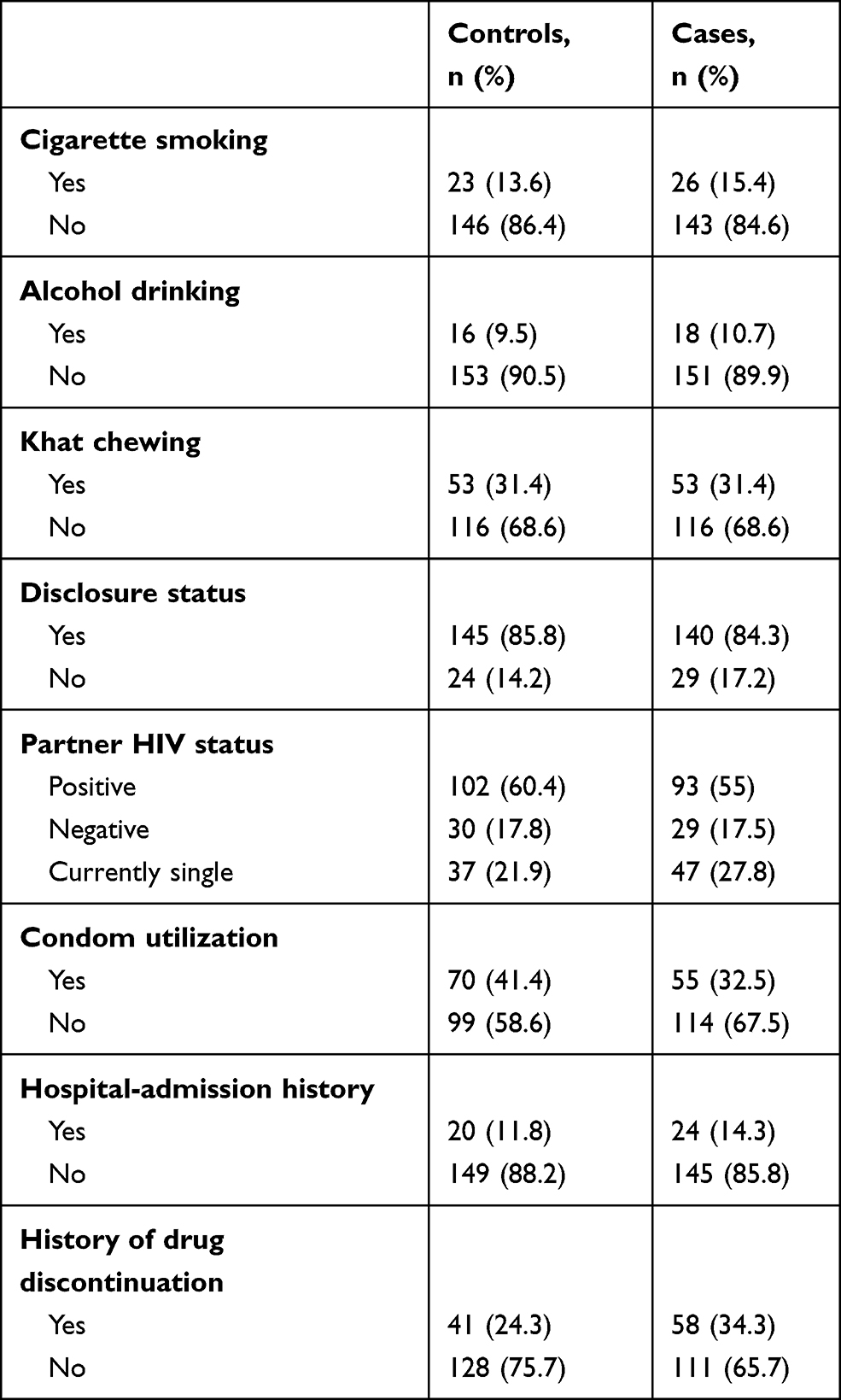 |
Table 2 Behavioral and Clinical Characteristics of Adult First-Line ART Clients with VF After Adherence-Enhancement Counseling in Kombolcha, Northeast Ethiopia, 2019 |
Antiretroviral Medication–Related Characteristics
Over half (93, 55.4%) the cases and 28 (16.5%) of the controls had poor adherence to treatment during adherence-enhancement sessions, while 63 (37.5%) of the cases and nearly a third (57,33. 5%) of the controls had been on highly active ART ≥10 years. Among patients, 69 (41.1%) cases and 50 (29.4%) controls had a history of opportunistic infections. Of those with an initial high viral load, 116 (69%) cases 51 (30%) controls had an initial load ≥ 10,000 copies/mL. Over half the cases (88, 52.1%) and controls 96 (56.8%) were receiving twice-daily antiretroviral drug doses. Regarding the history of missing antiretroviral drug doses during adherence-enhancement counseling, 22 (13%) and 29 (17.2%) were missing their doses in cases and controls, respectively (Table 3).
