Back to Journals » Patient Preference and Adherence » Volume 19
Predictors of Patient Engagement in a Care Coordination Program
Authors Adejumo KL ![]() , Kakyomya J, Bank A
, Kakyomya J, Bank A ![]() , Mineard AD, Soublet JH
, Mineard AD, Soublet JH ![]() , Blackwelder AC, Huyck K, Lurie JD, Patterson CG
, Blackwelder AC, Huyck K, Lurie JD, Patterson CG ![]() , McDonough C
, McDonough C
Received 30 April 2025
Accepted for publication 25 October 2025
Published 26 December 2025 Volume 2025:19 Pages 4245—4256
DOI https://doi.org/10.2147/PPA.S537769
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qizhi (Cathy) Yao
Kelechi L Adejumo,1 Joseph Kakyomya,1 Alison Bank,1 Amanda D Mineard,1 Joyce H Soublet,2 Alexis C Blackwelder,2 Karen Huyck,2 Jon D Lurie,2 Charity G Patterson1 ,† Christine McDonough1, †
1School of Health and Rehabilitation Science, Data Center, University of Pittsburgh, Pittsburgh, PA, USA; 2Dartmouth Hitchcock Medical Center, Dartmouth Health, Lebanon, NH, USA
†Dr Christine McDonough passed away on December 18, 2024
Correspondence: Charity G Patterson, School of Health and Rehabilitation Science, Data Center, University of Pittsburgh, Suite 500, Pittsburgh, PA, USA, Tel +1 412-383-4812, Email [email protected]
Purpose: To identify predictors of patient engagement in a care coordination program for individuals with work disabilities, using a continuum-based definition of engagement and the PROGRESS-Plus framework.
Patients and Methods: This observational analysis used deidentified data from the Vermont RETAIN Phase II program, a cluster-randomized controlled trial testing the impact of early delivery of evidence-based stay-at-work (SAW) and return-to-work (RTW) strategies on employment outcomes of individuals with work-limiting physical or mental health conditions recruited from the primary care setting. We included 429 intervention participants with complete data on patient engagement and relevant predictors in this analysis. Based on care manager assessment, we categorized patient engagement into four ordinal levels (none, low, medium, and high). We conducted bivariable analyses to identify potential predictors of engagement, followed by multivariable ordinal logistic regression. Variables were defined according to the PROGRESS-Plus framework, encompassing sociodemographic, clinical, and work-related characteristics.
Results: Having an injury or illness-related absence from work significantly predicted higher odds of engagement (OR = 2.87, 95% CI: 1.81– 4.56), while unemployment predicted lower engagement (OR = 0.43, 95% CI: 0.27– 0.63) compared to employer-based job. Participants with a high school education or less (OR = 0.40, 95% Cl: 0.23– 0.69), followed by college education (OR = 0.52, 95% Cl: 0.31– 0.88) engaged less than those with post-graduate education. Also, poor or fair self-rated health (OR = 1.87, 95% Cl: 1.31– 2.68) and age (OR = 1.02 per year, 95% CI: 1.01– 1.04) significantly predicted higher engagement odds. Multivariate model diagnostics supported the proportional odds assumption (χ2(14) = 18.5, p = 0.183).
Conclusion: These findings highlight the importance of tailored work disability prevention strategies based on health, work, and educational profiles to optimize patient engagement.
Keywords: work disability, out-of-work, stay-at-work, return-to-work, PROGRESS-plus, social determinants of health
Introduction
Engaging patients in work disability interventions has remained an elusive challenge within the healthcare community, with little research exploring influential factors.1,2 Conventional definitions of patient engagement typically assess success based only on measurable outcomes, such as return-to-work (RTW) and stay-at-work (SAW) statistics.3–7 These outcome-focused definitions often overlook the broader nature of patient engagement, which extends beyond whether a person returns to or remains in the workforce. Instead, the overall effectiveness of the intervention depends on the unfolding of the engagement process over time, including active involvement, communication with care coordinators, and adherence to treatment protocols.1,2 Individuals facing work disability encounter a unique set of barriers that extend beyond clinical recovery or stabilization that profoundly impact their ability to remain involved in care programs.8 Focusing solely on SAW and RTW outcomes neglects the complex, evolving interaction between patients and their care teams, which is central to understanding and improving engagement in work disability programs. In light of this, the complexities of patient engagement throughout the care coordination process are vastly underexplored.9
Many common engagement measures such as enrollment numbers or session attendance fail to address the complex nature of engagement including that level of engagement does not necessarily correlate with frequency of contact.10–12Engagement can be viewed through a continuum framework, including the influence of psychological readiness, motivation, healthcare resources, social support and healthcare system interactions.1,2 Patient engagement can be conceptualized in three interconnected phases: recruitment and commitment, active participation, and sustained retention. These phases have the potential for engagement fluctuations, acknowledging that temporary disengagement and re-engagement patterns are typical, especially among individuals experiencing the interplay of health and occupational challenges.9 Therefore, this framework embraces the notion that engagement is an ongoing, evolving process that can ebb and flow throughout a care program. Moreover, patients may engage in their care plan in ways that do not require frequent care coordinator contact.
Prior studies suggest that engagement with case management (support for those managing health conditions) and work reintegration services (which help employees RTW after injury or illness) depends on individual, work, and program factors and need to be further explored.13 Individually, higher education/health literacy (the ability to process health information), as well as older age, support sustained participation.8–10,14 In contrast, pain, limitations, depression, and multimorbidity (two or more health conditions) are barriers.15 At work, supervisor support, early coordination, and flexibility encourage plan adherence, while high demands and low control reduce engagement.16 Additionally, structured intake, shared goals, frequent monitoring, multidisciplinary access, and rapid problem-solving in interventions promote participant engagement.17
Despite the increasing recognition of patient engagement as critical to healthcare success, substantial gaps remain in our understanding of how engagement unfolds, particularly in programs designed for individuals facing work disability. Several factors have been shown to influence engagement in work disability prevention programs, including socioeconomic status, health literacy, perceived self-efficacy, employer support, and workplace accommodations.8–10 However, there is limited research on the influence of such factors throughout the intervention process.9 Moreover, few studies have examined whether subgroups of patients, such as those with comorbid conditions, lower socioeconomic status, or high perceived job insecurity, face disproportionate barriers to sustained engagement.8,11,18 In addition, most existing models of engagement focus on treatment adherence rather than considering engagement as a multi-phase process that accounts for fluctuations in patient commitment.5,9 These findings are derived mainly from cross-sectional or qualitative studies, limiting their long-term applicability in healthcare settings. The absence of longitudinal analyses further limits the ability to predict disengagement risks and identify critical intervention points.11,12
Given the relative paucity of studies directly measuring engagement in care coordination settings, we sought to identify social determinants of health (SDOH) that are associated with patient engagement, by applying a continuum-based definition of engagement drawn from related RTW and case-management literature to inform our a priori hypotheses and covariate models that distinguishes between early dropout and sustained adherence, informing targeted interventions for at-risk groups.
Materials and Methods
Vermont (VT) RETAIN Phase II Program
The Retaining Employment and Talent After Injury/Illness Network (RETAIN) initiative is a collaborative effort between the US Department of Labor’s (DOL) Office of Disability Employment Policy (ODEP), DOL’s Employment and Training Administration (ETA), the Social Security Administration (SSA) focused on evaluating evidence-based early intervention strategies to improve SAW and RTW outcomes for individuals facing work disability, defined as the inability to work because of a health condition.19
The Vermont (VT) RETAIN care coordination program (NCT05146362)20 presents a unique opportunity to investigate factors influencing patient engagement from case management initiation to study completion, thereby advancing our understanding of real-world barriers and facilitators to sustained participation in work disability interventions.
Study Design and Population
The VT RETAIN Phase II program was a structured, parallel-group, cluster-randomized trial with primary care practices as the unit of allocation. The allocation ratio was 1:1, randomly assigning 119 primary care clinics as participant clusters to the intervention or control groups. VT RETAIN recruited clinics through the state’s Accountable Care Organization (ACO), OneCare Vermont, which maintains a list of practices that serve the target population in all 14 counties, including the 12 counties with designated Opportunity Zones.21 The study population was adults aged 18 and older who were either working or out of work but wanted to work and who had a work-limiting mental or physical health condition. Healthcare providers from enrolled sites, employers, and workforce development agencies could refer individuals to the VT RETAIN program or individuals could self-refer. Enrolled sites were in both urban centers and rural areas of Vermont, US Outreach and recruitment efforts eased access to the program through posters in medical offices and community spaces and through newspaper and social media advertisements.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The Institutional Review Board (IRB) at Dartmouth Health reviewed and approved the VT RETAIN Phase II program protocol and all recruitment materials and deemed the program exempt (STUDY00031704); therefore, signed written consent was not required. However, to ensure ethical compliance and participant autonomy, verbal informed consent was obtained from all participants prior to enrollment. Participants also signed a HIPAA-compliant authorization form permitting communication between the RETAIN intervention team, their primary care provider, and other individuals they selected to participate in their SAW and RTW care team. The Human Research Protection Office IRB at the University of Pittsburgh approved the VT RETAIN program protocol for the Data Coordinating Center (STUDY21080174) and separately approved the Center on Health Services Training and Research (CoHSTAR) (STUDY23080195) pilot grant for secondary analysis of deidentified VT RETAIN data. All data used in this study were deidentified prior to analysis, and participant confidentiality was maintained throughout the research process.
Care Coordination and Partnerships
The VT RETAIN Phase II program, in partnership with Mathematica—with expertise in long-term employment outcomes and Social Security Disability Insurance (SSDI) claims—performed statistical analyses to assess sample size and detect meaningful changes in disability proportions using SSA claims at one year post-enrollment. Recognizing that VT RETAIN is spearheading a crucial statewide initiative to standardize questionnaires that incorporate the burden of work as a vital SDOH, CoHSTAR was poised to leverage this moment by evaluating the barriers and facilitators of engagement—a key focus of CoHSTAR’s expertise in implementation science and quality improvement research—deepening our insights and potentially transforming the way we support individuals on their path to recovery from work disability and reintegration into the workforce.
VT RETAIN delivered its Phase II program through a multi-institutional collaboration involving Dartmouth Health, the University of Pittsburgh, the Vermont DOL, and additional statewide partners. Clinical teams, including WHCs and study coordinators (SCs), oversaw participant recruitment, intake, and program adherence to ensure fidelity. The University of Pittsburgh DCC managed data collection, quality assurance, and reporting. This structure ensured consistency in enrollment, data capture, and program delivery across clinical sites.
All practices received evidence-based SAW and RTW information, training, and resources, including access to an “Occ Doc Hotline.” All enrolled participants received a list of work-health resources and SAW and RTW tips to self-navigate their RTW process.
VT RETAIN Phase II Program Initiative
VT RETAIN provided up to six months of individualized work health coaching to participants with work disability, delivered primarily via phone or mobile application, with in-person support available as needed. Work-health coaches (WHC)—licensed professionals with expertise in SAW and RTW—conducted structured intake assessments, identified health-job mismatches, and collaboratively developed SAW and RTW plans with participants and their care teams. Additionally, WHCs facilitated weekly multidisciplinary hub team meetings to provide access to expertise in areas such as occupational medicine, vocational rehabilitation, employment law, and rapid referral pathways for mental health or social service crises, as well as community resources, while monitoring progress toward participants’ work and health goals. Discharge for participants occurred either after they achieved their work and health goals or after six months, with referrals made to ongoing services as needed.