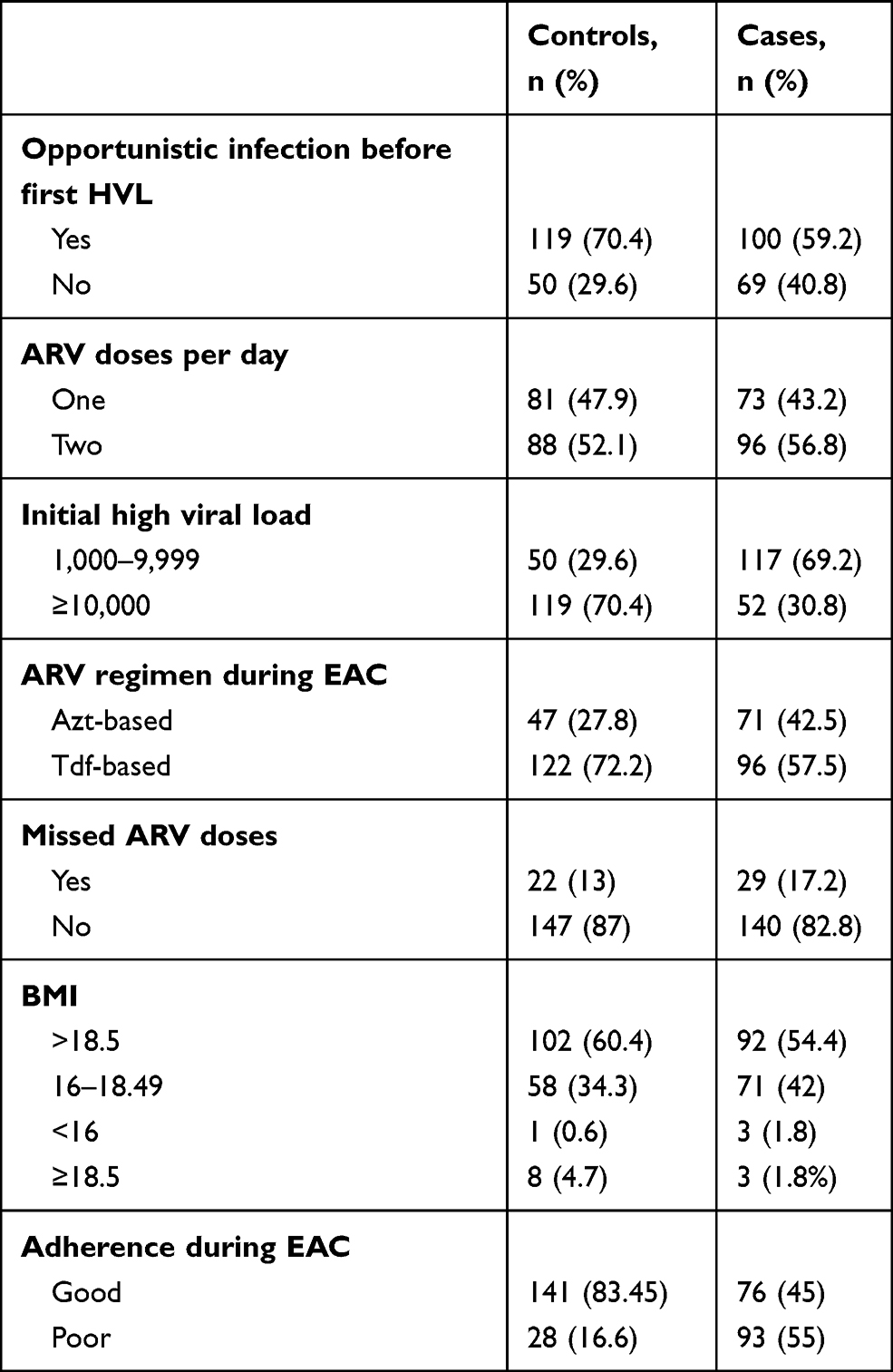 |
Table 3 Antiretroviral Medication-Related Characteristics of Adult First-Line ART Clients With VF After Adherence-Enhancement Counseling in Kombolcha, Northeast Ethiopia, 2019 |
Predictors of Virological Failure
The bivariable logistic regression analysis showed that age, marital status, education, type of antiretroviral regimen, ART-medication adherence during adherence-enhancement counseling, history of opportunistic infections (within 2 years before first high viral load), depression status, first high viral load value, ART discontinuation, and condom utilization were associated with virological failure after adherence-enhancement counseling (P<0.2, Table 4).