Data Collection
Participants were enrolled through structured participant self-report surveys, standardized screening instruments, and WHC documentation. Demographic and socioeconomic characteristics (including age, sex, race and ethnicity, rural or urban residence, education level, employment status, occupation, monthly income, and workers’ compensation status) were self-reported. Health predictors included the presence of comorbidities (such as back pain, hypertension, diabetes, or depression), general health status assessed using a single-item self-rated health question, and behavioral health risk evaluated through the Behavioral Screening and Intervention (BSI) tool. The BSI incorporated validated instruments, including the Patient Health Questionnaire-2 (PHQ-2)22–24 for depression, the Generalized Anxiety Disorder-2 (GAD-2) for anxiety,24 and a brief mental health screening tool for substance use disorders,22 symptoms, mood, sleep, and motivation. An outgrowth of the VT RETAIN program continues to integrate SDOH questionnaires with the inclusion of a question that helps to quickly and easily identify work disability to aid in more timely identification and intervention, such as injury or illness-related work absence, time since last worked, and industry classification, collected during structured intake interviews and verified when available with clinical or employer documentation.
Data Management
We used Research Electronic Data Capture (REDCap) and a customized electronic data capture system (EDC) to collect, manage, and store all evaluation data. REDCap was used to manage all primary care practice data, including clinic contact information, clinic size, clinician lists, and randomization status. The EDC, a customized web application, was used to store all participant-level data and was built using the .NET and Angular development stack with Microsoft Windows Server for an operating system, SQL Server for a relational database system, and the C# programming language. Access to both the REDCap project and the customized EDC was password-protected with each user having a unique login and role-based access. Participant-level data was stored on a secure server and maintained by the DCC. Data entry was completed by WHCs and SCs, with oversight from the DCC, and structured in alignment with requirements from the US DOL to ensure comparability across RETAIN demonstration projects.
PROGRESS-Plus Framework
The PROGRESS-Plus framework was initially proposed to support interventions targeting disparities in health outcomes and has since been expanded to guide the routine collection and classification of participant-level data in observational and interventional research.25 The acronym PROGRESS refers to: Place of residence, Race/ethnicity/culture/language, Occupation, Gender/sex, Religion, Education, Socioeconomic status, and Social capital. The “Plus” component extends the framework to include additional context-specific factors such as age, disability, and other personal characteristics that may contribute to health inequities.
Study Sample and Cohort Selection
The study sample includes intervention participants who met the inclusion criteria for the Vermont RETAIN Phase II program, enrolled from May 31, 2022, until May 16, 2024, and have complete data for variables relevant to the PROGRESS-Plus framework. Participants assigned to control clinics during the enrollment period did not receive care coordination services, resulting in no measure of engagement; therefore, they were excluded from this analysis.
Sample Size Considerations
We performed no independent power calculation since the VT RETAIN program determined the sample size. The original cluster-randomized controlled trial was powered to detect differences in RTW outcomes between intervention and control clinics. Specifically, assuming a control rate of 25% of participants out of work at one year, an intra-cluster correlation coefficient of 0.02, and alpha of 0.05, the planned enrollment of 1,020 participants per group (34 clinic clusters with about 30 participants each) provided 85% power to detect a 27.5% relative reduction (absolute difference of 6.8%) in work disability between groups.20 Although the present analysis includes only intervention participants, the achieved sample size was adequate for multivariable modeling, as indicated by the stability of estimates and model diagnostics.
Study Variables
Potential Predictors
To guide the selection of potential predictors in our analysis, we included a selection of PROGRESS-Plus variables based on data availability and relevance to our care coordination context. These included Place of Residence [Rural vs Urban]; Race/Ethnicity/Culture/Language [White vs Non-White, Hispanic vs Non-Hispanic]; Occupation [current employment status, North American Industry Classification System (NAICS) recategorized as manual vs non-manual labor,26 and Standard Occupational Classification (SOC)];27 Sex [female vs male]; Education (high school or less vs college vs post-graduate); Socioeconomic Status [<$1000 vs ≥$1000 income per month], workers’ compensation claim [yes vs no], health insurance [yes vs no], PLUS indicators (age [at enrollment], general health [poor/fair vs good/very good/excellent], and mental health disorder, including psychoactive substance related disorders [yes vs no], Injury or illness-related absence from work [yes vs no], program-eligible condition [injury vs illness], condition chronicity [new onset condition vs worsening of an existing condition]. PROGRESS-Plus data on Religion and Social Capital (community engagement, social support, or networks) were unavailable.
We characterized rural-urban residence using a spatial join to classify Zip Code Tabulation Areas (ZCTAs) as urban or rural based on the spatial relationship between ZCTA boundaries and the US Census Urban Area boundaries, using shapefiles from the TIGER/Line dataset.28
Outcome
The primary outcome variable was based on the WHC’s response to the statement “Please check the option that best describes the enrollee’s level of engagement with the WHC and their SAW and RTW plan.” The WHC served as the care coordinator in VT RETAIN. Allowing for engagement to be measured on a continuum—adapted from the ODEP questions on employer and healthcare provider engagement—response options were on a four-point ordinal scale including no engagement, low engagement, medium engagement, or high engagement based on the WHC’s perspective. WHCs received formal training on the use of this scale, including examples and case vignettes to ensure consistency across sites:
- None: Participant were either lost to contact (LTC) at enrollment with SCs, did not complete the case management intake process with WHCs, withdrew immediately, or had no meaningful interaction beyond enrollment.
- Low: Participant completed enrollment with SCs and case management intake with WHCs but had limited interaction thereafter, demonstrated minimal follow-through on agreed tasks, and did not actively collaborate on a SAW and RTW plan.
- Medium: Participant maintained some follow-through interactions following enrollment and case management intake, collaborated with WHCs on a SAW and RTW plan, and addressed at least one barrier or resource referral, though engagement throughout the 6-month period was inconsistent.
- High: Participant actively collaborated with the WHC throughout the 6-month period, consistently followed through on SAW and RTW planning tasks, addressed multiple barriers (eg, health, workplace, or social), engaged during resource referrals and demonstrated self-advocacy in work-health management.
Engagement scoring was based on WHC documentation in structured progress notes. WHCs promoted scoring consistencies during weekly multidisciplinary hub meetings to enhance inter-rater reliability across WHCs and minimized variability in engagement ratings.
This framework captures varying levels of participant involvement in achieving successful employment outcomes in a care coordination setting.
Statistical Analyses
Descriptive statistics summarized the study sample’s baseline characteristics. Means (± standard deviations) or medians (± interquartile ranges) provided summary statistics for continuous variables. Counts and percentages summarized categorical variables. Additionally, we reported the distribution of the WHC-reported level of engagement to provide an overview of overall patient engagement.
We first examined each potential predictor (based on the PROGRESS-Plus framework) in isolation to determine its association with the WHC-reported level of engagement. We assessed associations comparing engagement levels using ANOVA for continuous predictors and Pearson’s Chi-square tests (or Fisher’s exact tests, as appropriate) for categorical predictors.
We used a liberal p-value threshold of p < 0.20 from the bivariable analyses to retain variables for multivariable model inclusion, consistent with best variable selection practices.29 We evaluated the final models using Akaike Information Criterion (AIC) values to compare relative model fit. We also excluded variables that worsened the model fit (ie, increased AIC) unless justified by theoretical or clinical relevance. We further evaluated multicollinearity using Variance Inflation Factors (VIFs). We ensured that predictors exhibiting a VIF of more than five were not in the same multivariate model. Lastly, we assessed the score test for the proportional odds assumption during the analysis. A nonsignificant test statistic indicated that the assumption holds, and therefore the relationship between predictors and the odds of higher engagement levels was consistent across thresholds.
We conducted all analyses using SAS 9.4, employing appropriate procedures to run the statistical analyses and to estimate effect size. We also used ArcGIS Pro version 3.4.3 to characterize urban-rural residence. We evaluated statistical significance at a two-tailed alpha level of 0.05.
Results
Of the 798 program-eligible participants within the enrollment period, 56.4% (n = 450) were assigned to the intervention group. Ninety five percent (n = 429) Vermonters receiving the intervention had complete data on either level of engagement or LTC status from before and after case management intake and at discharge. For these participants, all predictor variables were complete, and no imputation was required.