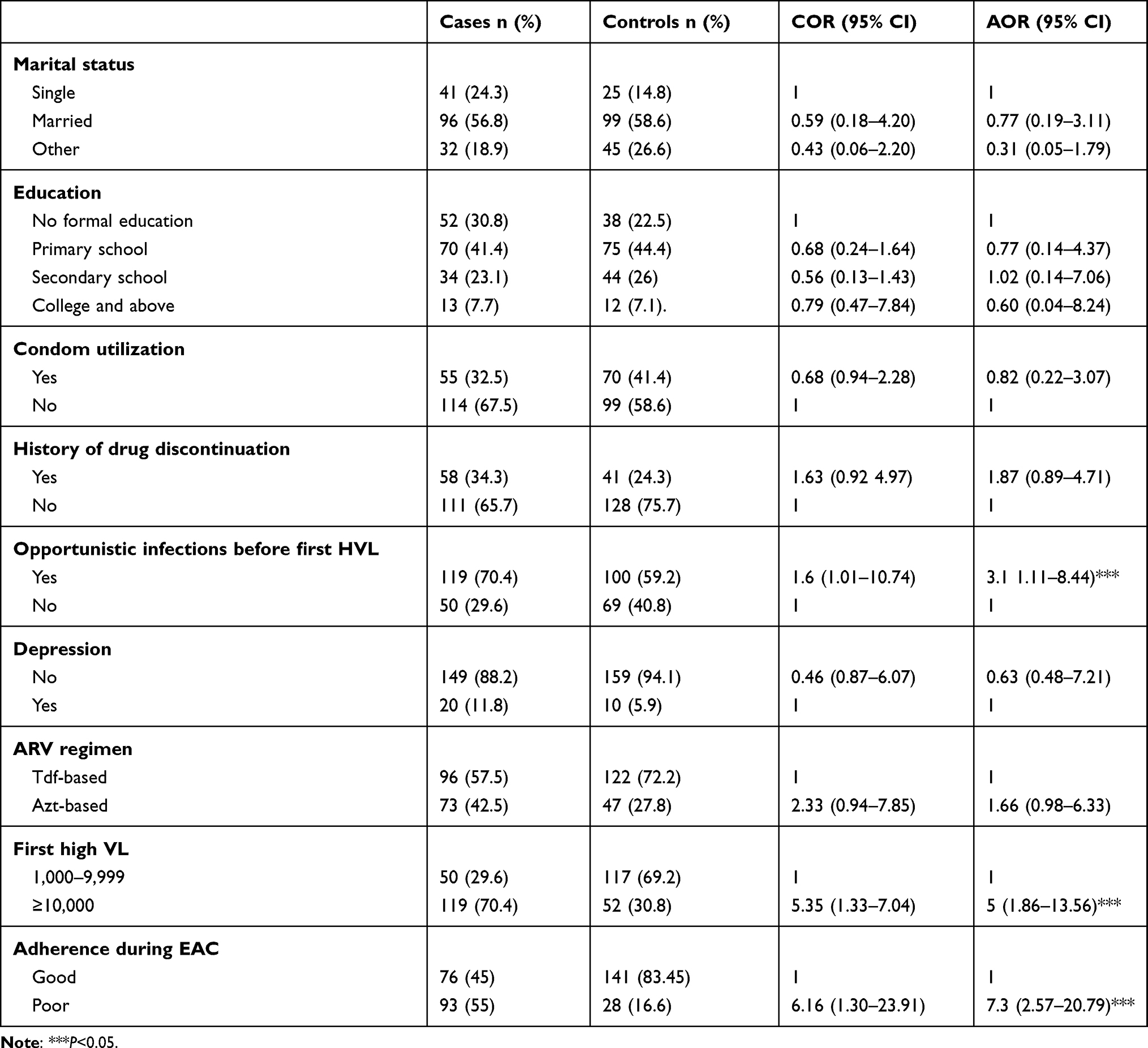 |
Table 4 Predictors of Adult First-Line ART Clients With VF After Adherence-Enhancement Counseling in Kombolcha, Northeast Ethiopia, 2019 |
After adjustment for possible effects of confounding variables, poor ART-medication adherence during adherence-enhancement counseling, first viral load ≥10,000 copies/mL, and history of opportunistic infection (within 2 years before high viral load) were significantly associated with virological failure. The likelihood of developing virological failure was 7.3-fold higher among patients with poor ART-medication adherence during adherence-enhancement counseling than those with good adherence (AOR 7.3, 95% CI 2.57–20.79). Patients who had had a first viral load >10,000 copies/mL were five times as likely to have virological failure as those with a first viral load <10,000 copies/mL (AOR 5, 95% CI 1.86 –13. 56). The odds of developing virological failure were found to be 3.7 times higher among subjects with a history of opportunistic infections than their counterparts (AOR 3.7, 95% CI, 1.11–8.44, Table 4).
Discussion
Regarding determinants of virological failure after adherence-enhancement counseling, the current study revealed that patients who had recent opportunistic infections, first high viral load ≥10,000, and poor adherence to ART medication during adherence-enhancement counseling were found to have increased odds of virological failure after adherence-enhancement counseling (Table 4).
Nonadherence to antiretroviral drugs in adult ART clients on adherence-enhancement counseling was a predictor of virological failure. This finding is similar to studies conducted at Gondar University Referral Hospital,6 Debre Markos Referral Hospital,17 and Dessie and Woldia referral hospitals,18 Ethiopia and Zimbabwe,19 where subjects who had good adherence were more likely to achieve viral load suppression. Survival studies conducted in southwestern Uganda showed that virological failure rates were significantly higher among participants who reported adherence <90% than those who reported good adherence >95%.9 It is grossly apparent that poor adherence to antiretroviral medication reduce treatment response due to suboptimal drug concentration and increases viral replication, which leads to virological failure. This may be due to the fact that individuals missing three or more doses of ART drugs per month are at increased risk of drug resistance and reduced immunity. This in turn results in a loss of opportunity to suppress viral replication and leads to virological failure.