The most significant proportion of patients were highly engaged, 35.7% (n = 153), followed by low engagement at 24.7% (n = 106), no engagement at 22.4% (n = 96), and medium engagement at 17.2% (n = 74). Program participants were primarily female (61.9%, n = 255), White (91.4%, n = 392), and non-Hispanic/Latino (95.6%, n = 410) (Table 1). Age (at enrollment), program-eligible primary condition (injury vs illness), general health status (poor/fair vs good/very good/excellent), injury or illness-related absence from work (yes vs no), and employment status (employer-based vs [not employed and self-employed]) were significantly associated with engagement, while presence of mental health disorders, including psychoactive substance related disorders was marginally significant.
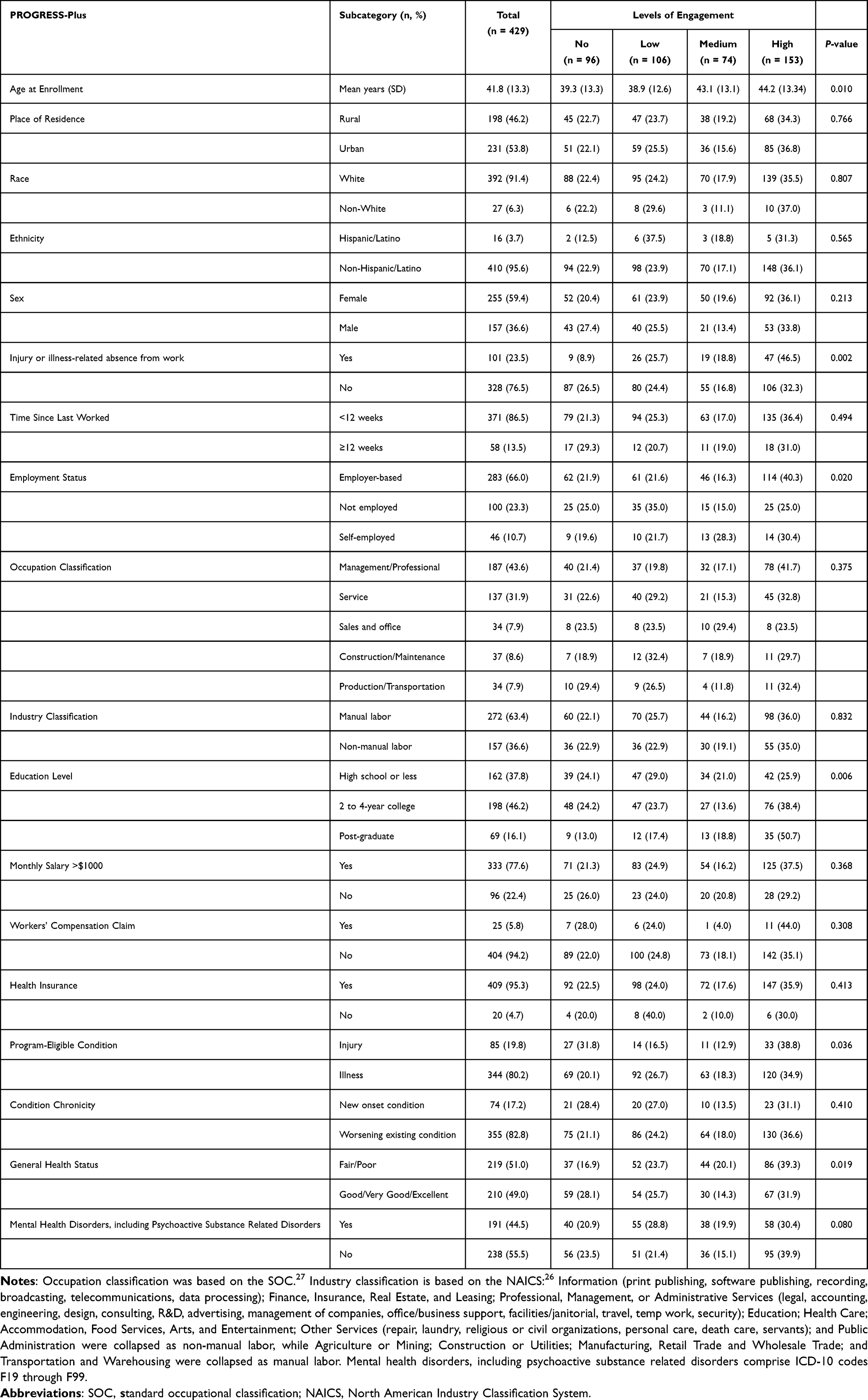 |
Table 1 Bivariable Analyses of Baseline Characteristics by Level of Engagement |
Engagement levels appeared evenly distributed across rural and urban settings (Table 1). The mean age of participants increased progressively from lower to higher engagement levels (p = 0.010). Participants with employer-based jobs demonstrated the highest engagement compared to those who were self-employed and unemployed (p = 0.020). Similarly, injury or illness-related absence from work was significantly associated with higher engagement levels than those without (p = 0.002). Also, individuals with post-graduate education demonstrated higher engagement levels than those with a high school education or less (p = 0.006). Individuals reporting poor or fair health had higher engagement compared to those who reported good, very good, or excellent health (p = 0.019). Moreover, participants with illnesses had higher engagement than those with injuries (p = 0.036). However, those with a mental health diagnosis had lower engagement levels, although it was marginally significant (p = 0.080).
Guided by the p-value threshold of p < 0.20 from the bivariate analyses, we constructed a multivariable ordinal regression, including the potential predictors as listed in Table 2. Model 1 and Model 2 excluded mental health diagnosis and program-eligible primary condition, respectively, because they were not significant, worsened the logit model fit, and violated the proportional hazard assumption.
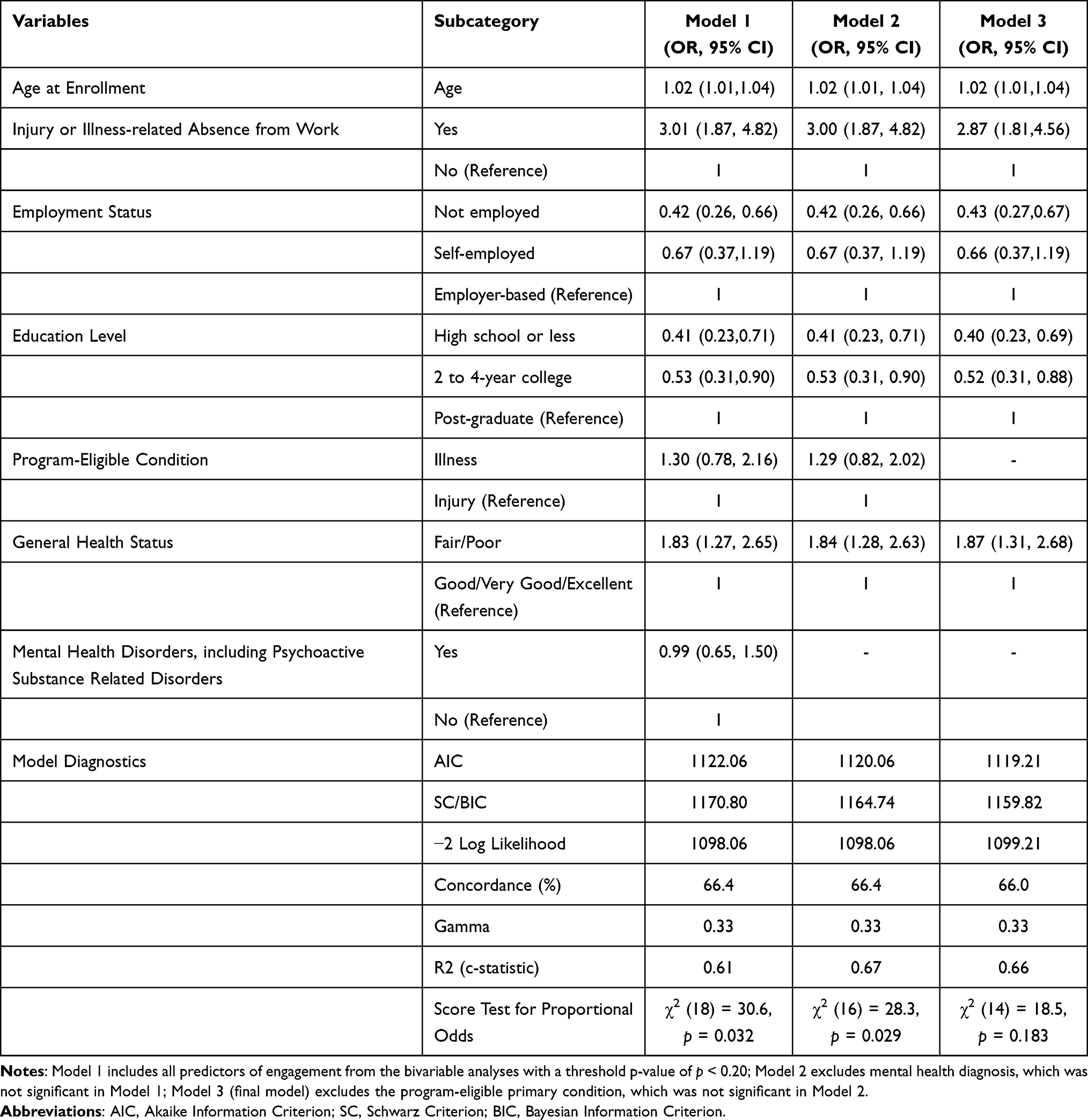 |
Table 2 Multivariable Modeling of Predictors of Engagement |
In the final model (Model 3), participants with a injury or illness-related absence from work had significantly higher odds of engagement compared to those without a health-related work absence (OR = 2.87, 95% CI: 1.81–4.56), while being unemployed was associated with significantly lower odds of engagement compared to those with employer-based jobs (OR = 0.43, 95% CI: 0.27–0.67). Compared to participants with post-graduate education, those with a high school education or less (OR = 0.40, 95% CI: 0.23–0.69) and those with some college education (OR = 0.52, 95% CI: 0.31–0.88) had significantly lower odds of engagement. In contrast, reporting poor or fair health (OR = 1.87, 95% CI: 1.31–2.68) and being older (OR = 1.02 per year increase, 95% CI: 1.01–1.04) were associated with significantly higher odds of engagement.
Discussion
Our findings reveal that some PROGRESS-Plus factors predicted WHC-reported patient engagement in the care coordination program. Injury or illness-related work absence, age, and fair or poor self-rated health were associated with higher engagement. In contrast, not being employed and lower education attainment were linked to lower engagement. These results underscore the role of individual and social in patient engagement and are consistent with factors identified in the literature to improve engagement for vulnerable groups.
The VT RETAIN Phase II program showed that injury or illness-related absence from work increased the odds of engagement by approximately three-fold. While specific studies directly linking health-related work absences to higher engagement are limited, research indicates that individuals with health-related work absences often have increased healthcare utilization, which could correlate with higher engagement levels.30,31 Although unemployed participants were less engaged in our care coordination program, those reporting poorer health were more engaged. However, prior research has shown that unemployment predicts poorer self-rated health.32 This contrast may reflect heightened healthcare needs among individuals with poor self-rated health, potentially overriding the disengagement typically associated with unemployment.33
We observed that the odds of higher engagement levels consistently increased with every mean increase in age, even after accounting for other factors. As individuals age, the prevalence of chronic conditions and the need for regular health monitoring increase, leading to higher engagement levels with healthcare services, which could account for this finding.34 Also, participants in our program with higher educational attainment had higher engagement levels, consistent with prior research showing that higher education level correlates with increased patient engagement and that patients with limited education and low health literacy are at risk for poorer engagement via lower adherence and health behavior changes.35 Encouragingly, education is a modifiable factor; interventions that improve patients’ knowledge and skills (such as coaching or health literacy programs) have the potential to boost engagement across educational strata.36
We did not detect an association between rural or urban residence and engagement. Typically, rural patients are less engaged due to well-known systemic barriers in rural healthcare, such as extended travel distances to providers, transportation difficulties, lower access to health information and services, and healthcare workforce shortages.37 One study noted that 24% of rural adults had no primary care visit in the past year, compared to 19% of urban adults,38 highlighting a gap in engagement with routine care. In addition, rural patients are particularly vulnerable to dropping out of treatment, such as in substance use disorder programs.39 Despite these barriers documented in the literature, participants from rural areas in our care coordination program were as engaged as their urban counterparts. This absence of a rural-urban disparity could be due to the design of our care coordination intervention delivered via phone or telehealth, potentially minimizing geographic barriers.40
This study benefits from a comprehensive analytical framework (PROGRESS-Plus), which provides insight into who is less engaged and potential reasons in real-world contexts. Also, using an ordinal engagement measure captures gradations of patient involvement, adding nuance beyond a simple engaged or not engaged dichotomy. Hence, our approach reflects the multifactorial nature of engagement, isolates the independent effect of predictors, and enhances the internal validity of our findings.
It is important to note that data used in this analysis was observational, so we cannot definitively establish causality for the associations observed; unmeasured confounders such as patient motivation, health literacy, or intervening circumstances (eg, caregiving responsibilities, hospitalizations, or family emergencies), study factors such as enrolling solely for the financial compensation, or program factors such services that were not in the scope of the program that would meet participant needs might explain some findings. Another limitation is that our study population comes from a specific program context (a workforce health management setting), which may limit generalizability. In addition, some PROGRESS-Plus dimensions were not fully represented in our data. For instance, we did not analyze social capital and religious belief systems in depth. Importantly, all predictor variables were complete for these participants; hence, the regression analyses were on the full analytic sample without imputation. Given the negligible degree of missingness, bias due to incomplete data is unlikely.