This study also reflected that the odds of developing virological failure were higher among HIV-positive adults receiving adherence-enhancement counseling with a history of opportunistic infections than those who did not report such a history. In agreement with this finding, a study conducted in Uganda20 showed that risk of virological failure was increased among participants who had had opportunistic infections. As patients’ immuno status declined, the rate of viral replication increases compared to immunocompetent counterparts. Clients with compromised immunity are more vulnerable to opportunistic infections, which sustain the vicious cycle of immunity and viral replication.21
The other variable found to be an independent predictor of virological failure was first viral load ≥10,000 copies/mL. This finding is supported by a study conducted in Zimbabwe, where viral load 1,000–5,000 copies/mL) was more associated with viral suppression than viral load >5,000 copies/mL.19 Higher viral loads show that the virus replicates easily and is resistant to antiretroviral drugs, and patients face different opportunistic infections.7 High viral loads consume body nutrients, emaciating clients on ART and exposing the to further complications.
Conclusion
Poor ART-medication adherence during adherence-enhancement counseling, first viral load ≥10,000 copies/mL, and a recent history of opportunistic infections are known to be positive determinants of virological failure. This study highlights the need for more commitment and effort from all stakeholders to sustain the long-term efficacy of highly active ART, thereby achieving the ambitious target of 2020 and sustainable development goal to end the HIV epidemic by 2030.
Acknowledgment
We acknowledge the School of Public Health, College of Health and Medical Science, Wollo University for periodic follow-up and support. We also acknowledge the Kombolcha Town Health Office and health facilities for allowing access to the data and also our thanks go to the data collectors and supervisors for the carefully undertaking of their tasks.