Despite these limitations, our study contributes new knowledge about the predictors of engagement in a coordinated care setting and offers practical insights for enhancing patient participation. While participants absent from work due to their health showed increased engagement, this pattern may reflect elevated healthcare needs rather than structural supports. Future studies with more diverse samples and in different settings should confirm whether these findings hold. Finally, while we focused on patient engagement as the outcome, we did not directly measure downstream outcomes in this analysis such as functional improvement or SAW and RTW success. Future studies could show that improving engagement through the identified factors will translate into better health or work outcomes.
Conclusion
Our study reveals the influence of individual and social factors highlighted through the PROGRESS-Plus framework on patient engagement in care coordination. Key factors such as employment context, education, age, and self-rated health significantly shape how patients engage with care coordination. Our findings highlight practical ways to improve engagement among vulnerable populations and advancing more care coordination strategies.
Acknowledgments
We thank the Foundation for Physical Therapy Research (FPTR) in partnership with the American Physical Therapy Association (APTA) for funding the CoHSTAR program involving collaborating institutions: Brown University (Research Career Training Program Core) and University of Pittsburgh (Pilot Studies Core). Our gratitude also goes to the VT RETAIN federal sponsors: the US DOL’s ODEP, ETA, and SSA. We appreciate the contributions from the independent evaluator, Mathematica, the American Institutes for Research for their technical assistance, the entire VT RETAIN team, including SCs and WHCs, as well as to the workers, clinicians, employers, and partners involved in the program. Finally, we thank Ugochi Person for classifying urban and rural residences using ZCTA and US Census boundaries.
Funding
This study was supported through a pilot grant from CoHSTAR under the Research Career Training Program Core at Brown University (Grant Office ID: AWD00008077; Funding Source ID: 00002224). The CoHSTAR project represents a secondary analysis of deidentified data collected through the VT RETAIN Phase II program and fulfills CoHSTAR’s objectives, which are distinct from those of the original VT RETAIN study The VT RETAIN Phase II program is funded by the US Department of Labor (DOL) and the Social Security Administration (SSA) under a grant award to the Vermont Department of Labor (Phase I #OD-32547-18-75-4-50; Phase II #OD-36366-21-75-4-50) totaling $21,600,000 in US federal funds.The content of this paper does not necessarily reflect the views, policies, or positions of FPTR, APTA, or US DOL’s ODEP, ETA, and SSA. Mention of trade names, commercial products, or organizations does not imply endorsement by any US government agency.
Disclosure
The authors report no conflicts of interest in this study.
References
1. O’Connor S, Hanlon P, O’Donnell CA, et al. Understanding factors affecting patient and public engagement and recruitment to digital health interventions: a systematic review of qualitative studies. BMC Med Inform Decis Mak. 2016;16:
2. Barello S, Graffigna G, Vegni E. Patient engagement as an emerging challenge for healthcare services: mapping the literature. Nurs Res Pract. 2012;2012:
3. Bombard Y, Baker GR, Orlando E, et al. Engaging patients to improve quality of care: a systematic review. Implement Sci. 2018;13:
4. Main CJ, Shaw WS, Nicholas MK, et al. System-level efforts to address pain-related workplace challenges. Pain. 2022;163:1425–1431.20211129. doi:10.1097/j.pain.0000000000002548
5. Mease P, Arnold LM, Bennett R, et al. Fibromyalgia syndrome. J Rheumatol. 2007;34:1415–1425.
6. Vooijs M, Hazelzet AM, van Kesteren NMC, et al. A qualitative study into the perspectives of clients on shared decision-making as a method to support return to work. Work. 2023;74:227–235. doi:10.3233/wor-211023
7. Vooijs M, van Kesteren NMC, Hazelzet AM, et al. Shared decision making from reintegration professionals’ perspectives to support return to work: a qualitative study. BMC Public Health. 2021;21:
8. Tousignant-Laflamme Y, Longtin C, Coutu MF, et al. Self-management programs to ensure sustainable return to work following long-term sick leave due to low back pain: a sequential qualitative study. Work. 2023;75:729–739. doi:10.3233/wor-220202
9. Shaw WS, McLellan RK, Besen E, et al. A worksite self-management program for workers with chronic health conditions improves worker engagement and retention, but not workplace function. J Occup Rehabil. 2022;32:77–86.20210513. doi:10.1007/s10926-021-09983-6
10. Brouwer S, Franche RL, Hogg-Johnson S, et al. Return-to-work self-efficacy: development and validation of a scale in claimants with musculoskeletal disorders. J Occup Rehabil. 2011;21:244–258. doi:10.1007/s10926-010-9262-4
11. Gudu T, Kiltz U, de Wit M, et al. Mapping the effect of psoriatic arthritis using the international classification of functioning, disability and health. J Rheumatol. 2017;44:193–200.20161215. doi:10.3899/jrheum.160180
12. Marinescu LG. Integrated approach for managing health risks at work--the role of occupational health nurses. Aaohn J. 2007;55:75–87. doi:10.1177/216507990705500205
13. Föhner K, Seipp H, Becker A, et al. Factors associated with return-to-work outcomes in inpatient rehabilitation - a systematic scoping review. Psychol Health Med. 2024;29:191–215.20240109. doi:10.1080/13548506.2023.2269497
14. Lo CH, Knox MJ, Hernandez EA, et al. Factors associated with patient engagement in a health and social needs case management program. J Am Board Fam Med. 2024;37:418–426. doi:10.3122/jabfm.2023.230388R1
15. Hedlund Å, Nilsson A, Boman E, et al. Predictors of return to work and psychological well-being among women during/after long-term sick leave due to common mental disorders - a prospective cohort study based on the theory of planned behaviour. Health Soc Care Community. 2022;30:e5245–e5258.20220727. doi:10.1111/hsc.13943
16. Haveraaen LA, Skarpaas LS, Aas RW. Job demands and decision control predicted return to work: the rapid-RTW cohort study. BMC Public Health. 2017;17:
17. Lettinga HAM, van Oostrom SH, Zijlstra HP, et al. Facilitators and barriers for a stepped care approach to promote return to work of employees with distress: a multi-perspective qualitative study. J Occup Rehabil. 2025:20250516. doi:10.1007/s10926-025-10301-7
18. Peinado-Rubia A, Osuna-Pérez MC, Rodríguez-Almagro D, et al. Impaired balance in patients with fibromyalgia syndrome: predictors of the impact of this disorder and balance confidence. Int J Environ Res Public Health. 2020;17:20200501. doi:10.3390/ijerph17093160
19. U.S. Department of Labor. Retaining employment and talent after injury/illness network (RETAIN) impact evaluation. Available from: https://www.dol.gov/resource-library/retaining-employment-and-talent-after-injuryillness-network-retain-impact. (2021,
20. Mathematica policy research i. vermont RETAIN Impact Evaluation, 2022. Available from: https://clinicaltrials.gov/study/NCT05146362.
21. State of Vermont AoCaCD. Opportunity Zones, 2025. Available from: https://accd.vermont.gov/OpportunityZones.
22. Kroenke K, Spitzer RL, Williams JB, et al. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. 2009;50:613–621. doi:10.1176/appi.psy.50.6.613
23. Duarte M, Salamanca M, Gonzalez JM, et al. Prediction of positive patient health questionnaire-2 screening using area deprivation index in primary care. Clin Nurs Res. 2024;33:355–369.20240527. doi:10.1177/10547738241252887
24. Bisby MA, Karin E, Scott AJ, et al. Examining the psychometric properties of brief screening measures of depression and anxiety in chronic pain: the patient health questionnaire 2-item and generalized anxiety disorder 2-item. Pain Pract. 2022;22:478–486.20220312. doi:10.1111/papr.13107
25. Karran EL, Cashin AG, Barker T, et al. Using PROGRESS-plus to identify current approaches to the collection and reporting of equity-relevant data: a scoping review. J Clin Epidemiol. 2023;163:70–78.20231004. doi:10.1016/j.jclinepi.2023.09.017
26. U.S. Census Bureau. North American Industry Classification System (NAICS), Office of Management and Budget (OMB), 2025. Available from: https://www.census.gov/naics/.
27. U.S. Bureau of Labor Statistics. Standard Occupational Classification. Available from: www.bls.gov/SOC.
28. U.S Census Bureau. ZIP code tabulation areas (ZCTAs), Available from: https://www.census.gov/programs-surveys/geography/guidance/geo-areas/zctas.html.
29. Bursac Z, Gauss CH, Williams DK, et al. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:
30. Gangan N, Yang Y. The impact of work absences on health services utilization and costs among employed individuals with depression. J Occup Environ Med. 2018;60:e139–e145. doi:10.1097/jom.0000000000001259
31. Salkar M, Gangan N, Yang Y. Association between work absence and health services utilization and costs among employed individuals with arthritis. J Occup Environ Med. 2020;62:e240–e244. doi:10.1097/jom.0000000000001836
32. Kaleta D, Makowiec-Dabrowska T, Jegier A. Employment status and self rated health. Int J Occup Med Environ Health. 2008;21:227–236. doi:10.2478/v10001-008-0023-y
33. Silver SR, Li J, Quay B. Employment status, unemployment duration, and health-related metrics among US adults of prime working age: behavioral risk factor surveillance system, 2018-2019. Am J Ind Med. 2022;65:59–71.20211108. doi:10.1002/ajim.23308
34. Gao Q, Bone JK, Bu F, et al. Associations of social, cultural, and community engagement with health care utilization in the us health and retirement study. JAMA Netw Open. 2023;6:
35. Boyd B, McAlister C, Arrotta K, et al. Self-reported behavior change and predictors of engagement with a multidomain brain health intervention for midlife and older adults: a pilot clinical trial. J Aging Health. 2022;34:109–119.20210715. doi:10.1177/08982643211032483
36. Wigfall LT, Tanner AH. Health literacy and health-care engagement as predictors of shared decision-making among adult information seekers in the USA: a secondary data analysis of the health information national trends survey. J Cancer Educ. 2018;33:67–73. doi:10.1007/s13187-016-1052-z
37. Nelson L. Top patient engagement challenges affecting rural healthcare. Available from: https://www.techtarget.com/patientengagement/feature/Top-Patient-Engagement-Challenges-Affecting-Rural-Healthcare#:~:text=Top%20Patient%20Engagement%20Challenges%20Affecting,the%20long%20travel%20distances.
38. Loftus J, Allen EM, Call KT, et al. Rural-urban differences in access to preventive health care among publicly insured minnesotans. J Rural Health. 2018;34(1):s48–s55.20170314. doi:10.1111/jrh.12235
39. Raver E, Retchin SM, Li Y, et al. Rural–urban differences in out-of-network treatment initiation and engagement rates for substance use disorders. Health Serv Res. 2024;59:
40. National Rural Health Association (NRHA). Telehealth’s impact on rural hospitals: a literature review. RuralHealth.us. Available from: https://www.ruralhealth.us/blogs/2025/02/telehealth-s-impact-on-rural-hospitals-a-literature-review#:~:text=Telehealth%27s%20impact%20on%20rural%20hospitals%3A,distance%20travel.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.