Funding
This study was self-sponsored.
Disclosure
The authors declare that they have no competing interests.
References
1. WHO. The use of antiretroviral drugs for treating and preventing hiv infection. 2016
2. EFMoH National Consolidated Guidelines For Comprehensive Hiv Prevention, Care And. 2018
3. Shroufi A, Cutsem GV, Cambiano V, et al. Simplifying switch to second-line antiretroviral therapy in sub Saharan Africa: predicted effect of using a single viral load to define efavirenz-based first-line failure. AIDS. 2019;33(10):1635–1644. doi:10.1097/QAD.0000000000002234
4. Ripin D, Prabhu VR. OPINION A cost-savings analysis of a candidate universal antiretroviral regimen. Curr Opin HIV AIDS. 2017;12(4):403–407. doi:10.1097/COH.0000000000000375
5. UNAIDS. UNAIDS data 2018. 2018
6. Bayu B, Tariku A, Bulti AB, Habitu YA, Derso T, Teshome DF. Determinants of virological failure among patients on highly active antiretroviral therapy in University of Gondar Referral Hospital, Northwest Ethiopia: a case – control study. Hiv/aids (Auckland, NZ). 2017. 153–159.
7. Etoori D, Ciglenecki I, Ndlangamandla M, et al. Successes and challenges in optimizing the viral load cascade to improve antiretroviral therapy adherence and rationalize second-line switches in Swaziland. J Int AIDS Soc. 2018;1–8.
8. Kumar S, Earla R, Kumar A. Drug – drug interactions between anti-retroviral therapies and drugs of abuse in HIV systems. Expert Opin Drug Metab Toxicol. 2015;343–355.
9. Nasuuna E, Kigozi J, Babirye L, Muganzi A, Sewankambo NK. Low HIV viral suppression rates following the intensive adherence counseling (IAC) program for children and adolescents with viral failure in public health facilities in Uganda. BMC Public Health. 2018;1–9.
10. Ford N. REVIEW HIV viral resuppression following an elevated viral load: a systematic review and meta-analysis. J Int AIDS Soc. 2019;1–6.
11. MSF. Making viral load routine. Successes and challenges in the implementation of routine HIV viral load monitoring 2016
12. Hailu GG, Hagos DG, Hagos AK, Wasihun AG, Dejene TA. Virological and immunological failure of HAART and associated risk factors among adults and adolescents in the Tigray region of Northern Ethiopia. PLoS One. 2018;13(5):1–17.
13. Wilson DP, Law MG, Grulich AE, Cooper DA, Kaldor JM. Relation between HIV viral load and infectiousness: a model-based analysis. Lancet. 2008;372.
14. UNAIDS. An ambitious treatment target to help end the AIDS epidemic. 2014
15. PEPFAR. Ethiopia Country/ Regional Operational Plan (COP/ROP) 2017 Strategic Direction Summary. 2017
16. Jobanputra K, Parker LA, Azih C, et al. Factors Associated with Virological Failure and Suppression after Enhanced Adherence Counselling, in Children, Adolescents and Adults on Antiretroviral Therapy for HIV in Swaziland. Plos One. 2015;450:1–12.
17. Abebaw A. Magnitude of virologic failure and associated factors among adult patients on antiretroviral therapy at Debre Markos Referral Hospital, Northwest Ethiopia, 2018. 2018.
18. Ahmed M, Merga H, Jarso H. Predictors of virological treatment failure among adult HIV patients on first-line antiretroviral therapy in Woldia and Dessie hospitals, Northeast Ethiopia: a case-control study. BMC Infect Dis. 2019;1–7.
19. Id TB, Id SS, Takarinda KC, Bara H. Enhanced adherence counselling and viral load suppression in HIV seropositive patients with an initial high viral load in Harare, Zimbabwe: operational issues. Cancer Letters. 2019;444:1–13. doi:10.1016/j.canlet.2018.11.033
20. Bulage L, Ssewanyana I, Nankabirwa V, et al. Factors associated with virological non- suppression among HIV-positive patients on antiretroviral therapy in Uganda, August 2014 – July 2015. BMC Infect Dis. 2017;1–11.
21. DHHS. Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults. 2018
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.